

An aberrant right posterior hepatic duct is one of the most common risk factors for bile duct injury during surgical procedures. Complete transection of the bile duct necessitates surgical repair. Recently, endoscopic ultrasound (EUS)-guided hepaticojejunostomy using a forward-viewing echoendoscope to manage complete biliary obstruction in patients with surgically altered anatomy has been reported 1 2 3 4 . Although most of the reports described complete stenosis of hepaticojejunostomy anastomoses with pancreaticoduodenectomy and modified Child reconstruction, none has documented repairing a completely transected bile duct with Roux-en-Y hepaticojejunostomy.
A 72-year-old woman who underwent total pancreatectomy with Roux-en-Y hepaticojejunostomy for intraductal papillary mucinous carcinoma 2 months prior presented with abdominal pain. Abdominal computed tomography showed dilatation of the right posterior hepatic duct and small abscesses ( Fig. 1 ). A retrospective imaging review of the patient’s preoperative magnetic resonance images revealed an aberrant right posterior hepatic duct ( Fig. 2 ). Complete transection and ligation of the aberrant duct during the previous operation were suspected (Strasberg classification type B) 5 .
Fig. 1.
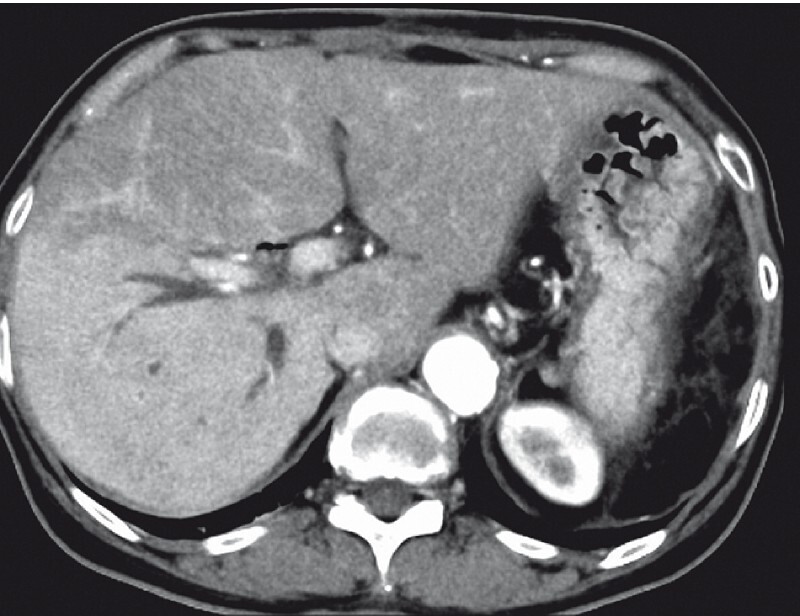
Computed tomography image shows the dilated right posterior sectoral hepatic duct and small abscesses in the area.
Fig. 2.
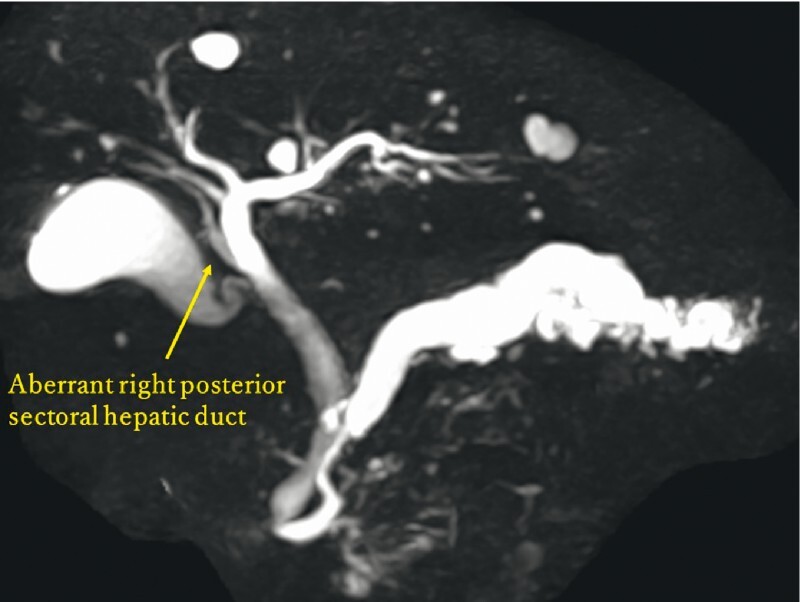
Preoperative magnetic resonance cholangiopancreatography showed an aberrant right posterior hepatic duct.
We considered performing an EUS-guided hepaticojejunostomy using the forward-viewing echoendoscope (TGF-UC260J; Olympus Medical Systems, Tokyo, Japan). However, we assumed that insertion into the bilioenteric limb around the anastomosis would be challenging owing to the Roux-en-Y reconstruction; thus, we initially performed balloon enteroscopy (SIF-290H; Olympus Medical Systems, Tokyo, Japan) to confirm the direction of the anastomosis. Upon reaching the anastomosis, a nasobiliary drainage tube was placed into the bilioenteric limb. The forward-viewing echoendoscope was then successfully advanced into the hepaticojejunostomy anastomosis with tube guidance. Subsequently, the dilated right posterior hepatic duct was punctured with a 19-gauge needle, and a 0.025 guidewire was introduced into the bile duct. The puncture site was dilated with a mechanical dilator (ES dilator; Zeon Medical, Tokyo, Japan) and a plastic stent was placed (SUZAKU; Kaneka Medix, Osaka, Japan) ( Fig. 3 , Fig. 4 , Fig. 5 , Video 1 ). The patient immediately recovered and was promptly discharged 4 days after the procedure.
Fig. 3.
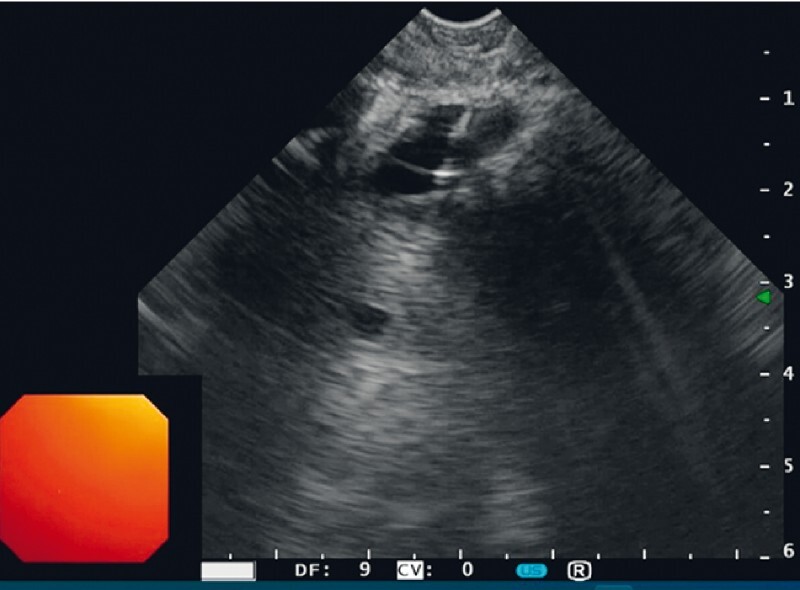
Endoscopic ultrasound image: The completely transected right posterior hepatic duct was punctured using a forward-viewing echoendoscope.
Fig. 4.

Fluoroscopic image shows plastic stent placement into the completely transected right posterior hepatic duct using a forward-viewing echoendoscope.
Fig. 5.
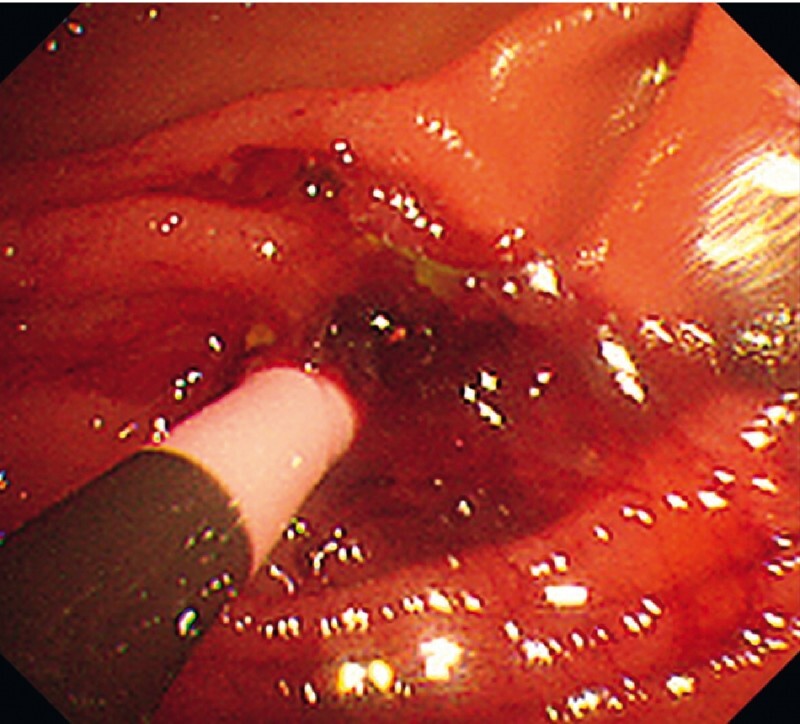
Endoscopic image shows plastic stent placement into the completely transected right posterior hepatic duct using a forward-viewing echoendoscope.
Video 1 Endoscopic ultrasound-guided hepaticojejunostomy for completely transected aberrant right posterior sectoral duct in a patient with total pancreatectomy and Roux-en-Y hepaticojejunostomy successfully performed using a forward-viewing echoendoscope.
Endoscopy_UCTN_Code_CPL_1AL_2AD
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Kida M, Yamauchi H, Okuwaki K et al. Endoscopic ultrasound-guided choledochojejunostomy with a forward-viewing echoendoscope for severe benign bilioenteric stricture in a patient with Child's resection. Endoscopy. 2015;47:E303–E304. doi: 10.1055/s-0034-1392208. [DOI] [PubMed] [Google Scholar]
- 2.Iwai T, Kida M, Yamauchi H et al. EUS-guided transanastomotic drainage for severe biliopancreatic anastomotic stricture using a forward-viewing echoendoscope in patients with surgically altered anatomy. Endosc Ultrasound. 2021;10:33–38. doi: 10.4103/eus.eus_72_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ishiwatari H, Sato J, Kaneko J. Hepaticojejunostomy for the right hepatic bile duct using a forward-viewing echoendoscope in a patient after pancreatoduodenectomy. Dig Endosc. 2019;31:e82–e83. doi: 10.1111/den.13390. [DOI] [PubMed] [Google Scholar]
- 4.Okamoto T, Nakamura K, Yabuta M et al. Retrograde endosonography-guided hepaticojejunostomy after failed rendezvous in a patient with Childʼs resection. Endoscopy. 2022;54:E131–E132. doi: 10.1055/a-1443-4244. [DOI] [PubMed] [Google Scholar]
- 5.Strasberg S M, Hertl M, Soper N J. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180:101–125. [PubMed] [Google Scholar]