

The usefulness of therapeutic modalities using double-balloon endoscopy for biliary disease in postoperative patients has been widely reported 1 2 3 , while papers published about its use in pancreatic disease are scarce, despite an increasing demand for such treatment. This is the first report of successful double-balloon endoscopy-assisted endoscopic retrograde pancreatography (DB-ERP) using a clear long cap for a pinhole-like benign stricture in the pancreaticojejunal anastomosis after pancreaticoduodenectomy.
A 63-year-old woman who had undergone pancreaticoduodenectomy for a lower bile duct cyst with abnormal confluence suffered recurrent pancreatitis 1 year after surgery. Obstructive pancreatitis due to stenosis in the pancreaticojejunal anastomosis was suspected on imaging ( Fig. 1 ). The main pancreatic duct (PD) was mildly dilated, which posed a risk for intervention by endoscopic ultrasound (EUS), so we decided to perform DB-ERP instead. A clear long cap ( Fig. 2 ) was attached in an attempt to make any endoscopic maneuvers smoother. The expected advantages of this were: to allow it to be pressed against the intestinal wall, so that even sutures covered by mucosa could be easily detected; to allow the pancreaticojejunal anastomosis to be shown in the vertical direction, instead of the normal tangential direction; to allow a certain distance to be maintained between the endoscope and the pancreaticojejunal anastomosis, which would enable smooth endoscopic procedures and blind maneuvers to be avoided.
Fig. 1 .

Image from a preprocedure computed tomography scan showing mild pancreatic duct dilatation.
Fig. 2.
Photograph showing the difference between the clear long cap (left) and a conventional cap (right).
First, the pancreaticojejunal anastomosis was identified by fluoroscopic image, and the sutures fixing the pancreas and jejunum were then detected endoscopically ( Fig. 3 a ). By careful observation in the area of the sutures, the scar-like mucosa and the pinhole-like stricture of the pancreaticojejunal anastomosis were successfully identified ( Fig. 3 b ). Pancreatography and deep cannulation were performed successfully, and were followed by anastomotic dilation and PD stenting ( Video 1 ). Following the successful completion of DB-ERP, the patient was discharged on the fourth day, without experiencing any major complications or any further pancreatitis.
Fig. 3.
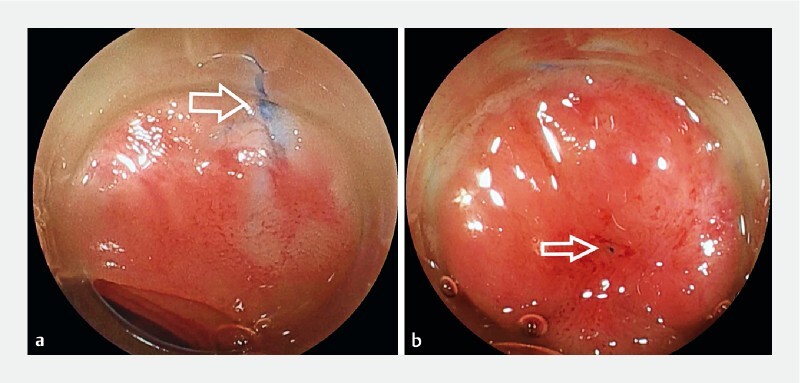
Endoscopic views showing: a the suture (arrow) fixing the pancreas and jejunum; b a scar-like ulcer in the mucosa, with a pinhole-like stenosis of the pancreaticojejunal anastomosis at its center (arrow).
Video 1 A double-balloon endoscope with a clear long cap attached is successfully used to identify a pinhole-like benign stenosis in a pancreaticojejunal anastomosis, which then allowed pancreatography and deep cannulation to be successfully performed, prior to anastomotic dilation and pancreatic duct stenting.
EUS intervention is reported to be effective for pancreatic diseases 4 5 , yet it is invasive for postoperative cases and only used selectively. In conclusion, double-balloon endoscopy approaches can be safely used in patients with a mildly dilated PD, and DB-ERP using a clear long cap is effective for pancreaticojejunal anastomosis stenosis in symptomatic patients.
Endoscopy_UCTN_Code_TTT_1AR_2AK
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Shimatani M, Hatanaka H, Kogure H et al. Diagnostic and therapeutic endoscopic retrograde cholangiography using a short-type double-balloon endoscope in patients with altered gastrointestinal anatomy: a multicenter prospective study in Japan. Am J Gastroenterol. 2016;111:1750–1758. doi: 10.1038/ajg.2016.420. [DOI] [PubMed] [Google Scholar]
- 2.Shimatani M, Mitsuyama T, Tokuhara M et al. Recent advances of endoscopic retrograde cholangiopancreatography using balloon assisted endoscopy for pancreaticobiliary diseases in patients with surgically altered anatomy – Therapeutic strategy and management of difficult cases. Dig Endosc. 2021;33:912–923. doi: 10.1111/den.13848. [DOI] [PubMed] [Google Scholar]
- 3.Skinner M, Popa D, Neumann H et al. ERCP with the overtube-assisted enteroscopy technique: a systematic review. Endoscopy. 2014;46:560–572. doi: 10.1055/s-0034-1365698. [DOI] [PubMed] [Google Scholar]
- 4.Itoi T, Sofuni A, Tsuchiya T et al. Initial evaluation of a new plastic pancreatic duct stent for endoscopic ultrasonography-guided placement. Endoscopy. 2015;47:462–465. doi: 10.1055/s-0034-1391083. [DOI] [PubMed] [Google Scholar]
- 5.Basiliya K, Veldhuijzen G, Gerges C et al. Endoscopic retrograde pancreatography-guided versus endoscopic ultrasound-guided technique for pancreatic duct cannulation in patients with pancreaticojejunostomy stenosis: a systematic literature review. Endoscopy. 2021;53:266–276. doi: 10.1055/a-1200-0199. [DOI] [PubMed] [Google Scholar]