

Colorectal endoscopic submucosal dissection (ESD) is becoming the standard of care for colorectal tumors; however, troubleshooting for complications remains a challenge, particularly when dealing with large intraoperative perforations 1 2 3 . Here, we present a case where such a large perforation was successfully treated with polyglycolic acid (PGA) sheets and a purse-string suture method using a detachable snare.
A 76-year-old woman was referred to our institution for treatment of a large flat-elevated rectal tumor. Colonoscopy revealed that the tumor involved two-thirds of the circumferential surface, and covered the area above and below the peritoneal reflection, and extended to the anal margin ( Fig. 1 ). The entire lesion was soft, and magnifying chromoendoscopy using crystal violet staining identified type IV and V irregular low-pit patterns; thus, we diagnosed the lesion as adenoma or intramucosal adenocarcinoma. Computed tomography (CT) showed no lymph node or distant metastasis, and ESD was performed.
Fig. 1.
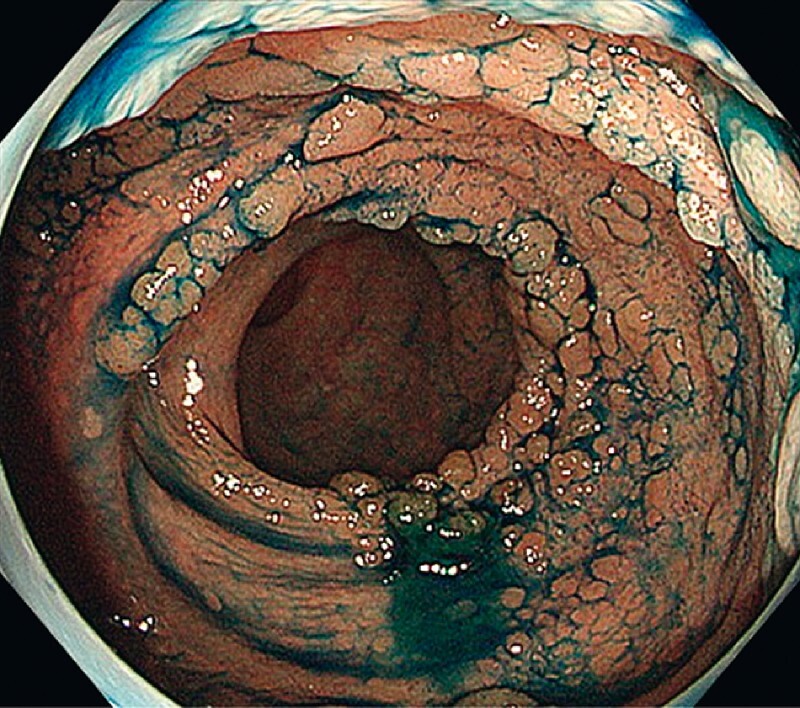
Endoscopic findings of two-thirds of the circumferential flat-elevated type of rectal tumor. The tumor resembled a collection of small lesions, and the boundaries of some lesions were unclear.
The lesion was difficult to dissect because of the high degree of fibrosis. However, when approximately 90 % of the dissection was completed, a large, approximately 40 mm, perforation was identified ( Fig. 2 ). The lesion was excised as quickly as possible, and the purse-string suture method was used to close the perforation ( Fig. 3 ). PGA sheets were used to fill the gap, and fibrin glue was sprayed ( Video 1 ). CT, obtained immediately after the procedure, showed fluid retention, increased lipid density around the rectum, and retroperitoneal emphysema extending around the right kidney. The patient was managed conservatively, She resumed eating 7 days post ESD and was discharged on Day 11.
Fig. 2.
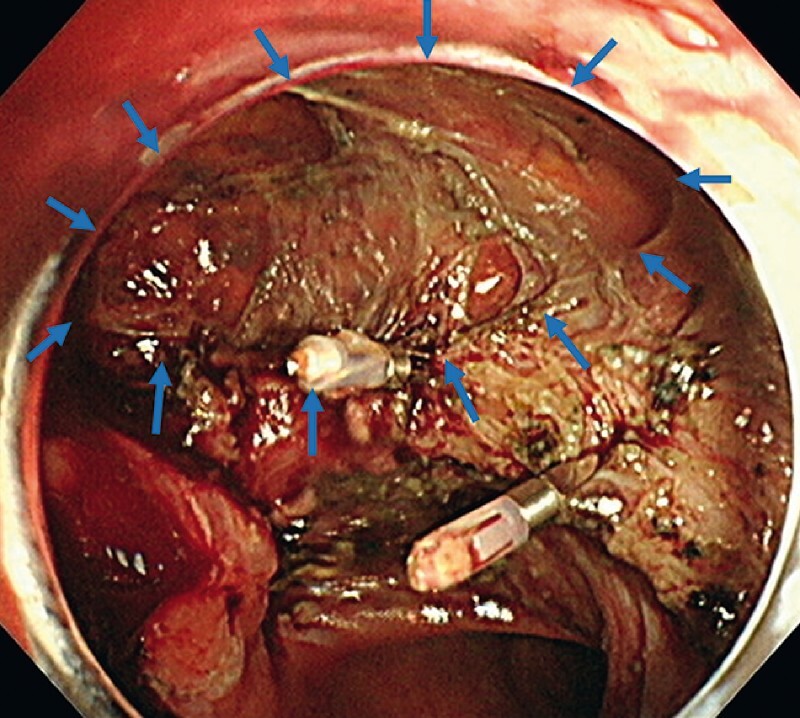
Giant perforation of the lower rectum, measuring 40 mm in size, located below the peritoneal reflection (areas marked with blue arrows). The serosa and retroperitoneal cavity were visible at the perforation site.
Fig. 3.
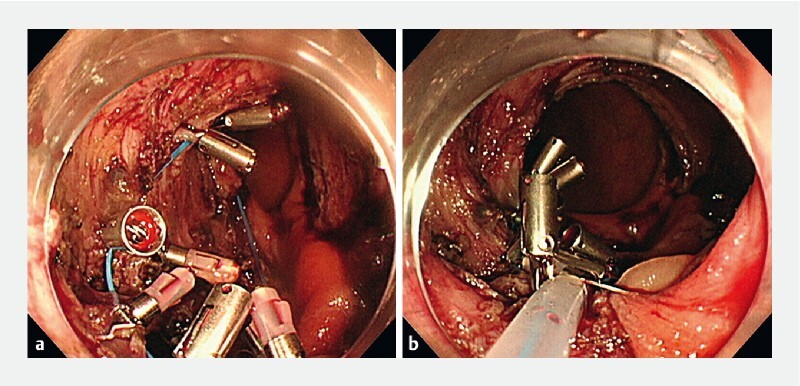
Endoscopy images. a The detachable snare was spread around the perforation and fixed to the muscle layer or mucosa with clips. b By tightening the fixed detachable snare, the purse-string suture method was used to close the perforation. Polyglycolic acid sheets filled the gap, and fibrin glue was sprayed.
Video 1 Management of intraoperative giant perforation of colorectal endoscopic submucosal dissection.
Although colonoscopy performed 8 weeks after discharge showed mild postoperative stenosis, partial obstruction was not observed, and no local recurrence occurred ( Fig. 4 ). The resected specimen was 80 × 66 mm in size and contained a 78 × 64 mm tumor. Histopathological analysis revealed high-grade tubular adenoma.
Fig. 4.
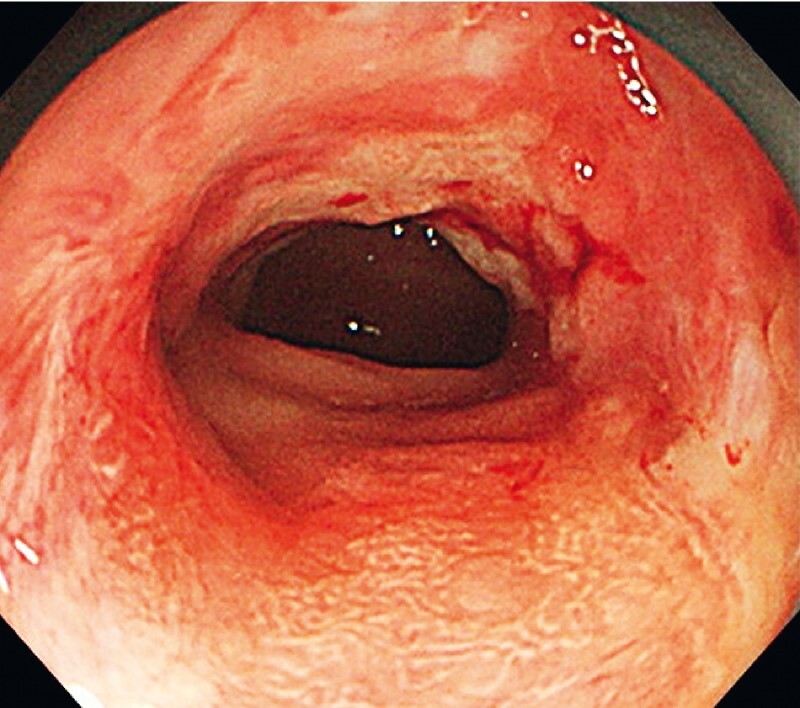
Colonoscopy 8 weeks after endoscopic submucosal dissection showed mild stenosis but no passage obstruction.
Endoscopy_UCTN_Code_CPL_1AJ_2AD
Acknowledgement
We would like to thank Editage ( www.editage.com ) for English language editing.
Footnotes
Competing interests Mitsuhiro Fujishiro has received research grants from Olympus Corporation, Fujifilm Corporation, and HOYA Pentax Corporation, and honoraria from Olympus Corporation and Fujifilm Corporation. Yosuke Tsuji has received research grants from Olympus Corporation, GUNZE and HOYA Pentax Corporation. The remaining authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Tsuji Y, Ohata K, Gunji T et al. Endoscopic tissue shielding method with polyglycolic acid sheets and fibrin glue to cover wounds after colorectal endoscopic submucosal dissection (with video) Gastrointest Endosc. 2014;79:151–155. doi: 10.1016/j.gie.2013.08.041. [DOI] [PubMed] [Google Scholar]
- 2.Sakaguchi Y, Tsuji Y, Yamamichi N et al. Successful closure of a large perforation during colorectal endoscopic submucosal dissection by application of polyglycolic acid sheets and fibrin glue. Gastrointest Endosc. 2016;84:374–375. doi: 10.1016/j.gie.2016.03.787. [DOI] [PubMed] [Google Scholar]
- 3.Takimoto K, Matsuura N, Nakano Y et al. Efficacy of polyglycolic acid sheeting with fibrin glue for perforations related to gastrointestinal endoscopic procedures: a multicenter retrospective cohort study. Surg Endosc. 2022;36:5084–5093. doi: 10.1007/s00464-021-08873-5. [DOI] [PubMed] [Google Scholar]