

Cholangioenteric Roux-en-Y anastomosis is a classic surgical approach for bile duct reconstruction. The common postoperative complications include anastomotic leakage and stenosis, cholangitis, and recurrent stone formation 1 . However, the occlusion of the manually created side-to-side anastomosis between the proximal jejunum and the jejunum at a distance of 40 cm from the cholangioenteric anastomosis is rare 2 .
A 77-year-old woman was admitted for intermittent upper abdominal pain with hypoalbuminemia and severe electrolyte disturbance. The patient had undergone radical resection of cholangiocarcinoma and cholangioenteric Roux-en-Y anastomosis 2 weeks previously ( Fig. 1 ). Abdominal computed tomography (CT) after admission revealed dilation of upper gastrointestinal tract ( Fig. 2 , Fig. 3 ). All possible treatments were administered, but her general condition worsened. Digital subtraction angiography (DSA) showed an increased frequency of intestinal peristalsis, and the contrast agent could not pass through the jejunal side-to-side anastomosis. DSA-guided placement of the enteral feeding tube failed. Based on the patient's age and physical condition, a laparoscopic exploration was urgently performed.
Fig. 1.
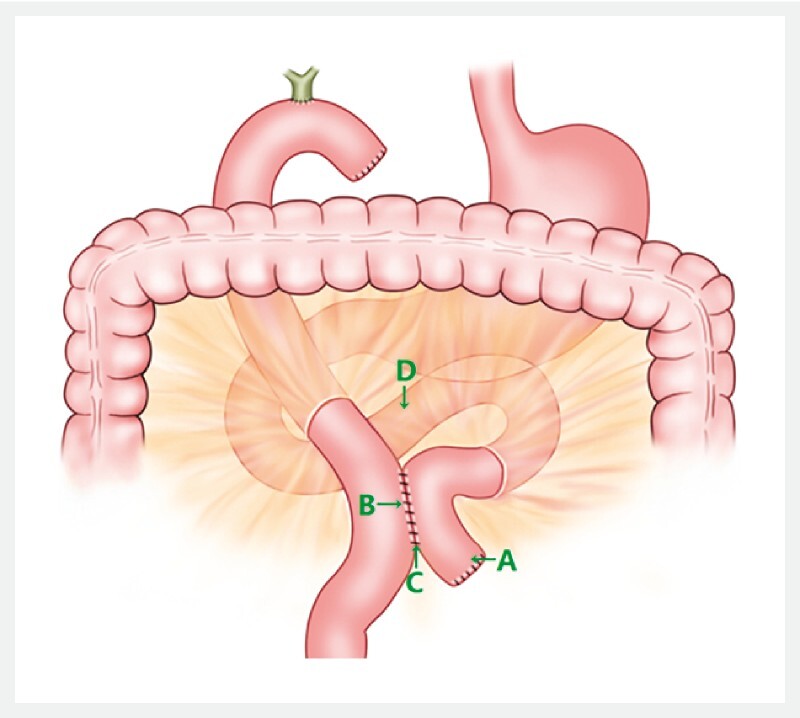
Cholangioenteric Roux-en-Y anastomosis. Proximal jejunal blind loop (A), jejunal side-to-side anastomosis (B), single suture (C), mesocolon (D). Source: Hohhot First Hospital.
Fig. 2.
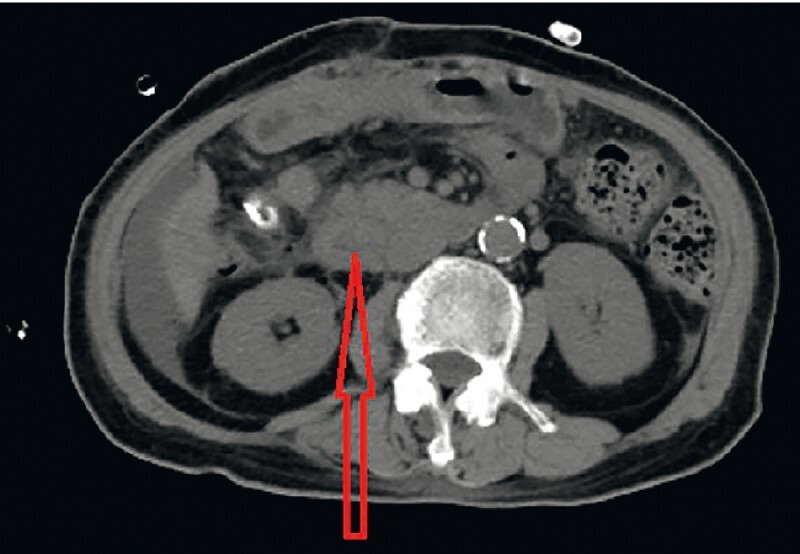
The upper gastrointestinal tract was not dilated after the first operation (the red arrow indicates the descending segment of the duodenum).
Fig. 3.
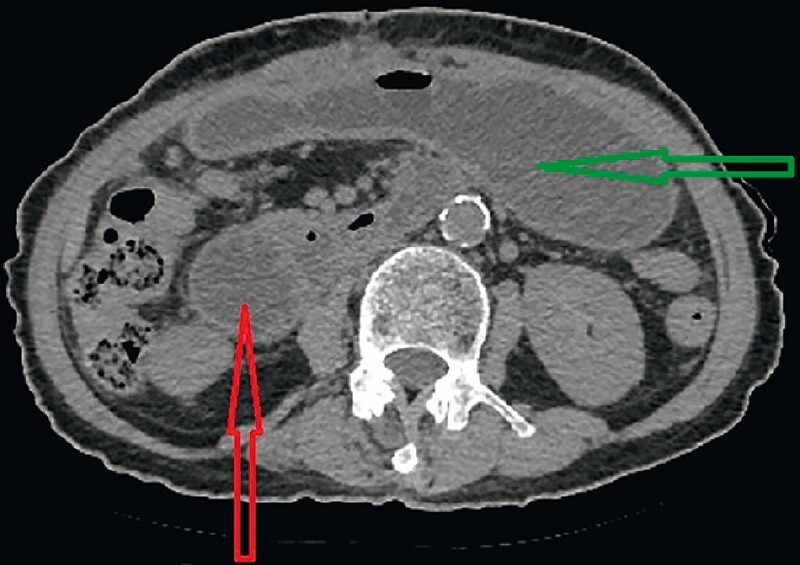
The upper gastrointestinal tract was notably dilated on admission (the red arrow indicates the descending segment of the duodenum; the green arrow indicates the stomach).
During the operation, it was found that the blind loop ( Fig. 1 , A) was adhered to the mesocolon, along with anastomotic angulation, which may have been the main cause of the rare anastomotic occlusion. In addition, the suture at the anastomosis was completely loosened and detached ( Video 1 ). However, whether the complete detachment of the anastomotic suture was involved in the occlusion or was just an isolated event remains unclear.
Video 1 Occlusion of the jejunum side-to-side anastomosis: causes and management.
There are a variety of treatment methods for anastomotic occlusion, and an endoscopic technique should be one of the important options 3 . Our case had poor anastomosis healing that was found during the operation ( Video 1 ). If endoscopic balloon dilation was used, it might have had more serious or even catastrophic consequences (e. g., intestinal fistula). Fortunately, our patient underwent laparoscopic surgery, which proved to be proper and feasible.
Endoscopy_UCTN_Code_CPL_1AK_2AI
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Lye T JY, Eng A KH. Late stricture from marginal ulceration after Roux-en-Y gastric bypass: endoscopic complications and surgical management. Obes Surg. 2021;31:5508–5509. doi: 10.1007/s11695-021-05716-z. [DOI] [PubMed] [Google Scholar]
- 2.Homma T, Yamamoto K, Tsuchiya T et al. A case of severe hepatolithiasis after hepaticojejunostomy with Roux-en-Y reconstruction treated by endoscopic ultrasound-guided transhepatic antegrade stone removal. Endoscopy. 2021;53:E230–E231. doi: 10.1055/a-1244-9556. [DOI] [PubMed] [Google Scholar]
- 3.Inoue T, Shichijo S, Yasui M et al. Endoscopic incision and balloon dilation using the rendezvous technique for complete anastomotic obstruction after rectal low-anterior resection. Endoscopy. 2022;54:E90–E91. doi: 10.1055/a-1393-5165. [DOI] [PubMed] [Google Scholar]