

Abstract
BACKGROUND
Many persons with a history of smoking tobacco have clinically significant respiratory symptoms despite an absence of airflow obstruction as assessed by spirometry. They are often treated with medications for chronic obstructive pulmonary disease (COPD), but supporting evidence for this treatment is lacking.
METHODS
We randomly assigned persons who had a tobacco-smoking history of at least 10 pack-years, respiratory symptoms as defined by a COPD Assessment Test score of at least 10 (scores range from 0 to 40, with higher scores indicating worse symptoms), and preserved lung function on spirometry (ratio of forced expiratory volume in 1 second [FEV1] to forced vital capacity [FVC] ≥0.70 and FVC ≥70% of the predicted value after bronchodilator use) to receive either indacaterol (27.5 μg) plus glycopyrrolate (15.6 μg) or placebo twice daily for 12 weeks. The primary outcome was at least a 4-point decrease (i.e., improvement) in the St. George’s Respiratory Questionnaire (SGRQ) score (scores range from 0 to 100, with higher scores indicating worse health status) after 12 weeks without treatment failure (defined as an increase in lower respiratory symptoms treated with a long-acting inhaled bronchodilator, glucocorticoid, or antibiotic agent).
RESULTS
A total of 535 participants underwent randomization. In the modified intention-to-treat population (471 participants), 128 of 227 participants (56.4%) in the treatment group and 144 of 244 (59.0%) in the placebo group had at least a 4-point decrease in the SGRQ score (difference, −2.6 percentage points; 95% confidence interval [CI], −11.6 to 6.3; adjusted odds ratio, 0.91; 95% CI, 0.60 to 1.37; P=0.65). The mean change in the percent of predicted FEV1 was 2.48 percentage points (95% CI, 1.49 to 3.47) in the treatment group and −0.09 percentage points (95% CI, −1.06 to 0.89) in the placebo group, and the mean change in the inspiratory capacity was 0.12 liters (95% CI, 0.07 to 0.18) in the treatment group and 0.02 liters (95% CI, −0.03 to 0.08) in the placebo group. Four serious adverse events occurred in the treatment group, and 11 occurred in the placebo group; none were deemed potentially related to the treatment or placebo.
CONCLUSIONS
Inhaled dual bronchodilator therapy did not decrease respiratory symptoms in symptomatic, tobacco-exposed persons with preserved lung function as assessed by spirometry. (Funded by the National Heart, Lung, and Blood Institute and others; RETHINC ClinicalTrials.gov number, NCT02867761.)
Chronic obstructive pulmonary disease (COPD) is defined by a reduced ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) after bronchodilator use.1 However, we previously found that some tobacco-exposed persons who have preserved lung function as assessed by spirometry report having substantial respiratory symptoms, activity limitation, and exacerbations, similar to those in persons with airflow obstruction measured on spirometry.2 These tobacco-exposed persons with preserved lung function on spirometry who have respiratory symptoms as defined by a COPD Assessment Test (CAT) score of 10 or greater (scores range from 0 to 40, with higher scores indicating worse symptoms) also have airway-wall thickening and higher sputum mucin concentrations than nonsymptomatic persons.3 In the COPDGene cohort, a significant percentage of tobacco-exposed persons with preserved lung function on spirometry were noted to have respiratory impairments and abnormalities on computed tomography (CT), such as emphysema and air trapping.4 In the CanCOLD cohort, exacerbations among tobacco-exposed persons with preserved lung function on spirometry were associated with missed social activities, missed work for income, and an inability to do housework, which suggests that they constitute a real-life clinical burden.5
Many symptomatic tobacco-exposed persons with preserved lung function on spirometry are treated with COPD medications, including inhaled bronchodilators and glucocorticoids.2 Because spirometry is infrequently performed in primary care,6,7 it is unclear whether physicians believe they are treating COPD or whether they believe COPD medications are effective for these patients. Regardless, randomized trials to guide treatment in this patient population are lacking.
In response to this evidence gap, we hypothesized that persons who currently or formerly smoked cigarettes with at least a 10 pack-year history and who have clinically significant respiratory symptoms despite also having preserved lung function on spirometry (i.e., FEV1:FVC ≥0.70 and FVC ≥70% of the predicted value) would benefit from treatment with inhaled bronchodilators. We tested this hypothesis in a randomized trial using an inhaled dual bronchodilator (combined long-acting β2-agonist [LABA] and long-acting muscarinic antagonist [LAMA]). Because dual bronchodilators yield greater improvements in lung function and abatement of symptoms than a single bronchodilator,8,9 we used a dual bronchodilator to provide a rigorous test of whether bronchodilation benefits this patient population.
METHODS
TRIAL OVERSIGHT
We conducted the Redefining Therapy in Early COPD (RETHINC) trial as an investigator-initiated, multicenter, blinded, randomized, controlled trial within the National Heart, Lung, and Blood Institute (NHLBI)–funded Pulmonary Trials Cooperative10 based on evidence generated from Subpopulations and Intermediate Outcome Measures in COPD Study (SPIROMICS).2 The trial was designed by the authors. The University of Pittsburgh Network Management Core and the leadership committee of the Pulmonary Trials Cooperative contributed to the writing of the protocol, operations, and site management. The 20 enrolling centers included academic, Veterans Affairs, and community medical centers. The NHLBI organized the data and safety monitoring board, and Novartis Pharmaceuticals donated masked trial medication and placebo. Industry funders were not involved in the design or conduct of the trial, the collection or analysis of the data, the writing of the manuscript, or the decision to submit the report for publication. The protocol was approved by the institutional review boards at the University of Michigan and each participating center. The authors vouch for the accuracy and completeness of the data and for the fidelity of the trial to the protocol, available with the full text of this article at NEJM.org.
PARTICIPANTS
We enrolled persons 40 to 80 years of age who currently or formerly smoked cigarettes with at least a 10 pack-year history, had respiratory symptoms as defined by a CAT score of 10 or higher, and had an FEV1:FVC of at least 0.70 and a FVC that was at least 70% of the predicted value after bronchodilator use. We excluded persons who had a primary diagnosis of asthma based on criteria from National Institute for Health and Care Excellence guidelines,11 those with other known concomitant lung disease, and those already using a maintenance inhaled LAMA, LABA, fixed combination of LABA with an inhaled glucocorticoid, a short-acting anticholinergic agent, or fixed combination of a short-acting β2-agonist (SABA) and short-acting anticholinergic, unless the potential participant was able to undergo a 30-day medication washout. SABAs were allowed as needed during the trial, without specific instructions given regarding their use. A complete list of the inclusion and exclusion criteria is provided in the protocol. Recruitment methods included advertising in clinics, community venues, and social media. Some participants also participated in the SPIROMICS and COPDGene observational studies. All participants provided written informed consent.
TRIAL PROCEDURES
We used permuted block randomization with varying block sizes of 2, 4, and 6, stratified according to center, smoking status (current or former), and whether a medication washout was warranted. We randomly assigned participants in a 1:1 ratio to receive indacaterol (27.5 μg) plus glycopyrrolate (15.6 μg) or placebo twice daily for 12 weeks; these doses of indacaterol and glycopyrrolate are the Food and Drug Administration (FDA)–approved doses for the treatment of COPD in the United States, although they are lower than the doses approved elsewhere (110 μg of indacaterol and 50 μg of glycopyrrolate in Canada and 85 μg and 43 μg, respectively, in Europe). We planned to enroll 290 participants in each group. We administered the St. George’s Respiratory Questionnaire (SGRQ), CAT, and Baseline Dyspnea Index (BDI) at baseline and the Transition Dyspnea Index (TDI) at follow-up; performed spirometry (with Hankinson reference equations12) at baseline and 12 weeks; and followed up by telephone at 4 weeks to assess adverse events. SGRQ scores range from 0 to 100, with higher scores indicating worse health status; the minimum clinically important difference is 4 points. The minimum clinically important difference for the CAT score is 2 points. BDI scores range from 0 to 12, with higher scores indicating greater dyspnea at baseline. TDI scores are a measure of the change in dyspnea severity from the baseline value established by the BDI score; scores range from −9 to 9, with higher scores indicating greater decreases in dyspnea severity; the minimum clinically important difference is 1 point.
OUTCOMES
The primary outcome was a decrease (i.e., improvement) by more than 4 points in the SGRQ score after 12 weeks without treatment failure.13 We defined treatment failure as an increase in lower respiratory symptoms leading to treatment with a long-acting bronchodilator, glucocorticoid, or antibiotic agent. Important prespecified secondary outcomes included a decrease by at least 2 points in the CAT score,14 a TDI score of at least 1,15 and a decrease by at least 4 points in the SGRQ score plus a TDI score of at least 1, all without treatment failure; the mean changes from baseline in the SGRQ and CAT scores; the TDI score; the change from baseline in predose FEV1 and inspiratory capacity measured 12 hours after receipt of treatment or placebo; the FEV1 assessed hourly over the first 3 hours after a dose of treatment or placebo (expressed as the area under the curve [AUC0–3hr]) at 12 weeks; treatment failure itself (as defined above); and the percentage of days with symptoms or use of rescue medication determined on the basis of information recorded by participants in a daily diary. Because of the coronavirus disease 2019 (Covid-19) pandemic, we evaluated the primary outcome by telephone in 20 participants in the treatment group and 22 in the placebo group. SGRQ administration by telephone has been shown to have good comparability to in-person administration.16
STATISTICAL ANALYSIS
We designed the trial to enroll 580 participants, which would provide 90% power to detect a 14-percentage-point difference in the percentage of participants meeting the primary outcome, accounting for 10% attrition (two-sided chi-square test), on the basis of data from the Novartis FDA development program studies.17 Because of the pandemic and time limits associated with funding and drug supply, the trial was ended with 535 participants having undergone randomization, with an estimated 87% power accounting for 10% attrition.
Disruption of our ability to conduct in-person trial visits during the Covid-19 pandemic led to missing or very delayed (>16 weeks after randomization) primary outcome data for 10 participants. Dropouts due to treatment failure were considered to be informative and contributed to the composite primary outcome. We considered other missing data to be missing completely at random. To handle this, we excluded participants who had neither treatment failure nor week 12 data for the primary outcome from the intention-to-treat population, yielding a modified intention-to-treat population for our primary analysis.
In addition, we performed four sensitivity analyses: one in which we reassigned 12 participants who were determined to have received the incorrect drug kit (i.e., not the one that had been randomly assigned), one in which we excluded 11 participants who had an FEV1:FVC of less than 0.70, one in which we limited our analyses to participants who completed the trial before the start of the Covid-19 pandemic, and one in which we included the 10 participants who were excluded from the modified intention-to-treat population because they had the primary outcome measured more 16 weeks after randomization. Finally, we analyzed a per-protocol population that excluded participants who had a protocol deviation or had unknown or incorrect adherence (defined as having taken <80% or >120% of protocol-specified doses).
The primary analysis was conducted by the University of Michigan Statistical Analysis of Biomedical and Educational Research (SABER) Group. Primary and secondary analyses with binary outcomes were conducted with the use of generalized-estimating-equation regression with logit link, with adjustment for clinical center of recruitment, baseline smoking status, previous maintenance treatment warranting washout, body-mass index (BMI, the weight in kilograms divided by the square of the height in meters), and the baseline value of the outcome being evaluated. For continuous outcomes, we used linear mixed-effects models with adjustment for the same covariates. No interim statistical analysis of efficacy was conducted.
Prespecified subgroup analyses of the primary outcome were based on participant-reported baseline smoking status, baseline bronchodilator responsiveness,18,19 and BMI (>30 or ≤30). Additional exploratory subgroup analyses included subgroups defined according to sex, age (<65 years or ≥65 years), baseline percent of predicted FEV1 (either less than the median or greater than or equal to the median for all participants who underwent randomization), baseline inspiratory capacity (either less than the median or greater than or equal to the median for all participants who underwent randomization), and status with respect to chronic bronchitis according to the Medical Research Council (MRC) definition (cough and sputum on most days during at least 3 consecutive months for more than 2 successive years).20 We tested interactions between each of these subgroups and treatment. For secondary analyses, we provide 95% confidence intervals that have not been adjusted for multiplicity and are excluded from formal hypothesis testing.
RESULTS
CHARACTERISTICS OF THE PARTICIPANTS
From July 2017 through March 2021, a total of 535 participants at 20 centers underwent randomization; 261 were assigned to receive active treatment and 274 to receive placebo (Fig. 1). Overall, 28% of participants were already using some type of inhaled COPD medication (SABA, short-acting muscarinic agonist [SAMA], LABA, LAMA, or inhaled glucocorticoid). Of the 32 potential participants who were screened but were already using long-acting bronchodilators and at least began washout, 20 underwent randomization, 5 were ultimately deemed ineligible, 2 were lost to follow-up, 2 were unable to undergo randomization because of the pandemic, and only 3 were not able to complete the washout. Overall, 4% of participants were enrolled after a washout of a maintenance COPD medication. After the exclusion of participants who did not complete the trial (53), had a missing SGRQ score (1), or had a very delayed final assessment because of the pandemic (10), a total of 471 participants were included in the modified intention-to-treat analysis. Participants who were excluded from the modified intention-to-treat analysis were slightly younger and more likely to be currently smoking tobacco and had slightly higher oxygen saturation than those who were included (Table S1 in the Supplementary Appendix, available at NEJM.org). Further excluding the 125 participants who had a major protocol deviation (defined as eligibility criteria violations for which no exemption was granted, nonadherence to treatment or placebo, or receipt of a prohibited medication) yielded 346 participants for the per-protocol analysis.
Figure 1. Enrollment, Randomization, and Follow-up.
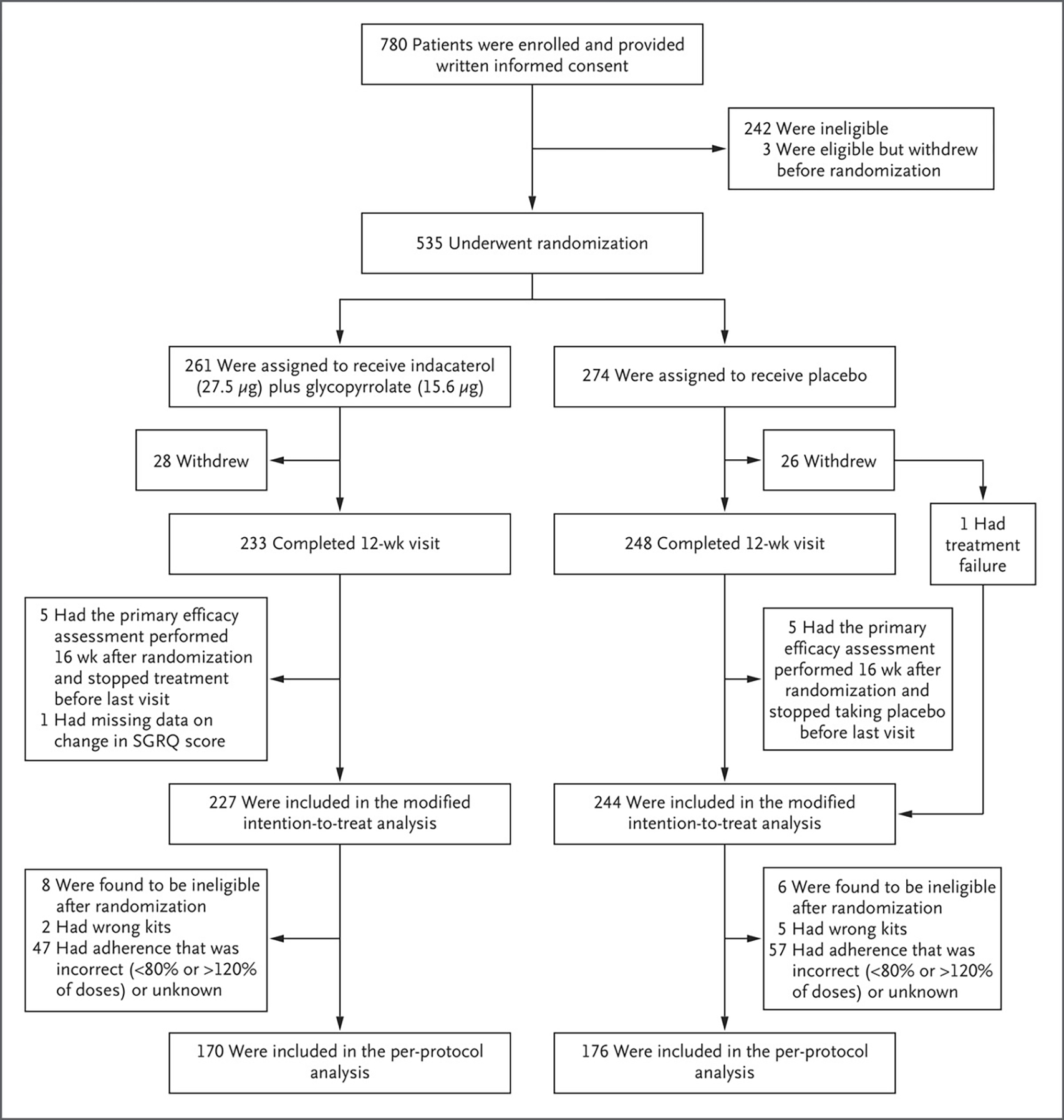
Participants were randomly assigned to receive indacaterol (27.5 μg) plus glycopyrrolate (15.6 μg) or placebo twice daily for 12 weeks. The modified intention-to-treat population excluded participants who had neither treatment failure nor week 12 data for the primary outcome. The per-protocol population excluded participants who had a protocol deviation or incorrect or unknown adherence. SGRQ denotes St. George’s Respiratory Questionnaire.
The baseline characteristics of the participants in the two groups were balanced in the intention-to-treat population (Table 1 and Table S2). Approximately half the trial population identified as female, 56.4% as White, and 35.7% as Black; 64.1% of the participants were currently smoking. The most common coexisting condition was diabetes (16.7%). Chronic bronchitis based on the MRC definition was present in 36.5% of the participants,20 although the percentage was higher when alternative definitions of chronic bronchitis based on the SGRQ and CAT were used.21,22 Baseline characteristics in the modified intention-to-treat population were also well balanced (Table S3); the balance between numbers of male and female participants was similar to that in the population in SPIROMICS, an observational study involving persons with a history of smoking. The prevalence of Black participants was higher and the prevalence of Hispanic or Latino participants lower than that observed in the 2020 U.S. Census; current epidemiologic data on this patient population are insufficient to determine whether these differences are expected (Table S4).
Table 1.
Demographic and Clinical Characteristics of the Participants at Baseline.*
| Characteristic | Treatment (N = 261) | Placebo (N = 274) | Overall (N = 535) |
|---|---|---|---|
| Age — yr | 58.6±9.6 | 59.1±9.8 | 58.8±9.7 |
| Male sex — no. (%) | 127 (48.7) | 133 (48.5) | 260 (48.6) |
| Race — no. (%)† | |||
| Black | 92 (35.2) | 99 (36.1) | 191 (35.7) |
| White | 148 (56.7) | 154 (56.2) | 302 (56.4) |
| Other | 3 (11) | 4 (15) | 7 (13) |
| More than one race or missing race | 18 (6.9) | 17 (6.2) | 35 (6.5) |
| Hispanic or Latino ethnic group — no. (%)† | 25 (9.6) | 22 (8.0) | 47 (8.8) |
| Current smoking — no. (%) | 169 (64.8) | 174 (63.5) | 343 (64.1) |
| Use of prohibited medication warranting washout — no. (%)‡ | 9 (3.4) | 11 (4.0) | 20 (3.7) |
| Body-mass index | 29.5±4.9 | 29.4±5.3 | 29.5±5.1 |
| Medical history — no./total no. (%) | |||
| Coronary artery disease | 12/252 (4.8) | 11/264 (4.2) | 23/516 (4.5) |
| Congestive heart failure | 1/252 (0.4) | 5/264 (1.9) | 6/516 (1.2) |
| Chronic bronchitis§ | |||
| MRC definition | 87/251 (34.7) | 101/264 (38.3) | 188/515 (36.5) |
| SGRQ definition | 141/261 (54) | 145/273 (53.1) | 286/534 (53.6) |
| CAT definition | 183/261 (70.1) | 193/274 (70.4) | 376/535 (70.3) |
| CAT score¶ | 17.5±6.7 | 17.6±6.0 | 17.6±6.4 |
| SGRQ score‖ | 37.9±21.0 | 38.4±19.3 | 38.2±20.2 |
| BDI score** | 7.7±2.0 | 7.5±2.0 | 7.6±2.0 |
| Postbronchodilator FEV1 — % of predicted value | 93.8±14.0 | 94.9±12.6 | 94.4±13.3 |
| Postbronchodilator FVC — % of predicted value | 92.9±12.8 | 94.2±13.3 | 93.6±13.0 |
| Postbronchodilator FEV1:FVC | 0.78±0.05 | 0.78±0.05 | 0.78±0.05 |
| Bronchodilator responsiveness — no. (%)†† | 30 (11.5) | 32 (11.7) | 62 (11.6) |
Plus–minus values are means ±SD. FEV1 denotes forced expiratory volume in 1 second, and FVC forced vital capacity.
Race and ethnic group were reported by the participants. The category “other” included American Indian, Alaska Native, Asian, Native Hawaiian, and other Pacific Islander.
Prohibited medications warranting washout included a long-acting β2-agonist (LABA), long-acting muscarinic agonist, a fixed combination of a LABA with an inhaled glucocorticoid, a short-acting anticholinergic agent, or a fixed combination of a short-acting β2-agonist and short-acting anticholinergic.
The Medical Research Council (MRC) definition of chronic bronchitis is cough and sputum on most days during at least 3 consecutive months for more than 2 successive years. The St. George’s Respiratory Questionnaire (SGRQ) definition is the selection of the option “cough for most days a week” or “several days a week” for the cough question on that questionnaire and the options indicating production of phlegm, sputum, or both on “most days a week” or “several days a week” for the sputum question. The COPD Assessment Test (CAT) definition is a score of 2 or higher for the cough question on that test (anchored question ranging from “I never cough” to “I cough all the time” on a scale of 0 to 5) and a score of 2 or higher for the phlegm-production question (anchored question ranging from “I have no phlegm in my chest at all” to “My chest is full of phlegm” on a scale of 0 to 5).
Scores on the CAT range from 0 to 40, with higher scores indicating worse symptoms.
Scores on the SGRQ range from 0 to 100, with higher scores indicating worse health status.
Scores on the Baseline Dyspnea Index (BDI) range from 0 to 12, with higher scores indicating greater dyspnea at baseline.
Bronchodilator responsiveness was defined as an increase in either FEV1 or FVC by at least 12% and at least 200 ml after bronchodilator use, in accordance with the American Thoracic Society and European Respiratory Society definition.
FOLLOW-UP AND OUTCOMES
In our primary analysis involving the modified intention-to-treat population, we found no observable treatment effect; 128 of 227 participants (56.4%) in the treatment group and 144 of 244 participants (59.0%) in the placebo group had at least a 4-point decrease (improvement) in the SGRQ score without treatment failure (difference, −2.6 percentage points; 95% confidence interval [CI], −11.6 to 6.3; adjusted odds ratio, 0.91; 95% CI, 0.60 to 1.37; P=0.65). No significant treatment effect was found in any of our sensitivity analyses (Fig. 2). The results were similar in the per-protocol analysis, with 101 of 170 participants (59.4%) in the treatment group and 110 of 176 (62.5%) in the placebo group having at least a 4-point decrease in the SGRQ score without treatment failure (odds ratio, 0.88; 95% CI, 0.65 to 1.20) (Fig. 2). Treatment failure was uncommon, occurring in only 5 participants (2.2%) in the treatment group and 9 (3.7%) in the placebo group. Data on prespecified secondary analyses are provided in Figures 2 and 3 and Table 2. The results of prespecified subgroup analyses of the primary outcome are shown in Figure 2.
Figure 2. Primary and Secondary Binary Outcomes.

(facing page). The primary outcome was at least a 4-point decrease (i.e., improvement) in the SGRQ score after 12 weeks without treatment failure (defined as an increase in lower respiratory symptoms leading to treatment with a long-acting bronchodilator, glucocorticoid, or antibiotic agent). All odds ratios were based on generalized-estimating-equation models with adjustment for clinical center of recruitment, baseline smoking status, previous maintenance treatment for chronic obstructive pulmonary disease (COPD) warranting a washout period, body-mass index at baseline, and the baseline value of the outcome being evaluated. In sensitivity analysis 1, we reassigned 12 participants in the modified intention-to-treat analysis who had been incorrectly given treatment or placebo at randomization. In sensitivity analysis 2, we excluded 11 participants from the modified intention-to-treat population who actually had a ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) of less than 0.70 (meeting the definition of COPD). In sensitivity analysis 3, we excluded 56 participants from the modified intention-to-treat population who were enrolled after the start of the coronavirus disease 2019 (Covid-19) pandemic (March 30, 2020). In sensitivity analysis 4, we included 10 participants who had been excluded from the modified intention-to-treat population because they had the primary outcome measured more than 16 weeks after randomization. In the analysis shown, bronchodilator responsiveness was defined as an increase in either FEV1 or FVC by at least 12% and at least 200 ml after bronchodilator use, in accordance with the American Thoracic Society and European Respiratory Society definition. SGRQ scores range from 0 to 100, with higher scores indicating worse health status. COPD Assessment Test (CAT) scores range from 0 to 40, with higher scores indicating worse symptoms. The Transition Dyspnea Index (TDI) score is a measure of the change in dyspnea severity from the baseline value established by the Baseline Dyspnea Index score; TDI scores range from −9 to 9, with higher scores indicating greater decreases in dyspnea severity. For all secondary and exploratory analyses, 95% confidence intervals have not been adjusted for multiplicity and therefore cannot be used in place of hypothesis tests.
Figure 3. Lung Function and Symptom Scores.
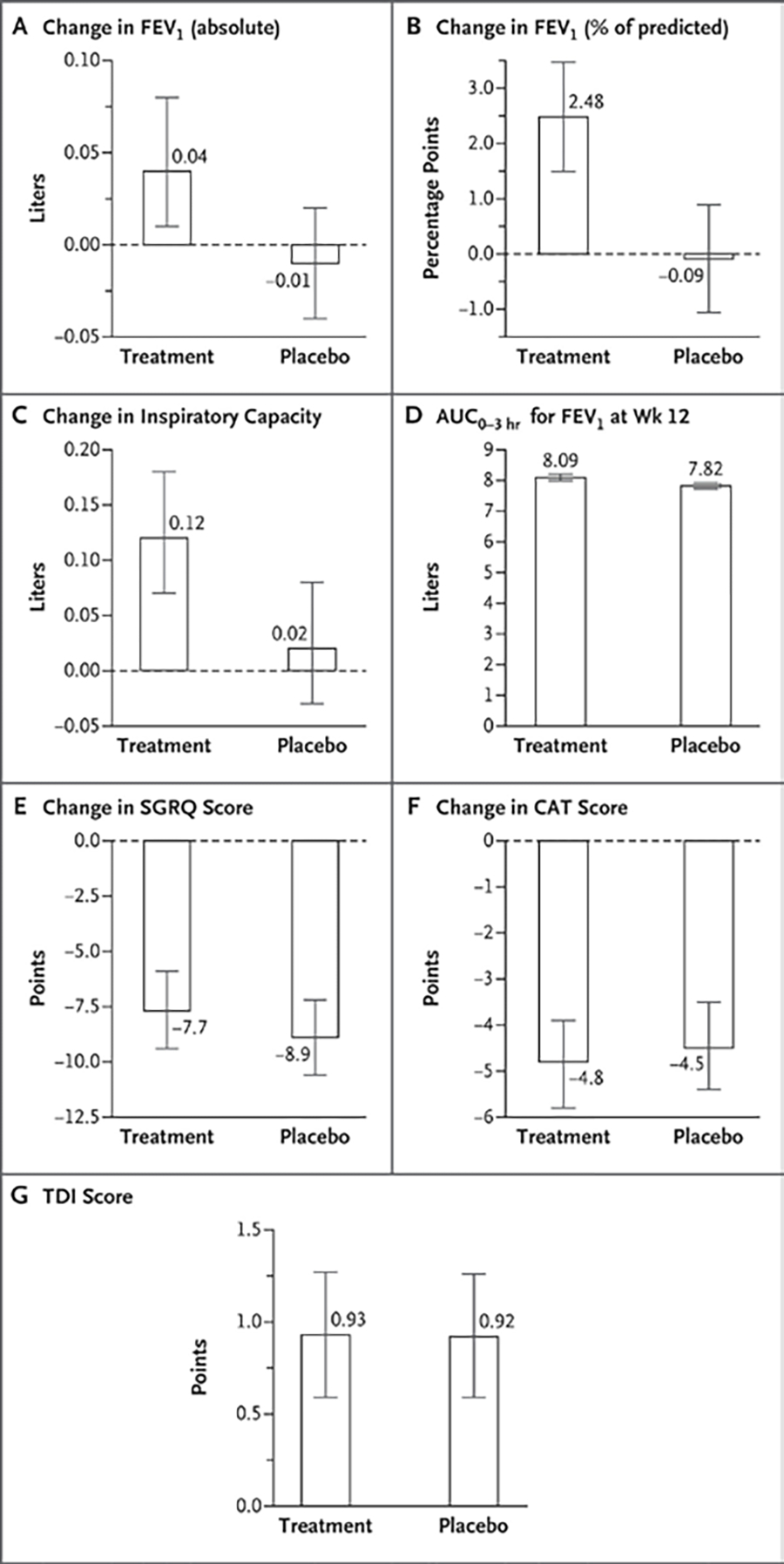
Changes in lung-function measures were assessed as baseline prebronchodilator values as compared with those obtained 12 hours after the final dose of trial medication or placebo at 12 weeks. Heights of bars indicate the mean, and I bars indicate the 95% confidence interval based on linear mixed-effects model estimates. All changes were from baseline to the week 12 visit. AUC0–3hr is the area under the curve, assessed hourly over the first 3 hours after a dose. For all analyses shown here, 95% confidence intervals have not been adjusted for multiplicity and therefore cannot be used in place of hypothesis tests.
Table 2.
Efficacy Results for Continuous Outcomes.*
| Outcome | Treatment (N = 227) | Placebo (N = 244) |
|---|---|---|
| Mean (95% CI) | ||
| Change in questionnaire results from baseline to week 12 | ||
| SGRQ score | −7.7 (−9.4 to −5.9) | −8.9 (−10.6 to −7.2) |
| CAT score | −4.8 (−5.8 to −3.9) | −4.5 (−5.4 to −3.5) |
| TDI score† | 0.93 (0.59 to 1.27) | 0.92 (0.59 to 1.26) |
| Change in pulmonary function from baseline to week 12 | ||
| Inspiratory capacity — liters | 0.12 (0.07 to 0.18) | 0.02 (−0.03 to 0.08) |
| FEV1 — liters | 0.04 (0.01 to 0.08) | −0.01 (−0.04 to 0.02) |
| Percent of predicted FEV1 — percentage points | 2.48 (1.49 to 3.47) | −0.09 (−1.06 to 0.89) |
| FEF25–75 — liters/sec | 0.07 (0.00 to 0.15) | −0.08 (−0.15 to 0.00) |
| AUC0–3hr for FEV1 at week 12 — liters | 8.09 (7.99 to 8.20) | 7.82 (7.72 to 7.92) |
| Outcomes from daily diary — % of days | ||
| Any symptoms or use of albuterol | 67.0 (59.0 to 75.0) | 63.6 (55.7 to 71.5) |
| Shortness of breath | 30.7 (23.6 to 37.7) | 32.5 (25.6 to 39.4) |
| Chest tightness | 21.2 (15.0 to 27.4) | 23.5 (17.4 to 29.6) |
| Wheezing | 23.5 (17.8 to 29.2) | 24.3 (18.7 to 29.8) |
| Cough | 53.1 (45.9 to 60.2) | 48.0 (41.1 to 54.9) |
| Sputum | 45.1 (37.7 to 52.5) | 43.4 (36.1 to 50.6) |
| Use of albuterol | 9.3 (5.0 to 13.6) | 9.7 (5.5 to 14.0) |
Participants received indacaterol (27.5 μg) plus glycopyrrolate (15.6 μg) or placebo twice daily for 12 weeks. Means and 95% confidence intervals are based on linear mixed-effects model estimates with baseline covariates set at the group mean. For all secondary and exploratory analyses, 95% confidence intervals have not been adjusted for multiplicity and therefore cannot be used in place of hypothesis tests. The results shown are for prespecified outcomes. Excluded is the FEV1 12-hour trough value at the final follow-up visit, which, although specified in the protocol, the authors judged to not truly be a “trough” given that the half-life of indacaterol–glycopyrrolate is longer than 12 hours. AUC0–3hr denotes area under the curve during the first 3 hours, and FEF25–75 forced expiratory flow between 25% and 75% of the forced vital capacity.
The TDI score is a measure of the change in dyspnea severity from the baseline value established by the BDI score; scores range from −9 to 9, with higher scores indicating greater decreases in dyspnea severity.
ADHERENCE AND SAFETY
Adherence was high, with 88% of doses taken in both the treatment group and the placebo group. Four serious adverse events occurred in the treatment group (in 4 participants [1.5%]), and 11 occurred in the placebo group (in 8 participants [2.9%]), with no deaths and no events deemed by the investigators to be potentially related to treatment or placebo. The most common nonserious adverse events were cough (3.4% of participants in the treatment group and 4.4% in the placebo group) and headache (3.4% and 4.4%, respectively) (Table S5).
DISCUSSION
We found that dual long-acting bronchodilator treatment did not decrease respiratory symptoms in persons who currently or formerly smoked cigarettes and had substantial respiratory symptoms despite also having preserved lung function as assessed by spirometry. This stands in contrast to data on symptom abatement with dual long-acting bronchodilators in tobacco-exposed persons who meet criteria for COPD.17
In the absence of clinical trial data, physicians have responded to this patient population in the “real world” by prescribing treatments known to work for COPD or asthma. In SPIROMICS, we found that 43% of these patients used bronchodilators: 31% used SABAs, 11% SAMAs, 31% LAMAs, 15% LABAs, and 23% inhaled glucocorticoids.2 In the COPDGene study, 20% of patients with normal lung function on spirometry who had one or more impairments (increased respiratory symptoms, history of severe exacerbation, CT abnormality, or reduced 6-minute walk distance) used respiratory medication.4 This is not surprising. Spirometry is underused in primary care,6,7 and either the diagnosis of COPD is incorrectly assumed without spirometry or, despite a lack of clinical trial data in this population, treatments found to be beneficial in COPD have been extended to this population.
Our results have important implications for clinical practice. Preserved lung function on spirometry (FEV1:FVC ≥0.70) in a person with current or former exposure to smoked tobacco and respiratory symptoms should generally discourage the prescription of bronchodilators for symptom control. This stands in contrast to the use of bronchodilators in patients with diagnoses of bona fide COPD who, on average, do derive symptomatic benefit from this treatment.17 It follows that it is important to distinguish between the two groups of patients, which is often not done in clinical practice, in which the use of spirometry in primary care for COPD has historically been infrequent.6 It is important to note, however, that we did not study inhaled glucocorticoids, azithromycin, or other COPD medications or therapeutics that target pathologic mucus.
Our trial has some limitations. Symptoms in some of our participants may have been driven by factors other than pulmonary abnormalities — for example, cardiac disease or sleep apnea — and a more narrowly defined patient population might have benefited. For instance, the trial may have been underpowered to study the subgroup of participants with chronic bronchitis specifically. Furthermore, we enrolled only a small sample of participants who were taking long-acting bronchodilators before enrollment; it is possible that patients identified by their physicians as needing these medications are a unique subgroup that benefit from treatment. We observed abatement of symptoms in both the treatment group and the placebo group, which suggests a strong placebo effect (improvement directly related to receipt of any type of therapy), a Hawthorne effect (improvement related to being in a clinical trial), or regression to the mean (reduction in symptoms after selection for substantial symptoms). Given that we recruited participants with substantial respiratory symptoms and used a symptom score as our primary outcome, we suspect that regression to the mean contributed to the observed improvements (un derscoring the value of the placebo control). We know that persons with a history of smoking who have symptoms despite having preserved lung function on spirometry are at increased risk for respiratory exacerbations, and our follow-up period was too short to adequately assess the effects of treatment on exacerbations. It is also possible that 12 weeks was not a long enough period to observe symptomatic improvement; however, given the significant improvement in SGRQ score that has been documented at 12 weeks with the use of indacaterol plus glycopyrrolate in two COPD clinical trials,17 we believe this is less likely. Finally, although we used the drug doses that are FDA-approved for COPD in the United States, the higher doses that are approved in other countries might produce different results.
Our trial provides data on the treatment of patients without COPD who have a history of smoking tobacco and who have respiratory symptoms despite having preserved lung function on spirometry. The number of such persons is likely to be substantial. Data from the general population cohort study CanCOLD suggest that 25% of persons with any smoking history and normal lung function on spirometry report substantial dyspnea on exertion.23 Smoking-cessation therapy remains a primary goal for this patient population. However, our data suggest that long-acting bronchodilators do not result in abatement of respiratory symptoms in these patients. Further research is urgently needed to better understand and treat the respiratory disease in these persons.
Supplementary Material
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Minneapolis VA Health Care System. The work here represents the views of the authors and not necessarily the views of the Department of Veterans Affairs or the U.S. government.
Supported by grants from the National Heart, Lung, and Blood Institute (HL128952, HL128954, HL137880, K24HL138188, K24HL137013, and K24HL140108) and the National Center for Advancing Translational Sciences (KL2TR001882) and by Sunovion Pharmaceuticals (financial support to the clinical centers for costs of conducting the trial through the COPD Foundation). Novartis Pharmaceuticals donated the trial medication and placebo.
Footnotes
Contributor Information
M.K. Han, Division of Pulmonary and Critical Care, University of Michigan, Ann Arbor
W. Ye, School of Public Health, University of Michigan, Ann Arbor
D. Wang, School of Public Health, University of Michigan, Ann Arbor
E. White, School of Public Health, University of Michigan, Ann Arbor
M. Arjomandi, Division of Pulmonary, Critical Care, Allergy, and Sleep Medicine, University of California San Francisco San Francisco Veterans Affairs (VA) Healthcare System, San Francisco.
I.Z. Barjaktarevic, Division of Pulmonary and Critical Care Medicine, David Geffen School of Medicine at UCLA, Los Angeles
S.-A. Brown, Division of Pulmonary and Critical Care Medicine, Johns Hopkins School of Medicine, Baltimore
R.G. Buhr, Division of Pulmonary and Critical Care Medicine, David Geffen School of Medicine at UCLA, Los Angeles
A.P. Comellas, Division of Pulmonary, Critical Care, and Occupational Medicine, University of Iowa, Iowa City
C.B. Cooper, Division of Pulmonary and Critical Care Medicine, David Geffen School of Medicine at UCLA, Los Angeles
G.J. Criner, Department of Thoracic Medicine and Surgery, Lewis Katz School of Medicine at Temple University, Philadelphia
M.T. Dransfield, Division of Pulmonary, Allergy, and Critical Care Medicine, Heersink School of Medicine, University of Alabama at Birmingham, Birmingham
F. Drescher, Geisel School of Medicine at Dartmouth and Pulmonary and Critical Care Medicine, VA Medical Center, White River Junction, VT
R.J. Folz, Division of Pulmonary, Critical Care, and Sleep Medicine, Houston Methodist Academic Medicine Associates, Houston
N.N. Hansel, Division of Pulmonary and Critical Care Medicine, Johns Hopkins School of Medicine, Baltimore
R. Kalhan, Division of Pulmonary and Critical Care Medicine, Northwestern University Feinberg School of Medicine, Chicago
R.J. Kaner, Department of Genetic Medicine, Weill Cornell Medicine and New York–Presbyterian Hospital, New York Joan and Sanford I. Weill Department of Medicine, Weill Cornell Medicine and New York–Presbyterian Hospital, New York.
R.E. Kanner, Division of Respiratory, Critical Care, and Occupational Pulmonary Medicine, University of Utah School of Medicine, Salt Lake City, North Carolina
J.A. Krishnan, Breathe Chicago Center, Division of Pulmonary, Critical Care, Sleep, and Allergy, University of Illinois Chicago, Chicago
S.C. Lazarus, Division of Pulmonary, Critical Care, Allergy, and Sleep Medicine, University of California San Francisco Cardiovascular Research Institute, University of California San Francisco.
V. Maddipati, East Carolina University, Greenville, North Carolina
F.J. Martinez, Joan and Sanford I. Weill Department of Medicine, Weill Cornell Medicine and New York–Presbyterian Hospital, New York
A. Mathews, Duke University School of Medicine, Durham, North Carolina
C. Meldrum, Division of Pulmonary and Critical Care, University of Michigan, Ann Arbor
C. McEvoy, HealthPartners Institute, Bloomington, Minnesota
T. Nyunoya, Division of Pulmonary, Allergy, and Critical Care Medicine, University of Pittsburgh, Pittsburgh
L. Rogers, Division of Pulmonary, Critical Care, and Sleep Medicine, Icahn School of Medicine at Mount Sinai, New York
W.W. Stringer, Lundquist Institute for Biomedical Innovation at Harbor–UCLA Medical Center, Los Angeles
C.H. Wendt, Minneapolis VA Healthcare System, Minneapolis, Minnesota
R.A. Wise, Division of Pulmonary and Critical Care Medicine, Johns Hopkins School of Medicine, Baltimore
S.R. Wisniewski, Epidemiology Data Center, University of Pittsburgh, Pittsburgh
F.C. Sciurba, Division of Pulmonary, Allergy, and Critical Care Medicine, University of Pittsburgh, Pittsburgh
P.G. Woodruff, Division of Pulmonary, Critical Care, Allergy, and Sleep Medicine, University of California San Francisco Cardiovascular Research Institute, University of California San Francisco.
Data Availability
A data sharing statement provided by the authors is available with the full text of this article at NEJM.org.
References
- 1.Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med 2017;195:557–82. [DOI] [PubMed] [Google Scholar]
- 2.Woodruff PG, Barr RG, Bleecker E, et al. Clinical significance of symptoms in smokers with preserved pulmonary function. N Engl J Med 2016;374:1811–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kesimer M, Ford AA, Ceppe A, et al. Airway mucin concentration as a marker of chronic bronchitis. N Engl J Med 2017;377:911–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Regan EA, Lynch DA, Curran-Everett D, et al. Clinical and radiologic disease in smokers with normal spirometry. JAMA Intern Med 2015;175:1539–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tan WC, Bourbeau J, Hernandez P, et al. Exacerbation-like respiratory symptoms in individuals without chronic obstructive pulmonary disease: results from a population-based study. Thorax 2014;69:709–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Han MK, Kim MG, Mardon R, et al. Spirometry utilization for COPD: how do we measure up? Chest 2007;132:403–9. [DOI] [PubMed] [Google Scholar]
- 7.Heffler E, Crimi C, Mancuso S, et al. Misdiagnosis of asthma and COPD and underuse of spirometry in primary care unselected patients. Respir Med 2018;142:48–52. [DOI] [PubMed] [Google Scholar]
- 8.Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J 2013;42:1484–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Singh D, Donohue JF, Boucot IH, Barnes NC, Compton C, Martinez FJ. Future concepts in bronchodilation for COPD: dual- versus monotherapy. Eur Respir Rev 2021;30:210023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Han MK, Ye W, Kim D-Y, Woodruff P. Design of the redefining therapy in early COPD study. Chronic Obstr Pulm Dis 2020;7:382–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.National Institute for Health and Care Excellence. Chronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary care. February 25, 2004. (https://www.nice.org.uk/guidance/cg12).
- 12.Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med 1999;159:179–87. [DOI] [PubMed] [Google Scholar]
- 13.Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD 2005;2:75–9. [DOI] [PubMed] [Google Scholar]
- 14.Kon SSC, Canavan JL, Jones SE, et al. Minimum clinically important difference for the COPD Assessment Test: a prospective analysis. Lancet Respir Med 2014;2:195–203. [DOI] [PubMed] [Google Scholar]
- 15.Mahler DA, Witek TJ Jr. The MCID of the transition dyspnea index is a total score of one unit. COPD 2005;2:99–103. [DOI] [PubMed] [Google Scholar]
- 16.Rocha V, Jácome C, Martins V, Marques A. Are in person and telephone interviews equivalent modes of administrating the CAT, the FACIT-FS and the SGRQ in people with COPD? Front Rehabilit Sci 2021;2:729190 ( 10.3389/fresc.2021.729190/full). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mahler DA, Kerwin E, Ayers T, et al. FLIGHT1 and FLIGHT2: efficacy and safety of QVA149 (indacaterol/glycopyrrolate) versus its monocomponents and placebo in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2015;192:1068–79. [DOI] [PubMed] [Google Scholar]
- 18.Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J 2005;26:319–38. [DOI] [PubMed] [Google Scholar]
- 19.Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948–68. [DOI] [PubMed] [Google Scholar]
- 20.Definition and classification of chronic bronchitis for clinical and epidemiological purposes: a report to the Medical Research Council by their Committee on the Aetiology of Chronic Bronchitis. Lancet 1965;1:775–9. [PubMed] [Google Scholar]
- 21.Stott-Miller M, Müllerová H, Miller B, et al. Defining chronic mucus hypersecretion using the CAT in the SPIROMICS cohort. Int J Chron Obstruct Pulmon Dis 2020;15:2467–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Choi JY, Yoon HK, Shin K-C, et al. CAT score and SGRQ definitions of chronic bronchitis as an alternative to the classical definition. Int J Chron Obstruct Pulmon Dis 2019;14:3043–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tan WC, Sin DD, Bourbeau J, et al. Characteristics of COPD in never-smokers and ever-smokers in the general population: results from the CanCOLD study. Thorax 2015;70:822–9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
A data sharing statement provided by the authors is available with the full text of this article at NEJM.org.