

Abstract
Background:
There is an increasing array of treatment options for addressing clinically significant thyroid nodules, including radiofrequency ablation (RFA). While effective, the cost compared to alternative approaches has not been well elucidated.
Methods:
This study involved a retrospective chart review, focusing on variable direct cost (VDC) of each procedure, from April 2016 to January 2020. We analyzed costs for 53 open lobectomies and 16 RFA procedures.
Results:
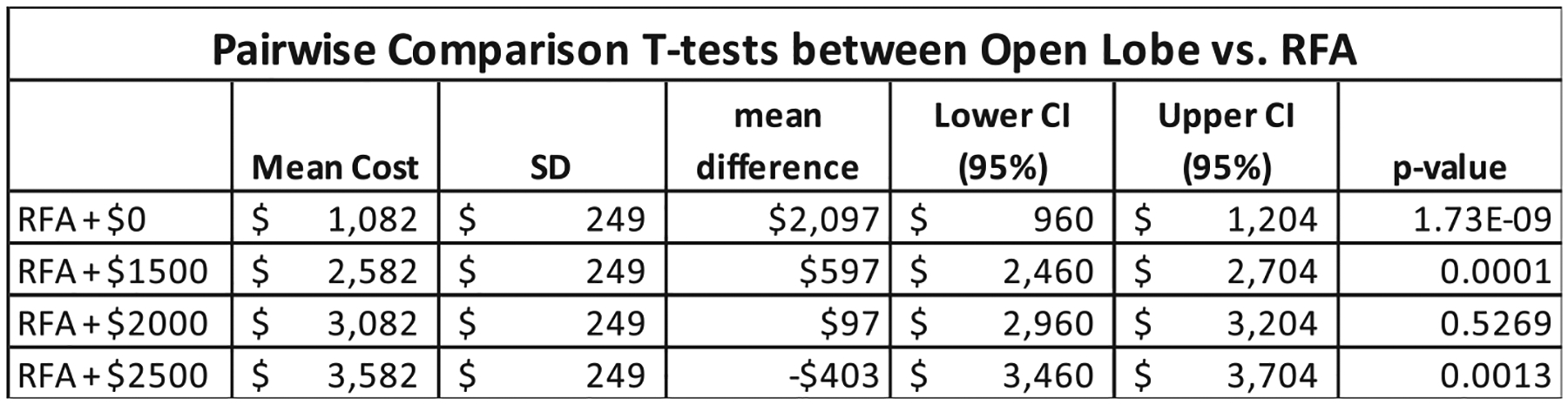
Cost effectiveness depended on the simulated cost of the RFA probe. In comparison to open lobectomy, the VDC to perform RFA was $597 (19%) cheaper when the simulated probe cost was $1500 and $403 (13%) more expensive for a probe cost of $2500. Statistical significance was achieved for both these differences.
Conclusions:
If cost per RFA probe can be less than $2100—the break-even dollar amount between open lobectomy and RFA—there would be considerable cost savings for treating thyroid nodules.
Keywords: cost effectiveness, health care costs, minimally invasive techniques, radiofrequency ablation, thyroid nodules
1 |. INTRODUCTION
Thyroid nodules are a common finding in the general population. While approximately 70% of Americans have a thyroid nodule,1 detection of nodules has been estimated at 6% in women and 1.5% in men.2 Most of these nodules are asymptomatic, do not impact overall thyroid function, and can be monitored conservatively.3 When patients have clinically relevant nodules, surgery is historically the primary treatment option, depending on the clinical scenario.
There is an increasing array of treatment options for addressing clinically significant thyroid nodules. As above, open surgical approaches were the mainstay for removal of symptomatic FNAC (fine needle aspiration cytology) benign thyroid nodules (BTNs). Percutaneous ethanol injection (PEI) may be an option for nodules that are purely cystic. More recently, radiofrequency ablation (RFA) of BTNs has been noted as an option and may decrease symptoms and improve cosmesis without significantly altering thyroid function.4 RFA is an ultrasound guided procedure performed percutaneously, typically under local anesthesia in an outpatient setting. While progress with the technique has been limited in North America, RFA has grown in popularity internationally as a safe alternative for managing select thyroid nodules and even small papillary thyroid carcinomas.5–7
The optimal candidate for RFA remains debated, and often is a mixture of appropriate pathology, surgical candidacy (or lack thereof), and patient preference.6 RFA has shown efficacy in treating benign thyroid neoplasms in comparison to open surgery, with VRR (volume reduction rate) ranging up to 85%, and showing lower complication rates with lower long-term costs.8 Additionally, a recent study examining the efficacy of successful onetime RFA in symptomatic autonomously functioning small to medium benign thyroid nodules, found a positive response, with a mean volume reduction of 75% by 12 months and withdrawal of antithyroid medication in 50% of patients.9 You et al. discusses the advantage of RFA in the treatment of solid nodules as compared to PEI for cystic nodules. They note skepticism of RFA in comparison to PEI in South Korea despite superior efficacy due to RFA’s cost ramifications.10
Given the wide variety of therapeutic options for symptomatic thyroid pathology, which effect a sizeable portion of the population, it is advisable to perform cost-based analysis of RFA to analyze the potential impact on health care utilization. There have been several international studies conveying cost effectiveness of RFA to date, but there remains a dearth of literature on cost comparison domestically.11 This study compares the cost-effectiveness of open thyroid lobectomy versus RFA for treatment of thyroid nodules.
2 |. MATERIALS AND METHODS
A retrospective chart review at a tertiary academic medical center was performed from April 2016 to January 2020. Cost data were collected from 53 open lobectomies from September 2016 to March 2019 and 16 RFA procedures between April 2016 and January 2020. RFA was performed under general anesthesia in the operating room. For open lobectomies, inclusion criteria specifically for this study, were as follows: thyroid lobe no larger than 10 cm, with an index nodule no larger than 6 cm if the nodule was deemed to be benign or indeterminate, and no larger than 2 cm for differentiated thyroid carcinoma. Patients with lymph node metastasis, substernal or extrathyroidal extension were excluded.12 For cost data, we queried CPT code 60220, which is used for “total thyroid lobectomy, unilateral.” RFA patients were found by initially querying CPT code 60699 (“other procedures of the endocrine system”), and then manually searching the electronic medical records under this umbrella for those that underwent RFA. Johns Hopkins institutional review board approval was obtained for this study.
We focused on the variable direct cost (VDC) of each procedure. By definition, this cost category encompasses the costs that vary with level of output.13 For example, this would include medications, anesthesia time, surgical supplies, and nursing expenses in the recovery unit. Please see Figure 1 for line-item detail of an example patient in each cohort.
FIGURE 1.
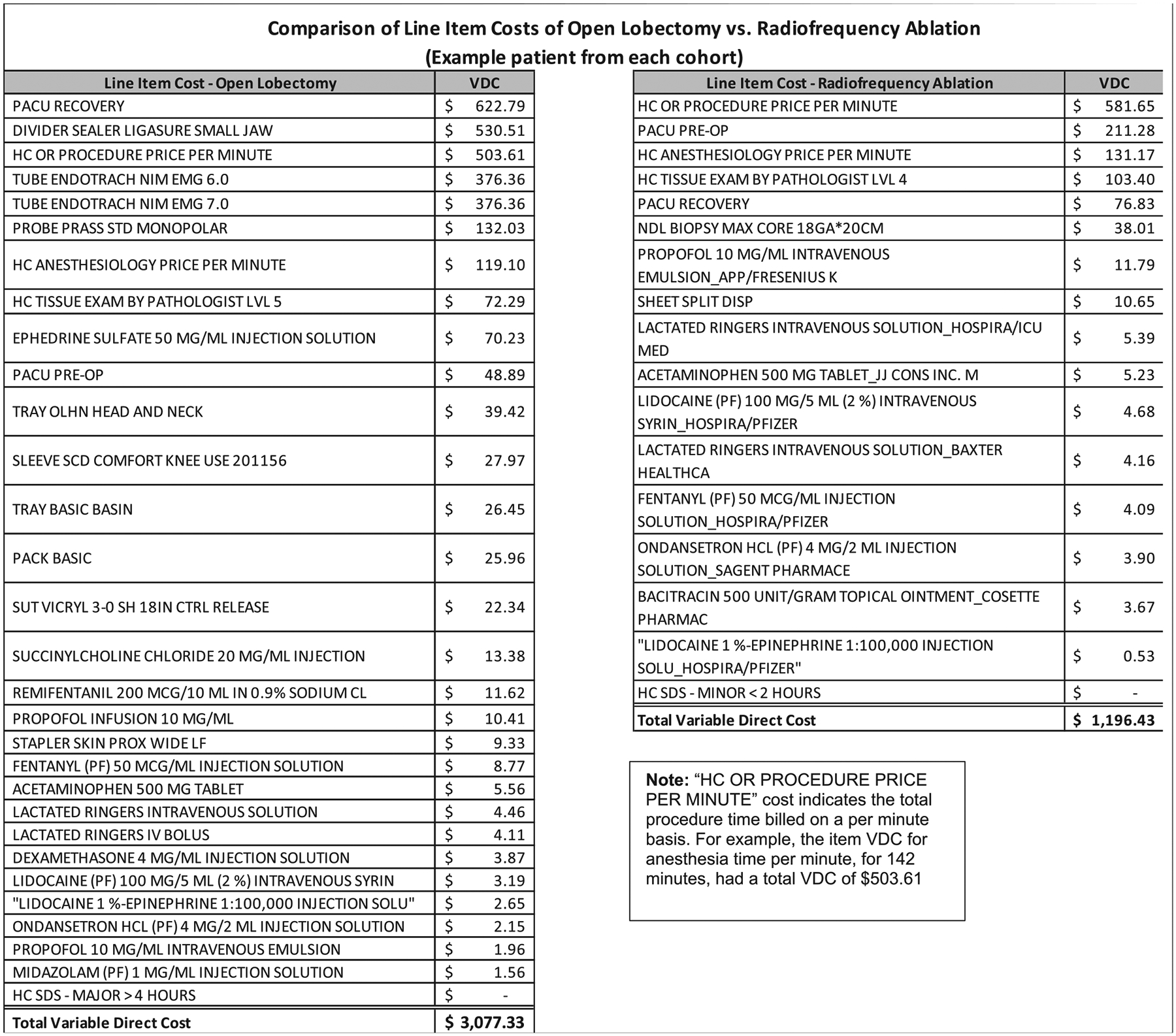
Comparison of line item costs of open lobectomy versus radiofrequency ablation (example patient from each cohort)
A few key assumptions were made in order ensure uniformity in our analysis. First, we did not consider total charge, as this differs based on an individual patient’s insurance. Additionally, fixed hospital costs (overhead costs) were not considered as these costs were deemed to be largely similar throughout either procedure, and thus would be negated. It should be noted that this assumption only holds true if RFA and surgery are both completed in an operative suite. Fixed costs may also vary by institution and therefore may be less generalizable. Moreover, in the initial series of radiofrequency ablation procedures at our institution, the cost of the radiofrequency ablation probe was provided free of charge14 by the manufacturer to assist our group with familiarity of their product line, and subsequently was not captured in the line-item cost details. As such, a range of cost was added to the available data, varying from $1500–$2500 per probe. Additionally, we compared average procedure time between open lobectomies and RFA to capture relative healthcare utilization. This was taken directly from the anesthesia record in the medical chart.
For our statistical analysis, we conducted four pairwise tests to compare open thyroid lobectomy with RFA, RFA + $1500, RFA + $2000, and RFA + $2500 to account for the range in cost estimate for the RFA probe. We applied a Bonferroni correction stipulating that the α value to determine significance is 0.05/4 = 0.0125. The homogeneity of variances was found not to be equal based on a Levene homogeneity of variances test. Therefore, nonparametric methods were used for comparison. Wilcoxon tests were subsequently performed using the Bonferroni correction for multiple testing.
3 |. RESULTS
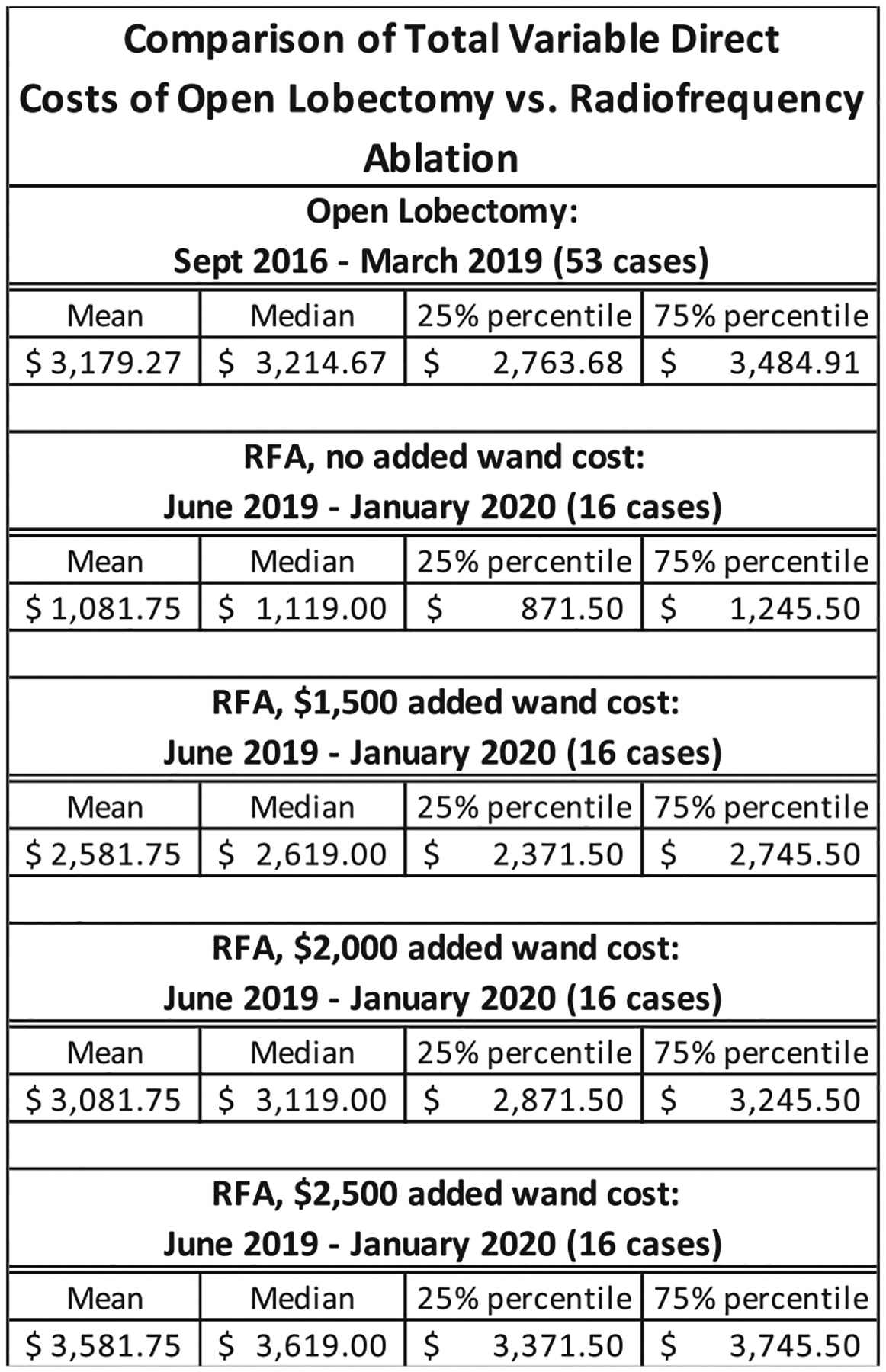
Cost savings largely depended on the cost of the RFA probe. In comparison to open lobectomy, the VDC to perform RFA was $597 (19%) cheaper when the probe cost was assumed to be $1500. However, RFA became more costly by $403 (13%) once estimated probe costs reached $2500. Statistical significance was achieved for both these differences (see Figure 2 for details). As seen in Figure 3, the median total VDC for the open lobectomies, 53 in total, was $3179. The median VDC for RFA + $1500 estimated probe cost was $2582, and $3582 with RFA + $2500 estimated probe cost.
FIGURE 2.
Pairwise comparison t tests between open lobe versus RFA
FIGURE 3.
Comparison of total variable direct costs of open lobectomy versus radiofrequency ablation
Additionally, we looked further into the source of cost differences between both approaches. Looking into the differences in operating room time for RFA procedures and open lobectomy. Figure 4 shows, on average, 53 less minutes of operating room time for RFA in comparison to open lobectomy, with 95% CI of 30.8–73.8 min (p < 0.001).
FIGURE 4.

Comparison of procedural time for open lobectomy versus radiofrequency ablation
4 |. DISCUSSION
In our analysis, we have demonstrated that the magnitude of cost savings ultimately depends on the cost of the radiofrequency ablation probe. There are additional benefits to shorter operative times as well when this procedure is completed in an operative suite. Specifically, in a tertiary academic medical center, savings can be achieved when the cost of the RFA probe is roughly $2100 or less, given the average costs of open lobectomy and RFA (seen in Figure 3). Moreover, there is the potential for substantially greater savings when RFA is performed in an outpatient clinic as opposed to in an operating room, where costs such as anesthesia fees, OR time, PACU time, and sedative medications would be eliminated (additional savings of approximately $1082 per procedure at our institution).
There are some shortcomings in our observation to be noted. First, our study does not capture the large up-front investment in equipment, training, staffing, and available space needed in the outpatient setting. Furthermore, our study does not capture whether open lobectomy was done for a benign thyroid nodule or malignant disease. This may make operative time for open lobectomy longer, and thus inflate open lobectomy costs. Additionally, a certain percentage of RFA will require sequential ablation in the future—especially for larger nodules—should the nodule regrow over time and necessitate repeated intervention.
More recently, remote access surgical approaches using endoscopic and robotic techniques—which often come with high procedural costs—have been developed and are increasing in popularity. As different approaches for removal of thyroid nodules are offered to the population, cost-effectiveness cannot be ignored. Currently, there is not widespread endorsement of RFA from government and private insurers in the United States.15 One contributing factor is cost transparency, which has been implicated in wider adoption internationally.16 Very recently, a small prospective randomized study from Brazil showed statistically significant decreased hospital utilization and costs (24% cheaper) in comparison to partial thyroidectomy.17 This study noted the cost of the probe as the major contributor to RFA costs. Yue et al.’s 2016 study showed probe costs as the driving factor for greater expense of RFA in comparison to open lobectomy.18
With concern for minimizing postprocedural hospitalizations and hospital resource optimization in the setting of COVID-19 limitations, emphasizing minimally invasive, outpatient techniques are even more desirable. Further discussion is needed to help elucidate the cost and health benefits of RFA for patients with symptomatic thyroid nodules who are not candidates for invasive surgical approaches. RFA has become a viable, safe, and affordable option that is more likely to preserve thyroid function. Given the less invasive nature of this procedure and the potential therapeutic benefits, it is expected that commercial payers will recognize the need to support this technique in the appropriate clinical scenario.
Funding information
Taewoong Medical Co. Ltd.; RF Medical Co. Ltd.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- 1.Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Al-qurayshi Z, Farag M, Shama MA, Ibraheem K, Randolph GW, Kandil E. Total thyroidectomy versus lobectomy in small nodules suspicious for papillary thyroid cancer: cost-effectiveness analysis. Laryngoscope. 2020;130:2922–2926. [DOI] [PubMed] [Google Scholar]
- 3.Cappelli C, Franco F, Pirola I, et al. Radiofrequency ablation of functioning and non-functioning thyroid nodules: a single institution 12-month survey. J Endocrinol Invest. 2020;43:477–482. [DOI] [PubMed] [Google Scholar]
- 4.Solbiati M, Ierace T, Dellanoce M. Percutaneous US-guided radiofrequency ablation of metastatic lymph nodes from papillary cancer of the thyroid gland: initial experience in two cases. Radiology. 1998;209:385. [Google Scholar]
- 5.Zhang M, Tufano RP, Russell JO, et al. Ultrasound-guided radiofrequency ablation versus surgery for low-risk papillary thyroid microcarcinoma: results of over 5 years’ follow-up. Thyroid. 2020;30(3):408–417. [DOI] [PubMed] [Google Scholar]
- 6.Lee GM, You JY, Kim HY, et al. Successful radiofrequency ablation strategies for benign thyroid nodules. Endocrine. 2019;64(2):316–321. [DOI] [PubMed] [Google Scholar]
- 7.Kim JH, Baek JH, Lim HK, et al. Thyroid radiofrequency ablation guideline: Korean Society of Thyroid Radiology. Korean J Radiol. 2018;19(4):632–655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Che Y, Jin S, Shi C, et al. Treatment of benign thyroid nodules: comparison of surgery with radiofrequency ablation. AJNR Am J Neuroradiol. 2015;36(7):1321–1325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bernardi S, Stacul F, Michelli A, et al. 12-month efficacy of a single radiofrequency ablation on autonomously functioning thyroid nodules. Endocrine. 2017;57(3):402–408. [DOI] [PubMed] [Google Scholar]
- 10.You JY, Park DW, Kim HY. Answer to the readers of “Successful radiofrequency ablation strategies for benign thyroid nodules”. Endocrine. 2019;65(3):719. [DOI] [PubMed] [Google Scholar]
- 11.Bernardi S, Dobrinja C, Fabris B, et al. Radiofrequency ablation compared to surgery for the treatment of benign thyroid nodules. Int J Endocrinol. 2014;2014:934595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Razavi CR, Tanavde VA, Kim AS, Shaear M, Tufano RP, Russell JO. The variable direct cost and cost drivers of transoral endoscopic thyroidectomy vestibular approach. Gland Surg. 2021;10(2):521–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Taheri PA, Butz D, Griffes LC, Morlock DR, Greenfield LJ. Physician impact on the total cost of care. Ann Surg. 2000;231(3):432–435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.RFA probes provided by RF Medical Co. Ltd. and Taewoong Medical Co. Ltd.
- 15.“Thyroid nodule ablation FAQs.” University of Virginia Health System. https://uvahealth.com/services/imaging/thyroid-ablation/faqs. [Google Scholar]
- 16.Sosa JA, Hanna JW, Robinson KA, Lanman RB. Increases in thyroid nodule fine-needle aspirations, operations, and diagnoses of thyroid cancer in the United States. Surgery. 2013;154(6):1420–1426. discussion 1426–1427. [DOI] [PubMed] [Google Scholar]
- 17.Schalch MS, Costa ACN, de Souza RP, Guerra FLB, Guerreiro R, De Cicco R. Radiofrequency ablation of thyroid nodules: prospective cost-effectiveness analysis in comparison to conventional thyroidectomy. Arch Endocrinol Metab. 2021;65(5):752–757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yue WW, Wang SR, Li XL, et al. Quality of life and cost-effectiveness of radiofrequency ablation versus open surgery for benign thyroid nodules: a retrospective cohort study. Sci Rep. 2016;6:37838. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.