

Abstract
We examined how gender, body mass, race, age, and sexual orientation were linked to appearance evaluation, overweight preoccupation, and body image-related quality of life among 11,620 adults recruited via Mechanical Turk. Men were less likely than women to report low appearance evaluation, high overweight preoccupation, negative effects of body image on their quality of life, being on a weight-loss diet, and trying to lose weight with crash diets/fasting. Racial differences were generally small, but greater appearance evaluation was reported by Black men versus other groups and Black women versus White women. Across all measures, gay and bisexual men reported poorer body image than heterosexual men, with only small effect sizes observed for sexual orientation differences among women. Body mass, but not age, was strongly associated with body image. The prevalence of poor body image highlights the need for interventions. On the positive side, half of men and women reported high appearance evaluation. Examination of this group could identify factors promoting positive body image.
Keywords: Body image, Gender, Sexual orientation, Body mass index, Race, Age
1. Introduction
Body dissatisfaction, defined as negative attitudes about one’s body (Cash, 1990), plays a critically important role in shaping physical and mental health (Frederick, Lever, et al., 2007; Gillen & Markey, 2018; Gillespie, Frederick, Harari & Grov, 2015; Ridolfi & Crowther, 2013). For example, in a national sample of adult Australian women, the degree of body dissatisfaction is associated with poorer mental health and psychosocial functioning as well as increased risk of impairment in physical health, even when controlling for body weight (Mond, Mitchison, Latner, Hay, Owen & Rodgers, 2013). Despite the importance of body dissatisfaction in many people’s lives, little is known about body dissatisfaction on the national level in the United States (U.S.), across men and women with samples that are diverse in terms of body mass, race, age, and sexual orientation. Demographic characteristics have been an important focus of past research for the identification of at-risk populations for body image problems. Understanding the factors linked to body image across demographic groups is critical to guide effective public health policy and interventions by better identifying population subgroups at risk, disparities, and facilitating more targeted and tailored resources for at risk subgroups.
Below, we highlight key findings and knowledge gaps from studies examining body satisfaction across men and women, and other demographic characteristics.
1.1. Gender Differences in Body Image
Sociocultural theories of body image emphasize that women face more intensive appearance-related pressures, particularly to be slender, and more recently, to be toned and fit. leading to more women than men experiencing high levels of body dissatisfaction (Fredrickson & Roberts, 1997; Thompson, Heinberg, Altabe & Tantleff-Dunn, 1999). However, the magnitude of these differences varies depending on the specific aspect of body image being assessed. In meta-analyses, women report slightly lower physical appearance-related self-esteem than men (d = 0.35; Gentile, Grabe, Dolan-Pascoe, Twenge, Wells & Maitino, 2009), and moderately higher thinness-oriented body dissatisfaction (d = 0.51; Karazsia et al., 2017). For example, several national studies with one-item measures document that men are less likely than women to report overall dissatisfaction with their physical appearances (Fallon et al., 2014; Frederick, Sandhu, Morse & Swami, 2016; Frederick, Tomiyama, Bold & Saguy, 2020), less likely to say they were unhappy with their appearance than women, regardless of their marital status (Frederick, Garcia, Gesselman, Mark, Hatfield & Bohrnstedt, 2020), and that men were less likely than women to report overall dissatisfaction with their weights (Fallon et al., 2014; Frederick et al., 2020; Frederick, Sandhu, et al., 2016;). However, the magnitude of differences between the genders was small, with one national study finding no statistically significant difference between genders on evaluation of appearance (Fallon et al., 2014). In contrast, relatively large gender differences are found in overweight preoccupation, which assesses cognitions about weight as well as weight-loss diet behaviors. Men are less likely to report high overweight preoccupation (1.00–2.74 out of 5.00 on Likert scale) than women (d = 0.45; 9% vs. 22%; Fallon et al., 2014). However, this overweight preoccupation measure averages together cognitions (worrying about being or becoming fat) along with behaviors (fasting, crash dieting, and dieting to lose weight). Although these constructs are intercorrelated, the current study provided the opportunity to investigate the prevalence of these attitudes and behaviors as individual items and as composite scales to allow for cross-study comparisons with previous research.
The degree to which body image impacts quality of life is important for investigation; but remains an understudied topic within U.S. national studies. A convenience sample drawn in Canada found a more positive body image quality of life among men than women (Rusticus et al., 2008), as did studies of college students in Spain (Lobera & Rios, 2011) and in the United States (Cash et al., 2004). Further research is needed in this area.
Although national studies have documented differences in body image across gender, a paucity of research exists from an intersectionality framework (Burke, Schaefer, Hazzard & Rodgers, 2020). An intersectional approach highlights that body image experiences are shaped by multiple aspects of a person’s identities and can bring attention to the unique experiences of people with multiple marginalized identities. For example, the experiences of Black women and Asian women within the U.S. cultural context might differ markedly from each other (Cole, 2009). The current study builds upon the existing literature by examining how body mass, age, race, and sexual orientation are connected to body image experiences among women and among men in a national sample.
1.2. Body Mass Differences in Body Image
Men and women with higher BMIs report greater body dissatisfaction in national samples (Fallon et al., 2014; Frederick, Forbes, Grigorian & Jarcho, 2007; Frederick et al., 2020; Frederick et al., 2006; Frederick, Sandhu, et al., 2016; Kruger, Lee, Ainsworth & Macera, 2008; Peplau, Frederick, Yee, Maisel, Lever & Ghavami, 2009; Swami, Tran, Stieger & Voracek, 2015). Sociocultural ideals emphasize slenderness (Sypeck, Gray, Etu, Ahrens, Mosimann & Wiseman, 2006) or slenderness with large breasts and narrow waist-to-hip ratios for women (Burch & Johnsen, 2020), and about half of women report feeling worse about their bodies after exposure to these images (Frederick, Daniels, Bates & Tylka, 2017). In contrast, popular media features leanness, muscularity, and athleticism as the ideals for men (Burch & Johnsen, 2020; Frederick et al., 2005; Morrison & Halton, 2009). In parallel, many men report preferences for slender dating partners (Fales, Frederick, Garcia, Gildersleeve, Haselton & Fisher, 2016), and many women prefer relatively toned and muscular men (Frederick & Haselton, 2007; Gray & Frederick, 2012; Sell et al., 2017). Consistent with these sociocultural pressures, most women in industrialized cultures want to be thinner (Swami et al., 2010), and increasingly, fit and toned (Tiggemann & Zaccardo, 2015), whereas most young men want to be more muscular (Frederick, Buchanan, et al., 2007). Men and women with higher body weight are also the targets of greater prejudice and discrimination, leading to negative health consequences (Major et al., 2018).
In addition to this general linear association between BMI and body image satisfaction, the association may have a curvilinear component. Men with very low BMIs in some studies report higher body dissatisfaction than men in the “normal weight” range (Frederick, Forbes, et al., 2007; Frederick, Sandhu, et al., 2016). This curvilinear trend is also evident in the risk of anabolic steroids use among men, with men who describe themselves as either very underweight or very overweight being at greatest risk (Jampel, Murray, Griffiths & Blashill, 2016). This lower satisfaction among both very thin and very overweight men may reflect the fact that both body types deviate from the muscular or athletic ideal.
1.3. Racial Differences in Body Image
Body image experiences vary across racial groups, with differences theorized to be due to acculturation (Schooler, 2008), group differences in privilege and power (Cole, 2009), as well as sexual objectification experiences, particularly for women (Watson, et al., 2019). In a recent national study, Black women reported greater happiness with their appearance than White women (Frederick et al., 2020), while White women reported lower overall happiness with their appearance than Asian women, even when controlling for BMI (Frederick, Garcia, et al., 2020). In contrast, meta-analyses on racial differences in body satisfaction among women generally find small differences or no differences across Asian, White, and Hispanic women (ds < 0.20). Black women, however, tend to report greater body satisfaction than White women (d = 0.29, Grabe & Hyde, 2006; d = 0.28, Roberts, Cash, Feingold & Johnson, 2006). The lack of group differences between White and Asian American women is somewhat surprising, given that Asian women tend to have lower BMIs than other groups (Ogden, Carroll, Fryar & Flegal, 2015) and BMI is strongly tied to body satisfaction. Some research on college students in California and Hawaii found that Asian American women report lower appearance evaluation, but not higher overweight preoccupation, than White women (Frederick & Forbes et al., 2007; Forbes & Frederick, 2008; Frederick, Kelly, Latner, Sandhu & Tsong, 2016), which is driven in part by differences in satisfaction with facial features (Frederick & Kelly et al., 2016).
Research on racial differences in body image among men is less common. Some studies found no differences across minority groups (Bucchianeri, Arikian, Hannan, Eisenberg & Neumark-Sztainer, 2013), while other studies observed that Asian American men reported higher levels of body dissatisfaction than other minority men (Frederick, Forbes, et al., 2017; Kelly, Cotter, Tanofsky-Kraff & Mazzeo, 2015). In a national study, White men reported lower appearance happiness than Black men (d = 0.17; β = .26) and Hispanic men (d = 0.10; β = .16). The experiences of minority men have been under-studied, and greater understanding of the experiences of all racial groups is needed at the national level.
1.4. Age Differences in Body Image
Understanding the impact of age on body image is important. Youthful appearance is routinely featured as attractive and prestigious in popular culture, creating a discrepancy between sociocultural ideals and normative age-related changes in body weight and appearance. As people age, however, they take on new social identities that can provide self-esteem and meaning (e.g., parenthood, employment) (Tiggemann, 2004; Greenleaf, 2005).
In some national studies, there are no statistically significant differences between specific age groups for men or women (Fallon et al., 2014). Other national studies find in regression analyses that men and women report slightly lower body satisfaction, but almost all associations between age and body image outcomes fall below β = 0.20 and most below β = 0.10 (Frederick et al., 2020; Frederick & Sandhu et al., 2016). These findings are consistent with longitudinal studies reporting that weight dissatisfaction in women remains relatively stable over time (Keel, Baxter, Heatherton & Joiner, 2007).
1.5. Sexual Orientation Differences in Body Image
Previous research suggests that sexual orientation relates to body image differently for men and women. Several theoretical frameworks have been used to understand differences in body image for gay, lesbian and bisexual individuals. Minority Stress Theory posits that individuals who identify as gay, lesbian, or bisexual are vulnerable to stigma, a chronic social stressor, in addition to ‘normative’ gender-related sociocultural pressure about appearance (Meyer, 1995). This combination of stressors may in turn increase risks for body dissatisfaction. (Morrison & McCutcheon, 2012). Relatedly, intersectionality, or recognition that individuals can have multiple and identities across sex, gender, race, class, and sexual orientation, can also be used to understand appearance-related experiences among sexual minorities (Cole, 2009; Morrison & McCutcheon, 2012).
In one meta-analysis, gay men were less satisfied with their body image than heterosexual men. The effect size was small (d = 0.29), but there were only 49 gay men per study on average (Morrison et al., 2004). National studies also consistently find that gay men report greater body dissatisfaction but with typically small or small-to-moderate effect sizes (Frederick et al., 2020; Frederick, Lever, & Peplau, 2007; Frederick, Sandhu, et al., 2016; Peplau et al., 2009). Gay men are more likely to report that their feelings about their body image have a negative impact on their quality of life as it relates to their sex life (Peplau et al., 2009). Furthermore, reviews of the literature indicated that sexual minority men are more likely than heterosexual men to report poorer body image (He, Sun, Lin & Fan, 2020) and to exhibit and report disordered eating patterns (Murray et al., 2017).
Patterns are less clear for how sexual orientation relates to body satisfaction among women. Existing research typically observed no differences or only small differences between lesbian and heterosexual women in their levels of body dissatisfaction (He et al., 2020; Moore & Keel, 2003; Moreno-Dominguez et al., 2019; Morrison et al., 2004). In the Morrison et al. (2004) meta-analysis, lesbian women reported slightly higher body satisfaction overall (d = 0.12), and when controlling for BMI (d = 0.22). Similarly, small or null effects are seen in national studies (Frederick et al., 2020; Frederick, Lever, & Peplau, 2007; Frederick, Sandhu, et al., 2016; Peplau et al., 2009).
1.6. National Body Image Studies
The first national body image study in the U.S. was conducted 50 years ago with Psychology Today (Berscheid et al., 1973; Frederick, Bohrnstedt, Hatfield & Berscheid, 2014), followed up with two additional studies (Cash et al., 1986; Garner & Kearney-Cooke, 1996). In the intervening years, few subsequent large-scale national studies focused specifically on affective body image – defined as how people feel about their appearance and bodies - were undertaken (for reviews, see Fiske, Fallon, Blissmer & Redding, 2014; Frederick, Jafary, Daniels & Gruys, 2012).
Over the past 20 years, most national studies in the United States focusing on affective body image have relied on one-item measures of key constructs (Frederick & Essayli, 2016; Frederick et al., 2006; Frederick et al., 2008; Frederick, Garcia, et al., 2020; Krueger et al., 2008; Lever et al., 2006; Lever, Frederick, Laird & Sadeghi-Azar, 2007; Peplau et al., 2009; Swami et al., 2015). This provided useful information, but body image is a multidimensional construct consisting of cognitive, behavioral, affective, and perceptual factors (Banfield & McCabe, 2002). One national study, which used a Mechanical Turk sample, relied on multi-item validated measures of affective body image and related constructs (N = 1893; Fallon et al., 2014). This study provided an important look at gender, body mass, and age differences on commonly used body image measures such as appearance evaluation, which assess people’s feelings regarding their attractiveness and looks, and overweight preoccupation, which assesses both cognitions about weight and dieting/fasting behaviors (Brown et al., 1990; Cash, 2000). However, this study did not examine differences by sexual orientation, and comparisons by race were limited by the fact that there were fewer than 50 participants identifying with each racial group.
The current study, The U.S. Body Project I, was conceived as a follow-up to the important work conducted by Fallon et al. (2014) by examining additional dimensions of body image using well-validated measures, and examining body image differences from an intersection framework including body mass, race, age, and sexual orientation, across men and women. The current study recruited and analyzed a substantially larger sample (N = 11,620) than Fallon and colleagues (2014) which allowed larger subsamples of groups with marginalized identities such as gay, lesbian, and bisexual adults. Due to the rare opportunity afforded by this large national dataset, we provide a detailed and comprehensive summary of the prevalence and demographic predictors of body image concerns. Further, we identify the percentage of men and women who report a very negative impact of their body image on their quality of life.
Data derived from large, national samples that identifies how demographic factors relate to body image beliefs, attitudes, and behaviors is critical in order to identify differential risk factors for body dissatisfaction, provide inspiration for investigations of how sociocultural factors shape the body image experiences of different groups, evaluate sociocultural trends in body image at the population level, and inform more sensitive clinical and population-based body image interventions. Importantly, These data also have the potential to inform our understanding of factors that are associated with positive body image (Tylka & Wood-Barcalow, 2015), including people’s perceptions of the positive impacts of their body image on different aspects of their lives (Cash & Fleming, 2002).
1.7. Hypotheses
1.7.1. Hypothesis 1: Gender Comparisons
Based on the extant literature, we hypothesized significant gender differences between men and women, with women reporting more appearance evaluation, overweight preoccupation cognitions, overweight preoccupation behaviors, and poorer body image quality of life relative to men.
1.7.2. Hypothesis 2: BMI Comparisons
We hypothesized that men and women with higher body mass would report poorer body image, and potentially an uptick in body dissatisfaction among very slender men and women.
1.7.3. Hypothesis 3: Racial Group Comparisons
We hypothesized that Black men and women would report the most appearance satisfaction relative to other racial groups, while Asian men and women would report lower appearance evaluation than other groups. All other racial group differences were exploratory, and this study provided the rare opportunity to study these differences among men.
1.7.4. Hypothesis 4: Age Comparisons
Consistent with the existing literature, we hypothesized age to be unrelated or weakly related to the body image variables.
1.7.5. Hypothesis 5: Sexual Orientation Comparisons
Overall, relatively less research has examined body image for bisexual men and women; most studies have combined bisexual and gay orientations into a sexual minority group, likely due to small sample sizes. Taking these findings into account, we hypothesized small-to-moderate differences among men with sexual minority men reporting poorer body image, and negligible differences among women across the sexual orientation groups.
1.7.6. Additional Analyses: Examining Individual Items in Addition to Full Validated Measures
Finally, in addition to examining demographic differences on the full validated body image measures, we also selected some individual items to analyze as well. In particular, we focus on the items assessing weight-related behaviors in these scales (dieting; fasting) in contrast to the items assessing weight-related cognitions (e.g., being conscious of weight and changes in weight). This was done for two reasons. The first is that large national studies are often restricted to only a few items, so presenting the results for selected items of interest allows future national studies with that restriction to compare with the current study. The second is that analyzing scales on an item-by-item basis can reveal notable differences in absolute level of weight-related cognitions versus behaviors, even if both are connected by a single underlying factor. In terms of group differences, we hypothesized the same patterns for these items as the ones hypothesized in the aforementioned sections.
2. Method
2.1. Participants
Data were drawn from the U.S. Body Project I, which is described in detail in the Procedures section. The sample was restricted to include only participants who completed the full survey and who fit the following criteria: (a) reported currently living in the United States; (b) completed all key body image items; (c) were aged 18–65; (d) had body mass indexes (BMI) ranging from 14.50 to 50.50 based on self-reported height and weight. Age and BMI restrictions were placed on the sample to prevent outliers or mis-entered values from having undue influence on the effect size estimates. The data were collected in 2016. A total of 13,518 people clicked on the survey, 12,571 answered the first question, and 12,151 completed the full survey. After applying the inclusion criteria, the analyzed sample included 11,620 participants. Key demographics are shown in Table 1.
Table 1.
Demographics.
| Demographics | Overall | Men | Women | Demographics | Overall | Men | Women |
|---|---|---|---|---|---|---|---|
| Age (M, SD) | 34.1 (10.7) | 33.0 (10.0) | 34.1 (10.7) | Hours Worked (M, SD) | 33.1 (15.6) | 36.1 (14.4) | 33.1 (15.6) |
| Years in U.S. (M, SD) | 33.1 (11.3) | 32.0 (10.5) | 33.1 (11.3) | BMI (M, SD) | 27.6 (6.3) | 27.5 (5.6) | 27.6 (6.3) |
| Gender (%, N) | Education (%, N) | ||||||
| Men | 45.6 (5293) | – | – | Some High School or Less | 0.6 (74) | 0.5 (28) | 0.7 (46) |
| Women | 54.4 (6327) | – | – | High School Degree | 9.1 (1052) | 9.8 (518) | 8.4 (534) |
| Race (%, N) | Some College | 32.3 (3749) | 32.5 (1718) | 32.1 (2031) | |||
| White | 75.2 (8742) | 74.5 (3945) | 75.8 (4797) | College Degree | 44.2 (5131) | 43.7 (2311) | 44.6 (2820) |
| Hispanic | 4.0 (470) | 5.0 (265) | 3.2 (205) | Advanced Degree | 13.9 (1614) | 13.6 (718) | 14.2 (896) |
| Black | 6.7 (774) | 5.6 (297) | 7.5 (477) | Orientation (%, N) | |||
| Asian | 6.1 (714) | 7.0 (370) | 5.4 (344) | Heterosexual | 88.3 (10264) | 92.0 (4869) | 85.3 (5395) |
| Indian | 0.3 (34) | 0.3 (16) | 0.3 (18) | Gay or Lesbian | 3.5 (407) | 3.7 (194) | 3.4 (213) |
| Native American | 0.5 (55) | 0.5 (26) | 0.5 (29) | Bisexual | 6.8 (792) | 3.7 (194) | 9.5 (598) |
| Pacific Islander | 0.1 (16) | 0.1 (6) | 0.2 (10) | Asexual | 0.5 (56) | 0.2 (9) | 0.7 (47) |
| White-Hispanic | 1.9 (225) | 2.0 (108) | 1.8 (117) | Other | 0.9 (101) | 0.5 (27) | 1.2 (74) |
| White-Black | 0.8 (90) | 0.5 (29) | 1.0 (61) | BMI (%, N) | |||
| White-Asian | 1.0 (119) | 1.0 (54) | 1.0 (65) | Lowest BMI (Underweight) | 1.6 (190) | 1.2 (64) | 2.0 (126) |
| White-Middle Eastern | 0.9 (110) | 0.9 (45) | 1.0 (65) | Low BMI (Normal Weight) | 39.0 (4535) | 36.2 (1918) | 41.4 (2617) |
| Other | 2.3 (271) | 2.3 (132) | 2.2 (139) | Medium BMI (Overweight) | 31.3 (3632) | 36.8 (1947) | 26.6 (1685) |
| High I BMI (Obese I) | 15.1 (1755) | 15.4 (815) | 14.9 (940) | ||||
| In College (%, N) | 17.4 (2021) | 18.7 (988) | 16.3 (1033) | High II BMI (Obese II) | 7.2 (840) | 6.5 (343) | 7.9 (497) |
| High III BMI (Obese III) | 5.7 (668) | 3.9 (206) | 7.3 (462) | ||||
| Born In U.S. (%, N) | 94.0 (10923) | 94.1 (4981) | 93.9 (5942) |
In addition to these demographics, men and women also reported their relationship status: married (men = 32.3%, n = 1712; women = 43.3%, n = 2738), cohabiting (15%, 793; 19%, 1204), dating one person exclusively (20%, 1060; 16%, 1013), dating multiple people (3.2%, 168; 1.8%, 113), widowed (0.3%, 18; 0.8%, 51), not currently involved (29.1%, 1542; 19.1%, 1208).
Looking across men and women with differing sexual orientations, the average BMIs ranged from 27.4 to 28.8 among heterosexual men (27.5), heterosexual women (27.5), gay men (27.3), lesbian women (28.1), bisexual men (28.2), bisexual women (28.4), other men (25.2) and other women (27.6). The average age for each of these groups, rounded to the nearest whole number, were 33, 36, 32, 34, 31, 29, 29, and 27, respectively. Looking across men and women with differing races, the BMIs for Asian women (23.3) and Asian men (24.6) were notably below that of White women (27.9), White men (27.8), Hispanic women (27.0), Hispanic men (27.4), Black Women (29.0), and Black men (27.6), other men (27.1) and other women (27.6). The average ages for each of these groups were 30, 29, 36, 34, 31, 30, 34, 34, 31, and 32, respectively.
2.1.1. Comparison to Nationally Representative Datasets
Participants came from all 50 states as well as Washington D.C. and Puerto Rico. The current study relies on a national dataset, but the sample is not nationally representative. We provide nationally representative data as a comparison. In terms of BMI, the average body mass in 2015–2016 was 29.1 for men and 29.6 for women (Fryar, Kruszan-Moran, Gu & Ogden, 2018) which is slightly higher than the average BMI for men (27.5) and women (27.6) in our sample. In our sample, there are more non-Hispanic White participants (74.5% of men, 75.8% of women) compared to the population overall (60.7%, United States Census Bureau, 2018). The percentage of men and women in our sample with a high school degree (99.5% men, 99.3% women) and a college degree (57.3% men, 58.8% women) was higher than the national percentage of people with a high school degree (87%) and Bachelor’s degree or higher (30.9%), respectively.
The percentage of men and women identifying as heterosexual was slightly lower in our sample (92.0% men, 85.3% women) than in nationally representative samples (95.1% men, 92.3% women), although the comparison national survey did not have an “other” option where participants could specify identities other than “bi-sexual,” “homosexual, gay, or lesbian,” “don’t know,” or “refused” (Copen et al., 2016). The seven states with the largest number of men and women came from California (11.7% men, 9.7% women), New York (6.1% men, 5.3% women), Florida (7.4% men, 7.0% women), Texas (6.3% men, 6.7% women), Pennsylvania (4.8% men, 5.5% women), Illinois (4.5% men, 4.2% women), and Ohio (4.4% men, 4.1% women) which also corresponds to the seven most populous states in the U.S. (United States Census Bureau, 2014).
2.2. Procedure and Overview of The U.S. Body Project I
The first author’s university institutional review board approved the study. Adult participants were recruited via Amazon Mechanical Turk, a widely used online panel system used by researchers to access adult populations (Berinsky et al., 2012, Buhrmester et al., 2011, Kees, Berry, Burton & Sheehan, 2017; Paolacci et al., 2010; Robinson, Rosenzweig, Moss & Litman, 2019). Participants were paid 51 cents for taking the survey. The survey was advertised with the title “Personal Attitudes Survey,” and the description explained that “We are measuring personal attitudes and beliefs. The survey will take roughly 10–15 min to complete.” The general wording of the advertisement was used to avoid selectively recruiting people particularly interested in body image. After clicking on the advertisement, the participants read a consent form providing more details about the content of the study, including that it would contain items related to sex, love, work, and appearance. They were then given the option to continue with the survey or exit.
After providing informed consent, participants completed the numerical textbox questions (e.g., hours per week worked, number of times in love, sex frequency per week, longest relationship), followed by appearance evaluation (Cash, 2000), the Sociocultural Attitudes Towards Appearance Questionnaire-4 (Schaefer et al., 2015), face satisfaction (Frederick, Kelly, et al., 2016), overweight preoccupation (Cash, 2000), body image quality of life (Cash & Fleming, 2002), body surveillance (McKinley & Hyde, 1996), and finally demographics.
This manuscript is part of a series of papers emerging from The U.S. Body Project I. This project invited over 20 body image and eating disorder researchers, four sexuality researchers, and six computational scientists to apply their content and data-analytic expertise to the dataset. This project resulted in the following set of 11 papers for this special issue.
The first two papers examine how demographic factors (gender, sexual orientation, BMI, age, race) are related to body satisfaction and overweight preoccupation (current paper) and to measures derived from objectification theory and the tripartite influence model, including body surveillance, thin-ideal and muscular/athletic ideal internalization, and perceived peer, family, and media pressures (Frederick, Pila, et al., 2022). The second set of papers examine how these measures and demographic factors predict sexuality-related body image (Frederick, Gordon, et al., 2022) and face satisfaction (Frederick, Reynolds, Barrera, Alley, Garcia & Murray, 2022).
The third set of papers use structural equation modelling to examine the links between sociocultural appearance concerns and body satisfaction among women and across BMI groups (Frederick, Tylka, Rodgers, Pennesi, et al., 2022), among men and across different BMI groups (Frederick, Tylka, Rodgers, Convertino, et al., 2022), across racial groups (Frederick, Schaefer, et al., 2022) and across sexual orientations (Frederick, Hazzard, Schaefer, Rodgers, et al., 2022).
The fourth set of papers focus on measurement and statistical issues by examining measurement invariance of the scales across different demographic groups (Hazzard, Schaefer, Thompson, Rodgers & Frederick, 2022) and conducting a psychometric evaluation of an abbreviated version of the Body Image Quality of Life Inventory (Hazzard, Schaefer, Thompson, Murray & Frederick, 2022). Finally, the last paper uses machine learning modelling to compare the effectiveness of nonlinear models versus linear regression for predicting body image outcomes (Liang et al., 2022).
2.3. Body Image Outcome Measures
For all of the measures below, we report the Cronbach’s alpha for the participants overall and by gender. The measures showed high measurement invariance across different demographic groups (e.g., race, sexual orientation), which can be viewed in another manuscript emerging from this dataset (Frederick, Hazzard, Schaefer, Thompson, et al., 2022).
2.3.1. Multidimensional Body-Self Relations Questionnaire - Appearance Evaluation Subscale
Participants completed the Appearance Evaluation subscale of the Multidimensional Body-Self Relations Questionnaire (Brown et al., 1990; Cash, 2000). This scale measures feelings of physical attractiveness and satisfaction with one’s appearance and contains seven items (e.g., “I like the way I look without my clothes on”). Responses were recorded on a 5-point Likert scale (1 = Definitely Disagree to 5 = Definitely Agree). Items were all coded or reverse-coded and then averaged so that higher scores indicated more positive evaluations of appearance. The scale showed high internal reliability for the overall sample, for men, and for women, respectively (α = 0.93;0.93;0.93).
2.3.2. Multidimensional Body-Self Relations Questionnaire – Overweight Preoccupation Subscale
Participants completed the Overweight Preoccupation subscale of the Multidimensional Body-Self Relations Questionnaire (Brown et al., 1990; Cash, 2000). This scale measures fat anxiety, weight vigilance, dieting, and eating restraint. There are four items, two of which measure thoughts about weight (i.e., “I constantly worry about being or becoming fat;” “I am very conscious of even small changes in my weight”) and two of which measure weight loss dieting attempts (i.e., “I am on a weight loss diet;” “I have tried to lose weight by fasting or going on crash diets”). Responses to the first three questions were recorded on the previously described 5-point Likert scale (1 = Definitely Disagree; 5 = Definitely Agree), whereas the last question was recorded on a different scale (1 = Never, 5 = Very Often). Items were examined individually and averaged into a scale, with higher scores indicating more preoccupation with weight. Good internal reliability was obtained for the overall sample, men, and women, respectively (α = 0.80;0.78;0.79). All of the items were analyzed individually as well.
2.3.3. Body Image Quality of Life Inventory
This 19-item measure assesses participants’ beliefs about how their body image affects their lives (Cash & Fleming, 2002). Participants indicated whether their feelings about their bodies had positive, negative, or no effects on various aspects of their lives, including “My day-to-day emotions,” “How confident I feel in my everyday life,” and “How happy I feel in my everyday life.” Participants responded on a 7-point Likert scale (1 = Very Negative Effect to 7 = Very Positive Effect). Scores on all 19 items were averaged to create a mean scale score. Higher scores indicated more positive effects of one’s body image on quality of life. Items were averaged into a scale, with higher scores indicating more positive effects of body image on quality of life. Internal reliability was high in the overall sample and among men and women (α = 0.96;0.96;0.96).
2.4. Demographic Variables
Participants self-reported their age, height in feet and inches, weight in pounds, sexual orientation, highest level of education, current relationship status, sex, and current U.S state, and race (e.g., 10 options where they could check all that apply; see Table 1 for distribution of commonly reported races).
Using the self-reported height and weight data, we calculated BMI. We then divided participants into the traditional BMI categories used by the CDC: Underweight (14.5–18.49), Normal or Healthy (18.5–24.9), Overweight (25–29.9), Obese I (30–34.9), Obese II (35–39.9), and Obese III (40 and above). We hasten to add that these widely-used categories were chosen as a heuristic so that the BMI results could be compared to existing studies, and do not represent uniform endorsement of the categories by the entire authorship team in terms of semantic accuracy or as clear indicators of a person’s health status (e.g., see Tomiyama, Hunger, Nguyen-Cuu & Wells, 2016). To avoid any stigmatizing effects of these labels, we instead label these BMI groups as Lowest (Underweight), Low (Normal), Medium (Overweight), and High (Obese) BMI groups from this point forward.
2.5. Overview of Data Analytic Approach
2.5.1. Effect Sizes
What is considered a small, moderate, or large effect size can vary dramatically based on the research question of interest. As a very rough guide, Cohen (1988) suggests that effect size d can be interpreted as small (0.20), moderate (0.50), or large (0.80). These values correspond to Pearson’s r correlations of.10,.24, and.37. Ferguson (2009, p. 533) suggested somewhat higher thresholds for what should be considered the “recommended minimum effect size representing a ‘practically’ significant effect for social science data” (d = 0.41; β or r = .20).
With very large sample sizes, it is possible for even miniscule effects to be statistically significant at traditional thresholds (p < .05). Therefore, we note in the tables whether effects were significant at the p < .05. 01, or.001 levels and emphasize effect sizes when presenting and discussing the results with an emphasis on the results significant at the p < .001 level due to the large sample size and multiple statistical comparisons.
For this paper, we elected to highlight statistically significant findings with Cohen’s d values greater than |0.19|, β values greater than |.09|, and percentage differences greater than eight percentage points. We draw particular attention to Cohen’s d values greater than |0.29| and β values greater than |.19|.
2.5.2. Frequency Distributions and Percentages
Consistent with past research, we present frequency distributions showing the percentage of participants falling on different points on the Likert scale to highlight the distribution of low and high body satisfaction across different groups (e.g., Cash & Henry, 1995; Fallon et al., 2014; Frederick & Forbes et al., 2007; Frederick & Kelly et al., 2016; Peplau et al., 2009). For example, we present the percentage of people who systematically are on the “agree” end of the Likert scale when asked if they want their body to look very thin. This strategy of reporting the percentage of people in each group who embrace this attitude maximizes the accessibility of the findings to the lay public, clinicians, and scientists, in conjunction with the more advanced statistical analyses. Additionally, it encourages thinking about differences across groups in terms of not just the central tendencies, but also to the variations of experiences with groups and the overlaps in experiences across groups.
For each of the measures with 5-point scales, we calculated the percentage of people who systematically fell below the midpoint of the Likert scale (Low: mean scores of 1.00–2.74), around the midpoint (Neutral: 2.75–3.25), or systematically above the midpoint (High: 3.26–5.0). For example, the “high appearance evaluation (agree)” category included the participants who systematically agreed that they liked the way they looked, whereas the “low appearance evaluation (disagree)” category included the participants who systematically disagreed that they liked the way they looked. For the 7-point scales, consistent with past research, we used the categories Low (1–3.49), Neutral (3.5–4.5), and High (4.51–7.0). For the body image quality of life measure, low indicates that participants overall reported their body image had a “negative” effect on their quality of life and high indicates that it had a “positive” effect.
2.5.3. Analyses Examining Demographic Predictors of Body Image
We first conducted multiple regression analyses with each of the demographic predictors entered: gender, age, BMI, BMI-squared (curvilinear effect), education, sexual orientation, and race (Tables 2a 2b). The regression analyses allowed us to examine the association of each predictor variable to the outcome with control variables included. For dummy codes, men were coded as 0 (versus women), heterosexuals were coded as 0 (versus gay/lesbian, bisexual, and an “other” category collapsing all other respondents), and Whites were coded as 0 (versus Black, Hispanic, Asian, and an “other” category collapsing all other respondents). The “other” categories were created because each individual response for sexual orientation (e.g., asexual, pansexual, demisexual) and race (e.g., Pacific Islander, Biracial: White-Black) contained small sample sizes. Collapsing them into one category was done only to ensure they were not excluded from the regression analyses via listwise deletion and is not meant to indicate that the “other” category represents a shared overarching psychological construct or identity.
Table 2.
(a) Multiple Regression Analyses Predicting Body Image Outcomes.
| Appearance Evaluation | Overweight Preoccupation | Body Image Quality of Life | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Men | Women | All | Men | Women | All | Men | Women | |
| β | β | β | β | β | β | β | β | β | |
| Gender | −0.13 * ** | – | – | .47 * ** | – | – | −.18 * ** | – | – |
| BMI | −0.50 * ** | −.46 * ** | −.60 * ** | .43 * ** | .49 * ** | .46 * ** | −.32 * ** | −.28 * ** | −0.39 * ** |
| BMI2 | .01 * | −.00 | .08 * ** | −0.09 * ** | −.03 * ** | −.13 * ** | −.01 | .00 | .04 * ** |
| Age | −0.02 * | −.01 | −.01 | −0.10 * ** | −.11 * ** | −.11 * ** | .03 * ** | .01 | .06 * ** |
| Education | .05 * ** | .03 * * | .06 * ** | .03 * * | .05 * * | .02 | .04 * ** | .06 * ** | .03 * * |
| Hispanic | .13 * * | .08 | .20 * * | .08 | .09 | .11 | .20 * ** | .24 * ** | .16 * |
| Black | .46 * ** | .48 * ** | .46 * ** | −0.20 * ** | −.08 | −.27 * ** | .37 * ** | .42 * ** | .35 * ** |
| Asian | −0.21 * ** | −.21 * ** | −.24 * ** | .05 | .10 * | .02 | −.05 | −.06 | −0.07 |
| Other Race | .07 * | .08 | .07 | .01 | .05 | −.02 | .02 | .04 | .00 |
| Gay/Lesbian | −0.13 * * | −.25 * ** | −.04 | .06 | .39 * ** | −.23 * ** | −.26 * ** | −.41 * ** | −0.13 |
| Bisexual | −0.07 * | −.27 * ** | −.00 | −0.01 | .13 | −.06 | −.23 * ** | −.30 * ** | −0.19 * ** |
| Other Orientation | −0.14 * | −.33 * | −.08 | −0.31 * ** | −.16 | −.36 * ** | −.33 * ** | −.33 * | −0.31 * ** |
| Adjusted. R 2 | .26 * ** | .22 * ** | .29 * ** | .18 * ** | .15 * ** | .14 * ** | .13 * ** | .11 * ** | .14 * ** |
| F | 334.7 | 135.4 | 233.2 | 206.6 | 83.0 | 91.9 | 147.4 | 59.1 | 92.9 |
| (b) Multiple Regression Analyses Predicting Body Image Outcomes. | ||||||
|---|---|---|---|---|---|---|
| OP: I Am On A Weight Loss Diet | OP: Try Lose Weight By Fasting/Crash Diets | |||||
| All | Men | Women | All | Men | Women | |
| β | β | β | β | β | β | |
| Gender | .25 * ** | – | – | .35 * ** | – | – |
| BMI | .41 * ** | .44 * ** | .45 * ** | .36 * ** | .39 * ** | .37 * ** |
| BMI2 | −.10 * ** | −.03 * ** | −.14 * ** | −.07 * ** | −.02 * ** | −.07 * ** |
| Age | −.05 * ** | −.07 * ** | −.05 * ** | −.08 * ** | −.10 * ** | −.07 * ** |
| Education | −.04 * ** | .04 * * | .05 * ** | −.01 | .01 | −.01 |
| Hispanic | −.01 | .05 | −.05 | .05 | .05 | .06 |
| Black | −.21 * ** | −.15 * * | −.25 * ** | −.10 * * | −.05 | −.12 * * |
| Asian | .04 | .06 | .05 | .09 * | .14 * * | .04 |
| Other Race | −.06 | .00 | −.10 * | .05 | .01 | .07 |
| Gay/Lesbian | .02 | .20 * * | −.15 * | .06 | .27 * ** | −.11 |
| Bisexual | −.05 | .12 | −.09 * | .01 | .07 | −.01 |
| Other Orientation | −.26 * ** | −.23 | −.26 * * | −.22 * * | .0 | −.28 * * |
| Adjusted. R 2 | .13 * ** | .12 * ** | .13 * ** | .12 * ** | .09 * ** | .10 * ** |
| F | 144.1 | 64.2 | 83.6 | 129.2 | 46.2 | 63.8 |
| df | 12, 11607 | 11, 5281 | 11, 6315 | 12, 11607 | 11, 5281 | 11, 6315 |
| OP: I Constantly Worry About Fat | OP: Very Conscious of Small Changes Weight | |||||
| All | Men | Women | All | Men | Women | |
| β | β | β | β | β | β | |
| Gender | .42 * ** | – | – | .45 * ** | – | – |
| BMI | .41 * ** | .48 * ** | .44 * ** | .17 * ** | .22 * ** | .18 * ** |
| BMI2 | −.08 * ** | −.03 * ** | −.13 * ** | −.05 * ** | −.02 * ** | −.07 * ** |
| Age | −.13 * ** | −.14 * ** | −.15 * ** | −.05 * ** | −.04 * | −.08 * ** |
| Education | .03 * ** | .07 * ** | .02 | .01 | .03 * | .01 |
| Hispanic | .14 * * | .11 | .20 * * | .09 | .05 | .15 * |
| Black | −.21 * ** | −.11 * | −.28 * ** | −.09 * | .07 | −.19 * ** |
| Asian | .13 * * | .15 * * | .13 * | −.09 * | −.03 | −.15 * * |
| Other Race | .04 | .08 | .01 | .01 | .04 | −.02 |
| Gay/Lesbian | .07 | .41 * ** | −.23 * ** | .04 | .33 * ** | −.21 * * |
| Bisexual | .00 | .13 | −.04 | .00 | .08 | −.04 |
| Other Orientation | −.25 * * | −.10 | −.31 * ** | −.24 * * | −.16 | −.29 * * |
| Adjusted. R 2 | .16 * ** | .16 * ** | .13 * ** | .07 * ** | .03 * ** | .03 * ** |
| F | 187.7 | 89.2 | 84.9 | 72.7 | 15.7 | 17.0 |
| df | 12, 11607 | 11, 5281 | 11, 6315 | 12, 11607 | 11, 5281 | 11, 6315 |
Note.
p < .001,
p < .01,
p < .05.
OP: Overweight Preoccupation; BIQLI: Body Image Quality of Life Inventory.
Across all regression analyses, collinearity diagnostics did not identify high degrees of multicollinearity (most VIF values below 2.0, all below 4.5). Regression analyses were conducted first for the whole sample and then separately by gender. All continuous predictor and outcome measures were z-scored prior to the regressions, both for the full sample and then separately within each gender for the gender-specific analyses.
Gender differences in the overall prevalence of low, neutral, and high body image are presented along with t-tests and Cohen’s d comparing mean differences (Table 3). Body mass, racial, age, and sexual orientation differences in the prevalence of poor body image among each gender were examined using descriptive statistics (Table 4), and t-tests and Cohen’s d compared differences between specific racial and sexual orientation groups (Table 5).
Table 3.
Prevalence of Low, Neutral, and High Scores on Body Image Measures.
| Men | Women | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Disagree % | Neutral % | Agree % | M | SD | Disagree % | Neutral % | Agree % | M | SD | Vs. d | |
| Appearance Evaluation | 30 | 13 | 57 | 3.28 | 0.92 | 36 | 13 | 51 | 3.14 | 0.99 | 0.15 * ** |
| Overweight Preoccupation | 62 | 23 | 15 | 2.32 | 0.95 | 45 | 25 | 30 | 2.78 | 1.02 | −0.47 * ** |
| Constantly worry about fat | 53 | 16 | 31 | 2.60 | 1.30 | 37 | 14 | 49 | 3.15 | 1.35 | −0.41 * ** |
| Conscious small change weight | 50 | 16 | 34 | 2.69 | 1.29 | 32 | 13 | 55 | 3.27 | 1.33 | −0.44 * ** |
| I am on a weight loss diet | 69 | 12 | 19 | 2.12 | 1.25 | 59 | 14 | 27 | 2.45 | 1.37 | −0.25 * ** |
| Try lose weight by fasting or crash diets | 75 | 17 | 7 | 1.85 | 1.01 | 63 | 22 | 15 | 2.23 | 1.17 | −0.35 * ** |
| Negative % | None % | Positive % | M | SD | Negative % | None % | Positive % | M | SD | Vs. d | |
| Body Image Quality of Life | 16 | 27 | 57 | 4.66 | 1.15 | 24 | 27 | 49 | 4.43 | 1.24 | 0.19 * ** |
Note.
p < .001,
p < .01,
p < .05.
These two items were not reverse coded for this analysis (e.g., high scores indicate agreeing that I am physically unattractive). Frequency distributions are provided to show the percentage of men and women who scored on the low, neutral, or high end of each body image measure. For example, 30% of men reported low appearance evaluation with responses systematically below the midpoint of the Likert scale (1–2.74 out of 5.0). Means and standard deviations for each sex are presented. Effect size d and statistical significance for differences between men and women are shown in the last column. A positive effect size indicates that men scored higher on the measure than women (e.g., men reported higher appearance evaluation, d =0.15). A negative effect indicates that men scored lower on the measure than women (e.g, men reported lower preoccupation with weight, d = −0.47).
Table 4.
Prevalence of Low Appearance Evaluation, High Weight Preoccupation, and Negative Effects of Body Image.
| White % | Hispanic % | Black % | Asian % | Lowest BMI % | Low BMI % | Medium BMI % | High BMI I % | High BMI II % | High BMI III % | |
|---|---|---|---|---|---|---|---|---|---|---|
| Low Appearance Evaluation | 32 (39) | 27 (25) | 15 (26) | 26 (31) | 27 (22) | 16 (15) | 22 (37) | 52 (59) | 68 (70) | 84 (75) |
| High Overweight Preoccupation | 15 (31) | 19 (35) | 13 (25) | 13 (27) | 05 (12) | 08 (19) | 15 (33) | 24 (44) | 30 (48) | 31 (45) |
| Constantly worry about fat | 31 (49) | 36 (63) | 28 (42) | 31 (48) | 13 (25) | 18 (37) | 32 (53) | 46 (62) | 57 (66) | 60 (64) |
| Conscious small change weight | 34 (56) | 35 (62) | 39 (50) | 31 (46) | 28 (41) | 28 (51) | 36 (59) | 41 (59) | 38 (56) | 42 (57) |
| I am on a weight loss diet | 19 (28) | 19 (26) | 14 (22) | 15 (23) | 05 (10) | 08 (15) | 20 (32) | 29 (42) | 35 (42) | 38 (42) |
| Try lose weight fasting/crash diets | 07 (15) | 10 (17) | 08 (12) | 08 (11) | 05 (06) | 04 (09) | 07 (14) | 11 (21) | 17 (26) | 15 (29) |
| Negative Body Image Quality Life | 17 (25) | 10 (20) | 10 (21) | 15 (18) | 14 (24) | 10 (11) | 11 (23) | 27 (37) | 39 (47) | 49 (49) |
| Hetero. % | Gay/Les % | Bisexual % | Other % | 18–24 % | 25–29 % | 30–39 % | 40–49 % | 50–65 % | ||
| Low Appearance Evaluation | 29 (36) | 39 (37) | 40 (39) | − (44) | 24 (32) | 30 (31) | 29 (39) | 35 (39) | 34 (42) | |
| High Overweight Preoccupation | 15 (30) | 24 (25) | 20 (34) | − (18) | 15 (31) | 18 (31) | 15 (32) | 15 (28) | 09 (27) | |
| Constantly worry about fat | 30 (49) | 52 (40) | 38 (53) | − (38) | 32 (53) | 33 (51) | 32 (50) | 34 (47) | 20 (42) | |
| Conscious small change weight | 33 (55) | 48 (48) | 35 (56) | − (45) | 32 (54) | 34 (57) | 35 (56) | 36 (51) | 29 (54) | |
| I am on a weight loss diet | 18 (28) | 27 (21) | 24 (27) | − (21) | 17 (24) | 19 (25) | 19 (30) | 20 (28) | 19 (28) | |
| Try lose weight fasting/crash diets | 07 (15) | 12 (12) | 09 (14) | − (14) | 07 (17) | 10 (15) | 07 (15) | 06 (14) | 03 (11) | |
| Negative Body Image Quality Life | 15 (23) | 30 (25) | 24 (31) | − (30) | 14 (25) | 15 (22) | 16 (25) | 23 (25) | 17 (23) |
Note. The first number indicates the percentage of men with poor body image and the number in parentheses represents women (e.g., “low” appearance evaluation, 1.00–2.74; “high” overweight preoccupation, 3.26–5.00; “low” body image quality of life, 1.00–3.49). For example, 32% of White men (and 39% of White women) reported overall low appearance evaluation. Data is shown for cells with at least 40 participants.
Table 5.
Racial and Sexual Orientation Differences in Body Image Outcomes.
| Appearance Evaluation | Overweight Preoccupation | Body Image Quality of Life | ||||
|---|---|---|---|---|---|---|
| Men | Women | Men | Women | Men | Women | |
| Race | ||||||
| White M (SD) | 3.24 (0.92) | 3.09 (0.99) | 2.32 (0.95) | 2.80 (1.02) | 4.60 (1.15) | 4.38 (1.22) |
| Hispanic M (SD) | 3.34 (0.89) | 3.35 (0.98) | 2.40 (0.98) | 2.92 (1.01) | 4.89 (1.13) | 4.59 (1.21) |
| Black M (SD) | 3.69 (0.88) | 3.46 (1.04) | 2.24 (0.91) | 2.61 (1.04) | 5.09 (1.18) | 4.73 (1.35) |
| Asian M (SD) | 3.30 (0.85) | 3.27 (0.92) | 2.25 (0.92) | 2.60 (1.05) | 4.75 (1.06) | 4.60 (1.24) |
| Racial Comparisons White vs. Hispanic d | −0.11 | −0.26 * ** | −0.08 | −0.12 | −0.25 * ** | −0.17 * |
| White vs. Black d | −0.49 * ** | −0.37 * ** | 0.08 | 0.19 * ** | −0.43 * ** | −0.28 * ** |
| White vs. Asian d | −0.07 | −0.18 * * | 0.07 | 0.20 * ** | −0.13 * | −0.18 * * |
| Hispanic vs. Black d | −0.40 * ** | −0.11 | 0.17 * | 0.30 * ** | −0.17 * | −0.11 |
| Hispanic vs. Asian d | 0.05 | 0.08 | 0.16 * | 0.31 * ** | 0.13 | −0.01 |
| Black vs. Asian d | 0.45 * ** | 0.19 * * | −0.01 | 0.01 | 0.30 * ** | 0.10 |
| Sexual Orientation | ||||||
| Heterosexual M (SD) | 3.30 (0.91) | 3.15 (0.99) | 2.30 (0.94) | 2.78 (1.02) | 4.69 (1.14) | 4.48 (1.24) |
| Gay/Lesbian M (SD) | 3.09 (0.99) | 3.08 (1.00) | 2.66 (0.99) | 2.60 (1.03) | 4.22 (1.19) | 4.27 (1.10) |
| Bisexual M (SD) | 3.00 (0.95) | 3.06 (1.00) | 2.45 (0.99) | 2.84 (1.04) | 4.27 (1.15) | 4.11 (1.20) |
| Sexual Orientation Comparisons Heterosexual vs. Gay/Lesbian d | 0.23 * * | 0.07 | −0.38 * ** | 0.18 * | 0.41 * ** | 0.17 * |
| Heterosexual vs. Bisexual d | 0.33 * ** | 0.09 * | −0.16 * | −0.06 | 0.37 * ** | 0.30 * ** |
| Gay/Lesbian vs. Bisexual d | 0.09 | 0.02 | 0.21 * | −0.23 * * | −0.04 | 0.14 |
Note.
p < .001,
p < .01,
p < .05.
Means and standard deviations for each group are presented. Effect size d and statistical significance for differences between each group are shown. A positive effect size indicates that the first group listed scored higher than the second group (e.g., Black men reported higher appearance evaluation than White men, d =0.45). A negative effect size indicates the first group listed scored lower than the second group listed (White men reported lower overall appearance evaluation than Black men, d = −0.49).
3. Results
3.1. Gender Differences in Body Image (Hypothesis 1)
We hypothesized that women would be more likely than men to report poor body image. In regression analyses, women reported lower appearance evaluation (β = −.13), lower body image quality of life (β = −.18), and higher overweight preoccupation (β = .47) than men when controlling for other demographic variables in the model (Table 2a). Fewer than half of men and women reported overall low appearance evaluation (30% men vs. 36% women), negative effects of body image on quality of life (16% men vs. 24% women), and high preoccupation with weight (15% men vs. 30% women). Encouragingly, a majority or near majority of men and women reported high appearance evaluation (57% men vs. 51% women), low overweight preoccupation (62% men vs. 45% women), and positive effects of body image on their quality of life (57% men vs. 49% women) (Table 3).
The absolute level of body dissatisfaction varied notably across some individual items from the same validated measures and revealed interesting patterns (Table 3). Analyses of individual items revealed that men reported lower overweight preoccupation than women on all four items in the overweight preoccupation scale (ds = |0.25–0.44|). For example, approximately half of women endorsed overweight preoccupation cognitions (49–55% of women), but far fewer reported engaging in overweight preoccupation behaviors such as dieting and fasting (15–27% of women). Men were also more likely to report these cognitions (31–34%) than engaging in the behaviors (7–19%).
3.2. BMI Differences in Body Image Among Men and Women (Hypothesis 2)
We hypothesized that people with higher body mass would report poorer body image than people with lower body mass. For both men and women, there was a strong linear association of BMI to appearance evaluation, overweight preoccupation, body image quality of life, and individual items from these scales, with almost all βs exceeding |.20|. There were also weak curvilinear associations in some analyses, with all βs < |.15| (Tables 2a and 2b).
These associations are visually apparent Figs. 1–3, and they allow us to identify the BMI ranges where positive versus negative body image are common. As shown on Fig. 1, high appearance evaluation was reported by the majority of women with BMIs 17–27 and men with BMIs 17–31. However, low appearance evaluation was reported by the majority of women with BMIs above 31 and among men with BMIs above 32. As shown in Fig. 2, high overweight preoccupation was reported by over a quarter of women with BMIs above 27 and men with BMIs above 34. As shown in Fig. 3, overall negative effects of body image on quality of life were reported by over one-fourth of women with BMIs above 29 and men with BMIs above 32. Overall positive effects of body image on quality of life were reported by over half of women with BMIs 19–27 and men with BMIs 18–31.
Fig. 1. The Percentage of Men and Women Reporting Low or High Appearance Evaluation By BMI.
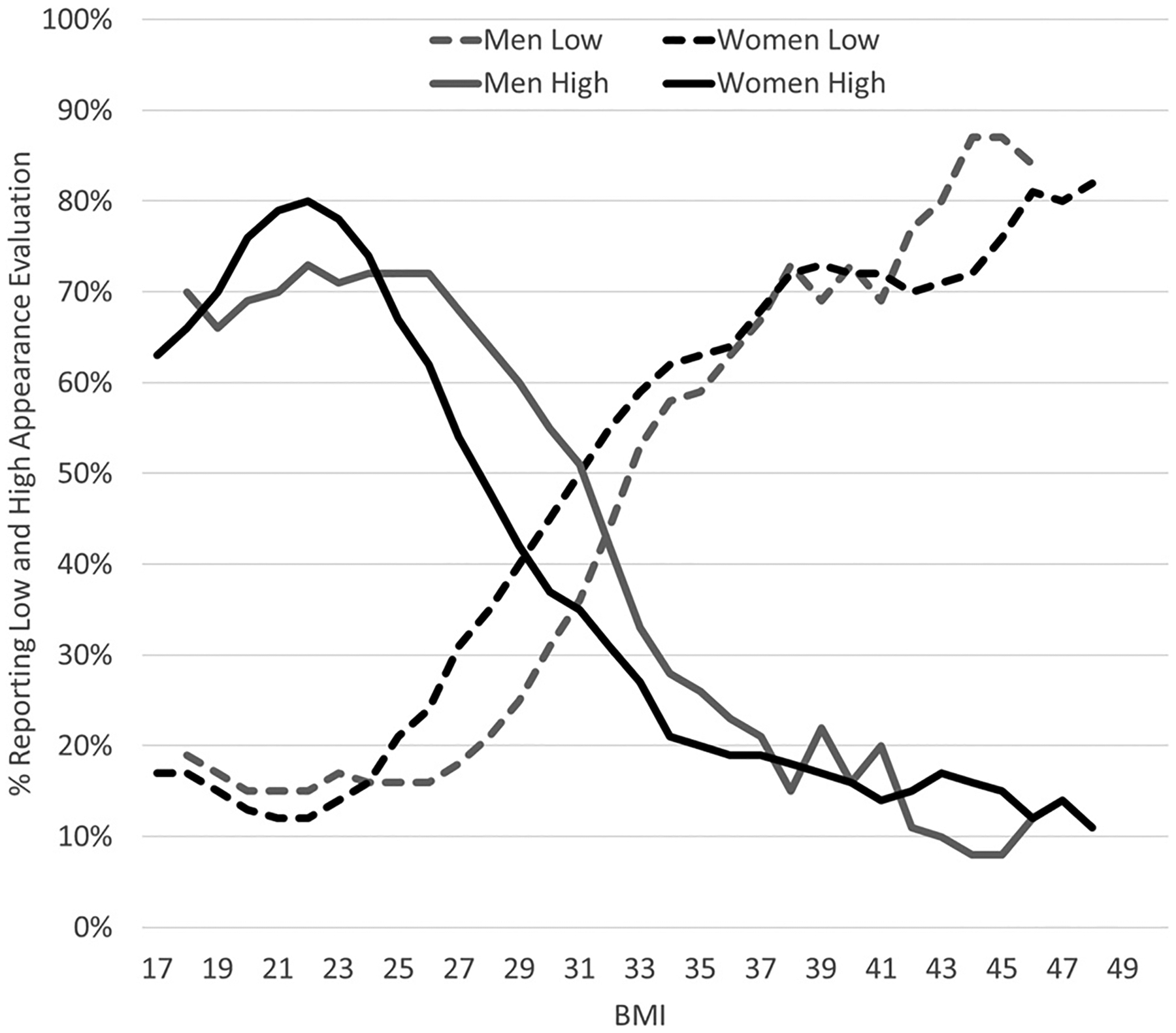
Note. The darker lines represent women and the lighter lines represent men. BMI was strongly associated with likelihood of reporting low (1.00–2.74) and high (3.26–5.00) appearance evaluation on the Likert scale. High appearance evaluation was reported by a majority of women with BMIs 17–27 and men with BMIs 17–31. Low appearance evaluation was reported by a majority of women with BMIs above 31 and men with BMIs above 32. The values represent moving averages. Only cells with at least 20 participants are plotted.
Fig. 3. The Percentage of Men and Women Reporting Low or High Body Image Quality of Life By BMI.
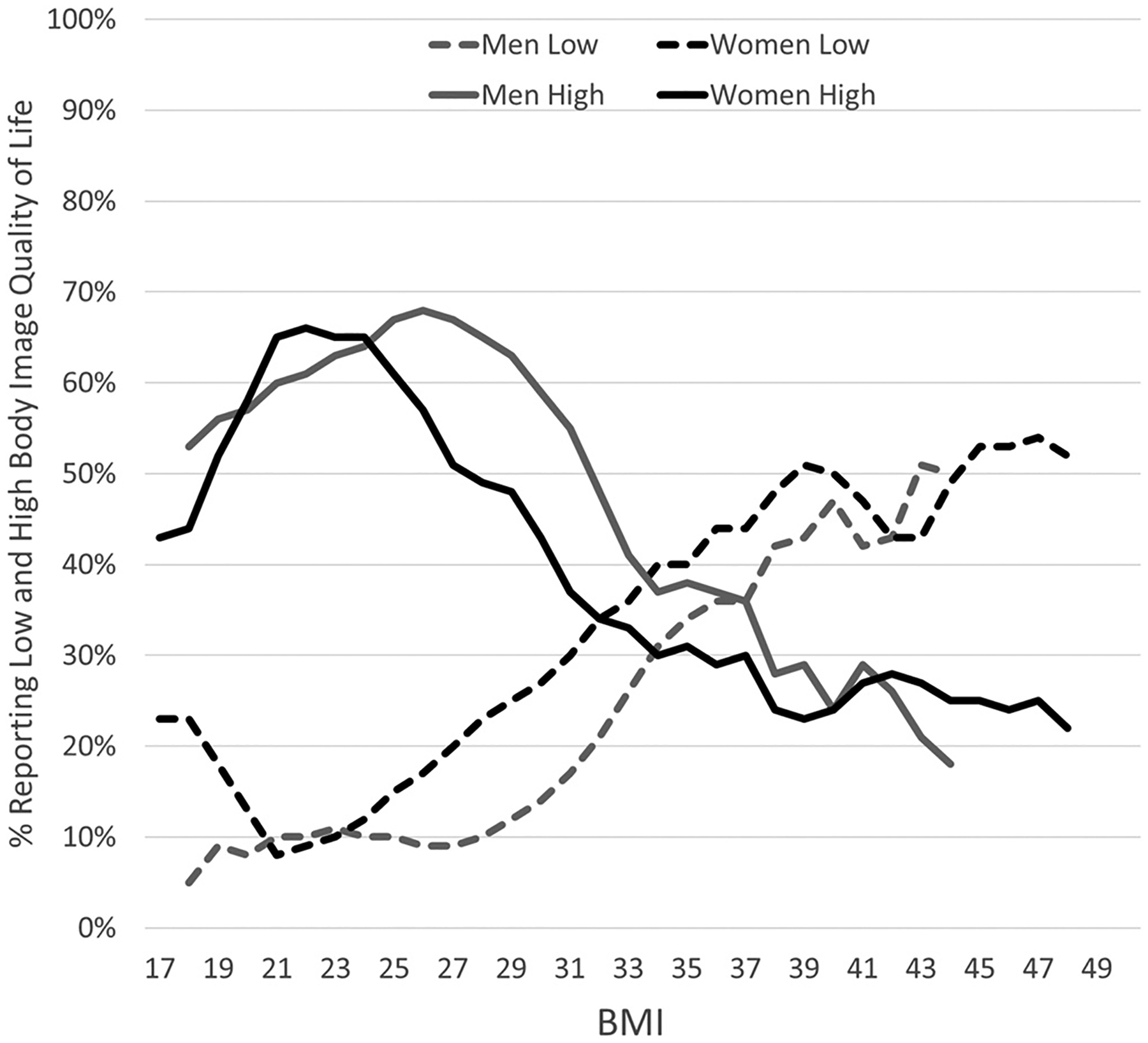
Note. The darker lines represent women and the lighter lines represent men. BMI was strongly associated with likelihood of reporting negative (low: 1.00–3.49) and positive (high: 4.51–7.00) effects of body image on quality of life on the Likert scale. Overall negative effects of body image were reported by over one-fourth of women with BMIs above 29 and men with BMIs above 32. Overall positive effects of body image were reported by over half of women with BMIs 19–27 and men with BMIs 18–31. The values represent moving averages. Only cells with at least 20 participants are plotted.
Fig. 2. The Percentage of Men and Women Reporting Low or High Overweight Preoccupation By BMI.
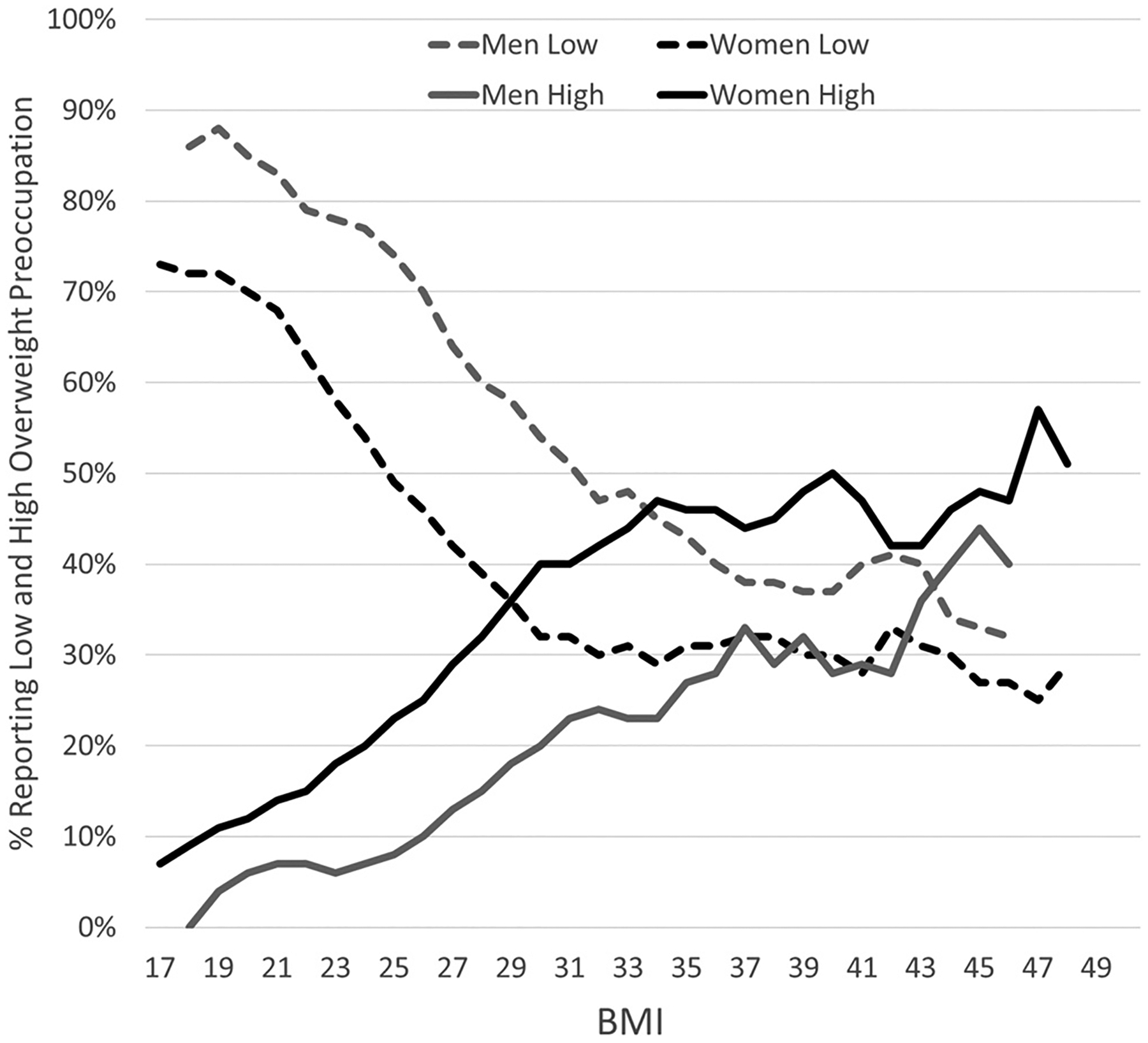
Note. The darker lines represent women and the lighter lines represent men. BMI was strongly associated with likelihood of reporting low (1.00–2.74) and high (3.26–5.00) overweight preoccupation on the Likert scale. High overweight preoccupation was reported by over one-fourth of women of women with BMIs above 27 and men with BMIs above 34. The values represent moving averages. Only cells with at least 20 participants are plotted.
The links between BMI and body image were immediately apparent when looking across the BMI categories used by the CDC. As shown in Table 4, only 16% of men and 15% of women classified as normal weight reported overall low appearance evaluation, compared to 52% and 59% of men and women classified as High BMI I. Similarly, only 10% of men and 11% of women classified as normal weight reported overall low appearance evaluation, compared to 27% and 37% of men and women classified as High BMI I. Despite being classified as Low BMI, 8% of men and 19% of women reported high overweight preoccupation, compared to 24% and 44% of men and women classified as High BMI I.
3.3. Racial Differences in Body Image Among Men and Women (Hypothesis 3)
We hypothesized that Asian men and women would report the poorest body image, and Black men and women would report the highest body image. Consistent with past meta-analyses, in regression analyses, Black women reported better body image than White women, including higher appearance evaluation (βs =0.46), lower overweight preoccupation (β = −.27), and higher body image quality of life (β = .35). Black men reported higher appearance evaluation (βs =0.48), higher body image quality of life (β = .42), but not lower overweight preoccupation (β = 0.08). Hispanic participants did not consistently differ from Whites, but when there was a difference, it was in the direction of Hispanics reporting better body image than Whites. Compared to White men and women, Asian men and women reported lower appearance evaluation (βs = −0.21 men, −0.24 women), but not lower body image quality of life, and only Asian men tended towards reporting greater overweight preoccupation (β = .10).
The links between race and body image are evident when looking at the frequency distributions. As shown in Table 4, low appearance evaluation was reported by only 15% of Black men compared to 26%– 32% of other race groups. Both White men (32%) and women (39%) reported higher prevalence rates of low appearance evaluation compared to the other groups. More Hispanic men (19%) and women (35%) reported high overweight preoccupation compared to the other groups. White women (25%) were more likely than other groups to report negative body image, and more White men (17%) indicated more negative body image quality of life compared to Hispanic (10%) and Black men (10%).
In multiple regression analyses (see Tables 2a and 2b), Black men and women reported more appearance evaluation body image concerns, and less overweight preoccupation and worry about fat compared to White individuals. Hispanic women also reported significantly greater appearance evaluation, body image quality of life, worry about fat, and being very conscious of even small weight changes. Hispanic men reported more positive body image quality of life when compared to White men.
Asian men and women also reported lower appearance evaluation and more constant worry about fat than White participants. These differences are also apparent when examining racial differences without covariates (see Table 5). When not considering covariates, Asian women reported greater appearance evaluation than White women, and Asian men did not differ from Whites. Once covariates such as BMI are included in regression models, the patterns flip to Asian men and women reporting lower appearance evaluation than White men and women (β = −0.21; −0.24).
3.4. Age Differences in Body Image Among Men and Women (Hypothesis 4)
We hypothesized that age would be unrelated or only weakly related to body image. In regression analyses (see Table 2a–b), age was not strongly associated with appearance evaluation and body image quality of life measures or the individual items we highlighted (βs < 0.10). Older men and women were less likely to report overweight preoccupation (βs = −0.11 men, −0.11 women), and the only item that exceeded βs = |.10| was that older men and women were less likely to constantly worry about fat (βs = −0.14 men, −0.15 women).
As shown in Table 4, without controls for covariates with age such as body mass, the prevalence of low appearance evaluation increased with age for men, ranging from 24% for 18–24 year-old men to 34% for 50–65 year-old men. A similar pattern observed for women, with rates ranging from 32% for women aged 18–24 years to 42% of women aged of 50–65 years. Rates of high overweight preoccupation were greater among younger versus older men (15% younger men vs. 9% older men) and younger versus older women (31% younger women vs. 27% women), although percentages were consistently higher for women than men across all age ranges. Similar trends were observed for items pertaining to constant worry about fat, current dieting, and trying to lose weight via fasting or crash dieting.
3.5. Sexual Orientation Differences in Body Image Among Men and Women (Hypothesis 5)
We hypothesized that sexual minority men would report poorer body image than heterosexual men, and that there would be no differences or negligible differences among women. Consistent with previous research, compared to heterosexual men, regression analyses revealed that gay men reported lower appearance evaluation (β = −0.25) and body image quality of life (β = −0.41), and higher overweight preoccupation (β = 0.39). Gay men also reported poorer body image on every individual item (βs = |.17 to.41|; Tables 2a–2b). Compared to heterosexual men, bisexual men reported lower appearance evaluation (β = −0.27) and body image quality of life (β = −0.30), but not significantly higher overweight preoccupation (β = 0.13). Consistent with this pattern, mean comparisons without controlling for covariates revealed small to medium effect size differences between gay and heterosexual men on appearance evaluation, overweight preoccupation, and body image quality of life, and between bisexual and heterosexual men on appearance evaluation and body image quality of life (Table 5).
The patterns identified in the regressions were apparent in the frequency distributions (see Table 4). More gay men (39%) and bisexual men (40%) reported low appearance evaluation compared to 29% of heterosexual men. Similarly, 30% of gay men and 24% of bi-sexual men reported low body image quality of life compared to only 15% of heterosexual men. High overweight preoccupation was reported by 24% of gay men and 20% of bisexual men, versus 15% of heterosexual men. Of interest, however, was that constantly worrying about fat and being conscious about small changes in weight were substantially higher among gay men (52% worry, 48% conscious) than among heterosexual men (30% worry, 33% conscious) and bisexual men (38% worry, 35% conscious).
In regression models, compared to heterosexual women, lesbian women reported lower overweight preoccupation (β = −0.23), and bisexual women reported lower body image quality of life (β = −0.19), but they did not differ on the other measures (see Table 2a–b). In mean comparisons, bisexual women demonstrated a small to moderate effect size difference on body image quality of life compared to heterosexual women (see Table 5). Looking at the frequency distributions, minimal differences were observed across sexual orientations among women in appearance evaluation (36–39%), overweight preoccupation (25–30%), and body image quality of life (23–31%).
4. Discussion
4.1. Summary of Key Findings
This study evaluated how gender, BMI, race, age, and sexual orientation were related to appearance evaluation, overweight preoccupation, and body image quality of life in a large U.S. national sample. Results for gender were consistent with previous research finding slightly to moderately higher body image concerns in women compared to men (e.g., Fallon et al., 2014; Frederick et al., 2016, 2020). These gender differences are also consistent with sociocultural theories, including objectification theory (Fredrickson & Roberts, 1997) and the tripartite theory of body image and eating disturbance (Thompson et al., 1999), highlighting that intense and disproportionate pressures for women from media, potential partners, family, and friends to pursue a thin body may lead them to internalize and adopt these pressures, leading to body dissatisfaction. However, the gap between these cultural pressures for women and men may be narrowing in recent years, and research also supports the application of these social pressures and the tripartite theory in men (Tylka, 2011).
Results regarding BMI are consistent with previous research showing strong links between body image-related quality of life and BMI (Fallon et al., 2014; Frederick et al., 2020; Frederick, Lever, & Peplau, 2007; Frederick, Sandhu, et al., 2016; Peplau et al., 2009). There are likely several routes through which BMI is related to body image. Having a higher BMI may put greater stress on joints as people age, leading to more physical pain, leading to poorer body image and negative impacts of body image people’s daily emotions and quality of life. Much of the link between BMI and body image, however, is likely mediated through internalization of the thin-ideal and weight-based stigma from others. There is pervasive weight-based stigma and fat-phobia in the United States (Puhl et al., 2008), which can render harmful effects on mental health and well-being (Tomiyama, 2014). This may be compounded by the fact that the overvaluation of thinness is prevalent in industrialized, Western countries (Swami et al., 2010).
In terms of race, White women reported greater body image concerns compared to racial minority groups when covariates were not included. The largest of these effects, however, was small-to-moderate, which aligns with previous meta-analyses supporting minimal differences in body satisfaction among White, Black, Hispanic, and Asian American women in the United States (Grabe & Hyde, 2006). Black men reported higher appearance evaluation than the four other groups and the effect sizes were moderate. Black men also reported higher body image quality of life than White men. All other racial differences were small. Of note, the measures included within the present study were developed and evaluated in populations of predominantly White participants and thus, results should be interpreted within this context. The small racial differences observed in overall body image, however, do not necessarily indicate that the factors contributing to body (dis)satisfaction are the same for each group. For example, experiences of appearance-based discrimination due to skin color and other phenotypic features likely vary across races, genders, and the intersection between these identities (Cole, 2009; Burke et al., 2020).
However, our findings relating to race highlight the importance of including covariates when comparing appearance evaluation among Asian and White women. Without controlling for personal characteristics such as BMI, White women reported lower appearance evaluation than Asian women. When controlling for these characteristics, however, the pattern reversed, with Asian women reporting lower appearance evaluation. Previous research on how race and gender intersect with experiences of oppression, sexism, and racism for Asian American women (Brady, Kaya, Iwamoto, Park, Fox & Moorhead, 2017) suggests that factors contributing to these observed differences may include satisfaction with facial appearance (Frederick, Kelly, et al., 2016), including eye size (Brady et al., 2017), skin tone (Brady et al., 2017) and breast size (Forbes & Frederick, 2008). It will be important for future research to measure these body image concerns and how body image may be linked to experiences of racism when comparing White and Asian women.
Regarding age, results support that even the strongest associations between age and body image were relatively small, consistent with past cross-sectional age cohort research (Tiggemann, 2004; Frederick et al., 2020; Frederick & Sandhu et al., 2016). Thus, overall, body image concerns appear relatively stable across age cohorts from 18 to 65, with some differences supporting a trend towards individuals in midlife reported less concerns regarding their bodies. While this could be consistent with the premise that across genders individuals may become more accepting of their bodies as they age (Forrester-Knauss & Stutz, 2012; Hughes et al., 2016), the cross-sectional cohort design and small to negligible effects observed limit the conclusions that can be drawn in this manner.
The small to moderate effect size differences between gay men and heterosexual men are consistent with previous research demonstrating higher body image concerns for sexual minority men (Brown & Keel, 2012; Frederick & Essayli, 2016; Morrison et al., 2004; Peplau et al., 2009). These differences for men may reflect the influence of sexual minority stress from being part of a marginalized group and/or sociocultural pressures from media, friends, family, partners, and within the sexual minority male community (Meyer, 1995; Tylka & Andorka, 2012). Also consistent with previous research (Moore & Keel, 2003; Moreno-Dominguez et al., 2019; Morrison et al., 2004; Frederick et al., 2020; Frederick, Lever, & Peplau, 2007; Frederick, Sandhu, et al., 2016; Peplau et al., 2009), almost all differences among lesbian, bisexual, and heterosexual women were small and/or not statistically significant. These findings indicate relatively similar levels of body image concerns among lesbian, bisexual, and heterosexual women, but do not necessarily indicate that the factors contributing to these overall levels of body image are identical across the groups. The pathways that lead to body dissatisfaction and how these may differ for lesbian, bisexual, and heterosexual women require further exploration.
Finally, presenting the results for individual items revealed some interesting results. Overweight preoccupation cognitions were endorsed more frequently than were overweight preoccupation behaviors. Despite the fact that the measure shows high internal reliability, averaging these cognitions and behaviors into the same scale into one mean score obscures these differences between cognitions and behaviors. The item-by-item analyses highlights the importance of considering the extent to which there are demographic differences in degree of endorsement across items within a scale.
4.2. Strengths and Limitations
The present study benefited from several strengths including a diverse, large, national sample of men and women across a broad range of ages, sexual orientations, race, and body masses. To our knowledge, this represents the largest national study of body image using validated multi-item measures.
However, with these strengths there are also limitations of note. First, while this study used a national sample with participants drawn from all 50 states, it was not a nationally representative or national probability sample. For example, people with a college degree were overrepresented in the sample relative to the national population. The sample was drawn from Mechanical Turk, which may limit the generalizability of the sample. Conducting comparisons with nationally representative samples could help mitigate this concern. Additionally, all measures were trait-based and taken at one time point, even though body image satisfaction is known to have state components that can vary moment-to-moment and day-to-day (Colautti, Fuller-Tyszkiewicz, Skouteris, McCabe, Blackburn & Wyett, 2011).
Of note, the topic of the survey was not revealed in the survey description, minimizing concerns regarding self-selection into the study by people with heightened body image concerns. While the inclusion of body image quality of life items is a strength, it is possible that potential comorbidities that may lead to body image concerns, such as depression, may have influenced responses. These comorbidities limit conclusions regarding whether body image may be the primary concern impacting functioning for all assessed. Additionally, results from the present study are descriptive and cross-sectional, and therefore no causal or temporal associations can be inferred. Longitudinal studies are needed to better understand the relationships between age and body image.
While the sample benefited from assessing sexual orientation, we were not able to examine body image concerns across gender identities, including transgender, gender nonconforming, or non-binary individuals. Body mass index was based on self-reported height and weight, and therefore it is very likely that the link between BMI and body image is not precisely identified due to some degree of measurement error. Additionally, BMI as a metric itself is not without criticism (Gutin, 2018; Nuttall, 2015), meaning that results using this measure should be interpreted with this in mind.
Although the racial diversity of the sample was a strength, sample sizes only permitted comparison of White, Black, Hispanic, and Asian racial groups, limiting the ability to explore body image concerns among groups outside of these categories. While the present study was able to examine the intersection variations within each gender (e.g., racial differences in body image among men), we did not have the sample size to examine more nuanced relationships between multiple social identities that may affect body image (e.g., crossing between gender, sexual orientation, and race), which will be a critical future direction for body image research how the intersections of identities and social factors impact people’s experiences. Additionally, the level of acculturation was not assessed, which prevents a more in depth understanding of associations between racial background and body dissatisfaction. Given the diverse identities of participants in the present study, it is possible that participants may have responded to the same questions in distinct ways based on their demographics and lived experiences, which may impact our ability to draw conclusions across groups. Partially mitigating this concern, concurrent research using the same sample as in the present study supports that the body image measures used demonstrate measurement invariance across gender, sexual orientation, race, and weight status (Frederick, Hazzard, Schaefer, Thompson, et al., 2022). However, it is still plausible that differential responding across participants may have impacted the results.
4.3. Clinical and Public Health Implications
This study has potential implications for both body image assessment and intervention and adds to the evidence base for identifying patterns of body image-related concerns and related mental and physical health impacts. A prominent theoretical model for the development of eating disorders and disordered eating purports sociocultural factors influence body image and eating disturbances (Ata et al., 2015). Thus, as sociocultural factors change, large scale, nationally representative studies need to be regularly conducted to examine cultural trends in putative risk factors for eating disorders. Multiple studies are needed at any given time point because estimates can vary due to sampling error and variation in methods across studies.
While large, national studies can provide helpful information on cultural trends and patterns, it is also important to consider where the boundary is placed in terms of deciding what constitutes a clinically-meaningful effect in large-scale survey studies. It is important that researchers consider how we use this information to make decisions with regards to directing preventative or intervention efforts to ensure we are not overinterpreting our data. The widespread prevalence of body dissatisfaction within the present study is notable and begs consideration regarding whether these data reflect the phenomena of “normative discontent,” (Rodin et al., 1984; Tantleff-Dunn et al., 2011) or to levels of body dissatisfaction that impair daily functioning. Considering factors like replication across different samples and studies may be helpful to ensure responsible data interpretation.
The current study provides insights into health disparities across different demographic groups. One concern raised with focusing on group differences is that it can obscure variation within each group. For example, it can be easy for relative difference (men reported higher body satisfaction than women) to be encoded in people’s minds as a categorical difference (men are satisfied, women are dissatisfied), causing them to view people on the basis of their category membership rather than their own individual needs and experiences. To help address this concern, we have used truncated frequency distributions to highlight the variability of experiences within each demographic group as well. For example, many men and women report low appearance evaluation, but many men and women also report high appearance evaluation. While keeping this variability within each group in mind, the purpose of this paper was to identify groups that have elevated risks for body dissatisfaction. This can lead to examination of what factors might underly this elevated risk that could be targeted. For example, the pressures on gay men who have poor body image may differ on average from the pressures on heterosexual men who have poor body image, whose pressures differ from heterosexual women. These heightened or different pressures are valuable for clinicians to keep in mind when interacting with people with one or more risk factor for body dissatisfaction.
While caution should be employed in deriving clinical implications from cross-sectional research, results from the present study align with recent research on body image interventions in specific demographic groups. Within the present study, limited differences in body dissatisfaction across age coincide with recent research supporting importance of programs promoting a healthy body image are relevant across the lifespan (Lewis-Smith et al., 2016). Given that the present study and previous research support elevated rates of body dissatisfaction in sexual minority men, developing body image programming specific to this population’s unique needs may be useful and has shown initial promise (Brown & Keel, 2015).
While media literacy interventions have found some support (McLean, Wertheim, Marques & Paxton, 2019; Rodgers et al., 2018), interventions involving the addition of warning labels to popular media have generally not been effective in promoting enhanced body image (Danthinne et al., 2020). Exposure to media messages emphasizing that high body mass is not inherently dangerous, uncontrollable, and/or unacceptable to stigmatize have been effective in reducing anti-fat prejudice compared to messages framing high body mass as dangerous, controllable, and/or acceptable to stigmatize (Frederick, Saguy, & Gruys, 2016; Frederick, Saguy, Sandhu & Mann, 2016; Frederick, Tomiyama, et al., 2020; Saguy et al., 2014). Scaling down to the individual level, physical activity, such as participation in yoga, can be beneficial in promoting improved body image (Borden & Cook-Cottone, 2020; Cox, Ullrich-French, Cook-Cottone, Tylka & Neumark-Sztainer, 2020; Halliwell, Jarman, Tylka & Slater, 2018).
4.4. Conclusions
A key finding from this study is that no demographic group was immune to negative body image. We suggest that a critical next step in body image research is to examine the sociocultural pressures that shape body image satisfaction in these groups, and to specifically design measures that assess body image concerns that may vary across these groups, such as concern with hair and skin tone (Harper & Choma, 2019), as well as facial features (Frederick & Kelly et al., 2016). The one demographic factor that was strongly related to body image was weight status (body mass), with many Medium and High BMI men and women expressing body image dissatisfaction – a topic that should continue to be investigated in future research.
Identifying factors that promote body satisfaction is critical because of its link to better mental health, higher self-esteem, and engagement in fewer unhealthy dieting behaviors, and more positive health-related behaviors (Gillen, 2015). Encouragingly, some proportion of every demographic group reported satisfaction with their appearance, and across the High BMI range, 20%– 40% of men and women reported that their feelings about their body had a positive effect on their quality of life. Our findings underscore the importance of identifying the factors that enable some people to maintain positive body image (Tylka & Wood-Barcalow, 2015; Wood-Barcalow et al., 2010) and greater body appreciation (Alleva, Paraskeva, Craddock & Diedrichs, 2018; Homan & Tylka, 2018).
Funding
This research was supported by the National Institute of General Medical Science (1P20GM134969-01A1), and the Kay Family Foundation Data Analytic Grant. 201920202021.
Footnotes
CRediT authorship contribution statement
The first author completed the conceptualization and methodology. The second author took the lead on writing and data analyses. All authors engaged in the writing, and made suggestions for interpreting and enhancing the formal analysis. Along with the first author, the last authors engaged in supervision. The first author was primarily involved with funding acquisition (grant PI), along with the second to last author (grant CO-PI).
Declaration of Competing Interest
There are no conflicts of interest.
References
- Alleva JM, Paraskeva N, Craddock N, & Diedrichs PC (2018). Body appreciation in British men: Correlates and variation across sexual orientation. Body Image, 27, 169–178. 10.1016/j.bodyim.2018.09.004 [DOI] [PubMed] [Google Scholar]
- Ata RN, Schaefer LM, & Thompson JK (2015). Sociocultural theories of eating disorders. In Smolak L, & Levine MP (Eds.). The Wiley handbook of eating disorders: Assessment, prevention, treatment, policy and future directions. New York, NY: John Wiley & Sons Ltd. [Google Scholar]
- Banfield SS, & McCabe MP (2002). An evaluation of the construct of body image. Adolescence, 37, 373–393. [PubMed] [Google Scholar]
- Berinsky AJ, Huber GA, & Lenz GS (2012). Evaluating online labor markets for experimental research: Amazon. com’s Mechanical Turk. Political Analysis, 20, 351–368. 10.1093/pan/mpr057 [DOI] [Google Scholar]
- Berscheid E, Hatfield [Walster] E, & Bohrnstedt G (1973). The Happy American Body: A survey report. Psychology Today, 7, 119–131. [Google Scholar]
- Borden A, & Cook-Cottone C (2020). Yoga and eating disorder prevention and treatment: A comprehensive review and meta-analysis. Eating Disorders, 28, 400–437. 10.1080/10640266.2020.1798172 [DOI] [PubMed] [Google Scholar]
- Brady JL, Kaya A, Iwamoto D, Park A, Fox L, & Moorhead M (2017). Asian American women’s body image experiences: A qualitative intersectionality study. Psychology of Women Quarterly, 41, 479–496. 10.1177/0361684317725311 [DOI] [Google Scholar]
- Brown TA, Cash TF, & Mikulka PJ (1990). Attitudinal body-image assessment: Factor analysis of the Body-Self Relations Questionnaire. Journal of Personality Assessment, 55, 135–144. 10.1080/00223891.1990.9674053 [DOI] [PubMed] [Google Scholar]
- Brown TA, & Keel PK (2012). The impact of relationships on the association between sexual orientation and disordered eating in men. International Journal of Eating Disorders, 45, 792–799. 10.1002/eat.22013 [DOI] [PubMed] [Google Scholar]
- Brown TA, & Keel PK (2015). A randomized controlled trial of a peer co-led dissonance- based eating disorder prevention program for gay men. Behaviour Research and Therapy, 74, 1–10. 10.1016/j.brat.2015.08.008 [DOI] [PubMed] [Google Scholar]
- Bucchianeri MM, Arikian AJ, Hannan PJ, Eisenberg ME, & Neumark-Sztainer D (2013). Body dissatisfaction from adolescence to young adulthood: Findings from a 10-year longitudinal study. Body Image, 10, 1–7. 10.1016/j.bodyim.2012.09.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buhrmester M, Kwang T, & Gosling SD (2011). Amazon’s Mechanical Turk: A new source of inexpensive, yet high-quality, data? Perspectives on Psychological Science, 6, 3–5. 10.1177/1745691610393980 [DOI] [PubMed] [Google Scholar]
- Burch RL, & Johnsen L (2020). Captain Dorito and the bombshell: supernormal stimuli in comics and film. Evolutionary Behavioral Sciences. 10.1037/ebs0000164 [DOI] [Google Scholar]
- Burke NL, Schaefer LM, Hazzard VM, & Rodgers RF (2020). Where identities converge: The importance of intersectionality in eating disorders research. International Journal of Eating Disorders, 53, 1605–1609. 10.1002/eat.23371 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cash TF (1990). The psychology of physical appearance: Aesthetics, attributes, and images. In Cash TF, & Szymanski ML (Eds.). Body images: Development (pp. 51–79). Guilford Press. [Google Scholar]
- Cash TF (2000). The Multidimensional Body-Self Relations Questionnaire users’ manual: 3rd Revision. Available from the author: http://www.bodyimages.com/assessments.
- Cash TF, & Fleming EC (2002). The impact of body image experiences: Development of the body image quality of life inventory. International Journal of Eating Disorders, 31, 455–460. 10.1002/eat.10033 [DOI] [PubMed] [Google Scholar]
- Cash TF, & Henry PE (1995). Women’s body images: The results of a national survey in the USA. Sex Roles, 33, 19–28. 10.1007/BF01547933 [DOI] [Google Scholar]
- Cash TF, Jakatdar TA, & Williams EF (2004). The body image quality of life inventory: Further validation with college men and women. Body Image, 1, 279–287. [DOI] [PubMed] [Google Scholar]
- Cash TF, Winstead BW, & Janda LH (1986). The great American shape-up: Body image survey report. Psychology Today, 20, 30–37. 10.1016/S1740-1445(03)00023-8 [DOI] [Google Scholar]
- Cohen J (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Earlbaum. [Google Scholar]
- Colautti LA, Fuller-Tyszkiewicz M, Skouteris H, McCabe M, Blackburn S, & Wyett E (2011). Accounting for fluctuations in body dissatisfaction. Body Image, 8, 315–321. 10.1016/j.bodyim.2011.07.001 [DOI] [PubMed] [Google Scholar]
- Cole ER (2009). Intersectionality and research in psychology. American Psychologist, 64, 170–180. 10.1037/a0014564 [DOI] [PubMed] [Google Scholar]
- Copen CE, Chandra A, & Febo-Vazquez I (2016). Sexual behavior, sexual attraction, and sexual orientation among adults aged 18–44 in the United States: data from the 2011–2013 national survey of family growth. National Health Statistics Reports, 88, 1–14. https://www.cdc.gov/nchs//data/nhsr/nhsr088.pdf. [PubMed] [Google Scholar]
- Cox AE, Ullrich-French S, Cook-Cottone C, Tylka TL, & Neumark-Sztainer D (2020). Examining the effects of mindfulness-based yoga instruction on positive embodiment and affective responses. Eating Disorders, 28(4), 458–475. 10.1080/10640266.2020.1738909 [DOI] [PubMed] [Google Scholar]
- Danthinne ES, Giorgianni FE, & Rodgers RF (2020). Labels to prevent the detrimental effects of media on body image: A systematic review and meta-analysis. International Journal of Eating Disorders, 53, 647–661. 10.1002/eat.23242 [DOI] [PubMed] [Google Scholar]
- Fales MR, Frederick DA, Garcia JR, Gildersleeve KA, Haselton MG, & Fisher HE (2016). Mating markets and bargaining hands: Predictors of mate preferences for attractiveness and resources in two national U.S. studies. Personality and Individual Differences, 88, 78–87. 10.1016/j.paid.2015.08.041 [DOI] [Google Scholar]
- Fallon EA, Harris BS, & Johnson P (2014). Prevalence of body dissatisfaction among a United States adult sample. Eating Behaviors, 15, 151–158. 10.1016/j.eatbeh.2013.11.007 [DOI] [PubMed] [Google Scholar]
- Ferguson CJ (2009). An effect size primer: a guide for clinicians and researchers. Professional Psychology: Research and Practice, 40, 532–538. 10.1037/a0015808 [DOI] [Google Scholar]
- Fiske L, Fallon EA, Blissmer B, & Redding CA (2014). Prevalence of body dissatisfaction among United States adults: Review and recommendations for future research. Eating Behaviors, 15, 357–365. 10.1016/j.eatbeh.2013.11.007 [DOI] [PubMed] [Google Scholar]
- Forbes GB, & Frederick DA (2008). The UCLA Body Project II: Breast and body dissatisfaction among African, Asian, European, and Hispanic American college women. Sex Roles, 58, 449–457. 10.1007/s11199-007-9362-6 [DOI] [Google Scholar]
- Forrester-Knauss C, & Stutz EZ (2012). Gender differences in disordered eating and weight dissatisfaction in Swiss adults: Which factors matter? BMC Public Health, 12, 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frederick DA, Bohrnstedt GW, Hatfield E, & Berscheid E (2014). Factor structure and validity of the Body Parts Satisfaction Scale: Results from the 1972 Psychology Today Survey. Psychological Topics, 23, 223–243. http://hrcak.srce.hr/index.php?show=clanak&id_clanak_jezik=184664. [Google Scholar]
- Frederick DA, Buchanan GM, Sadehgi-Azar L, Peplau LA, Haselton MG, Berezovskaya A, & Lipinski RE (2007). Desiring the muscular ideal: Men’s body satisfaction in the United States, Ukraine, and Ghana. Psychology of Men and Masculinity, 8, 103–117. 10.1037/1524-9220.8.2.103 [DOI] [Google Scholar]
- Frederick DA, Daniels EA, Bates ME, & Tylka TL (2017). Exposure to thin-ideal media affects most, but not all, women: Results from the perceived effects of media exposure scale and open-ended responses. Body Image, 23, 188–205. 10.1016/j.bodyim.2017.10.006 [DOI] [PubMed] [Google Scholar]
- Frederick DA, & Essayli JH (2016). Male body image: The roles of sexual orientation and body mass index across five national U.S. studies. Psychology of Men & Masculinity, 17, 336–351. 10.1037/men0000031 [DOI] [Google Scholar]
- Frederick DA, Fessler DMT, & Haselton MG (2005). Do representations of male muscularity differ in men’s and women’s magazines? Body Image, 2, 81–86. 10.1016/j.bodyim.2004.12.002 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Forbes GB, Grigorian K, & Jarcho JM (2007). The UCLA Body Project I: Gender and ethnic differences in self-objectification and body satisfaction among 2,206 undergraduates. Sex Roles, 57, 317–327. 10.1007/s11199-007-9362-6 [DOI] [Google Scholar]
- Frederick DA, Garcia JR, Gesselman AN, Mark KP, Hatfield E, & Bohrnstedt G (2020). The Happy American Body 2.0: Predictors of affective body satisfaction in two U.S. national Internet panel surveys. Body Image, 32, 70–84. 10.1016/j.bodyim.2019.11.003 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Gordon AR, Cook-Cottone CP, Brady JP, Reynolds TA, Alley J, Garcia JR, Brown TA, Best CR, Brady JP, Crerand CE, Compte EJ, Convertino AD, Malcarne VL, Nagata JM, Parent MC, Perez M, Pila E, Pennesi J-L, Rodgers RF, Schaefer LM, Thompson JK, Tylka TL, & Murray SB (2022). Demographic and sociocultural predictors of sexuality-related body image and sexual frequency: The U.S. Body Project I. Body Image. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frederick DA, & Haselton MG (2007). Why is muscularity sexy? Tests of the fitness indicator hypothesis. Personality and Social Psychology Bulletin, 33, 1167–1183. 10.1177/0146167207303022 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Hazzard VM, Schaefer LM, Rodgers RF, Gordon AR, Tylka TL, Pennesi J-L, Convertino AD, Parent MC, Brady JP, Brown TA, Brady JP, Crerand CE, Compte EJ, Cook-Cottone CP, Malcarne VL, Nagata JM, Perez M, Pila E, Thompson JK, & Murray SB (2022). Sexual orientation differences in pathways from sociocultural and objectification constructs to body satisfaction: The U.S. Body Project I. Body Image. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frederick DA, Jafary A, Daniels EA, & Gruys K (2012). Surveys and the epidemiology of body image. In Cash TF (Vol. Ed.), The encyclopedia of body image and human appearance: Vol. 2, (pp. 766–773). San Diego: Academic Press. 10.1016/B978-0-12-384925-0.00121-8 [DOI] [Google Scholar]
- Frederick DA, Kelly MC, Latner JD, Sandhu G, & Tsong Y (2016). Appearance concerns among White and Asian American women: Sociocultural predictors of body, face, and eye satisfaction. Body Image, 16, 113–125. 10.1016/j.bodyim.2015.12.002 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Lever J, & Peplau LA (2007). Interest in cosmetic surgery and body image: Views of men and women across the lifespan. Plastic and Reconstructive Surgery, 120, 1407–1415. 10.1097/01.prs.0000279375.26157.64 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Peplau LA, & Lever J (2006). The swimsuit issue: Correlates of body image in a sample of 52,677 heterosexual adults. Body Image, 4, 413–419. 10.1016/j.bodyim.2006.08.002 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Peplau LA, & Lever J (2008). The Barbie mystique: Satisfaction with breast size and shape across the lifespan. International Journal of Sexual Health, 20, 200–211. 10.1080/19317610802240170 [DOI] [Google Scholar]
- Frederick DA, Pila E, Malcarne VL, Compte EJ, Nagata JM, Best CR, Brady JP, Brown TA, Crerand CE, Convertino AD, Cook-Cottone CP, Gordon AR, Parent MC, Pennesi J-L, Perez M, Reynolds TA, Rodgers RF, Schaefer LM, Thompson JK, Tylka TL, & Murray SB (2022). Demographic predictors of objectification theory and tripartite influence model constructs: The U.S. Body Project I. Body Image. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frederick DA, Reynolds TA, Barrera CA, Alley J, Garcia JR, & Murray SB (2022). Demographic and sociocultural predictors of face image satisfaction: The U.S. Body Project I. Body Image. [DOI] [PubMed] [Google Scholar]
- Frederick DA, Saguy AC, & Gruys K (2016). Culture, health, and bigotry: How exposure to cultural accounts of fatness shape attitudes about health risk, health policies, and weight-based prejudice. Social Science and Medicine, 165, 271–279. 10.1016/j.socscimed.2015.12.031 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Saguy AC, Sandhu G, & Mann T (2016). Effects of competing news media frames of weight on antifat stigma, beliefs about weight, and support for obesity-related public policies. International Journal of Obesity, 40, 543–549. 10.1038/ijo.2015.195 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Sandhu G, Morse PJ, & Swami V (2016). Correlates of appearance and weight satisfaction in a U.S. national sample: personality, attachment style, television viewing, self-esteem, and life satisfaction. Body Image, 17, 191–203. 10.1016/j.bodyim.2016.04.001 [DOI] [PubMed] [Google Scholar]
- Frederick DA, Schaefer LM, Hazzard VM, Rodgers RF, Tylka TL, Ong LQ, Pennesi J-L, Convertino AD, Parent MC, Brady JP, Brown TA, Brady JP, Crerand CE, Compte EJ, Cook-Cottone CP, Gordon AR, Malcarne VL, Nagata JM, Perez M, Pila E, Thompson JK, & Murray SB (2022). Racial identity differences in pathways from sociocultural and objectification constructs to body satisfaction: The U.S. Body Project I. Body Image. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frederick DA, Tylka TL, Rodgers RF, Convertino AD, Pennesi J-L, Parent MC, Brady JP, Brown TA, Brady JP, Crerand CE, Compte EJ, Cook-Cottone CP, Gordon AR, Malcarne VL, Nagata JM, Perez M, Pila E, Schaefer LM, Thompson JK, & Murray SB (2022). Pathways from sociocultural and objectification constructs to body satisfaction among men: The U.S. Body Project I. Body Image. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frederick DA, Tomiyama AJ, Bold JG, & Saguy AC (2020). Can she be healthy at her weight? Effects of news media frames on antifat attitudes, dieting intentions, and perceived health risks of obesity. Stigma and Health, 5, 247–257. 10.1037/sah0000195 [DOI] [Google Scholar]
- Frederick DA, Tylka TL, Rodgers RF, Pennesi J-L, Convertino AD, Parent MC, Brady JP, Brown TA, Brady JP, Crerand CE, Compte EJ, Cook-Cottone CP, Gordon AR, Malcarne VL, Nagata JM, Perez M, Pila E, Schaefer LM, Thompson JK, & Murray SB (2022). Pathways from sociocultural and objectification constructs to body satisfaction among women: The U.S. Body Project I. Body Image. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fredrickson BL, & Roberts TA (1997). Objectification theory: Toward understanding women’s lived experiences and mental health risks. Psychology of Women Quarterly, 21, 173–206. 10.1111/j.1471-6402.1997.tb00108.x [DOI] [Google Scholar]
- Fryar CD, Kruszan-Moran D, Gu Q, & Ogden CL (2018). Mean body weight, weight, waist circumference, and body mass index among adults: United States, 1999–2000 through 2015–2016. National Health Statistics Report, No. 129. Retrieved from https://stacks.cdc.gov/view/cdc/61430. [PubMed]
- Garner DM, & Kearney-Cooke A (1996). Body image 1996. Psychology Today, 29, 55–61. [Google Scholar]
- Gentile B, Grabe S, Dolan-Pascoe B, Twenge JM, Wells BE, & Maitino A (2009). Gender differences in domain-specific self-esteem: a meta-analysis. Review of General Psychology, 13, 34–45. 10.1037/a0013689 [DOI] [Google Scholar]
- Gillen MM (2015). Associations between positive body image and indicators of men’s and women’s mental and physical health. Body Image, 13, 67–74. 10.1016/j.bodyim.2015.01.002 [DOI] [PubMed] [Google Scholar]
- Gillen MM, & Markey CH (2018). A review of research linking body image and sexual well-being. Body Image. 10.1016/j.bodyim.2018.12.004 [DOI] [PubMed] [Google Scholar]
- Gillespie BJ, Frederick D, Harari L, & Grov C (2015). Homophily, close friendship, and life satisfaction among gay, lesbian, heterosexual, and bisexual men and women. PLoS One, 10, Article e0128900. 10.1371/journal.pone.0128900 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grabe S, & Hyde JS (2006). Ethnicity and body dissatisfaction among women in the United States: A meta-analysis. Psychological Bulletin, 132, 622–640. 10.1037/0033-2909.132.4.622 [DOI] [PubMed] [Google Scholar]
- Gray PB, & Frederick DA (2012). Body image and body type preferences in St. Kitts, Caribbean: A cross-cultural comparison with U.S. samples regarding attitudes towards muscularity, body fat, and breast size. Evolutionary Psychology, 10, 631–655. 10.1177/147470491201000319 [DOI] [PubMed] [Google Scholar]
- Greenleaf C (2005). Self-objectification among physically active women. Sex Roles, 52, 51–62. 10.1007/s11199-005-1193-8 [DOI] [Google Scholar]
- Gutin I (2018). In BMI we trust: reframing the body mass index as a measure of health. Social Theory & Health, 16, 256–271. 10.1057/s41285-017-0055-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halliwell E, Jarman H, Tylka TL, & Slater A (2018). Evaluating the impact of a brief yoga intervention on preadolescents’ body image and mood. Body Image, 27, 196–201. 10.1016/j.bodyim.2019.03.002 [DOI] [PubMed] [Google Scholar]
- Harper K, & Choma BL (2019). Internalised White ideal, skin tone surveillance, and hair surveillance predict skin and hair dissatisfaction and skin bleaching among African American and Indian Women. Sex Roles, 80, 735–744. [Google Scholar]
- Hazzard VM, Schaefer LM, Thompson JK, Murray SB, Frederick DA (2022). Measurement invariance of body image measures by age, gender, sexual orientation, race, and weight status: The U.S. Body Project I. Body Image. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hazzard VM, Schaefer LM, Thompson JK, Rodgers RF, & Frederick DA (2022). An abbreviated 10-item, two-factor version of the Body Image Quality of Life Inventory (BIQLI-10): The U.S. Body Project I. Body Image. [DOI] [PMC free article] [PubMed] [Google Scholar]
- He J, Sun S, Lin Z, & Fan X (2020). Body dissatisfaction and sexual orientations: A quantitative synthesis of 30 years research findings. Clinical Psychology Review Article 101896. 10.1016/j.cpr.2020.101896 [DOI] [PubMed] [Google Scholar]
- Homan KJ, & Tylka TL (2018). Development and exploration of the gratitude model of body appreciation in women. Body Image, 25, 14–22. 10.1016/j.bodyim.2018.01.008 [DOI] [PubMed] [Google Scholar]
- Hughes EK, Dean C, & Allen JS (2016). Measures of eating disorder symptoms, drive for muscularity, and muscle dysmorphia: Norms and typologies of Australian men. Australian Journal of Psychology, 68, 270–280. 10.1111/ajpy.12105 [DOI] [Google Scholar]
- Jampel JD, Murray SB, Griffiths S, & Blashill AJ (2016). Self-perceived weight and anabolic steroid misuse among US adolescent boys. Journal of Adolescent Health, 58, 397–402. 10.1016/j.jadohealth.2015.10.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karazsia BT, Murnen SK, & Tylka TL (2017). Is body dissatisfaction changing across time? A cross-temporal meta-analysis. Psychological Bulletin, 143, 293–320. 10.1037/bul0000081 [DOI] [PubMed] [Google Scholar]
- Keel PK, Baxter MG, Heatherton TF, & Joiner TE Jr. (2007). A 20-year longitudinal study of body weight, dieting, and eating disorder symptoms. Journal of Abnormal Psychology, 116, 422–432. 10.1037/0021-843X.116.2.422 [DOI] [PubMed] [Google Scholar]
- Kees J, Berry C, Burton S, & Sheehan K (2017). An analysis of data quality: Professional panels, student subject pools, and Amazons Mechanical Turk. Journal of Advertising, 46, 141–155. 10.1080/00913367.2016.1269304 [DOI] [Google Scholar]
- Kelly NR, Cotter EW, Tanofsky-Kraff M, & Mazzeo SE (2015). Racial variations in binge eating, body image concerns, and compulsive exercise among men. Psychology of Men & Masculinity, 16, 326–336. 10.1037/a0037585 [DOI] [Google Scholar]
- Kruger J, Lee CD, Ainsworth BE, & Macera CA (2008). Body size satisfaction and physical activity levels among men and women. Obesity, 16, 1976–1979. 10.1038/oby.2008.311 [DOI] [PubMed] [Google Scholar]
- Lever J, Frederick DA, Laird K, & Sadeghi-Azar L (2007). Tall women’s satisfaction with their height: General population data challenge assumptions behind medical interventions to stunt girls’ growth. Journal of Adolescent Health, 40, 192–194. 10.1016/j.jadohealth.2006.09.004 [DOI] [PubMed] [Google Scholar]
- Lever J, Frederick DA, & Peplau LA (2006). Does size matter? Men’s and women’s views on penis size across the lifespan. Psychology of Men & Masculinity, 7, 129–143. 10.1037/1524-9220.7.3.129 [DOI] [Google Scholar]
- Lewis-Smith H, Diedrichs PC, Rumsey N, & Harcourt D (2016). A systematic review of interventions on body image and disordered eating outcomes among women in midlife. International Journal of Eating Disorders, 49, 5–18. 10.1002/eat.22480 [DOI] [PubMed] [Google Scholar]
- Liang D, Frederick DA, Eiroa-Lledo E, Rosenfield NS, Berardi V, Linstead E, Maoz U (2022). Examining the utility of nonlinear machine learning versus linear regression analyses for predicting body image outcomes: The U.S. Body Project I. Body Image. [DOI] [PubMed] [Google Scholar]
- Lobera IJ, & Ríos PB (2011). Body image and quality of life in a Spanish population. International Journal of General Medicine, 4, 63–72. 10.2147/IJGM.S16201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Major B, Tomiyama AJ, & Hunger JM (2018). The negative and bidirectional effects of weight stigma on health. In Major B, Dovidio JF, & Link BG (Eds.). Oxford library of psychology. The Oxford handbook of stigma, discrimination, and health (pp. 499–519). Oxford University Press. [Google Scholar]
- McKinley NM, & Hyde JS (1996). The objectified body consciousness scale: Development and validation. Psychology of Women Quarterly, 20, 181–215. 10.1111/j.1471-6402.1996.tb00467.x [DOI] [Google Scholar]
- McLean SA, Wertheim EH, Marques MD, & Paxton SJ (2019). Dismantling prevention: Comparison of outcomes following media literacy and appearance comparison modules in a randomised controlled trial. Journal of Health Psychology, 24, 761–776. 10.1177/1359105316678668 [DOI] [PubMed] [Google Scholar]
- Meyer IH (1995). Minority stress and mental health in gay men. Journal of Health and Social Behavior, 36, 38–56. [PubMed] [Google Scholar]
- Mond J, Mitchison D, Latner J, Hay P, Owen C, & Rodgers B (2013). Quality of life impairment associated with body dissatisfaction in a general population sample of women. BMC Public Health, 13, 920. 10.1186/1471-2458-13-920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore F, & Keel PK (2003). Influence of sexual orientation and age on disordered eating attitudes and behaviors in women. International Journal of Eating Disorders, 34, 370–374. 10.1002/eat.10198 [DOI] [PubMed] [Google Scholar]
- Moreno-Domínguez S, Raposo T, & Elipe P (2019). Body image and sexual satisfaction: dfferences among heterosexual, bisexual and lesbian women. Frontiers in Psychology, 10, 903. 10.3389/fpsyg.2019.00903 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morrison TG, & Halton M (2009). Buff, tough, and rough: representations of muscularity in action motion pictures. The Journal of Men’s Studies, 17, 57–74. 10.3149/jms.1701.57 [DOI] [Google Scholar]
- Morrison TG, & McCutcheon JM (2012). Body image among gay, lesbian, and bi-sexual individuals. In Encyclopedia of body image and human appearance. Academic Press; 103–107. [Google Scholar]
- Morrison MA, Morrison TG, & Sager CL (2004). Does body satisfaction differ between gay men and lesbian women and heterosexual men and women? A meta-analytic review. Body Image, 1, 127–138. 10.1016/j.bodyim.2004.01.002 [DOI] [PubMed] [Google Scholar]
- Murray SB, Nagata JM, Griffiths S, Calzo JP, Brown TA, Mitchison D, … Mond JM (2017). The enigma of male eating disorders: a critical review and synthesis. Clinical Psychology Review, 57, 1–11. 10.1016/j.cpr.2017.08.001 [DOI] [PubMed] [Google Scholar]
- Nuttall FQ (2015). Body mass index: obesity, BMI, and health: a critical review. Nutrition Today, 50, 117–128. 10.1097/NT.0000000000000092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogden CL, Carroll MD, Fryar CD, & Flegal KM (2015). Prevalence of obesity among adults and youth: United States, 2011–2014. National Center for Health Statistics Data Brief, no. 219. Retrieved from http://htuneup.com/diseases/d_overweight.pdf. [PubMed] [Google Scholar]
- Paolacci G, Chandler J, & Ipeirotis PG (2010). Running experiments on Amazon Mechanical Turk. Judgment and Decision Making, 5, 411–419 http://doi.org/10/10630a/jdm10630a.html. [Google Scholar]
- Peplau LA, Frederick DA, Yee CK, Maisel N, Lever J, & Ghavami N (2009). Body image satisfaction in heterosexual, gay, and lesbian adults. Archives of Sexual Behavior, 38, 713–725. 10.1007/s10508-008-9378-1 [DOI] [PubMed] [Google Scholar]
- Puhl RM, Andreyeva T, & Brownell KD (2008). Perceptions of weight discrimination: Prevalence and comparison to race and gender discrimination in America. International Journal of Obesity, 32, 992–1000. 10.1038/ijo.2008.22 [DOI] [PubMed] [Google Scholar]
- Ridolfi DR, & Crowther JH (2013). The link between women’s body image disturbances and body-focused cancer screening behaviors: A critical review of the literature and a new integrated model for women. Body Image, 10, 149–162. 10.1016/j.bodyim.2012.11.003 [DOI] [PubMed] [Google Scholar]
- Roberts A, Cash TF, Feingold A, & Johnson BT (2006). Are black-white differences in females’ body dissatisfaction decreasing? A meta-analytic review. Journal of Consulting and Clinical Psychology, 74, 1121–1131. 10.1037/0022-006X.74.6.1121 [DOI] [PubMed] [Google Scholar]
- Robinson J, Rosenzweig C, Moss AJ, & Litman L (2019). Tapped out or barely tapped? Recommendations for how to harness the vast and largely unused potential of the Mechanical Turk participant pool. Plos One, 14. 10.1371/journal.pone.0226394 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodin J, Silberstein L, & Striegel-Moore R (1984). Women and weight: A normative discontent. Nebraska symposium on motivation. University of Nebraska Press. [PubMed] [Google Scholar]
- Rodgers RF, McLean SA, & Paxton SJ (2018). When seeing is not believing: An examination of the mechanisms accounting for the protective effect of media literacy on body image. Sex Roles, 1–10. 10.1007/s11199-018-0973-x [DOI] [Google Scholar]
- Rusticus SA, Hubley AM, & Zumbo BD (2008). Measurement invariance of the appearance schemas inventory–revised and the body image quality of life inventory across age and gender. Assessment, 15, 60–71. 10.1177/1073191107306805 [DOI] [PubMed] [Google Scholar]
- Saguy AC, Frederick D, & Gruys K (2014). Reporting risk, producing prejudice: How news reporting on obesity shapes attitudes about health risk, policy, and prejudice. Social Science & Medicine, 111, 125–133. 10.1016/j.socscimed.2014.03.026 [DOI] [PubMed] [Google Scholar]
- Schaefer LM, Burke NL, Thompson JK, Dedrick RF, Heinberg LJ, Calogero RM, & Swami V (2015). Development and validation of the Sociocultural Attitudes Towards Appearance Questionnaire-4 (SATAQ-4). Psychological Assessment, 27, 54–67. 10.1037/a0037917 [DOI] [PubMed] [Google Scholar]
- Schooler D (2008). Real women have curves: A longitudinal investigation of TV and the body image development of Latina adolescents. Journal of Adolescent Research, 23(2), 132–153. 10.1177/0743558407310712 [DOI] [Google Scholar]
- Sell A, Lukazsweski AW, & Townsley M (2017). Cues of upper body strength account for most of the variance in men’s bodily attractiveness. Proceedings of the Royal Society B: Biological Sciences, 284, 1–8. 10.1098/rspb.2017.1819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swami V, Frederick DA, Aavik T, Alcalay L, Allik J, Anderson D, … Zivcic-Becirevic I (2010). The attractive female body weight and female body dissatisfaction in 26 countries across 10 world regions: results of the International Body Project I. Personality and Social Psychology Bulletin, 36, 309–325. 10.1177/0146167209359702 [DOI] [PubMed] [Google Scholar]
- Swami V, Tran US, Stieger S, & Voracek M (2015). Associations between women’s body image and happiness: Results of the YouBeauty.com Body image survey (YBIS). Journal of Happiness Studies, 16, 705–718. 10.1007/s10902-014-9530-7 [DOI] [Google Scholar]
- Sypeck MF, Gray JJ, Etu SF, Ahrens AH, Mosimann JE, & Wiseman CV (2006). Cultural representations of thinness in women, redux: playboy magazine’s depiction of beauty from 1979 to 1999. Body Image, 3, 229–235. 10.1002/cpp.769 [DOI] [PubMed] [Google Scholar]
- Tantleff-Dunn S, Barnes RD, & Larose JG (2011). It’s not just a “woman thing:” the current state of normative discontent. Eating Disorders, 19, 392–402. 10.1080/10640266.2011.609088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson JK, Heinberg LJ, Altabe M, & Tantleff-Dunn S (1999). Exacting Beauty: Theory, Assessment, and Treatment of Body Image Disturbance. American Psychological Association 10.1037/10312-000 [DOI] [Google Scholar]
- Tiggemann M (2004). Body image across the adult life span: stability and change. Body Image, 1, 29–41. 10.1016/S1740-1445(03)00002-0 [DOI] [PubMed] [Google Scholar]
- Tiggemann M, & Zaccardo M (2015). Exercise to be fit, not skinny”: The effect of fitspiration imagery on women’s body image. Body Image, 15, 61–67. 10.1016/j.bodyim.2015.06.003 [DOI] [PubMed] [Google Scholar]
- Tomiyama AJ (2014). Weight stigma is stressful: A review of evidence for the cyclic obesity/weight-based stigma model. Appetite, 82, 8–15. 10.1016/j.appet.2014.06.108 [DOI] [PubMed] [Google Scholar]
- Tomiyama AJ, Hunger JM, Nguyen-Cuu J, & Wells C (2016). Misclassification of cardiometabolic health when using body mass index categories in NHANES 2005–2012. International Journal of Obesity, 40, 883–886. 10.1038/ijo201617 [DOI] [PubMed] [Google Scholar]
- Tylka TL (2011). Refinement of the tripartite influence model for men: dual body image pathways to body change behaviors. Body Image, 8, 199–207. 10.1016/j.bodyim.2011.04.008 [DOI] [PubMed] [Google Scholar]
- Tylka TL, & Andorka MJ (2012). Support for an expanded tripartite influence model with gay men. Body Image, 9, 57–67. 10.1016/j.bodyim.2011.09.006 [DOI] [PubMed] [Google Scholar]
- Tylka TL, & Wood-Barcalow NL (2015). What is and what is not positive. body image?? Conceptual foundations and construct definition. Body Image, 14, 118–129. 10.1016/j.bodyim.2015.04.001 [DOI] [PubMed] [Google Scholar]
- United States Census Bureau (2014). Florida passes New York to become nation’s third most populous state. Retrieved from https://www.census.gov/newsroom/press-releases/2014/cb14-232.html.
- United States Census Bureau (2018). QuickFacts. Retrieved from https://www.census.gov/quickfacts/fact/table/US/PST045218.
- Watson LB, Lewis JA, & Moody AT (2019). A sociocultural examination of body image among Black women. Body Image, 31, 280–287. [DOI] [PubMed] [Google Scholar]
- Wood-Barcalow NL, Tylka TL, & Augustus-Horvath CL (2010). But I like my body”: Positive body image characteristics and a holistic model for young-adult women. Body Image, 7, 106–116. 10.1016/j.bodyim.2010.01.001 [DOI] [PubMed] [Google Scholar]