

ABSTRACT
Dendriform pulmonary ossification (DPO) is a rare condition characterised by the formation of bones in lung tissues. This case report describes the first reported case of DPO in a patient with sickle cell disease (SCD), identifying DPO as a potential pulmonary consequence of SCD.
KEY WORDS: Acute chest syndrome, dendriform pulmonary ossification, interstitial lung disease, sickle cell disease
INTRODUCTION
Dendriform pulmonary ossification (DPO) is a rare form of interstitial lung disease characterised by the presence of mature bones within alveolar or interstitial spaces.[1,2] Sickle cell disease (SCD) is an inherited disease that affects red blood cells and is one of the most severe monogenic disorders in the world.[3] Although SCD has been associated with chronic lung disease, there is no documented connection between DPO and SCD. This case report describes the first reported case of DPO in a patient with SCD, identifying DPO as a potential pulmonary consequence of SCD.
CASE PRESENTATION
A 49-year-old female non-smoker with a past medical history of SCD and asthma was referred to a thoracic surgery clinic for a 1 year history of progressive dyspnea and cough. She was unable to walk more than one half mile on a flat ground and unable to climb more than 15 steps without rest. The patient had experienced two episodes of acute chest syndrome (ACS) in the past 3 years, an increase in frequency of SCD exacerbations from her prior history.
On presentation, the patient’s pulse oximetry was 99% on room air and she was normotensive. Respirations were unlabored, and breath sounds were clear bilaterally. A complete blood count and serum chemistry were within normal limits. Chest radiography showed bilateral nodular opacities. Chest computed tomography (CT) with IV contrast showed diffuse bilateral interstitial changes with multiple nodular opacities with varying levels of calcification, mostly in the periphery and the greatest in the lower lobes [Figures 1a, b]. Pulmonary function tests demonstrated normal FEV1 (95%), FEV1/FVC (101%), and DLCO/VA (99%). The only abnormal finding was a markedly reduced ERV (20%). Surgical lung biopsy was requested to guide further treatment.
Figure 1.

(a) Pre-operative CT scan coronal view demonstrating multiple nodular opacities bilaterally (b) Pre-operative CT scan axial view with the biopsied segment highlighted
At thoracoscopy, multiple lung nodules were extremely firm and appeared calcified. A wedge resection of the right upper lobe posterior segment was performed and included numerous nodules [biopsied segment noted in Figure 1b].
Grossly, the wedge resection showed a 2.2 x 1.9 x 1.7 cm ill-defined calcified lesion extending along the pleural surface. Representative sections of the specimen were de-calcified. On hematoxylin and eosin stain, there were abundant irregular foci of osseous trabeculae formation within the alveolar spaces, with some appearing to arise from the alveolar septa, and several bony fragments contained a fatty bone marrow [Figure 2a and 2b]. Focally, the osseous foci were adjacent to organising pneumonia and small areas of septal fibrosis. No morphological evidence of pulmonary hypertension or vascular congestion was seen. The patient was discharged on post-operative day 1 without complication.
Figure 2.
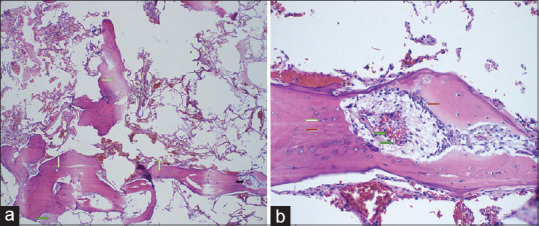
(a) Low-power (4X) photo-micrograph of the lung samples revealing branching ossification ( ) containing fibrotic cavity lined by osteoblastic cells (
) containing fibrotic cavity lined by osteoblastic cells ( ), adjacent to areas of fibrosis (
), adjacent to areas of fibrosis ( ) (b) High-power (20X) photo-micrograph showing a mature bone fragment (
) (b) High-power (20X) photo-micrograph showing a mature bone fragment ( ) with vascular proliferation () and lined by osteoblastic cells (
) with vascular proliferation () and lined by osteoblastic cells ( )
)
DISCUSSION
DPO is a rare form of interstitial lung disease whose pathogenesis is not fully understood. The mechanism of DPO is unclear; one theory involves angiogenesis and transformation of fibroblasts that exist in the lung to chondroblasts and osteoblasts.[1] The prevalence of DPO is 1.63 cases per 1,000.[4] There is no known treatment for DPO.
DPO and nodular pulmonary ossification (NPO) are the two types of pulmonary ossification. DPO is less common than NPO, but overlaps often arise. DPO is generally idiopathic or associated with primary lung pathologies, whereas NPO has been associated with mitral stenosis as well as other forms of cardiac, pulmonary, and systemic diseases.[4] DPO presents histologically with irregular tubules of a woven bone in a background of interstitial fibrosis with marrow elements present, differentiating it from NPO which lacks marrow elements.[5]
DPO has historically been diagnosed on autopsy of chronic lung disease patients.[4] However, with the expanded use of CT scans for lung disease, DPO is increasingly diagnosed pre-mortem. DPO usually presents on imaging with findings of calcifications, often nodular and often in the basal portions of the lungs. Chest CT has a high diagnostic yield for DPO.[5] CT is superior to X-ray for demonstrating the presence of calcium and delineating the ossification from associated lung disease. DPO can also be detected using TC-99 m methylene diphosphonate (the agent used for triple-phase bone scan).[6] The patient underwent a chest CT 2 months prior to surgery, which showed calcified nodular opacities. Our subsequent thoracoscopy revealed significantly increased dissemination of the calcifications. It has been suggested that CT can underestimate the true burden of DPO, which may have occurred in our case.[5]
SCD is an inherited multi-system disorder that can lead to chronic organ failure. ACS is the pre-eminent cause of morbidity and mortality within the sickle cell population. ACS occurs because of vaso-occlusion within the pulmonary vasculature, leading to chest pain, shortness of breath, and hypoxia. One of the consequences of SCD is chronic lung disease, with fibrosis occurring as a sequelae of recurrent episodes of ACS.[7] A study by Aquino et al.[8] found that 41% of the patients with SCD and a prior episode of ACS had interstitial lung abnormalities on CT. The study also noted a correlation between the extent of CT abnormalities and the number of prior ACS episodes.[8] Chronic lung disease because of SCD often presents with scattered foci of lung scarring, often with restrictive abnormalities on pulmonary function tests.[7] The patient’s only abnormality on pulmonary function tests was a decreased ERV, likely because of air trapping from obstructed small airways, which can occur in patients with pulmonary fibrosis.[9] Her multiple attacks of ACS prior to presentation and the relatively fast onset of her symptoms suggest a potential DPO diagnosis related to her history of SCD.
CONCLUSION
Our review of the literature indicates no previously reported case of DPO in a patient with SCD. The associations between SCD, ACS, and various types of chronic lung disease suggest that DPO may be another pulmonary consequence of SCD and its associated clinical cascade. Further studies are needed to better understand the relationship between sickle cell-associated lung disease and DPO.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Yomota M, Kamei T, Mirokuji K, Hishima T, Hosomi Y. A case of diffuse pulmonary ossification. Respirol Case Rep. 2021;9:e00812. doi: 10.1002/rcr2.812. doi:10.1002/RCR2.812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Desai HM, Amonkar GP. Florid bronchial cartilage ossification:A case report with literature revisited. Am J Forensic Med Pathol. 2013;34:125–6. doi: 10.1097/PAF.0b013e31828ce657. [DOI] [PubMed] [Google Scholar]
- 3.Rees DC, Williams TN, Gladwin MT. Sickle-cell disease. Lancet. 2010;376:2018–31. doi: 10.1016/S0140-6736(10)61029-X. [DOI] [PubMed] [Google Scholar]
- 4.Fernández-Bussy S, Labarca G, Pires Y, Díaz JC, Caviedes I. Dendriform pulmonary ossification. Respir Care. 2015;60:e64–7. doi: 10.4187/respcare.03531. doi:10.4187/RESPCARE.03531. [DOI] [PubMed] [Google Scholar]
- 5.Kim TS, Han J, Chung MP, Chung MJ, Choi YS. Disseminated dendriform pulmonary ossification associated with usual interstitial pneumonia:Incidence and thin-section CT-pathologic correlation. Eur Radiol. 2005;15:1581–5. doi: 10.1007/s00330-005-2671-7. [DOI] [PubMed] [Google Scholar]
- 6.Jamjoom L, Meziane M, Renapurkar R. Dendriform pulmonary ossification:Report of two cases. Indian J Radiol Imaging. 2013;23:15–8. doi: 10.4103/0971-3026.113613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Miller AC, Gladwin MT. Pulmonary complications of sickle cell disease. Am J Respir Crit Care Med. 2012;185:1154–65. doi: 10.1164/rccm.201111-2082CI. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aquino SL, Gamsu G, Fahy JV, Claster S, Embury SH, Mentzer WC, et al. Chronic pulmonary disorders in sickle cell disease:Findings at thin-section CT. Radiology. 1994;193:807–11. doi: 10.1148/radiology.193.3.7972829. [DOI] [PubMed] [Google Scholar]
- 9.Hochhegger B, Sanches FD, Altmayer SPL, Pacini GS, Zanon M, Guedes ÁD, et al. Air trapping in usual interstitial pneumonia pattern at CT:Prevalence and prognosis. Sci Rep. 2018;8:17267. doi: 10.1038/s41598-018-35387-3. [DOI] [PMC free article] [PubMed] [Google Scholar]