

ABSTRACT
The lifting of non-pharmaceutical measures preventing transmission of SARS-CoV-2 (and other viruses, including influenza viruses) raises concerns about healthcare resources and fears of an increased number of cases of influenza and COVID-19. For the 2021-2022 influenza season, the WHO and >20 European countries promoted coadministration of influenza and COVID-19 vaccines. Recently, the French Health Authority recommended coupling the COVID-19 vaccination with the 2022-2023 influenza vaccination campaign for healthcare professionals and people at risk of severe COVID-19. The present systematic review examines published data on the safety, immunogenicity, efficacy/effectiveness, and acceptability/acceptance of coadministration of influenza and COVID-19 vaccines. No safety concerns or immune interferences were found whatever the vaccines or the age of vaccinated subjects (65- or 65+). No efficacy/effectiveness data were available. The results should reassure vaccinees and vaccinators in case of coadministration and increase vaccine coverage. Healthcare systems promoting coupled campaigns must provide the necessary means for successful coadministration.
KEYWORDS: Coadministration, COVID-19 vaccines, influenza vaccines, patient acceptance of healthcare, patient compliance, patient safety, vaccine immunogenicity, vaccine efficacy
Plain Language Summary
The lifting of non-pharmaceutical measures recommended to prevent transmission of SARS-CoV-2 (and other viruses, including influenza viruses) raises concerns about healthcare resources, already under pressure. It also raises fears of an increase in the number of cases of influenza or COVID-19 infection during the winter season. For the 2021–2022 influenza season, the World Health Organization and several European countries promoted concomitant administration in distinct anatomic sites (i.e., coadministration) of influenza and COVID-19 vaccines to avoid additional stress on healthcare systems. In May 2022, the French Health Authority recommended coupling the COVID-19 vaccination with the 2022–2023 influenza vaccination campaign (i.e., starting COVID-19 vaccination at the date of influenza vaccination) for healthcare professionals and people at risk of severe COVID-19, in case of epidemic wave. Coadministration of influenza and COVID-19 vaccines is one of the factors of success for a coupled campaign. The present systematic review examines all published data (articles or reports, clinical trials, or surveys) on the safety, immunogenicity, efficacy/effectiveness, and acceptability/acceptance of coadministration of influenza and COVID-19 vaccines. The PRISMA method was used to collect information. No safety concerns or immune interferences were found whatever the vaccines or the age of vaccinated subjects (65- or 65+). No efficacy/effectiveness data were available. Acceptability and acceptance were good but could be improved. By reassuring vaccinees and vaccinators, these results are expected to favor coadministration and ultimately increase vaccine coverage, thus offering better protection. Healthcare systems promoting coupled campaigns with coadministration must provide the necessary means for their successful implementation.
Introduction
Since the beginning of the COVID-19 pandemic, non-pharmaceutical shielding measures such as hand-washing, mask-wearing, and social distancing have been taken to limit virus transmission in the community. These measures have been effective against COVID-19 and many other common infectious diseases, including seasonal influenza viruses.1 In fact, influenza virus circulation was drastically slowed in 2020 and 2021.1 However, influenza viruses are still circulating, and the lifting of non-pharmaceutical measures contributed to the return of influenza activity in 2022,2,3 raising concerns about health resources and fears of an increased number of cases of influenza and COVID-19.4,5
COVID-19 vaccination saved almost 20 million lives worldwide in 2021 and vaccination protects millions of individuals against seasonal influenza each year.6–9 In Autumn 2021, the World Health Organization (WHO) promoted concomitant administration in distinct anatomic sites (i.e., coadministration) of inactivated seasonal influenza and COVID-19 vaccines for the 2021–2022 flu season.10 Coadministration was allowed in more than 20 countries, including numerous European countries: e.g., Belgium, Denmark, Finland, France, Germany, Italy, Spain, Switzerland, and the UK.11–19 The decision to promote coadministration was taken by the WHO in a context of reduced public health and social measures to prevent SARS-CoV-2 transmission, given the potential impact of reduced herd immunity resulting from lack of influenza virus exposure in 2020 and 2021, and to avoid additional stress on health systems.10 This decision was based on the results of two studies that addressed coadministration of three COVID-19 vaccines (BNT162b2, ChAdOx1, and NVX-CoV2373) with various seasonal influenza vaccines (trivalent or quadrivalent, with or without adjuvant, cellular, or recombinant).20,21
Coadministration of seasonal inactivated influenza and COVID-19 vaccines was also supported by the cocirculation of influenza viruses and SARS-CoV-2 and coinfection.22 In France, in Week 17, 2022, according to the Sentinelles network (the French influenza surveillance network), 30% of the sampled cases of acute respiratory infection seen by general practitioners or pediatricians were positive for influenza viruses and 22% for SARS-CoV-2.23 In Week 19, 23 of the 472 influenza cases admitted to intensive care unit were cases of coinfection with SARS-CoV-2.24 Moreover, several studies showed that coinfection increased the risk of serious illness. In a large study conducted in England during the 2019–2020 season, 43% of individuals with coinfection died vs 27% of those who tested positive only for SARS-CoV-2.25 In the study by Swets et al.,26 coinfection was detected in 3% (N = 227/6,965) of patients with tests recorded for respiratory viral coinfection and was associated with greater likelihood of invasive mechanical ventilation and death than was isolated SARS-CoV-2 infection. Finally, according to simulations of future trajectories, the lifting of non-pharmaceutical shielding measures preventing COVID-19 transmission could result in large influenza outbreaks, increasing the risk of influenza and COVID-19 coinfection and ultimately the risk of serious illness.27
On 25 April 2022 (date of the literature search), several national vaccination programs indicated that COVID-19 vaccines could be coadministered with influenza vaccines.10–19 As an example, on 25 May 2022, the French Health Authority recommended coupling the COVID-19 vaccination with the 2022–2023 influenza vaccination campaign for healthcare professionals (HCPs) and people at risk of severe COVID-19, in case of epidemic wave. It recommended that the start of the campaign should be determined by the start date of influenza vaccination.28 This coupled approach will succeed only if the population, at least HCPs who are at increased risk of exposure (and to avoid nosocomial infection spread) and 65+ who are at risk of severe disease,7,20,28 agree to be vaccinated, and if the HCPs agree to administer both vaccines concomitantly (coadministration). According to Stefanizzi et al.,29 20% of HCPs reported concerns that coadministration of different vaccines increased the risk of adverse events.
The objective of the present literature review was to assess the safety, immunogenicity, and efficacy/effectiveness of the coadministration of inactivated influenza and COVID-19 vaccines, and their acceptability and/or acceptance. It is expected that a better knowledge of safety, immunogenicity, and efficacy/effectiveness of coadministration will reassure vaccinees and vaccinators, and thus will favor coadministration and increase vaccination coverage, ultimately offering better protection.
Materials and methods
The present systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), version 2020.30
Search strategy
ClinicalTrials (the largest database) and EudraCT (the European database) were searched to identify clinical studies using the keyword: “COVID-19” and “Influenza” on April 28 and 29, 2022, respectively.
PubMed was searched on 25 April 2022 to identify articles using different terms for COVID-19, influenza, vaccine, and coadministration. The terms needed to be present in the title or the abstract of the articles. No filters and no date restrictions were applied. Finally, the following equation was used: {[(“COVID-19” OR “SARS-CoV-2”) AND (“Influenza” OR “flu”)] AND [(“Vaccine” and “Vaccines”)] AND [(“coadministration” OR “co-administration” OR “co-injection” OR “coinjection” OR “concomitant administration” OR “concomitant injection” OR “concomitant vaccination” OR “covaccination” OR “co-vaccination”)]}. In addition, the lists of “similar” and “cited by” articles (cf. PubMed) were checked for missing articles. Finally, a free search on Google Scholar (“coadministration of covid-19 and influenza vaccines”) was performed to identify additional articles on clinical studies or surveys.
The information obtained from the various sources was merged.
Study selection
For studies identified on ClinicalTrials or EudraCT, selection was based on the title of the study and then on investigational products after exclusion of duplicate studies.
For articles identified on PubMed or Google Scholar, selection was based on the title of the article and then on the abstract. Only articles with an Abstract, reporting data from clinical trials or observational studies (case reports excluded), and written in English or in French were selected.
No selection was performed on the type of article or type of study. The PICO method was adopted to select studies: Population (no selection, all studied populations included), Intervention (influenza and COVID-19 vaccines regardless of their nature), Comparison (no selection), Outcomes (safety, efficacy, effectiveness, immunogenicity, acceptability, or acceptance).
Three investigators (SS, NP, and FP) independently selected the articles and clinical studies. Potential discrepancies were discussed and solved.
Data extraction
The following data were extracted from selected items: first author/investigator name, year of publication, type of study, and study country. The PICO method was then adopted to define the variables of interest: Population (number of subjects, age, and gender), Intervention (vaccines), Comparison (if applicable), Outcomes (safety, efficacy/effectiveness/immunogenicity, and acceptability or acceptance).
Results
A total of 352 clinical trials and 16 articles were identified by the systematic search strategy (Figure 1). A total of 330 clinical trials and two articles were immediately removed as they were out of scope. After screening, 16 clinical trials and seven articles were excluded. Two clinical trials found in additional databases and one report on a survey conducted by one of the authors (AM) were also assessed for eligibility. All the eligible clinical trials (Supplementary Table S1) were excluded from analysis, as no data were available (no posted results). Overall, eight items were included in the analysis: six original articles, one editorial, and one report. Three of the six original articles reported results from clinical trials on the safety and immunogenicity of coadministration; none compared efficacy between coadministration and isolated influenza or COVID-19 administration (monoadministration). The remaining items (n = 5) were studies on the acceptability and/or acceptance of coadministration.
Figure 1.
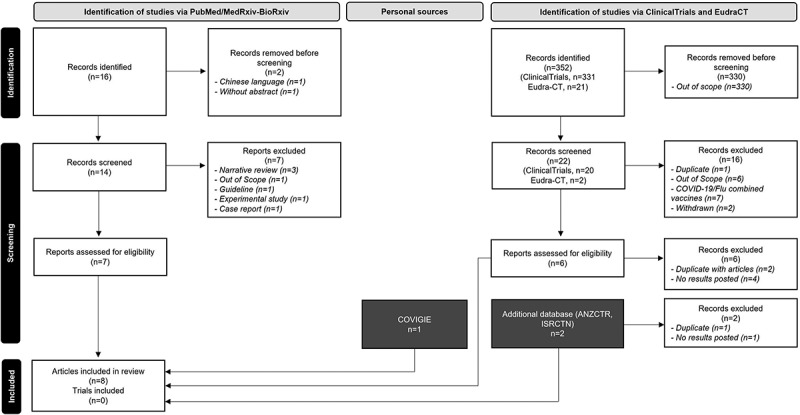
Study selection (PRISMA Flow chart)30.
Safety & immunogenicity
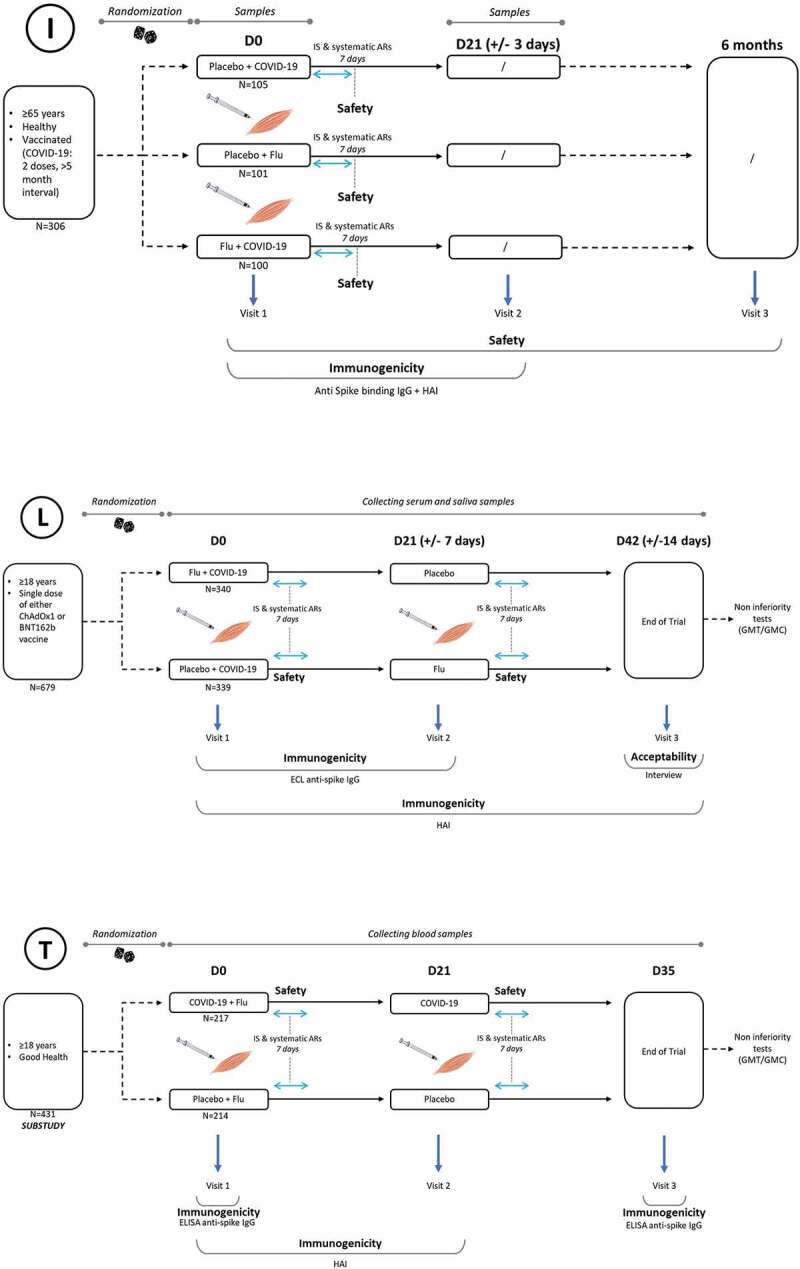
The three clinical trials comparing safety and immunogenicity between influenza/COVID-19 coadministration versus influenza or COVID-19 monoadministration (Table 1) were conducted in Europe (UK: n = 2),20,21 and in the USA (n = 1).31 They started between September 2020 and July 2021.20,21 Two were multicenter randomized controlled trials,20,31 and one was a substudy in a large randomized controlled trial.21 Overall, four influenza vaccines and four COVID-19 vaccines were used (Supplementary Table S2). Influenza vaccines were a trivalent inactivated and adjuvanted vaccine (aTIV: Fluad®, Seqirus),20,21 a quadrivalent inactivated nonadjuvanted vaccine produced on cell cultures (QIVc: Flucelvax® Tetra, Seqirus),20,21 a quadrivalent inactivated, recombinant vaccine (QIVr: Flublok® Quadrivalent, Sanofi Pasteur),20 and a quadrivalent inactivated high-dose vaccine (QIV HD: Fluzone® High-Dose Quadrivalent, Sanofi Pasteur). No assessment of live influenza vaccine coadministered with COVID-19 vaccine was performed. The four COVID-19 vaccines were one live replication-deficient recombinant vaccine (Vaxzevria®, AstraZeneca), one inactivated recombinant protein vaccine (Nuvaxovid®, Novavax), and two mRNA vaccines (Spikevax®, Moderna, and Comirnaty®, Pfizer/BioNTech). Participants (306, 431, and 679 in the studies by Izikson, Toback, and Lazarus, respectively)20,21,31 were either naive or non-naive for COVID-19 vaccination. All participants were aged 18 years and older. Participants in the study by Izkinson et al.31 had completed a two-dose primary series, those in the study by Lazarus et al.20 had received one dose of COVID-19 vaccine, and those in the study by Toback et al. 21 had never been vaccinated against COVID-19. In the study by Izikson et al.,31 all the participants were aged 65+ (median age, 71 years), while subgroups were 65+ in the studies by Lazarus et al. and Toback et al.20,21 Finally, study designs clearly differed between the three clinical trials (Figure 2).
Table 1.
Description of the safety & immunogenicity studies reviewed.
| Ref. | Izikson et al. (2022)31 | Lazarus et al. (2021)20 | Toback et al. (2022)21 |
|---|---|---|---|
| STUDY INFORMATION | |||
| Registration # | ClinicalTrials.gov NCT04969276 |
EudraCT 2021–001124-18 |
ClinicalTrials.gov NCT04583995 |
| Sponsor | Sanofi Pasteur | University hospitals Bristol and Weston NHS Foundation Trust | Novavax |
| Country | USA | UK | UK |
| Study dates | July/August 2021 | April/June 2021 | September/November 2020 |
| STUDY DESIGN | |||
| Phase 2 | Phase 4 | Phase 3 | |
| RCT | RCT | RCT | |
| Multicenter (6 centers) | Multicenter (12 centers) | Multicenter (33 centers) | |
| Interim report (on 21 d) | Substudy, 4 centers only | ||
| Participants | 306 adults: | 679 adults: | 431 adults: |
| ≥65 y, 100% | ≥65 y, 33% | ≥65 y, 7% | |
| Randomization (1:1:1) | Randomization (1:1) | Not randomized | |
3 groups:
|
2 groups per flu (n = 3), and COVID (n = 2) vaccines
|
2 groups:
|
|
N = 296
|
N = 679
|
N = 431
|
|
| Vaccines | I, 1 Flu vaccine:
|
I, 3 flu vaccines:
|
I, 2 flu vaccines:
|
C, 1 COVID vaccine:
|
C, 2 COVID vaccines:
|
C, 1 COVID vaccine:
|
|
| P, Placebo | P, Placebo | P, Placebo | |
| Vaccination schedule |
COVID-19: booster dose (last dose of primary vaccination >5 months) |
COVID-19: dose 2 of primary series (last dose >2/3 months ChAdOx1 or >1/3 months BNT162b2) | COVID-19: dose 1 of primary series |
| 2 injections on Day 0 (C+I, P+I or P+C) |
2 injections on Day 0 (C+I, or C+P) 1 injection on Day 21 (P or I) |
2 injections on Day 0 (C+I or I+P) 1 injection on Day 21 (C or P) |
|
| SAFETY | |||
| Reactogenicity | Follow-up: 21 d (Interim analysis) | Follow-up: 21 d after each injection | Follow-up: 35 d after the first injection |
| Solicited ISR − 7 d | Solicited ISR − 7 d | Solicited ISR − 7 d | |
| & | Solicited systemic AR − 7 d | Solicited systemic AR − 7 d | Solicited systemic AR − 7 d |
| Other safety | Unsolicited AE | Unsolicited AE | Unsolicited AE |
| information | SAE | SAE | SAE |
| AESI | AESI | AESI | |
| MAAE | MAAE | MAAE | |
| IMMUNOGENICITY | |||
| Influenza | HI | HI | HI |
| A/H1N1; A/H3N2; B/Yamagata; B/Victoria | A/H1N1; A/H3N2; B/Yamagata; B/Victoria | A/H1N1; A/H3N2; B/Yamagata; B/Victoria | |
| Day 0 & Day 21 | Day 0, Day 21, & Day 42 | Day 0 & Day 21 | |
| Titer (1/dil) | Titer (1/dil) | Titer (1/dil) | |
| COVID-19 | ELISA | ECLIA (Elecsys) | ELISA |
| Concentration (BAU/ml) Day 0 & Day 21 |
Titer (U/ml) Day 0, Day 21, & Day 42 |
Concentration (ELISA units/ml) Day 0 & Day 35 |
|
AESI: adverse event of special interest; AR: adverse reaction; aTIV: adjuvanted trivalent influenza vaccine; BAU: binding antibody units (=ELU (ELISA laboratory units)/ml÷7.9815); C: COVID-19 vaccine; d: days; ECLIA: electro-chemiluminescence immunoassay; ELISA: enzyme-linked immunosorbent assay; GMC: geometric mean concentration; GMT: geometric mean titer; HD-QIV: high dose quadrivalent influenza vaccine; HI: hemagglutinin inhibition; I: influenza vaccine; ISR: injection site reaction; MAAE: medically attended adverse event; P: placebo; QIVc: cellular quadrivalent influenza vaccine; QIVr: recombinant quadrivalent influenza vaccine; RCT: randomized clinical trials; SAE: serious/severe adverse event; y: years.
Figure 2.
Study designs of selected randomized controlled trials (N = 3).
(I) Izikson et al.31; (L) Lazarus et al.20; (T) Toback et al.21
ARs: adverse reactions; HAI: hemagglutinin-inhibiting antibodiegglutinin-inhibiting antibodies; IgG: immunoglobulin G; IS: injection site.
No major safety issues regarding coadministration were reported. No serious adverse events (SAEs) and no adverse events of special interest (AESIs) were reported by Izkinson et al.31 There was one SAE in the study by Lazarus et al. and one in the study by Toback et al.20,21 In the study by Lazarus et al.,20 one case of severe headache leading to hospital admission and considered related to vaccine administration was reported following concomitant administration of the ChAdOx1 vaccine and the cellular quadrivalent influenza vaccine (QIVc). No information was provided on the SAE reported in the study by Toback et al.21 Medically attended adverse events (MAAEs) were rare and reported at similar rates in coadministration and monoadministration groups. Adverse events were usually of mild or moderate intensity and self-limiting. Globally, reactogenicity profiles (i.e., percentage of participants reporting at least one solicited injection site reaction or at least one solicited systemic adverse reaction within 7 days following vaccine administration) were similar between the coadministration and COVID-19 vaccine groups, and lower in the influenza vaccine group than in the coadministration and COVID-19 vaccine groups (Figures 3 and 4). In the study by Izkinson et al.,31 86% [95% CI: 78–92] of participants reported at least one solicited injection site reaction following administration of high-dose quadrivalent inactivated vaccine (QIV-HD) and a booster dose of mRNA-173 SARS-CoV-2 vaccine, 91% [84–96] after administration of the booster dose of mRNA-173 SARS-CoV-2 vaccine, and 62% [51–72] after administration of the QIV-HD vaccine. Respectively, 84% [75–90], 80% [71–87], and 49% [39–60] of participants reported at least one systemic reaction.
Figure 3.
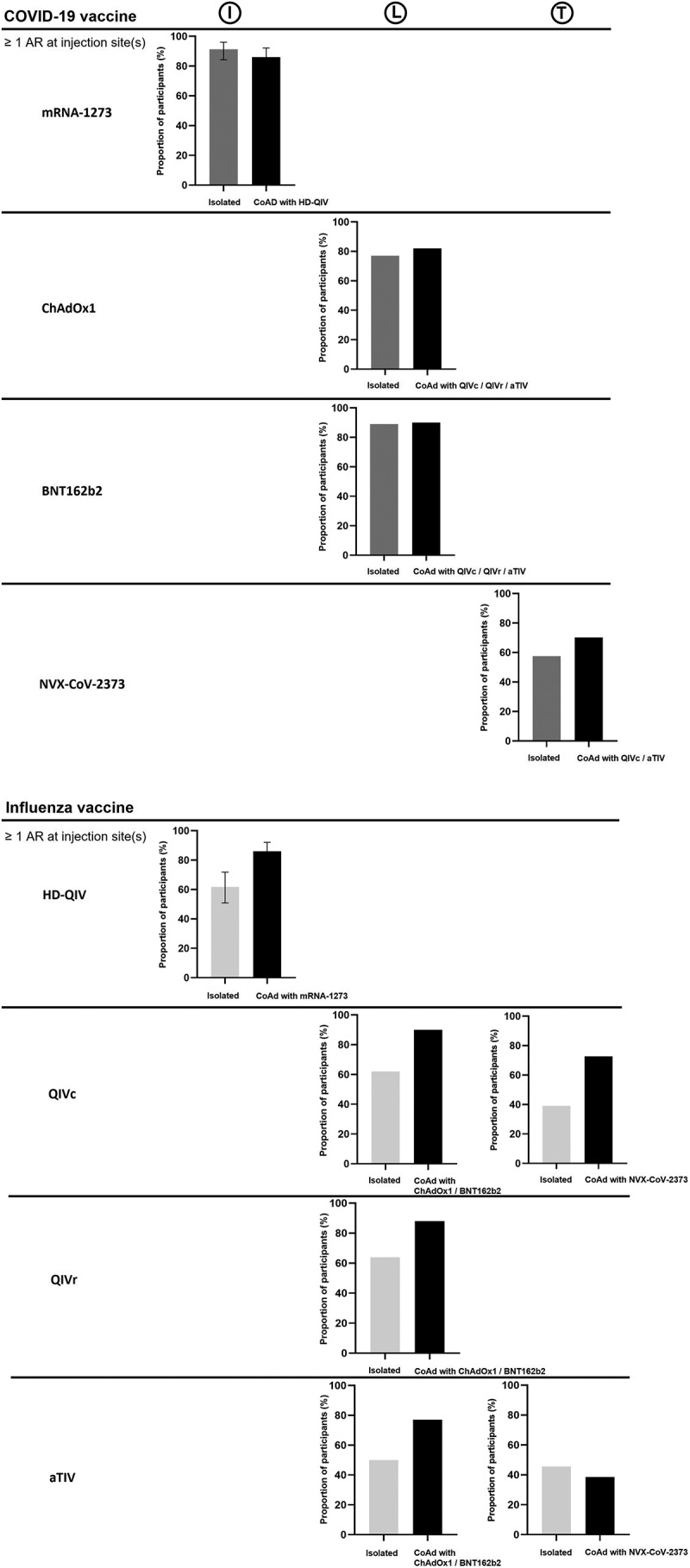
Proportion of vaccinees reporting at least one adverse reaction at injection site(s) through 7 d following mono or coadministration of influenza and COVID-19 vaccines.
(I) Izikson et al.31; (L) Lazarus et al.20; (T) Toback et al.21
AR: adverse reaction; aTIV: adjuvanted trivalent influenza vaccine; CoAd: coadministration; HD-QIV: high-dose quadrivalent influenza vaccine; QIVc: cellular quadrivalent influenza vaccine; QIVr: recombinant quadrivalent influenza vaccine.
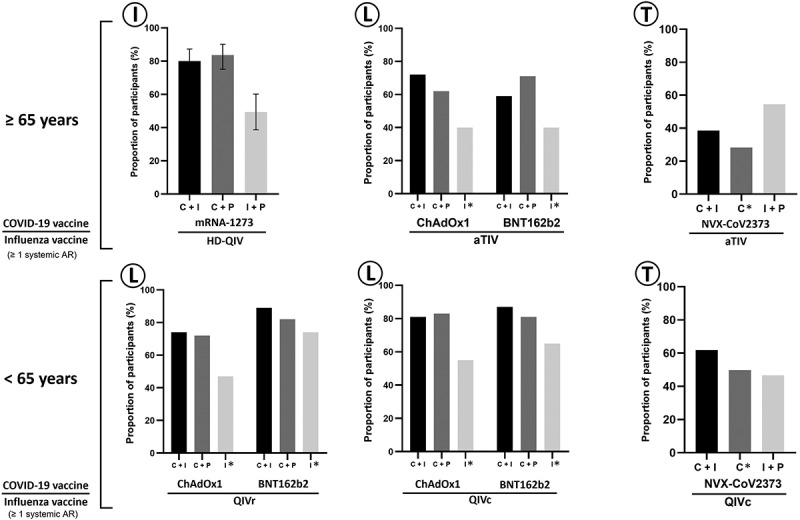
Figure 4.
Proportion of vaccinees reporting at least one systemic adverse reaction through 7 d following mono or coadministration of influenza and COVID-19 vaccines.
(I) Izikson et al.31; (L) Lazarus et al.20; (T) Toback et al.21
AR: adverse reaction; C: COVID-19 vaccine; C+I: coadministration of both vaccines; I: influenza vaccine; P: placebo.
*: Means the corresponding vaccine is administered 21 d after C+I for the COVID-19 vaccine and C+P for the influenza vaccine.
Coadministration had no significant negative impact on the immunogenicity of influenza or COVID-19 vaccination, although a modest decrease was observed in the immunogenicity of NVX-COV2373 in case of coadministration.21 In the study by Izkinson et al.,31 hemagglutination inhibition (HI) antibody titers increased 21 days after vaccine injections in the coadministration and QIV-HD groups, and anti-spike antibody concentrations increased in the coadministration and mRNA-1273 SARS-CoV-2 groups. Geometric mean titers (GMTs, for HI) or geometric mean concentrations (GMCs, for anti-spike antibodies) were similar in the coadministration and monoadministration groups. Coadministration vs monoadministration GMT or GMC ratios were close to 1: 0.87 [95% CI: 0.61–1.23] for A(H1N1), 0.89 [0.70–1.14] for H3N2, 0.88 [0.71–1.09] for B/Yamagata, 0.96 [0.79–1.16] for B/Victoria, and 0.97 [0.79–1.19] for SARS-CoV-2.8 In the study by Lazarus et al.,20 immune response was not adversely affected by coadministration. With BNT162b2 vaccine as COVID-19 vaccine, coadministration vs monoadministration GMT ratios ranged from 0.94 [0.85–1.05] for B/Yamagata to 1.38 [1.11–1.71] for A(H1N1) in 18–64-year-olds, and from 1.00 [0.86–1.15] for B/Yamagata strain to 1.18 [1.02–1.37] for A(H3N2) in 65+.They ranged from 0.86 [0.74–0.99] for A(H1N1) to 1.08 [0.96–1.21] for A(H3N2) and from 0.92 [0.83–1.03] for B/Yamagata to 1.15 [1.01–1.32] for A(H1N1) in case of ChAdOx1 as COVID-19 vaccine. In the 18–64-y-olds, coadministration vs monoadministration GMC ratios ranged from 0.86 [0.72–1.03] for BNT162b2 vaccine + recombinant quadrivalent influenza vaccine (QIVr) to 0.92 [0.81–1.04] for ChAdOx1 vaccine + QIVc or QIVr; in 65+, coadministration (adjuvanted trivalent influenza vaccine, aTIV) vs monoadministration GMC ratio was 0.97 [0.83–1.13] for BNT162b2 vaccine and 1.02 [0.91–1.14] for ChAdOx1 vaccine. Finally, according to Toback et al.,21 coadministration had no impact on influenza vaccine immune response, with a slight reduction in antibody responses to the NVX-CoV2373 vaccine. Coadministration vs monoadministration GMT ratios calculated by Domnich et al.8 ranged from 0.99 for B/Yamagata to 1.09 for A(H1N1) in 65- and from 0.54 for B/Victoria to 1.41 for A(H1N1) in 65+.The coadministration vs monoadministration GMC ratio was 0.66 in 65- and 0.71 in 65 +.
Acceptability & acceptance
The five studies assessing acceptability and/or acceptance of coadministration were conducted in Europe (Italy, n = 3; France, n = 1),32–34 and in China (n = 1).35 All were conducted between May 2020 and November 2021, except COVIGIE, an express survey, which was conducted between January and February 2022 (Table 2).
Table 2.
Description of the acceptability & acceptance studies reviewed.
| Ref. | Domnich et al. (2021)32 |
Domnich et al. (2022)33 |
Ma et al. (2022)35 |
COVIGIE (2022)34 |
Stefanizzi et al. (2022)29 |
Lazarus et al. (2021)20 |
|---|---|---|---|---|---|---|
| STUDY INFORMATION | ||||||
| Country | Italy | Italy | China | France | Italy | UK |
| Study dates | May 2020/21 | October/November 2021 | September/October 2021 | January/February 2022 | October 2021 | April/June 2021 |
| STUDY DESIGN | ||||||
| Survey CAWI |
Survey CAWI |
Survey 23-item online questionnaire |
Survey Online questionnaire |
Study Data collection about vaccination status |
Study Interview during the study |
|
| Questioned participants |
1979 adults: ≥18 y |
2463 adults: ≥18 y |
9424 adults: ≥18 y |
975 HCPs: ≥18 y |
2740 HCPs: ≥18 y |
679 adults: ≥18 y Previously vaccinated with both vaccines concomitantly |
| OUTCOME | ||||||
| Acceptability: willingness of being vaccinated concomitantly with both vaccines before concomitant administration | Acceptability: willingness of being vaccinated concomitantly with both vaccines before concomitant administration | Acceptability: willingness of being vaccinated concomitantly with both vaccines before concomitant administration | Acceptance: having agreed to vaccinate with both vaccines concomitantly (N = 529) or having agreed to be vaccinated with both vaccines concomitantly as reported by the HCPs (N = 719) | Acceptance(having agreed to be vaccinated concomitantly with both vaccines) | Acceptability (willingness of being vaccinated concomitantly with both vaccines before concomitant administration | |
CAWI: computer assisted web interview; d: days; HCPs: healthcare professionals; y: years.
Acceptability refers to the theoretical willing of participants to receive a concomitant injection of influenza and COVID-19 vaccines. Acceptance refers to the rate of participants who already chose the concomitant injection of both vaccines.
“Acceptability” is the quality of being accepted, measured a priori as the willingness to receive (or administer) both vaccines; “acceptance” is actually accepting the coadministration of vaccines, measured a posteriori. Most studies investigated the acceptability of coadministration of both influenza and COVID-19 vaccines.32,33,35 However, the study by Stefanizzi et al. examined the acceptance of coadministration by the HCPs,29 and COVIGIE interviewed HCPs on influenza and COVID-19 vaccine coadministration performed during the previous influenza season.34 In addition, participants in the clinical trial by Lazarus et al. who received concomitant administration of both COVID-19 and influenza vaccines were asked about their willingness to receive concomitant administration for the coming season.20
Regarding acceptability, in the Italian longitudinal survey by Domnich et al.,32 67.5% of the 1,979 respondents favored coadministration: 34.1% [95% CI: 32.0–36.2] expressed firm willingness to receive coadministration and 33.4% [31.3–35.5] expressed some willingness. According to the Chinese survey,35 77% of participants (n = 7,254) expressed willingness to receive coadministration whereas 1,637 (17.3%) were uncertain and 533 (5.7%) were unwilling. Higher percentages were reported in the study by Lazarus et al. which included participants vaccinated with both influenza and COVID-19 vaccines concomitantly.20 In this study, between 98% and 100% of those aged less than 65 years (65-) and between 98% and 99% of the 65+ who had previously received both vaccines concomitantly claimed their willingness to receive both vaccines concomitantly in the future.
Regarding acceptance, according to 719 of the HCPs included in the French express survey, during the 2021–2022 influenza season, patients agreed to receive both vaccines concomitantly for 64% of the HCPs (23% agreed immediately and 41% after thinking about it).34 Moreover, in 529 respondents, 49% of general practitioners (GPs) and 36% of pharmacists chose to administer both vaccines concomitantly when appropriate. COVID-19 or influenza vaccinations were otherwise postponed by 14 days for 22% of GPs and 34% of pharmacists. Finally, according to Stefanizzi et al.,29 1,643 (60%) of the 2,740 HCPs who attended the outpatient vaccination clinic of the Policlinico University Hospital of Bari (Italy) between October 12 and 24, 2021 chose coadministration, 718 (26.2%) chose to receive COVID-19 vaccine, and 379 (13.8%) to receive influenza vaccine. Coadministration acceptance was higher in HCPs directly involved in patient care (p < .001) and lower in nurses than in other HCPs (p = .001). Age was not associated with coadministration acceptance by Italian HCPs.
Discussion
Cocirculation of SARS-CoV-2 and influenza next autumn is uncertain, but coadministration of influenza and COVID-19 vaccines has been promoted and it seems important to synthesize available data about the safety and immunogenicity of this strategy. This review aims to inform, and hopefully reassure, future vaccinees and vaccinators.
No safety concerns or immune interferences were found with coadministration, regardless of which influenza or COVID-19 vaccines were administered and of age (65- or 65+). Although the number of studies (n = 3) and the total number of participants who received both vaccines (<1,500) are low, these results were extracted from well-conducted randomized studies. A retrospective cohort study published after the present literature search has collected patient self-reported vaccine data through a voluntary smartphone-based monitoring system on days 0 to 7 after vaccination. This study showed that respondents who concomitantly received an influenza vaccine and a booster dose of one of the two mRNA COVID-19 vaccines assessed were slightly more likely to report any health impact than those who received the mRNA COVID-19 vaccine alone (adjusted odds ratio, aOR = 1.05 [1.02–1.08]). No increased risk was reported for the other mRNA COVID-19 vaccine (aOR = 0.99 [0.97–1.02]).36 However, this observational study had limitations such as recruitment bias (volunteers with a complete COVID-19 vaccination, response by smartphone) or lack of distinction between the influenza vaccines used. Finally, the absence of safety alerts in countries that implemented coadministration for the 2021–2022 influenza season is reassuring for HCPs who will vaccinate individuals against influenza and COVID-19 in the coming influenza seasons and for those who will receive both vaccines concomitantly.10–13-37
Local and systemic reactions were frequent after coadministration and amplified by COVID-19 vaccination. The percentages of participants reporting at least one injection site reaction or at least one solicited systemic reaction were usually similar in coadministration and COVID-19 groups, and lower in influenza groups. These results were consistent with those of the literature showing that 50–90% of individuals who received COVID-19 vaccines reported adverse events including systemic adverse events for some individuals.20,38 However, serious adverse effects are rare with COVID-19 vaccines and vary between vaccines and brands for mRNA vaccines.38
As expected, no interference in immunological response was observed following coadministration. No interference is reported when inactivated influenza vaccines are coadministered with the vaccines of the routine childhood immunization program.1,7,39 Absence of interference is the rule for inactivated vaccines.40 However, as COVID-19 vaccines depend on new technologies, it seemed necessary to check. The various ongoing trials assessing the safety and immunogenicity of coadministration of influenza and COVID-19 vaccines at the time of writing of the present article demonstrate the interest in this topic (Supplementary Table S1).
As well as reassuring vaccinees and vaccinators, these results mainly taken from randomized controlled trials should improve vaccine coverage. From the vaccinees’ point of view, coadministration reduces the number of consultations, saves time, and may encourage vaccination with the two vaccines. Coadministration avoids any delay in protection. It also avoids schedule failures by missed opportunities or lack of motivation for a second injection. Surveys assessing the acceptability/acceptance of coadministration showed that acceptability and acceptance were good but could be improved. Acceptability was close to 100% in patients who had already received both vaccines in the clinical trial by Lazarus et al.20 It is to be noted that, from both vaccinees’ and vaccinators’ point of view, a combined vaccine would further improve acceptability (data not shown), in particular for subjects who are afraid of injections and those who develop severe local reactions at each injection site. In addition, a combined vaccine would save time for vaccinators. While awaiting combined vaccines, vaccinators (e.g., physicians, pharmacists) must be reassured of the possibility of administering the two vaccines concomitantly. From the point of view of the healthcare system, coadministration is cost-effective as demonstrated for other vaccinations.41 Administration of both vaccines at the same geographical place and at the same time could also lessen the burden of vaccination on healthcare systems. However, coadministration is not mandatory, and the two vaccines can be administered separately. In the event of a premature COVID-19 wave, ahead of the start of influenza vaccination, independent vaccination campaigns against COVID-19 and influenza would be a better choice.28
In Europe, COVID-19 has impacted national strategies. Pharmacists have been promoted as HCPs to enhance the roll-out of COVID-19 vaccination programs in numerous countries.42 Current policy and practice in relation to pharmacists’ involvement in vaccination vary between countries in Europe. The example of Portugal, one of the first countries where a pharmacist-led influenza vaccination service was implemented in order to enhance influenza vaccine coverage of at-risk populations,43 strongly suggests that policy favoring the implementation of both vaccinations in the same geographical place enhances vaccine coverage. On 16 June 2022, 72.6% of the European population had completed primary course COVID-19 vaccination and 52.1% had had a booster dose, compared to 86.2% and 64.3%, respectively, in Portugal.44 These national strategies implemented to maximize COVID-19 vaccination could now impact coadministration of influenza and COVID-19 vaccines. Moreover, while influenza vaccines are available in a prefilled syringe (i.e., single-dose presentation), COVID-19 vaccines are provided as multidose vials.
The present study has some limitations. Firstly, only ClinicalTrials and EudraCT were searched to identify clinical studies, and only articles with an Abstract written in English or in French were included in the analysis. The risk of bias was not ranked or graded. However, the PRISMA methodology was followed,30 characteristics of the selected studies are exposed in a transparent way (cf. Tables 1 and 2), and the safety and immunogenicity results were obtained from randomized clinical trials published in the Lancet or Lancet Respiratory Medicine.20,21,31 Secondly, few studies were identified, but additional results are expected in the forthcoming months. Thirdly, all the studies were performed on adult populations, no study assessed coadministration of live attenuated influenza and COVID-19 vaccines, and no study assessed coadministration efficacy or effectiveness. However, the coadministration of live attenuated influenza and COVID-19 vaccines is not a matter of concern as the current available live attenuated vaccine is for nasal administration in children. It should also be noted that coadministration of live attenuated influenza and COVID-19 vaccines can be implemented as live attenuated influenza vaccines are unlikely to be seriously affected by concomitant COVID-19 vaccination.19 Moreover, the COVID-19 vaccination schedule was a booster dose in only one of the three randomized controlled studies,31 whereas currently most of HCPs and 65+ have completed COVID-19 primary series.45 In addition, few people with heterogeneous characteristics were included in acceptability and acceptance studies. Finally, although coadministration of inactivated vaccines is usually not an issue, studies assessing the benefit and risk of coadministration of influenza and COVID-19 vaccines (and potentially other vaccines) are expected with the development of new COVID-19 vaccines.
In conclusion, a coupled influenza/COVID-19 vaccination campaign appears to be a good strategy to timely protect individuals against both infections and their complications and to reduce stress on healthcare systems for the coming winter in the event of concomitant influenza and COVID-19 epidemics. In the absence of combined vaccines, coadministration is the optimal method to successfully accomplish this strategy. In general, vaccine coadministration has been shown to be effective and more cost-effective than programs aimed at just one of the vaccines alone.46 Although few data are currently available, this literature review showed that coadministration of influenza and COVID-19 vaccines is possible and safe and does not induce immunological interference. Although no efficacy/effectiveness data are available, these results should reassure vaccinees and vaccinators. Public health decision-makers willing to implement a coupled influenza/COVID-19 vaccination campaign now need to create conditions allowing successful implementation (e.g., having a distribution circuit for both vaccines).
Supplementary Material
Acknowledgments
The authors want to thank Marie-Cécile Levant and Sandrine Samson (Sanofi) as well as Nicolas Kelle and Fabienne Péretz (Abelia Science) for their help in writing the manuscript. The article was written on MyPubli.online.
Funding Statement
Medical writing for this article was financially supported by Sanofi. The authors were not paid for the publication.
List of abbreviations
- AE
adverse event
- AESI
adverse event of special interest
- aTIV
adjuvanted trivalent influenza vaccine
- COVID-19
coronavirus infectious disease 2019
- GMC
geometric mean concentration
- GMT
geometric mean titer
- GP
general practitioner
- HI
hemagglutination inhibition
- HCP
healthcare professional
- MAAE
medically attended adverse event
- PICO
Population, Intervention, Comparison, Outcomes
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QIV
quadrivalent inactivated vaccine
- QIVc
cellular quadrivalent influenza vaccine
- QIV-HD
high-dose quadrivalent inactivated vaccine
- QIVr
recombinant quadrivalent influenza vaccine
- SAE
serious adverse event
- SARS-CoV-2
severe acute respiratory syndrome coronavirus-2
- TIV
trivalent influenza vaccine
- UK
United Kingdom
- USA
United States of America
- WHO
World Health Organization
Authors’ contributions
Cécile Janssen, Anne Mosnier, Gaëtan Gavazzi, Behazine Combadière, Pascal Crépey, Jacques Gaillat, Odile Launay, Elisabeth Botelho-Nevers made a significant contribution to the work reported (conception, validation of study design, analysis, and interpretation) and have critically reviewed the manuscript. They agreed on the journal to which the article was submitted. They reviewed the final version of manuscript and agreed on its submission.
The first author agreed to take responsibility and be accountable for the contents of the article and to share responsibility to resolve any questions raised about the accuracy or integrity of the published work.
Disclosure statement
C.J. reports fees for board membership from AstraZeneca, Pfizer, Sanofi and MSD, consultant and speaker for these companies, participation in congresses on invitation by these companies.
A.M. reports to participate in an advisory committee organized by Sanofi and to be a member of the scientific board of the GEIG and the scientific board of the POSTHER study (Herpes Zoster Study, GSK).
G.G. reports to participate in advisory committees organized by Astellas, AstraZeneca, BioMérieux, MSD, Pfizer, Sanofi, Sanofi Pasteur, Sanofi Pasteur-MSD and Vifor, consultant and speaker for these companies, participation in congresses on invitation by Eisai, MSD, Novartis, Pfizer, Sanofi, and Vifor.
B.C. reports to participate in advisory board organized by AstraZeneca, Sanofi and Osivax and to participate to conferences on invitation by Pfizer and GSK.
P.C. reports to participate in advisory committees organized by Sanofi and being consultant for Sanofi.
J.G. reports to participate in advisory committees organized by GSK, MSD, Pfizer, and Sanofi.
O.L. reports to be principal investigator in vaccine trials sponsored by Sanofi, MSD, Pfizer, GSK, Moderna. She received financial support for traveling to medical congress and personal fees for participation to advisory boards for Sanofi, MSD, Pfizer, and GSK.
E.B.-N. conducts vaccine trials including COVID-19 trials using Janssen, Pfizer, Moderna, and Sanofi COVID-19 vaccines. She participated in vaccines scientific advisory boards for Pfizer, Janssen, and Sanofi with honoraria paid to her institution.
Supplementary material
Supplemental data for this article can be accessed on the publisher’s website at https://doi.org/10.1080/21645515.2022.2131166.
References
- 1.WHO, World Health Organization . Vaccines against influenza: wHO position paper. Weekly Epidemiological Record. 2022. May 13 [accessed 2022 Jun 21]. https://www.who.int/publications-detail-redirect/who-wer9719-185-208.
- 2.Melidou A, Ködmön C, Nahapetyan K, Kraus A, Alm E, Adlhoch C, Mooks P, Dave N, Carvalho C, Meslé M, et al. Influenza returns with a season dominated by clade 3c.2a1b.2a.2 A(H3N2) viruses, WHO European region, 2021/22. Euro Surveill. 2022;27(15):1. PII: 2200255. doi: 10.2807/1560-7917.ES.2022.27.15.2200255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Australian Government Department of health . Australian influenza surveillance report - No 05 - fortnight ending 05 June 2022. Australia: Australian Government Department of Health; 2022. Report No: 05. [Google Scholar]
- 4.Li Y, Campbell H, Kulkarni D, Harpur A, Nundy M, Wang X, Nair H.. The temporal association of introducing and lifting non-pharmaceutical interventions with the time-varying reproduction number (R) of SARS-CoV-2: a modelling study across 131 countries. Lancet Infect Dis. 2021;21(2):193–12. doi: 10.1016/S1473-3099(20)30785-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Han S, Zhang T, Lyu Y, Lai S, Dai P, Zheng J, Yang W, Zhou X, Feng L. The incoming influenza season - China, the United Kingdom, and the United States, 2021-2022. China CDC Wkly. 2021;3:1039–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schaffer DeRoo S, Pudalov N, Fu L. Planning for a COVID-19 vaccination program. JAMA. 2020;323(24):2458–59. doi: 10.1001/jama.2020.8711. [DOI] [PubMed] [Google Scholar]
- 7.WHO, World Health Organization Vaccines against influenza WHO position paper — November 2012 = Note de synthèse de l’oms concernant les vaccins antigrippaux — novembre 2012. Wkly Epidemiol Rec. 2012. Nov 13 [accessed 2022 Apr 21];87:461–76 https://apps.who.int/iris/handle/10665/241993.23210147 [Google Scholar]
- 8.Domnich A, Orsi A, Trombetta C, Guarona G, Panatto D, Icardi G. COVID-19 and seasonal influenza vaccination: cross-protection, co-administration, combination vaccines, and hesitancy. Pharmaceuticals. 2022;15(3):322. doi: 10.3390/ph15030322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Watson O, Barnsley G, Toor J, Hogan A, Winskill P, Ghani A. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis. 2022;S1473-3099:00320–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.WHO, World Health Organization . Coadministration of seasonal inactivated influenza and COVID-19 vaccines: interim guidance. 2021. Oct 21 [accessed 2022 Apr 14]. https://apps.who.int/iris/handle/10665/346897.
- 11.Santé publique, Sécurité de la chaine alimentaire et environnement, SPF Santé publique . Avis 9675 - vaccination simultanée COVID-19. 2021. Oct 7 [accessed 2022 Feb 7]. https://www.health.belgium.be/fr/avis-9675-vaccination-simultanee-covid-19.
- 12.Del af Statens Serum Institut . Spørgsmål og svar om covid-19-vaccination. [accessed 2022 Feb 7]. https://covid19.ssi.dk/vaccination/sporgsmaal-og-svar.
- 13.Finnish Institute, Finnish Institute for Health and Welfare (THL) . New recommendations for coronavirus vaccinations – pregnant women may take a coronavirus vaccine if they wish - Press release - THL. Finland; [accessed 2022 Feb 7]. https://thl.fi/en/web/thlfi-en/-/new-recommendations-for-coronavirus-vaccinations-pregnant-women-may-take-a-coronavirus-vaccine-if-they-wish. [Google Scholar]
- 14.HAS, Haute Autorité de Santé . Covid-19 et grippe: undefined HAS précise les conditions d’une co-administration des vaccins. 2021. Sept 27 [accessed 2022 Feb 7]. https://www.has-sante.fr/jcms/p_3288855/fr/covid-19-et-grippe-la-has-precise-les-conditions-d-une-co-administration-des-vaccins.
- 15.RKI, Robert Koch Institut . STIKO-Empfehlung zur Koadministration von COVID-19-Impfstoffen und anderen Totimpfstoffen und die dazugehörige wissenschaftliche Begründung. Archiv. 2021. Sep 30 [accessed 2022 Feb 7]. https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2021/39/Art_03.html#: :text=Wie%20das%20Epidemiologische%20Bulletin%2039,24.9.2021%20online%20vorab%20ver%C3%B6ffentlicht.
- 16.Ministero de la Salute (IMH) . Influenza e vaccinazione antinfluenzale. FAQ. 2021. Oct 4 [accessed 2022 Feb 7]. https://www.salute.gov.it/portale/influenza/dettaglioFaqInfluenza.jsp?lingua=italiano&id=103
- 17.Ministerio de Sanidad . Preguntas y Respuestas Sobre la Vacunacion Frente a la Gripe. 2021. Oct [accessed 2022 Feb 07]. https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/programasDeVacunacion/gripe/faq/docs/Preguntas_respuestas_gripe_ciudadanos_2021-2022.pdf.
- 18.Office fédéral de la santé publique (OFSP) et Commission fédérale pour les vaccinations (CFV) . Recommandations de vaccination avec des vaccins à ARNm contre le COVID-19 (état au 23.5.2022). Switzerland; 2022. May 23. [Google Scholar]
- 19.UK Health Security Agency . In: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1102459/Greenbook-chapter-14a-4September22.pdf 28 February 2022. 2022. COVID-19: the green book, chapter 14a Sept 05.
- 20.Lazarus R, Baos S, Cappel-Porter H, Carson-Stevens A, Clout M, Culliford L, Emmett S, Garstang J, Gbadamoshi L, Hallis B, et al. Safety and immunogenicity of concomitant administration of COVID-19 vaccines (ChAdox1 or BNT162b2) with seasonal influenza vaccines in adults in the UK (ComFlucov): a multicentre, randomised, controlled, phase 4 trial. Lancet. 2021;398(10318):2277–87. doi: 10.1016/S0140-6736(21)02329-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Toback S, Galiza E, Cosgrove C, Galloway J, Goodman A, Swift P, Rajaram S, Graves-Jones A, Edelman J, Burns F, et al. Safety, immunogenicity, and efficacy of a COVID-19 vaccine (NVX-CoV2373) co-administered with seasonal influenza vaccines: an exploratory substudy of a randomised, observer-blinded, placebo-controlled, phase 3 trial. Lancet Respir Med. 2022;10(2):167–79. doi: 10.1016/S2213-2600(21)00409-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dadashi M, Khaleghnejad S, Abedi Elkhichi P, Goudarzi M, Goudarzi H, Taghavi A, Vaezjalali M, Hajikhani B. COVID-19 and influenza co-infection: a systematic review and meta-analysis. Front Med. 2021;8:681469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sentinelles . Observed situation in general practice for the week 8 of the year 2022, from 02/21/2022 to 02/27/2022. 2022. May 27 [accessed 2022 May 27]. https://www.sentiweb.fr/5558.pdf.
- 24.Santé publique France . Bulletin épidémiologique grippe, semaine 19. Saison 2021-2022. [accessed 2022 May 18]. https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/grippe/documents/bulletin-national/bulletin-epidemiologique-grippe-semaine-19.-saison-2021-2022.
- 25.Stowe J, Tessier E, Zhao H, Guy R, Muller-Pebody B, Zambon M, Andrews N, Ramsay M, Lopez Bernal J. Interactions between SARS-CoV-2 and influenza, and the impact of coinfection on disease severity: a test-negative design. Int J Epidemiol. 2021;50(4):1124–33. doi: 10.1093/ije/dyab081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Swets M, Russell C, Harrison E, Docherty A, Lone N, Girvan M, Hardwick H, Visser L, Openshaw P, Groeneveld G, et al. SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses. Lancet. 2022;399:1463–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Baker R, Park S, Yang W, Vecchi G, Metcalf C, Grenfell B. The impact of COVID-19 nonpharmaceutical interventions on the future dynamics of endemic infections. Proc Natl Acad Sci U S A. 2020;117(48):30547–53. doi: 10.1073/pnas.2013182117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Haute Autorité de Santé . Stratégie de vaccination contre la Covid-19 – anticipation des scénarios possibles à l’automne 2022. 2022. May 25 [accessed: 2022 May 27]. https://www.has-sante.fr/jcms/p_3340479/fr/strategie-de-vaccination-contre-la-covid-19-anticipation-des-scenarios-possibles-a-l-automne-2022.
- 29.Stefanizzi P, Martinelli A, Bianchi F, Migliore G, Tafuri S. Acceptability of the third dose of anti-SARS-CoV-2 vaccine co-administered with influenza vaccine: preliminary data in a sample of Italian HCWs. Hum Vaccin Immunother. 2022;18(1):1–2. doi: 10.1080/21645515.2021.2011652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Page M, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C, Shamseer L, Tetzlaff J, Akl E, Brennan S, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89. doi: 10.1186/s13643-021-01626-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Izikson R, Brune D, Bolduc J, Bourron P, Fournier M, Moore T, Pandey A, Perez L, Sater N, Shrestha A, et al. Safety and immunogenicity of a high-dose quadrivalent influenza vaccine administered concomitantly with a third dose of the mRNA-1273 SARS-CoV-2 vaccine in adults aged ≥65 years: a phase 2, randomised, open-label study. Lancet Respir Med. 2022;10:392–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Domnich A, Grassi R, Fallani E, Spurio A, Bruzzone B, Panatto D, Marozzi B, Cambiaggi M, Vasco A, Orsi A, et al. Changes in attitudes and beliefs concerning vaccination and influenza vaccines between the first and second COVID-19 pandemic waves: a longitudinal study. Vaccines. 2021;9(9):1016. doi: 10.3390/vaccines9091016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Domnich A, Grassi R, Fallani E, Ciccone R, Bruzzone B, Panatto D, Ferrari A, Salvatore M, Cambiaggi M, Vasco A, et al. Acceptance of COVID-19 and influenza vaccine co-administration: insights from a representative Italian survey. J Pers Med. 2022;12(2):139. doi: 10.3390/jpm12020139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.COVIGIE . [accessed 2022 May 31]. https://covigie.org/enquete-express/numero-5-resultat?liste=site-covigie.
- 35.Ma L, Yang J, Zhang T, Han X, Huang Q, Yang Y, Feng L, Yang W, Wang C. Willingness toward COVID-19 vaccination, coadministration with other vaccines and receive a COVID-19 vaccine booster: a cross-sectional study on the guardians of children in China. Hum Vaccin Immunother 18 5 . 2022:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hause A, Zhang B, Yue X, Marquez P, Myers T, Parker C, Gee J, Su J, Shimabukuro T, Shay D. Reactogenicity of simultaneous COVID-19 mRNA booster and influenza vaccination in the US. JAMA Netw Open. 2022;5:e2222241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hu C, Tang Y, Su Q, Lei Y, Cui W, Zhang Y, Zhou Y, Li X, Wang Z, Zhao Z. Public health measures during the COVID-19 pandemic reduce the spread of other respiratory infectious diseases. Front Public Health. 2021;9:771638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Beatty A, Peyser N, Butcher X, Cocohoba J, Lin F, Olgin J, Pletcher M, Marcus G. Analysis of COVID-19 vaccine type and adverse effects following vaccination. JAMA Netw Open. 2021;4(12):e2140364. doi: 10.1001/jamanetworkopen.2021.40364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.WHO, World Health Organization . Wh 202127o flumart outputs. [accessed 2022 Apr 21]. http://www.who.int/flunet.
- 40.ACIP . Timing and spacing guidelines for immunization. CDC. 2022. Apr 14. https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/timing.html.
- 41.Ament A, Baltussen R, Duru G, Rigaud-Bully C, de Graeve D, Ortqvist A, Jönsson B, Verhaegen J, Gaillat J, Christie P, et al. Cost-effectiveness of pneumococcal vaccination of older people: a study in 5 western European countries. Clin Infect Dis. 2000;31:444–50. [DOI] [PubMed] [Google Scholar]
- 42.Paudyal V, Fialová D, Henman M, Hazen A, Okuyan B, Lutters M, Cadogan C, da Costa F, Galfrascoli E, Pudritz Y, et al. Pharmacists’ involvement in COVID-19 vaccination across Europe: a situational analysis of current practice and policy. Int J Clin Pharm. 2021;43(4):1139–48. doi: 10.1007/s11096-021-01301-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kirkdale C, Nebout G, Taitel M, Rubin J, Jacinto I, Horta R, Megerlin F, Thornley T. Implementation of flu vaccination in community pharmacies: understanding the barriers and enablers. Ann Pharm Fr. 2017;75(1):9–16. doi: 10.1016/j.pharma.2016.08.006. [DOI] [PubMed] [Google Scholar]
- 44.ECDC, European Centre for Disease Prevention and Control . COVID-19 vaccine tracker. [accessed 2022 May 25]. https://vaccinetracker.ecdc.europa.eu/public/extensions/covid-19/vaccine-tracker.html#uptake-tab.
- 45.Ministère des solidarités et de la santé . Le Tableau de bord de la vaccination. [accessed 2022 May 25]. https://solidarites-sante.gouv.fr/grands-dossiers/vaccin-covid-19/article/le-tableau-de-bord-de-la-vaccination.
- 46.Gilchrist S, Nanni A, Levine O. Benefits and effectiveness of administering pneumococcal polysaccharide vaccine with seasonal influenza vaccine: an approach for policymakers. Am J Public Health. 2012;102(4):596–605. doi: 10.2105/AJPH.2011.300512. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.