

TO THE EDITOR,
The term inflammatory myofibroblastic tumor (IMT) refers to a tumor with chronic inflammatory infiltrate, aggressive behavior, and evidence of chromosomal rearrangement, especially anaplastic lymphoma kinase (ALK) translocation. 1
Here, we report a rare case of a myofibroblastic lung tumor with ALK translocation in a 50-year-old man, a former smoker, who complained of myalgias, sudoresis, fever, and weight loss for the past two months.
Initial thoracic computed tomography (CT) revealed a solid mass measuring 3.3 cm x 3 cm in the left pulmonary apex, and a positron emission tomography (PET) scan detected hypermetabolic uptake (SUV-26) in the pulmonary lesion, as well as diffuse exuberant osteomedullary hypermetabolism. Bronchioalveolar lavage was negative for mycobacteria and other microorganisms, and two transbronchial and one transthoracic biopsy only evidenced a chronic inflammatory infiltrate. A myelogram suggested a monoclonal gammopathy of undetermined significance.
Following failed attempts at diagnosis, the patient exhibited refractory fever, pleuritic pain, and productive cough. A follow-up CT detected the growth of the left pulmonary mass; thus, lobectomy was proposed (Figure 1A).
Figure 1. Computed tomography (CT) images. A - Left pulmonary apex with necrotic and abcessed tissue. B - Hepatic abcessed/nodular lesion with necrotic component.
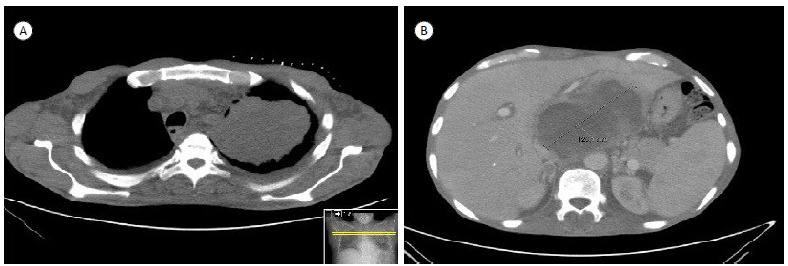
The intraoperative descriptions indicated a liquefied purulent mass. After surgery, the patient developed marked epigastralgia, and an abdominal CT revealed a hepatic lesion with a necrotic center (Figure 1B). Hepatic biopsy evidenced a necrotic liquefied and purulent content. Also, because of a transitory loss of consciousness, cranial CT was performed, with the identification of an intra-axial lesion suggestive of secondary deposit.
The histopathology of the lung specimen and cytology of the hepatic punction revealed an epithelioid variant of IMT in the lung, with ALK rearrangement. The patient started Crizotinib, with no time to establish an eventual response as he died 5 days later.
The biological behavior of IMTs is highly unpredictable and has a wide spectrum of severity. For years, there has been controversy regarding whether it should be categorized as a reactive lesion to an infection or local trauma with an aggressive local inflammatory response or an actual neoplastic lesion. The term “inflammatory myofibroblastic tumors” emerged in the past years according to the recent WHO classification of soft tissue tumors. 2 The expression of ALK-1 documented in approximately 50% of IMTs has contributed to distinguishing these tumors from other nonspecific inflammations, pointing also to a better prognosis of IMTs with ALK rearrangement. Distant metastases, although rare, may occur, primarily in ALK-negative IMTs. 1
These tumors are most frequent in children and young adults, accounting for around 50% of all pulmonary neoplasms in infants and less than 1% of lung tumors in adults. 3 Due to the broad spectrum of radiological manifestations and nonspecific clinical behavior, these tumors are difficult to diagnose. Surgical resection is usually performed in solitary lesions in order to establish the diagnosis and provide adequate treatment. Complete surgical resection with clear margins is associated with a favorable prognosis. 4 Radiation may also be applied in recurrent cases or situations of local organ invasion. 5
Despite the scarce evidence regarding the treatment of these tumors in adults, Crizotinib is widely used and effective in patients with ALK-positive non-small-cell lung cancer. Discussing the rationale for genomic target therapy, several case reports in which ALK inhibitors were used, namely Crizotinib, in ALK-positive IMTs, reported variable degrees of success. 5 - 7 A prospective study involving 20 patients with advanced, inoperable IMTs with ALK translocation stated that Crizotinib was an active treatment associated with objective responses in 50% of patients, with long-lasting progression-free survival in most of them. 8
In this case, the explosive local and metastatic growth conjectured the worsening of the prognosis, and Crizotinib was used as an unsuccessful lifesaving attempt. The highly variable reported outcomes, in addition to the lack of experience in most cancer centers in adult IMT, make the treatment still a matter of debate.
REFERENCES
- 1.Coffin CM, Patel A, Perkins S, Elenitoba-Johnson KSJ, Perlman E, Griffin CA. ALK1 and p80 Expression and Chromosomal Rearrangements Involving 2p23 in Inflammatory Myofibroblastic Tumor. Mod Pathol. 2001;14(6):569–576. doi: 10.1038/modpathol.3880352. [DOI] [PubMed] [Google Scholar]
- 2.Jo VY, Fletcher CDM. WHO classification of soft tissue tumours an update based on the 2013 (4th) edition. Pathology. 2014;46(2):95–104. doi: 10.1097/PAT.0000000000000050. [DOI] [PubMed] [Google Scholar]
- 3.Al-Obaidi A, Buess C, Mogire J, Reddy PS. Inflammatory Myofibroblastic Tumor of the Lung An Extremely Rare Condition in Adults. Cureus. 2019;11(12):e5432. doi: 10.7759/cureus.6432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Khalil S, Ghafoor T, Raja AKF. Inflammatory Myofibroblastic Tumor A Rare Presentation and an Effective Treatment with Crizotinib. Case Rep Oncol Med. 2020;2020:6923103–6923103. doi: 10.1155/2020/6923103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Alan O, Kuzhan O, Koca S, Telli TA, Basoglu T, Ercelep O. How long should we continue crizotinib in ALK translocation-positive inflammatory myofibroblastic tumors Long-term complete response with crizotinib and review of the literature. J Oncol Pharm Pract. 2020;26(4):1011–1018. doi: 10.1177/1078155219879757. [DOI] [PubMed] [Google Scholar]
- 6.Chennouf A, Arslanian E, Roberge D, Berthelet F, Bojanowski M, Bahary JP. Efficiency of Crizotinib on an ALK-Positive Inflammatory Myofibroblastic Tumor of the Central Nervous System A Case Report. Cureus. 2017;9(3):e1068. doi: 10.7759/cureus.1068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mansfield AS, Murphy SJ, Harris FR, Robinson SI, Marks RS, Johnson SH. Chromoplectic TPM3-ALK rearrangement in a patient with inflammatory myofibroblastic tumor who responded to ceritinib after progression on crizotinib. Ann Oncol. 2016;27(11):2111–2117. doi: 10.1093/annonc/mdw405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Schöffski P, Sufliarsky J, Gelderblom H, Blay JY, Strauss SJ, Stacchiotti S. Crizotinib in patients with advanced, inoperable inflammatory myofibroblastic tumours with and without anaplastic lymphoma kinase gene alterations (European Organisation for Research and Treatment of Cancer 90101 CREATE) a multicentre, single-drug, prospective, non-randomised phase 2 trial. Lancet Respir Med. 2018;6(6):431–441. doi: 10.1016/S2213-2600(18)30116-4. [DOI] [PubMed] [Google Scholar]