

ABSTRACT
Objective:
To evaluate COVID-19 knowledge, attitudes, and practices among health care workers (HCWs) practicing in Latin American countries during the first surge of the COVID-19 pandemic.
Methods:
This was a multinational cross-sectional survey study, using an online self-administered questionnaire. The final version of the questionnaire comprised 40 questions, organized in five sections: demographic and professional characteristics; COVID-19 knowledge; attitudes toward COVID-19; COVID-19 practices; and institutional resources.
Results:
The study involved 251 HCWs from 19 Latin American countries who agreed to participate. In our sample, 77% of HCWs participated in some sort of institutional training on COVID-19, and 43% had a low COVID-19 knowledge score. COVID-19 knowledge was associated with the type of health center (public/private), availability of institutional training, and sources of information about COVID-19. Concerns about not providing adequate care were reported by 60% of the participants. The most commonly used ventilatory strategies were protective mechanical ventilation, alveolar recruitment maneuvers, and prone positioning, and the use of drugs to treat COVID-19 was mainly based on institutional protocols.
Conclusions:
In this multinational study in Latin America, almost half of HCWs had a low COVID-19 knowledge score, and the level of knowledge was associated with the type of institution, participation in institutional training, and information sources. HCWs considered that COVID-19 was very relevant, and more than half were concerned about not providing adequate care to patients.
Keywords: COVID-19; Health knowledge, attitude, practice; Health personnel; Latin America
RESUMO
Objetivo:
Avaliar o conhecimento, atitudes e práticas em relação à COVID-19 entre profissionais de saúde atuantes em países da América Latina durante o primeiro surto da pandemia.
Métodos:
Estudo multinacional transversal com uso de questionário on-line autoaplicável. A versão final do questionário foi composta por 40 perguntas, organizadas em cinco seções: características demográficas e profissionais; conhecimento sobre COVID-19; atitudes em relação à COVID-19; práticas relacionadas à COVID-19; e recursos institucionais.
Resultados:
O estudo envolveu 251 profissionais de saúde de 19 países da América Latina que aceitaram participar. Em nossa amostra, 77% dos profissionais de saúde participaram de algum tipo de treinamento institucional sobre COVID-19 e 43% tiveram baixa pontuação de conhecimento sobre COVID-19. O conhecimento sobre COVID-19 apresentou associação com o tipo de instituição de saúde (pública/privada), disponibilidade de treinamento institucional e fontes de informação. Receio de não prestar atendimento adequado foi relatado por 60% dos participantes. As estratégias ventilatórias mais utilizadas foram ventilação mecânica protetora, manobras de recrutamento alveolar e posição prona, e o uso de medicamentos para tratar a COVID-19 foi baseado principalmente em protocolos institucionais.
Conclusões:
Neste estudo multinacional na América Latina, quase metade da amostra teve baixa pontuação de conhecimento sobre COVID-19 e o nível de conhecimento apresentou associação com o tipo de instituição, participação em treinamento institucional e fontes de informação. Os profissionais de saúde consideravam a COVID-19 muito relevante, e mais da metade tinha receio de não prestar atendimento adequado aos pacientes.
Descritores: COVID-19; Conhecimentos, atitudes e prática em saúde; Profissionais de saúde; América Latina
INTRODUCTION
In December of 2019, a new infectious disease caused by a beta coronavirus was identified in the province of Wuhan, China. 1 - 5 Since then, the virus has spread around the globe and infected nearly 174 million individuals and more than 3 million people have died as of June of 2021. 6
Research studies from all over the globe described the modes of transmission, which are now known to include mainly contact with respiratory droplets and aerosols, 7 , 8 whereas clinical studies have revealed that the most common symptoms of COVID-19 were fever, cough, headache, myalgia, dyspnea, and fatigue. 9 , 10 Additionally, clinical manifestations ranged from mild to severe illness and death, although a significant proportion of subjects infected with the virus never developed symptoms. 11
Health care workers (HCWs) are at highest risk of being infected since they provide direct care to infected patients. 8 The implementation of standard contact and respiratory precautions, as well as the use of adequate personal protective equipment (PPE), such as N95 masks, eye protection with goggles, and face shields; regular hand washing with soap or disinfection with alcohol hand sanitizer; maintenance of a distance of 1.5-2 m from other people; and avoidance of touching eyes, nose, and mouth constitute the major preventive measures against contamination. 4 , 8
Medical institutions in low-resource settings, such as Latin America, had limited access to PPE during the first surge of COVID-19 in early 2020. 12 , 13 In addition, the lack of institutional clinical protocols and training, increase in work hours, and shortage of resources, including ICU beds, medications, and ventilators, posed additional barriers to HCWs to care for patients with COVID-19 in those settings.
Adequate knowledge, attitudes, and practices (KAP) toward COVID-19-related diseases among HCWs may decrease the risk of infection and impact patient outcomes. 8 , 14 - 16 Therefore, institutions should ensure that frontline workers have access to information, adequate training, and emotional preparation, as well as access to PPE and resources, in order to provide evidence-based care to COVID-19 patients. 17 , 18
The objective of this study was to evaluate COVID-19 KAP among HCWs practicing in Latin America countries during the first surge of the COVID-19 pandemic.
METHODS
Study design and sample
This was a cross-sectional survey study using an online self-administered questionnaire. The study was approved by the Research Ethics Committee of the University of São Paulo Medical School (approval numbers: SDC 5047/20/076 and CAAE 32048620.0.0000.0068), and informed consent was electronically obtained from all participants before their answering of the survey questions (written self-administered electronic informed consent).
The inclusion criterion was being an HCW in Latin America, and the exclusion criterion was refusal to sign the informed consent. Invitations to participate in the study were sent by the Asociación Latinoamericana de Tórax (ALAT, Latin American Thoracic Society) to all members, via email, between June and October of 2020. In addition, the investigators sent invitations using social media, with a link to access the questionnaire, using a snowballing strategy to reach a broader group of HCWs, including those who were not ALAT members.
KAP questionnaire design
The questions on the questionnaire were developed based on contents and recommendations by the US Centers for Disease Control and Prevention, 19 the Associação de Medicina Intensiva Brasileira (AMIB, Brazilian Critical Care Association), 20 and the WHO. 4 The questionnaire was developed in Portuguese and then translated into Spanish by bilingual researchers using the back-translation process.
A panel of experts, consisting of one infectious disease physician, one pulmonologist, one respiratory therapist, and one nurse, reviewed the questionnaire for comprehensiveness, clarity, and relevance. These experts also evaluated face and content validity of the questions. 21
The final version of the questionnaire, after several rounds of review and expert evaluation, comprised 40 questions organized in five sections.
The first section focused on demographic and professional characteristics, including age, gender, job category (physician, respiratory therapist/physiotherapist, nurse, and other), work experience, and type of institution of employment (Table S1).
The second section evaluated knowledge about COVID-19. The knowledge section included 10 multiple choice questions on sources of information about COVID-19, training, prevention, diagnosis, and treatment. Correct answers to knowledge questions were given a score of 1, while incorrect or “I don’t know” answers were given a score of 0. Hence, the maximum score on this section was 10. Participants with scores ≥ 6 were considered to have a high level of knowledge about COVID-19.
The third section assessed attitudes toward COVID-19 and comprised 10 questions. Five questions assessed the perception of relevance of COVID-19, using a Likert scale ranging from 1 (not important) to 5 (very important), and the subsequent 5 questions assessed fears or concerns regarding the disease, the first 4 questions using a Likert scale ranging from 1 (strong fear) to 5 (no fear), and 1 dichotomous (yes/no) question regarding fear of not providing adequate care to COVID-19 patients, scored as 5 and 0 points, respectively. When respondents answered “Yes” to this question, they were asked about the reasons for such fear with 6 additional yes/no questions, which did not count for the attitude score. Attitude scores ranged from 10 (worst attitude) to 50 (best attitude).
The fourth section included three subsections describing practices regarding COVID-19. The first subsection included 8 yes/no questions about COVID-19 clinical practices. The second subsection inquired about ventilatory strategies for patients on mechanical ventilation (MV) using a 4-point Likert scale (“Always”, “Sometimes”, “Never” and “I don’t know”). The last subsection had 7 questions about treatment, including the use of specific medications for COVID-19, such as hydroxychloroquine/chloroquine, azithromycin, remdesivir, lopinavir/ritonavir, tocilizumab, systemic steroids, and convalescent plasma.
The fifth section assessed institutional resources available for patient care, such as numbers of hospital and ICU beds, number of mechanical ventilators, and PPE.
Statistical analysis
Data were collected and managed using the REDCap platform (Vanderbilt University, Nashville, TN, USA) hosted at ALAT. 22 , 23
The study sample size was calculated based on the proportion of HCWs with a sufficient level of knowledge about COVID-19. A previous publication reported that 89% of HCWs had sufficient knowledge on COVID-19. 24 We predicted that 60% of HCWs would be considered to have a sufficient knowledge, and we used a 5% margin of error (95% CI), resulting in a sample size of 150 participants.
Categorical variables were described as absolute and relative frequencies, as were continuous variables described as means and standard deviations in order to characterize the study population. We used the Fisher’s exact test and chi-square tests for comparisons between participants with knowledge scores above and below the median.
All data were entered and analyzed using the R statistical package, version 4.0.3 ((The R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p < 0.05.
RESULTS
Between June and October of 2020, 251 HCWs from 19 Latin American countries agreed to participate in the study. The main characteristics of the study respondents are presented in Table 1. Respondents were mainly from Mexico, Brazil, Argentina, and Colombia. The participation was very low in some countries: Bolivia (1.2%), Costa Rica (1.2%), Guatemala (1.2%), Honduras (0.4%), Nicaragua (1.2%), and Panama (1.2%), which added up to 6% of the sample. The mean age was 48 ± 13 years, and 62% of the sample were male. The majority of respondents were physicians, with a long period of professional experience (> 15 years), and currently working in a hospital or in a health care center. Nearly half of the respondents worked in public institutions, and 77% reported having participated in some sort of COVID-19 institutional training. The most commonly used sources of COVID-19 information were scientific publications, scientific society recommendations, and official government websites.
Table 1. Characteristics of the respondents (N = 251).a .
| Country | Result |
|---|---|
| Mexico | 48 (19) |
| Brazil | 36 (14) |
| Argentina | 29 (12) |
| Colombia | 27 (11) |
| Chile | 23 (9) |
| Ecuador | 17 (7) |
| Peru | 15 (6) |
| Venezuela | 9 (4) |
| Cuba | 6 (2) |
| Uruguay | 6 (2) |
| El Salvador | 5 (2) |
| Paraguay | 5 (2) |
| Dominican Republic | 5 (2) |
| Other | 16 (6) |
| Age, years | 48 ± 13 |
| Sex - Male | 156 (62) |
| Profession | |
| Physician | 213 (85) |
| Respiratory therapist/physiotherapist | 28 (11) |
| Nurse | 4 (2) |
| Other | 6 (2) |
| Experience, years | 20 [12-31] |
| Currently working in a hospital or clinic | 224 (89) |
| Hospital type | |
| Public | 131 (52) |
| Private | 67 (27) |
| University | 20 (8) |
| Mixed | 22 (9) |
| Philanthropic | 2 (1) |
| Other | 4 (2) |
| Direct care for COVID-19 patients | 217 (87) |
| Working in the ICU | 68 (27) |
| Working in the ER | 53 (21) |
| Researcher | 23 (9) |
| Academic supervisor | 52 (21) |
| Chief of staff | 32 (13) |
| Director | 8 (3) |
| Previously tested positive for COVID-19 | 39 (16) |
| Institutional training on COVID-19 | 194 (77) |
| Sources of information on COVID-19 | |
| Scientific publications in academic journals | 213 (85) |
| Professional or scientific society recommendations | 211 (84) |
| Official government websites | 192 (77) |
| Recommendations from other institutions | 100 (40) |
| Colleagues | 90 (36) |
| Media (e.g., TV, radio, newspaper) | 62 (25) |
| Social media (e.g., Facebook, Instagram, WhatsApp) | 59 (24) |
| Family and friends | 7 (3) |
| Other | 13 (5) |
Values expressed as n (%), mean ± SD, or median [IQR].
Table 2 presents the proportion of correct answers for each of the 10 knowledge questions. The median knowledge score (range, 0 to 10) was 6 (IQR: 5-6). In our sample, 107 participants (43%) had low knowledge scores (score < 6). Among the participants who had an adequate knowledge score (score ≥ 6), 17 (7% of the overall sample) had a knowledge score ≥ 8. Knowledge about asymptomatic presentation of COVID-19, risk factors, diagnostic criteria, and prevention measures was high, but that on COVID-19 treatment, transmission, complications, and protective MV was low.
Table 2. Performance on the COVID-19 knowledge section (N = 251).a .
| Question and topic | Correct answer |
|---|---|
| K1: Incubation period | 158 (63) |
| K2: Risk factors | 231 (92) |
| K3: Diagnostic criteria | 212 (85) |
| K4: Asymptomatic presentation | 245 (98) |
| K5: Transmission | 50 (20) |
| K6: Prevention measures | 202 (81) |
| K7: Treatment | 60 (24) |
| K8: Complications | 47 (19) |
| K9: Indication of mechanical ventilation | 158 (63) |
| K10: Protective mechanical ventilation | 41 (16) |
K: question in the COVID-19 knowledge section. aValues expressed as n (%).
The results in the attitude section are summarized in Figure 1. The median score was 43 (IQR: 38-49). There was no significant association between scores and characteristics of respondents (Table S1). The majority of the participants believed that COVID-19 was a very relevant issue in their institution, their country, and worldwide. Participants were more concerned about infecting family members than about being infected. Overall, respondents were very afraid of not having access to testing (40%) or medical assistance (60%) if they had COVID-19. In addition, 60% reported being concerned about not providing adequate patient care, the major reasons for that being lack of staff, lack of PPE, work overload, and ethical dilemmas.
Figure 1. Attitudes toward COVID-19. The width of bars represents the proportion of respondents that marked each response. A: question in the attitude section; and PPE: personal protective equipment. *≤ 1%.
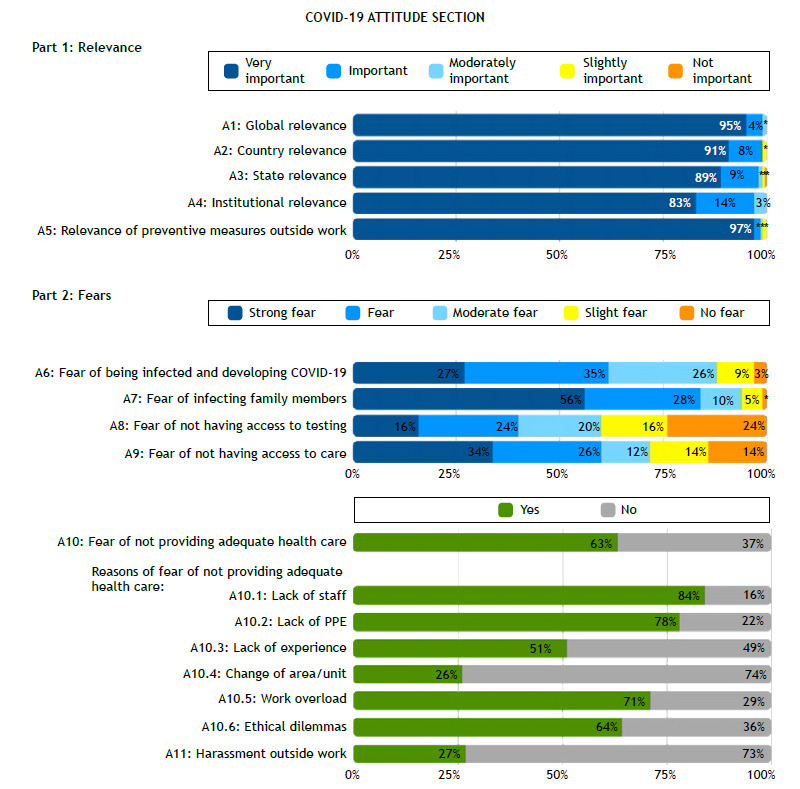
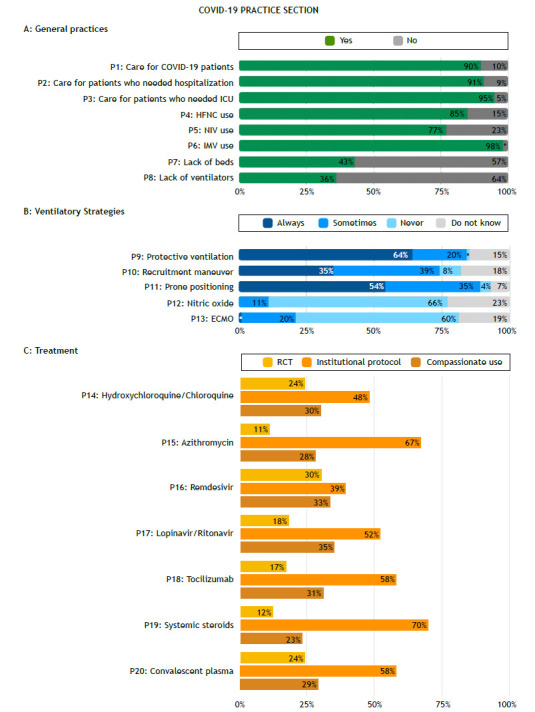
Figure 2 summarizes the results in the practice section. Nearly all participants reported caring for patients in the ICU (95%) on MV (98%). Almost half of the respondents reported lack of beds, and one third reported lack of mechanical ventilators in the institutions they worked at. The most commonly used ventilatory strategies for COVID-19 patients were protective MV, alveolar recruitment maneuvers, and prone positioning. Regarding COVID-19 treatment, the use of drugs was mainly based on institutional protocols. Remdesivir, hydroxychloroquine, and convalescent plasma were the most commonly used drugs.
Figure 2. Practices regarding COVID-19. The width of bars represents the proportion of respondents that marked each response. P: question in the practice section; HFNC: high-flow nasal cannula; NIV: noninvasive ventilation; IMV: invasive mechanical ventilation; ECMO: extracorporeal membrane oxygenation; and RCT: randomized controlled trial. *≤ 1%.
Comparing participants with a score in the knowledge section above the median with those with a score below the median, we found that those with higher scores more commonly worked in public institutions, had received institutional training on COVID-19, and used scientific publications, scientific society recommendations, and recommendations from other institutions as sources of information about COVID-19. However, the scores showed no associations with working in the ICU/ER or testing positive for COVID-19 (Table 3).
Table 3. Factors associated with a high level of knowledge about COVID-19.a .
| Factor | Level of knowledge | p | |
|---|---|---|---|
| Low | High | ||
| (n = 107) | (n = 144) | ||
| Age, years | 49 ± 13 | 48 ± 13 | 0.35 |
| Profession | 0.70 | ||
| Physician | 93 (87) | 120 (83) | |
| Respiratory therapist/ Physiotherapist | 9 (8) | 19 (13) | |
| Nurse | 2 (2) | 2 (2) | |
| Other | 3 (3) | 3 (2) | |
| Experience, years | 20 [14-32] | 20 [12-30] | 0.38 |
| Currently working in a hospital or clinic | 90 (86) | 134 (93) | 0.09 |
| Hospital type | 0.01 | ||
| Public | 45 (44) | 86 (60) | |
| Private | 35 (34) | 32 (22) | |
| University | 5 (5) | 15 (10) | |
| Mixed | 14 (14) | 8 (6) | |
| Philanthropic | 1 (1) | 1 (1) | |
| Other | 2 (2) | 2 (1) | |
| Direct care for COVID-19 patients | 89 (86) | 128 (90) | 0.46 |
| Working in the ICU | 28 (27) | 40 (27) | 0.95 |
| Working in the ER | 20 (19) | 33 (23) | 0.56 |
| Researcher | 10 (9) | 13 (9) | 1.00 |
| Academic supervisor | 21 (20) | 31 (22) | 0.83 |
| Chief of staff | 16 (15) | 16 (11) | 0.48 |
| Director | 4 (4) | 4 (3) | 0.73 |
| Previously tested positive for COVID-19 | 15 (14) | 24 (17) | 0.74 |
| institutional training on COVID-19 | 75 (71) | 119 (83) | 0.05 |
| Sources of information | |||
| Scientific publications | 84 (79) | 129 (90) | 0.03 |
| Scientific society recommendations | 82 (77) | 129 (90) | 0.01 |
| Official government websites | 81 (76) | 111 (77) | 0.92 |
| Recommendations from other institutions | 34 (32) | 66 (46) | 0.03 |
| Colleagues | 38 ((36) | 52 (36) | 1.00 |
| Media | 25 (23) | 37 (26) | 0.78 |
| Social media | 23 (22) | 36 (25) | 0.62 |
| Family and friends | 3 (3) | 4 (3) | 1.00 |
| Other | 4 (4) | 9 (6) | 0.56 |
Values expressed as n (%), mean ± SD, or median [IQR].
The characteristics of the participants’ institutions are presented in the supplementary material (Tables S2-S6) (208.5KB, pdf) . Regarding diagnostic imaging equipment, 20 (13%) and 34 (22%) of the respondents, respectively, reported that CT and ultrasound were unavailable in their institutions (Table S3). About one third of the participants reported that their institutions had insufficient numbers of physicians, nurses, or physiotherapists (Table S4). Regarding PPE availability, 53 participants (47%) reported that employees only sometimes had access to N95 respirators in their institutions, whereas 5 (3%) reported having no access to this PPE (Table S6).
DISCUSSION
In this cross-sectional study we assessed COVID-19 KAP among HCWs in 19 countries in Latin America. We found that more than one third of HCWs in our sample participated in some sort of institutional training on COVID-19 and that 43% had a low level of knowledge about COVID-19. The median attitude score was high, but 60% of the participants reported concerns about not providing adequate care to their patients. Most participants reported caring for COVID-19 patients on MV, the most commonly used ventilatory strategies being protective MV, alveolar recruitment maneuvers, and prone positioning, and the use of drugs to treat COVID-19 was mainly based on institutional protocols. We also found that COVID-19 knowledge was associated with the type of institution, availability of institutional training, and the type of sources of information.
This is a comprehensive Latin American study that addressed COVID-19 KAP among HCWs. KAP studies are important to provide valuable insights into how public health initiatives can protect health at the population level better. Because HCWs are more exposed to hazards of SARS-CoV-2 infection, it is important to understand their KAP to establish strategic behavioral interventions to prevent infections in this population. 25 - 27
Most participants reported having participated in institutional training on COVID-19, and that was associated with higher levels of knowledge. The COVID-19 pandemic had a significant impact on medical education all over the world, and webinars and online meetings have provided a great opportunity for teaching and learning during this period. 16 However, some HCWs reported feeling overwhelmed with the number and frequency of these events and had not attended all of these, reinforcing the importance of proposing effective training strategies, especially during the COVID-19 pandemic. 28
Despite high training participation, almost half of HCWs had low levels of knowledge about COVID-19. Although it is difficult to estimate how much knowledge is enough to achieve desirable changes in health outcomes, it is known that the type of information source might influence the level of knowledge and, potentially, the clinical practice. 26 , 29 Our finding that knowledge about COVID-19 treatment, transmission, complications, and protective MV was low might be explained by the lack of scientific knowledge during the first wave of the pandemic, especially in relation to complications and treatment. 18 , 26
HCWs had a high attitude score, believing that COVID-19 was very relevant. Previous studies have reported that the majority of HCWs have positive attitudes toward COVID-19, and that has been associated with age, gender, professional category, level of education, hospital type, and participation in online courses. 13 , 27 , 29 - 31
We also found that 60% of HCWs were concerned about not providing adequate care, and the main reasons were concerns about the lack of staff, lack of PPE, work overload, and ethical dilemmas. Latin America has one of the highest COVID-19 infection rates in the world, and several risk factors have been suggested, including the lack of human and institutional resources, 13 , 32 which may explain the concerns of HCWs. Furthermore, a considerable proportion of respondents reported lack of beds and/or of mechanical ventilators at the institutions they worked at.
Respondents also reported a lack of diagnostic imaging equipment. Restricted access to CT in low- and middle-income countries (LMICs) may be expected considering the high costs of the equipment. However, ultrasound is a portable and a relatively low-cost technology, but 22% of the respondents had no access to it. Previous studies have also reported a lack of access to ultrasound, and they suggested that this might reflect inequality in the supply and acquisition of medical equipment and in medical equipment training in LMICs, especially in rural areas. 33 , 34
The most commonly used ventilatory strategies for COVID-19 patients were protective MV, alveolar recruitment maneuvers, and prone positioning. This finding is in line with those of a scoping review that mapped MV strategies used in critically ill COVID-19 patients 35 ; the authors found that ventilator settings, especially tidal volume, plateau pressure, and driving pressure were relatively consistent across the studies and generally followed evidence-based recommendations for lung protective ventilation, and that prone positioning was widely used. 35
Regarding COVID-19 treatment, the respondents reported that the use of drugs was mainly based on institutional protocols. This might be explained by the fact that there were a very limited number of published randomized controlled trials on COVID-19 treatment published during the study period. The most commonly used drugs were remdesivir, hydroxychloroquine, and convalescent plasma. It is important to mention that, at the time the survey was distributed, there was no evidence of efficacy for these treatment strategies in COVID-19 patients.
We observed that the knowledge scores were higher among HCWs who worked at public institutions, those who had institutional training on COVID-19, and those who used scientific publications, scientific society recommendations, and recommendations from other institutions as sources of information. Other studies also reported a higher proportion of adequate knowledge among frontline HCWs working in public hospitals and those who received COVID-19 institutional training. 29 These findings emphasize the need for continuous medical training to guarantee access to evidence-based recommendations at all levels.
This study has several limitations. Knowledge was measured using a self-administered questionnaire and therefore may not reflect all aspects of medical knowledge about COVID-19. Our recruiting strategy was based on sending emails to ALAT members and invitations via social media, so the resulting sample may not be representative ofthe reality in all Latin American countries. In addition, because we used a snowballing strategy, it is possible that we had a sample clustering among well-trained staff, and we cannot estimate the response rate. The respondents of online surveys are most likely not representative of the whole universe of HCWs, since attitudes, risk perceptions, and knowledge may vary across countries and over time. Furthermore, self-reported behavior-related measures are subject to recall, response, and social desirability biases, and we lacked objective corroboration of real KAP among respondents. The majority of the participants in the survey were physicians, and other HCWs were not well represented. Since this was a cross-sectional study, we can only make assumptions for a single moment. Finally, our study design prevents us from making any assumptions about how the level of knowledge of the participants translated into patient outcomes. It is reasonable to expect that the level of knowledge varied throughout the COVID-19 pandemic, and it is important to consider that surges of cases during this first wave of the pandemic in the represented countries did not happen at the same time everywhere; there were peaks of COVID-19 cases in Argentina, Uruguay, and Paraguay after the survey period.
In conclusion, this multinational study involving several countries in Latin America showed that almost half of the HCWs surveyed had a low level of knowledge regarding COVID-19, and that was associated with the type of hospital that they worked at (public/private), their participation in institutional training, and their sources of information. HCWs considered that COVID-19 was very relevant, scoring high in the attitude section of the questionnaire, and more than half were concerned about not providing adequate care to patients. Our findings underscore the need for adequate institutional training on COVID-19, implementation of appropriate institutional measures to address frontline workers’ concerns about the disease, including the provision of necessary resources and PPE, and dissemination of trustworthy sources of information about COVID-19.
ACKNOWLEDGMENTS
The authors would like to thank the ALAT for supporting this project.
Footnotes
Financial support: This study received financial support from the Asociación Latinoamericana de Tórax (ALAT, Latin American Thoracic Association).
REFERENCES
- 1.Zhu N, Zhang D, Wang W, Li X, Yang B, Song J. Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi: 10.1056/NEJMoa2001017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Coronaviridae Study Group of the International Committee on Taxonomy of Viruses The species Severe acute respiratory syndrome-related coronavirus classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020;5(4):536–544. doi: 10.1038/s41564-020-0695-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rabi FA, Al Zoubi MS, Kasasbeh GA, Salameh DM, Al-Nasser AD. SARS-CoV-2 and Coronavirus. Disease. 2019:What–What. doi: 10.3390/pathogens9030231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.World Health Organization . Rational use of personal protective equipment for COVID-19 and considerations during severe shortages. Geneva: WHO; Interim guidance; c2021. https://www.who.int/publications/i/item/rational-use-of-personal-protective-equipment-for-coronavirus-disease-(covid-19)-and-considerations-during-severe-shortages [Google Scholar]
- 5.World Health Organization . WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020. Geneva: WHO; c2021. https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 [Google Scholar]
- 6.Johns Hopkins University & Medicine . Baltimore (MD): Johns Hopkins University & Medicine; c2021. https://coronavirus.jhu.edu [Google Scholar]
- 7.Asemahagn MA. Factors determining the knowledge and prevention practice of healthcare workers towards COVID-19 in Amhara region, Ethiopia a cross-sectional survey. Trop Med Health. 2020;48:72–72. doi: 10.1186/s41182-020-00254-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ahmed N, Shakoor M, Vohra F, Abduljabbar T, Mariam Q, Rehman MA. Knowledge, Awareness and Practice of Health care Professionals amid SARS-CoV-2, Corona Virus Disease Outbreak. Pak J Med Sci. 2020;36(COVID19-S4):S49–S56. doi: 10.12669/pjms.36.COVID19-S4.2704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi: 10.1056/NEJMoa2002032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [published correction appears in Lancet 2020. Jan 30;:]. Lancet. 2020;395(10223):497–506. doi: 10.1016/S0140-6736(20)30183-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China a retrospective cohort study [published correction appears in. Lancet. 2020;395(10229):1038–1038. doi: 10.1016/S0140-6736(20)30566-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Delgado D, Wyss Quintana F, Perez G, Sosa Liprandi A, Ponte-Negretti C, Mendoza I. Personal Safety during the COVID-19 Pandemic Realities and Perspectives of Healthcare Workers in Latin America. Int J Environ Res Public Health. 2020;17(8):2798–2798. doi: 10.3390/ijerph17082798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mendoza Millán DL, Carrión-Nessi FS, Mejía Bernard MD, Marcano-Rojas MV, Omaña Ávila ÓD, Doval Fernández JM. Knowledge, Attitudes, and Practices Regarding COVID-19 Among Healthcare Workers in Venezuela An Online Cross-Sectional Survey. Front Public Health. 2021;9:633723–633723. doi: 10.3389/fpubh.2021.633723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Al Demour S, Ababneh MA, Al-Taher RN, Alrabadi AF, Jaradat AF, Abushamma FA. Knowledge, Practice, and Attitude Toward COVID-19 Among Physicians in Jordan and Palestine Cross-Sectional Study. Int J Gen Med. 2021;14:77–87. doi: 10.2147/IJGM.S294221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rabbani U, Al Saigul AM. Knowledge, Attitude and Practices of Health Care Workers about Corona Virus Disease 2019 in Saudi Arabia. J Epidemiol Glob Health. 2021;11(1):60–68. doi: 10.2991/jegh.k.200819.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Noreen K, Rubab ZE, Umar M, Rehman R, Baig M, Baig F. Knowledge, attitudes, and practices against the growing threat of COVID-19 among medical students of Pakistan. PLoS One. 2020;15(12):e0243696. doi: 10.1371/journal.pone.0243696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zhang M, Zhou M, Tang F, Wang Y, Nie H, Zhang L. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J Hosp Infect. 2020;105(2):183–187. doi: 10.1016/j.jhin.2020.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bhagavathula AS, Aldhaleei WA, Rahmani J, Mahabadi MA, Bandari DK. Knowledge and Perceptions of COVID-19 Among Health Care Workers Cross-Sectional Study. JMIR Public Health Surveill. 2020;6(2):e19160. doi: 10.2196/19160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Centers for Disease Control and Prevention (CDC) Clinical Care Considerations. Atlanta, GA: CDC; https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/clinical-considerations-index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fhcp%2Fclinical-guidance-management-patients.html [Google Scholar]
- 20.Associação de Medicina Intensiva Brasileira (AMIB) Recomendações da Associação de Medicina Intensiva Brasileira para a abordagem do COVID-19 em medicina intensiva. São Paulo: AMIB; c2021. https://www.wficc.com/images/Recomendaco__es_AMIB-05.04.pdf [Google Scholar]
- 21.DeVellis RF. Scale Development: Theory and Applications. 4. Newbury Park(CA): Sage Publications; 2017. [Google Scholar]
- 22.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics. 2009;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap consortium Building an international community of software platform partners. Journal of Biomedical Informatics. 2019;95:1032083–undefined. doi: 10.1016/j.jbi.2019.103208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zhang M, Zhou M, Tang F, Wang Y, Nie H, Zhang L. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. Journal of Hospital Infection. 2020;105(2):183–187. doi: 10.1016/j.jhin.2020.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sarria-Guzmán Y, Fusaro C, Bernal JE, Mosso-González C, González-Jiménez FE, Serrano-Silva N. Knowledge, Attitude and Practices (KAP) towards COVID-19 pandemic in America A preliminary systematic review. Journal of Infection in Developing Countries. 2021;15(1):9–21. doi: 10.3855/jidc.14388. [DOI] [PubMed] [Google Scholar]
- 26.Gebremedhin T, Abebe H, Wondimu W, Gizaw AT. COVID-19 Prevention Practices and Associated Factors Among Frontline Community Health Workers in Jimma Zone, Southwest Ethiopia. Journal of Multidisciplinary Healthcare. 2021;14:2239–2247. doi: 10.2147/JMDH.S327293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Maurya VK, Upadhyay V, Dubey P, Shukla S, Chaturvedi A. Assessment of front-line healthcare workers' Knowledge, Attitude and Practice after several months of COVID-19 pandemic. Journal of Healthcare Quality Research. 2021;doi:https–https. doi: 10.1016/j.jhqr.2021.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cheikh Ismail L, Mohamad MN, Bataineh MF, Ajab A, Al-Marzouqi AM, Jarrar AH, et al. Impact of the Coronavirus Pandemic (COVID-19) Lockdown on Mental Health and Well-Being in the United Arab Emirates. Frontiers in Psychiatry. 2021:12–12. doi: 10.3389/fpsyt.2021.633230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tamang N, Rai P, Dhungana S, Sherchan B, Shah B, Pyakurel P, et al. COVID-19: a National Survey on perceived level of knowledge, attitude and practice among frontline healthcare Workers in Nepal. BMC Public Health. 2020;20(1) doi: 10.1186/s12889-020-10025-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Salman M, Ul Mustafa Z, Asif N, Zaidi HA, Shehzadi N, Khan TM. Knowledge, attitude and preventive practices related to COVID-19 among health professionals of Punjab province of Pakistan. Journal of Infection in Developing Countries. 2020;14(7):707–712. doi: 10.3855/jidc.12878. [DOI] [PubMed] [Google Scholar]
- 31.Tien TQ, Tuyet-Hanh TT, Linh TNQ, Hai Phuc H, van Nhu H. Knowledge, Attitudes, and Practices Regarding COVID-19 prevention among Vietnamese Healthcare Workers in 2020. Health Services Insights. 2021;14 doi: 10.1177/11786329211019225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Acosta LD. Response capacity to the COVID-19 pandemic in Latin America and the Caribbean. Revista Panamericana de Salud Publica/Pan American Journal of Public Health. 2020;44(1) doi: 10.26633/RPSP.2020.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Buonsenso D, De Rose C. Implementation of lung ultrasound in low- to middle-income countries a new challenge global health? Eur J Pediatr. 2022;181(1):1–8. doi: 10.1007/s00431-021-04179-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Stewart KA, Navarro SM, Kambala S, Tan G, Poondla R, Lederman S. Trends in Ultrasound Use in Low and Middle Income Countries A Systematic Review. Int J Matern Child Heal AIDS. 2020;9(1):103–120. doi: 10.21106/ijma.294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Grasselli G, Cattaneo E, Florio G, Ippolito M, Zanella A, Cortegiani A. Mechanical ventilation parameters in critically ill COVID-19 patients a scoping review. Crit Care. 2021;25(1):115–115. doi: 10.1186/s13054-021-03536-2. [DOI] [PMC free article] [PubMed] [Google Scholar]