

Abstract
The anterolateral thigh (ALT) flap has been extensively discussed in the literature as it allows for a wide variety and depth of tissues for complex wound coverage. Thanks to many cadaveric and angiographic studies of the subdermal plexus, it is to date ascertained that tailoring ALT thickness can be safely performed without compromising flap outcomes or causing additional morbidity. Recently, the authors applied and described a simpler, safer, and less time-consuming superthin ALT perforator (ALTP) free flap harvesting technique. The aim of this article is to show the versatility of the adipofascial flap harvested around the chosen perforators, which allowed us to safely expand the usage of ALTP superthin flaps.
Keywords: reconstructive surgical procedures, free tissue flaps, thigh, morbidity, microsurgery, perforator flap, neck, head, dermis, fascia
Since its introduction in 1984, 1 the anterolateral thigh (ALT) free flap has become the ideal, versatile soft tissue transfer to fulfill defects of various parts of the body. Its versatility allows for the harvest of a fasciocutaneous flap, myocutaneous flap with a portion of vastus lateralis, adipofascial flap, with vascularized nerve, innervated muscle, with tensor fascia lata, or as a sensate flap to provide all the necessary reconstructive tissue components. Nevertheless, particularly in western countries, one of the drawbacks of the ALT flap is represented by the excessive thickness of the subcutaneous tissue which, in overweight patients, may measure more than 5 cm. This makes ALT conventional flap not suitable for the reconstruction of districts, such as the dorsum of the foot/hand and head and neck areas which require a very thin and pliable coverage. Before the “superthin flap era,” flap debulking was usually performed either several months after primary surgery, often as a multiple stage procedure, or at the final stage of the harvest. However, it was not clear how much tissue was safe to remove and from where, due to the lack of knowledge of the rules of microcirculation. In 2014, Hong and colleagues described an innovative perforator flap harvesting technique based on a new plane of elevation, the superficial fascia. 2 3 Based on the cadaveric and angiographic studies of the subdermal plexus, 4 5 we thought, performed, and described a new ALT superthin flap harvesting procedure. As previously reported, 6 it consists of three surgical key-steps:
- Anteromedial subfascial approach;
- Dissection of a cylinder of adipofascial tissue, approximately 2 to 3 cm wide, centered on the chosen perforator/s with the aim of preserving the tiny collateral arteries contained in the suprafascial network and protect the vascular pedicle;
- Total deep fascia repair at the end of the procedure.
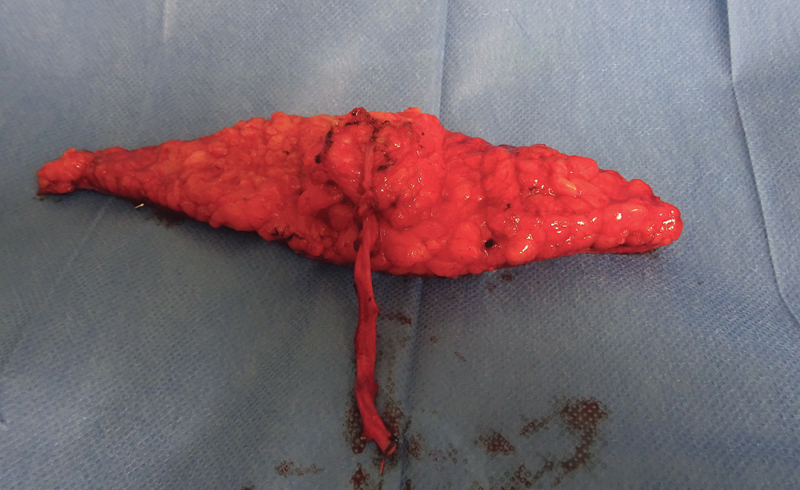
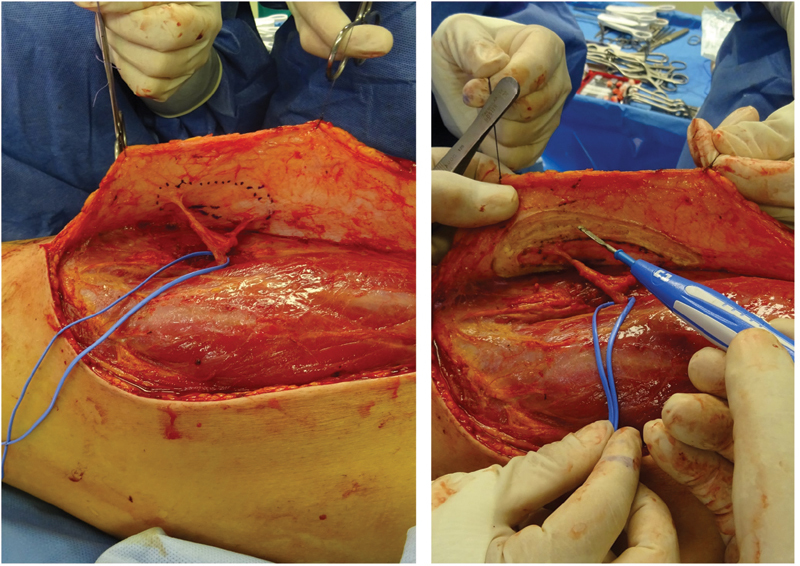
In our surgical practice, the described adipofascial flap harvested around the pedicle proved to be a versatile weapon in the hands of the surgeon. In fact, we were able to harvest it in various patterns: as a circular island flap in case of single perforator, as an oval island flap in case of single but branched perforator, and as double adipofascial flaps if two distant vessels vascularized ALT flaps ( Figs. 1 2 3 ). The described superthin harvesting procedure appeared to be safe in case of tubularized flaps as wells ( Video 1 ). This procedure is suggestable to safely decrease flap bulk and improve the contour and pliability necessary for appropriate function and aesthetics restoration of the treated areas. Consequently, it expands the scope of superthin flaps allowing for setting the donor site morbidity at zero.
Fig. 1.
In case of single perforator, a round adipofascial flap around the pedicle is harvested.
Fig. 2.

In case of two perforators feeding the superthin flap, two separated adipofascial cylinders centered on each perforator are harvested.
Fig. 3.
In case of single but branched perforator, an elliptical-shaped adipofascial flap around the pedicle is harvested.
Video 1 Tubularized anterolateral thigh (ALT) flap harvested with the described technique is showed, utilized for pharyngeal reconstruction.
Conflict of Interest Marco Innocenti is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Author contribution
Conceptualization: S Calabrese. M. Innocenti Data curation: S Calabrese Project administration: M Innocenti. Visualization: M Innocenti. Writing – original draft: S Calabrese. Writing – review & editing: S Calabrese , M Innocenti.
Patient Consent
Informed consent was obtained from all individual participants included in the study.
References
- 1.Song Y G, Chen G Z, Song Y L. The free thigh flap: a new free flap concept based on the septocutaneous artery. Br J Plast Surg. 1984;37(02):149–159. doi: 10.1016/0007-1226(84)90002-x. [DOI] [PubMed] [Google Scholar]
- 2.Hong J P, Choi D H, Suh H. A new plane of elevation: the superficial fascial plane for perforator flap elevation. J Reconstr Microsurg. 2014;30(07):491–496. doi: 10.1055/s-0034-1369807. [DOI] [PubMed] [Google Scholar]
- 3.Jeong H H, Hong J P, Suh H S. Thin elevation: a technique for achieving thin perforator flaps. Arch Plast Surg. 2018;45(04):304–313. doi: 10.5999/aps.2017.01529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nojima K, Brown S A, Acikel C. Defining vascular supply and territory of thinned perforator flaps: part I. anterolateral thigh perforator flap. Plast Reconstr Surg. 2005;116(01):182–193. doi: 10.1097/01.prs.0000170801.78135.00. [DOI] [PubMed] [Google Scholar]
- 5.Imanishi N, Nakajima H, Minabe T, Aiso S. Angiographic study of the subdermal plexus: a preliminary report. Scand J Plast Reconstr Surg Hand Surg. 2000;34(02):113–116. doi: 10.1080/02844310050159954. [DOI] [PubMed] [Google Scholar]
- 6.Innocenti M, Calabrese S, Tanini S, Malzone G, Innocenti A. A safer way to harvest a superthin perforator flap. Plast Reconstr Surg. 2021;147(03):466–469. doi: 10.1097/PRS.0000000000007676. [DOI] [PubMed] [Google Scholar]