

Abstract
Aims
The aims of the study were to identify factors affecting nurses' decision to undergo specialist education and choose a specialty and to describe differences between specialization areas with different types of care.
Design
A descriptive cross‐sectional design.
Methods
A survey was conducted among specialist nurse students in three nursing colleges in Sweden (n = 227). Instruments such as Big Five Inventory and RAND‐36 and items earlier used by Bexelius and Olsson were included. Survey data were analysed by using descriptive and analytical statistics, and for open‐ended question qualitative content analysis was used.
Results
Wage benefit during the education was regarded by 47% as an incentive to start studies. Most of the specialist nurse students considered an opportunity for new tasks (75%), new areas of responsibility (75%), intellectual challenges (72%) and higher wages (71%) to be of high importance when choosing a specialty. However, the students in specialization areas with transitory care‐rated challenges regarding the practical skills (84%) and the occurrence of acute events (82%) higher.
Conclusion
Although higher wages were important to make nurses feel that they will get value from the education, there were also other important aspects, such as opportunity for new tasks, new areas of responsibility and intellectual challenges that influenced nurses' willingness to undergo a specialist education. Our findings provide employers with the useful information to guide and influence nurses' decisions to enter specialist education and their choice of specialist area.
Keywords: career choice, decision‐making, education, nurse specialists, specialization
1. INTRODUCTION
Nearly 70% of countries worldwide report having continuous professional development programmes for nurses, and 50% have positions for advanced nurses available. Still, there is no consensus in definition of specialist nurses (SN), in the required educational level for admission to the SN education, in the length of education, in the degree of SNs nor in the number of specialization areas (Haryanto, 2019; Knap et al., 2020; Lowe, 2017; WHO, 2020). Furthermore, the demand for SNs has increased because of the greater need of advanced chronical disease management. Thus, the increasing shortage of SNs is affecting the quality of the health care worldwide (Haryanto, 2019; WHO, 2020). To meet the challenge of the shortage of SNs, it is necessary to get further knowledge of the nurses' reasons for choosing to specialize and to further understand reasons for choosing a certain specialty.
2. BACKGROUND
Although nearly 70% of countries worldwide report having continuous professional development programmes for nurses, the definition and educational background of specialist nurses is still somewhat unclear (Knap et al., 2020; Lowe, 2017; WHO, 2020). The SN is seen as an umbrella term by the European Society of Specialist Nurses (ESNO) containing other terms such as advanced nurse practitioner (ANP) or nurse practitioner (NP; Knap et al., 2020). At the same time, ANP and NP are more often seen as a link between a nursing domain and a medical domain with advanced nursing skills, higher education and expanded scopes of practice (Lowe, 2017). Also in Sweden, ANP programmes include two‐year master's degrees and are therefore placed at a higher level compared to specialist nurses with one‐year master's degrees (Swedish Higher Education Ordinance, 1993:100, Annex 2).
When comparing SN education in different countries, there is limited information due to of lack of coordination of regulations (WHO, 2020). A variation is also seen in the number of specialization areas and on the educational level worldwide. The same specialization area of the nursing field can in different countries, or even within one country, have different academic levels as a requirement for admission to the education. The duration of the education in different countries in the same specialization area of the nursing field can vary from a few days to two years. And more, there is no agreement about the role or level of independence when practising as SN (Dury et al., 2014; Ranchal et al., 2015; WHO, 2020). In Europe, there are today 24 different specialization areas available for SN education (Dury et al., 2014). This variation in conditions for SN education makes it difficult to compare different countries. Probably, therefore, there is a gap in the knowledge of factors affecting nurses' decisions to undergo a specialist education.
In Sweden, SN education is at a postgraduate level, that is education for Registered Nurses with a bachelor's degree in nursing. The education is regulated by the Swedish higher education ordinance, gives a professional degree at an advanced level and is eligible for central study grants. The duration of a full‐time SN education is 1–1.5 years (60–75 credits). Since 2007, there are 11 defined specialization areas available: ambulatory care, anaesthesia, public health care, intensive care, medical nursing, surgical nursing, oncology, operating room nursing, psychiatric care, elderly care and paediatric nursing. Since 2013, there is also an open specialization area which nursing colleges can decide themselves, dependent on the need of the community and what would expand the selection of specialization areas even more (Swedish Higher Education Ordinance, 1993:100, appendix 2; Governmental inquiry, 2018). In Sweden, as a midwife, the nurses are given a new licence and have an independent professional title while SNs keep their licence as nurses. Therefore, in Sweden, midwives are not regarded as SNs (Governmental inquiry, 2018).
Among all the Registered Nurses in Sweden, 45% are SNs. The number of SNs in Sweden has decreased during the last decades from 55,000–48,000 (The National Board of Health and Welfare, 2016). Some specialization areas, as ambulatory care, have shown a strong increase, while other specialization areas like medical and surgical nursing have shown a strong decrease. Despite the reduction in the number of employed SNs, more SNs are educated now than ever before. Yearly, roughly 2,300 students start a specialist education in Sweden. It is an increase with about 700 students since 2001. At the same time, almost half of the employed SNs are 55 years or older and will retire during the coming decade (The National Board of Health and Welfare, 2016). Furthermore, 1 of 10 nurses no longer work in health care, pointing out working and environmental conditions as the reason for their decision (Governmental inquiry, 2018). In the last years, employers can take advantage of targeted national government initiatives to offer part‐time or full‐time wage benefits during studies. In many cases, nurses commit themselves to work for an employer for a certain period if they receive a wage benefit. This has been done mostly in specialization areas such as anaesthesia, intensive care and operating room nursing. Still, the number of specialist nurses in those areas has not increased considerably (Governmental inquiry, 2018). As a result, the shortage of specialist nurses in Sweden is an acute and growing problem.
The association between shortage of nurses, educational level of nurses and increase in patients' mortality rate are global issues, since most of the regions in the world report shortages of nurses (Scheffler & Arnold, 2019; WHO, 2020). Previous studies have shown that an increase in a nurse's workload by one extra patient increased the mortality rate by 7%, whereas an increase in the educational level decreased the mortality rate by 7% (Aiken et al., 2014). When the proportion of nurses is higher, less adverse care outcomes as pressure ulcers or falls with injury occur and the patients give higher ratings of care satisfaction to the units. Also, nurses are more satisfied with their work, show a lower number of burnouts and are less commonly reporting poor safety culture in the units (Aiken et al., 2017). Audet et al. (2018) showed in their review article which evaluated the association between nurses' educational level and patient mortality or occurrence of adverse events that most often no separation was made between Registered Nurses with a bachelor's degree and nurses with a higher level of nursing education when analysing the data (Audet et al., 2018). Therefore, no conclusion can be drawn if a higher level of nursing education decreases mortality and the occurrence of adverse events. However, it has been shown that care given by experienced Registered Nurse anaesthetists and anaesthesiologists is associated with both lower occurrence of adverse events and patient mortality compared with being cared for by inexperienced nurses (Saager et al., 2021). Since the level of experience and a higher proportion of Registered Nurses with a bachelor's degree makes a difference, probably also a higher number of SNs is of importance for the quality of the health care.
There is a lack of consensus in the definition of SNs, in the required educational level for admission to the SN education, in the length of education, in the degree of SNs and in the number of specialization areas. This unclarity leads to many prerequisites, motivating factors and obstacles to further education, which nurses need to balance to make a choice to specialize. Therefore, there is a need to clarify what influences the nurses' willingness to specialize and to investigate if there are any differences between the specialization areas with different types of care.
2.1. Research question
The aims of this study were to identify factors affecting nurses' decision to undergo specialist education and to choose a specialty and to describe differences between specialization areas with different types of care.
3. THE STUDY
3.1. Design
The study had a descriptive cross‐sectional design where a structured web‐based survey with one open‐ended question was used. The analysis included descriptive and analytical statistics for the structured survey and qualitative content analysis for the open‐ended question. The open‐ended questions about SN students' reason for starting a specialist education were added to the structured survey to reassure that relevant information was not missed. The result from the open‐ended question is presented according to the recommendations from O'Cathain and Thomas (2004).
3.2. Method
3.2.1. Data collection
All first‐year SN students on postgraduation SN education programmes in three nursing colleges in Sweden were invited to answer a web‐based survey during January to April 2021. The selection of schools was based on the principle of convenience where all three nursing colleges were in an urban area with access to all eleven defined specialization areas. An open link to the study was posted on the SN students' learning platform or sent to them via email by a contact person at the nursing colleges. Due to the open link to the survey, all data collection was anonymous. All SN students received one request to take part in the survey and two reminders. All eleven defined specialization areas with four additional open areas were represented in the study (Table 1). The number of SN students in each specialist education specialization area ranged from 13–96 individuals, with a total number of 584 students to be included in this study.
TABLE 1.
Groups of different specialization areas and the response rate within the specialization areas
| Transitory care | N (%) | Long‐term care | N (%) |
|---|---|---|---|
| Ambulatory care | 27 (40) | Palliative care nursing | 34 (64) |
| Operating room nursing | 10 (50) | Public health care | 33 (34) |
| Emergency care nursing | 9 (24) | Psychiatric care | 24 (36) |
| Anaesthesia | 8 (38) | Paediatric nursing | 21 (37) |
| Intensive care | 8 (35) | Oncology | 15 (41) |
| Medical nursing | 10 (44) | ||
| Cardiac care nursing | 10 (27) | ||
| Cognitive illness nursing | 8 (62) | ||
| Surgical nursing | 4 (29) | ||
| Elderly care | 4 (21) |
The inclusion criterion was being a first‐year SN students on post‐graduation SN education programmes in one of the three selected nursing colleges in Sweden.
The exclusion criterion was being a student midwife. As midwives are not considered as SNs in Sweden, we did not include midwives in this study.
3.2.2. Response rate
We received 232 answers of the total of 584 SN students, which gave a response rate of 40%. One person failed to provide the correct information confirming their eligibility for the study and was therefore excluded from the study. Four persons were excluded because they declined participation, resulting in 227 answers to analyse. The response rate within all fifteen different specialization areas varied from 21%–64% (Table 1).
3.2.3. Survey instruments
The survey was divided into three parts: survey instrument items earlier used by Bexelius et al. (2016) and Olsson et al. (2019), the Big Five Inventory (BFI; John & Srivastava, 1999), and Measure of Health‐Related Quality of Life (RAND‐36; Hays et al., 1993).
The survey instrument items earlier used by Bexelius et al. (2016) and Olsson et al. (2019) were modified to fit SN students and the aims of this study and can be viewed in Appendix S1. Bexelius et al. (2016) and Olsson et al. (2019) survey was focused on physicians' education; therefore, we needed to adapt the content of the questions to fit the nurse's education instead. For part A.1, no major modifications were needed. For parts A.2 and A.3, major modification was needed because of differences between physicians and nurses' education. Still, the themes of the questions were the same as in items earlier used by Bexelius et al. (2016) and Olsson et al. (2019). In part A.4, more statements about important factors when choosing a particular specialty of nurse education were added to the original items from Bexelius et al. (2016) and Olsson et al. (2019). There were also survey items in Bexelius et al. (2016) and Olsson et al. (2019) which did not answer to our aim and were therefore not used.
Ten nursing students from the postgraduation specialist education programme tested the face validity for the survey and additional changes were made in accordance with their comments. The survey instrument covered areas such as general background, background as a nurse, more specific questions about their choice to start specialization education and choose a specialization (Appendix S1). Multiple‐choice questions were the most common question type. Five‐point Likert scale was used in two questions. There was also one open question about the SN students' reasons for applying for the specialist education.
BFI is a general taxonomy of personality traits covering five personality dimensions: extraversion (social and active), agreeableness (cooperative, trustful), conscientiousness (responsible, orderly), neuroticism (anxious) and openness to experience (curious, imaginative). Each dimension summarizes many personality traits and represents the personality at the broadest level of abstraction (John & Srivastava, 1999). The BFI has been validated in a Swedish context by Zakrisson (2010). BFI contains 44 statements with a five‐point Likert scale.
RAND‐36 is a health‐related quality of life survey instrument with 36 multiple‐choice questions divided into ten areas: physical functioning, physical role functioning, pain (bodily pain), general health, energy/fatigue, social functioning, emotional role functioning, emotional well‐being (mental health) and health transition score (Hays et al., 1993). The RAND‐36 has been validated in a Swedish context (Orwelius et al., 2017).
3.3. Analysis
3.3.1. Groups for analysis
For the analysis, two groups of different specialist education specialization areas were created (Table 1). The first group is characterized by a transitory patient care in connection with hospitals. For this group, a specific competence or longer working experience has been necessary and has normally been required by the employer. In these areas, therefore, SNs cannot normally be replaced by Registered Nurses. A more long‐term patient care characterizes the second group with the possibility of working outside of the hospital settings. Here, the specific competence has not been seen as traditionally mandatory and therefore specialist education is not normally demanded. In these areas, therefore, SNs can normally be replaced by Registered Nurses.
3.3.2. Data analysis
We used the Statistical Package for the Social Sciences (SPSS Inc.) version 25 for statistical analyses. For continuous variables, we used independent‐samples t test, two‐tailed, and for categorical variables, chi‐square test. For all tests, a significance level of p < .05 was set.
The modified survey instrument items earlier used by Bexelius et al. (2016) and Olsson et al. (2019) included two questions with Likert scale. Likert scale in questions on perceived status of 11 defined specialization areas had the answering options: (1) very low, (2) quite low, (3) moderate, (4) quite high, (5) very high. We coded answers 1–3 as low status and answers 4–5 as high status. Likert scale in questions on important factors for choosing a specialty specialization area had answering options: (1) not important at all, (2) little important, (3) moderately important, (4) quite important, (5) very important. Answers 1–3 were coded as low importance, answers 4–5 were coded as high importance. Thereafter, we analysed both status and important factors as categorical variables.
The instrument BFI had Likert scale with the options: (1) strongly disagree, (2) disagree, (3) neither agree nor disagree, (4) agree, (5) agree strongly. The answers were coded, calculated and analysed according to instructions given by Zakrisson (2010).
The Swedish version of RAND‐36 was ordered from the Registercentrum Sydost website. They also provided a calculation algorithm for SPSS which was used in the current study.
For the open‐ended question, simplified qualitative content analysis inspired by Lindgren et al. (2020) was used. Firstly, meaning units were identified, followed by condensing and coding. Thereafter the codes were sorted, and categories were created. The categories are presented in the results.
Because of multiple significance tests, the Bonferroni correction method was used to control type I error (Bland & Altman, 1995). In the current study, to a maintain significance level of p < .05, we needed p < .003 according to the Bonferroni correction.
Two participants had not reported their area of specialization, and therefore two responses were missing in the group comparison analyses. No other data were missing.
4. RESULTS
Of the total of 227 responding students, the majority (90%) were female. The mean age was 37.8 (SD 8.9) years, and they had been working for 9.0 (SD 7.2) years as a nurse. The significant difference between students in the transitory care or in the long‐term care specialization areas was seen in gender (p < .001), if they were studying full time (p < .001), and if another considered specialist education was within the same specialist group (p < .003). The basic demographic characteristics of the participants with significant differences between students in the transitory care or in the long‐term care specialization areas are presented in Table 2.
TABLE 2.
Basic characteristics of the participants
| Total | Transitory care | Long‐term care | p‐value | ||||
|---|---|---|---|---|---|---|---|
| N (%) | Mean (SD) | N (%) | Mean a (SD) | N (%) | Mean (SD) | ||
| Total | 227 (100) | — | 62 (27.3) | — | 163 (71.8) | ||
| Age | — | 37.8 (8.9) | — | 35.2 (7.3) | — | 38.6 (9.3) | .004 c |
| Years as a nurse | — | 9.0 (7.2) | — | 7.0 (5.2) | — | 9.7 (7.7) | .005 c |
| Female (ref: male) | 204 (89.9) | — | 47 (75.8) | — | 155 (95.1) | — | <.001 d |
| Sweden as country of origin (ref: no) a | 187 (82.4) | — | 52 (83.9) | — | 133 (81.6) | — | .690 d |
| Family member in care profession (ref: no) | 144 (63.4) | — | 38 (61.3) | — | 106 (65.0) | — | .602 d |
| Nurse b (ref: no) | 85 (37.5) | — | 21 (33.9) | — | 64 (39.3) | — | .456 d |
| Other b (ref: no) | 91 (40.1) | — | 24 (38.7) | — | 67 (41.1) | — | .744 d |
| Previous higher education (ref: no) | 26 (11.5) | — | 4 (6.5) | — | 22 (13.5) | — | .140 d |
| Previous not finished SN education (ref: no) | 24 (10.6) | — | 5 (8.1) | — | 17 (10.4) | — | .594 d |
| Previous SN education (ref: no) | 25 (11.0) | — | 5 (8.1) | — | 19 (11.7) | — | .435 d |
| Previous work in specialist area (ref: no) | 140 (61.7) | — | 30 (48.4) | — | 110 (67.5) | — | .008 d |
| Full‐time study pace (ref: no) | 37 (16.3) | — | 29 (46.8) | — | 12 (7.4) | — | <.001 d |
| Study funding with work, full or part‐time (ref: student wages or other) | 91 (40.1) | — | 29 (46.8) | — | 60 (36.8) | — | .172 d |
| Did possibility of partly paid studies made you start your studies (ref: no)? | 107 (47.1) | — | 27 (43.5) | — | 80 (49.1) | — | .458 d |
| Considered another specialist education (ref: no) | 93 (41.0) | — | 34 (54.8) | — | 57 (35.0) | — | .007 d |
| Within the specialist group (ref: outside the specialist group or mixed) | 46 (50.5) | — | 24 70.6) | — | 22 (38.6) | — | .003 |
| Returns to previous workplace (ref: no) | 158 (69.6) | — | 36 (58.1) | — | 122 (74.8) | — | .014 d |
| New work tasks (ref: no) | 189 (83.3) | — | 53 (85.5) | — | 135 (82.8) | — | .630 d |
Country of origin is considered as Sweden if they were born in Sweden, regardless of if any other family member originated from another country.
The presence of specific caring profession in the family is calculated, more than one may occur per family.
T‐test, significance level of p < .05 (Bonferroni correction for significance p < .003 marked in bold).
Chi‐square test, significance level of p < .05 (Bonferroni correction for significance p < .003 marked in bold).
4.1. Important factors when choosing to specialize
SN students were asked in one open‐ended question about their reason for starting a specialist education. There was a total of 460 statements which were divided in to five categories such as influence given by an employer, wish to make a change in a work‐related circumstance, expand a formal competence, achieve personal development and follow an emotional factor. For each category, there is a description, followed by quotes by the respondents to verify the results.
4.1.1. Achieve personal development
In 154 (33%) statements wished SN students for personal growth and to learn more. They did not wish to stand still on the same level of mindset, but wished for additional responsibilities and challenges, or for a career change.
“I want to learn more, be challenged and get new opportunities” [female student, 43 years]
“Because I want to get better at what I do, for the sake of the patients and for myself. I enjoy learning and developing in my field” [female student, 46 years]
“To develop in my profession and not get stuck in the same mindset of a workplace” [female student, 35 years]
4.1.2. Expand a formal competence
In total of 128 (28%) statements described SN students the need to deepen their knowledge in the areas they were working in or wanted to work in. They also wanted to improve their nursing skills and develop within the profession. Some had a goal to continue their education even further to be able to conduct research in the future.
“I want to improve my skills and develop within the profession and gain more responsibility and knowledge in an area I am interested in” [male student, 34 years]
“Because I want to become a specialist in palliative care and do a PhD/research in that area and advance knowledge and teach others about palliative care because it is such an incredibly valuable form of care” [female student, 34 years]
4.1.3. Wish to make a change in a work‐related circumstance
In 98 (21%) of the statements SN students explained that they wished to raise their wages and to be able to get more freedom to choose a workplace. They considered education as a foundation for making them more attractive on the labour market. The goal was to compete for the more attractive jobs with more attractive working conditions, and to do something new.
“Specializing will give me more opportunities in the future in terms of wages, working hours, and workplace” [female student, 33 years]
“Better conditions, working hours and wages” [female student, 34 years]
“Felt like I needed to move on and do something new” [female student, 35 years]
4.1.4. Follow an emotional factor
In 58 (13%) of statements had SN students a desire to work within a particular specialization area because of their personal interest, curiosity or passion.
“It was my dream” [female student, 37 years]
“Out of curiosity and restlessness” [male student, 45 years]
“Because I had a deep interest” [female student, 29 years]
4.1.5. Influence given by an employer
In 22 (5%) of the statements the SN students expressed that there was a requirement for specialist education to achieve the desired position, hey were encouraged to study or were offered a wage benefit during the education.
“Requirements for advancement in the competence ladder” [female student, 49 years]
“My employer suggested it” [female student, 33 years]
“Region Östergötland lets me study with a wage” [female student, 37 years]
4.2. Choosing a specialization area of the specialist education
When choosing a specialization area of the specialist education, 41% had considered starting with another specialist education than the one they had started now. Students in transitory care specialization areas were more commonly (p = .003) considering another specialist specialization area within the same group (Table 2). Considered alternative specialist educations are presented in Figure 1.
FIGURE 1.
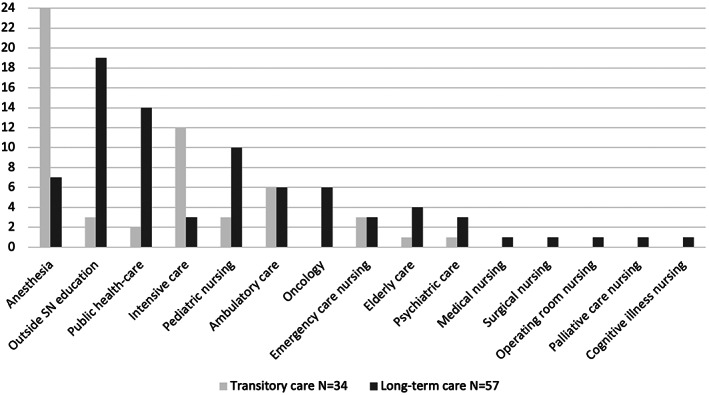
Considered alternative specialist educations before the choice of current specialist education, compared groups
4.2.1. Important factors when choosing a specialty
Over 70% of all the students regarded the opportunity for new tasks, opportunities for new areas of responsibility, intellectual challenge and higher wages as the most important factors when choosing a specialty. The students in the transitory care specialization areas regarded the challenge regarding the practical skills (p < .001), the possibility to take care of one patient at time (p < .001), and the occurrence of acute events (p < .001) to be of high importance when choosing a specialty. For the students belonging to the long‐term care specialization areas, factors like the opportunity for research (p < .001), and the opportunity to have the care of the same patients for a longer time (p < .001) were more important. The important factors when choosing a specialty are presented in Table 3.
TABLE 3.
Important factors when choosing a specialty
| Total N = 227 | Transitory care N = 62 | Long‐term care N = 163 | p‐value a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| High N (%) | Low N (%) | Nr. | High N (%) | Low N (%) | Nr. | High N (%) | Low N (%) | Nr. | ||
| Opportunity for new tasks | 171 (75.3) | 56 (24.7) | 1 | 48 (77.4) | 14 (22.6) | 3 | 122 (74.8) | 41 (25.2) | 1 | .732 |
| Opportunities for new areas of responsibility | 170 (74.9) | 57 (25.1) | 2 | 48 (77.4) | 14 (22.6) | 3 | 121 (74.2) | 42 (25.8) | 2 | .731 |
| Intellectually challenging specialty | 164 (72.2) | 63 (27.8) | 3 | 48 (77.4) | 14 (22.6) | 3 | 115 (70.6) | 48 (29.4) | 3 | .322 |
| Higher wages | 162 (71.4) | 65 (28.6) | 4 | 47 (75.8) | 15 (24.2) | 4 | 113 (69.3) | 50 (30.7) | 4 | .411 |
| The relationship with the patient | 131 (57.7) | 96 (42.3) | 5 | 28 (45.2) | 34 (54.8) | 9 | 103 (63.2) | 60 (36.8) | 5 | .016 |
| To combine work with family life | 129 (56.8) | 98 (43.2) | 6 | 28 (45.2) | 34 (54.8) | 9 | 100 (61.3) | 63 (38.7) | 6 | .035 |
| Specialty with good labour market | 126 (55.5) | 101 (44.5) | 7 | 38 (61.3) | 24 38.7) | 6 | 87 (53.4) | 76 (46.6) | 8 | .298 |
| The type of patient contact | 125 (55.1) | 102 (44.9) | 8 | 29 (46.8) | 33 (53.2) | 8 | 95 (58.3) | 68 (41.7) | 7 | .135 |
| Challenge regarding practical skills | 124 (54.6) | 103 (45.4) | 9 | 52 (83.9) | 10 (16.1) | 1 | 71 (43.6) | 92 (56.4) | 11 | <.001 |
| Economically beneficial specialty | 116 (51.1) | 111 (48.9) | 10 | 34 (54.8) | 28 (45.2) | 7 | 80 (49.1) | 83 (50.9) | 10 | .459 |
| Opportunity to adapt working hours to family | 109 (48.0) | 118 (52.0) | 11 | 25 (40.3) | 37 (59.7) | 10 | 83 (50.9) | 80 (49.1) | 9 | .180 |
| Possibility to take care of 1 patient at a time | 101 (44.5) | 126 (55.5) | 12 | 40 (64.5) | 22 (35.5) | 5 | 60 (36.8) | 103 (63.2) | 13 | <.001 |
| Occurrence of acute events | 99 (43.6) | 128 (56.4) | 13 | 51 (82.3) | 11 (17.7) | 2 | 47 (28.8) | 116 (71.2) | 16 | <.001 |
| To get away from a bad work environment | 82 (36.1) | 145 (63.9) | 14 | 23 (37.1) | 39 (62.9) | 11 | 57 (35.0) | 106 (65.0) | 14 | .876 |
| Opportunity for research | 73 (32.2) | 154 (67.8) | 15 | 8 (12.9) | 54 (87.1) | 15 | 63 (38.7) | 100 (61.3) | 12 | <.001 |
| Opportunity to have the same patients for a long time | 61 (26.9) | 166 (73.1) | 16 | 5 (8.1) | 57 (91.6) | 16 | 56 (34.4) | 107 (65.6) | 15 | <.001 |
| To reduce stress compared to current workplace | 61 (26.9) | 166 (73.1) | 16 | 18 (29.0) | 44 (71.0) | 12 | 41 (25.2) | 122 (74.8) | 17 | .612 |
| Opportunity to work in different places in Sweden | 60 (26.4) | 167 (73.6) | 17 | 25 (40.3) | 37 (59.7) | 10 | 34 (20.9) | 129 (79.1) | 18 | .004 |
| For the sake of your health | 44 (19.4) | 183 (80.6) | 18 | 11 (17.7) | 51 (82.3) | 13 | 32 (19.6) | 131 (80.4) | 19 | .851 |
| Opportunity to work abroad | 29 (12.8) | 198 (87.2) | 19 | 9 (14.5) | 53 (85.5) | 14 | 20 (12.3) | 143 (87.7) | 20 | .660 |
Chi‐squared test, significance level of p < .05 (Bonferroni correction for significance p < .003 marked in bold).
4.2.2. Status of 11 defined specialization areas
No significant differences were seen in the status rating of specialist education specialization areas (Table 4).
TABLE 4.
Status of 11 defined specialization areas
| Total N = 227 | Transitory care N = 62 | Long‐term care N = 163 | p‐value a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| High N (%) | Low N (%) | Nr. | High N (%) | Low N (%) | Nr. | High N (%) | Low N (%) | Nr. | ||
| Intensive care | 216 (95.2) | 11 (4.8) | 1 | 59 (95.2) | 3 (4.8) | 1 | 155 (95.1) | 8 (4.9) | 1 | 1.0 |
| Anaesthesia | 211 (93.0) | 16 (7.0) | 2 | 59 (95.2) | 3 (4.8) | 1 | 150 (92.0) | 13 (8) | 2 | .310 |
| Ambulatory care | 163 (71.8) | 64 (28.2) | 3 | 37 (59.7) | 25 (40.3) | 2 | 125 (76,7) | 38 (23.3) | 3 | .013 |
| Operating room nursing | 145 (63.9) | 82 (36.1) | 4 | 36 (58.1) | 26 (41.9) | 3 | 108 (66.3) | 55 (33.7) | 4 | .278 |
| Public health care | 116 (51.1) | 111 (48.9) | 5 | 30 (48.4) | 32 (51.6) | 4 | 84 (51.5) | 79 (48.5) | 5 | .766 |
| Oncology | 86 (37.9) | 141 (62.1) | 6 | 20 (32.3) | 42 (67.7) | 6 | 66 (40.5) | 97 (59.5) | 6 | .285 |
| Surgical nursing | 83 (36.6) | 144 (63.4) | 7 | 20 (32.3) | 42 (67.7) | 6 | 63 (38.7) | 100 (61.3) | 7 | .440 |
| Paediatric nursing | 78 (34.4) | 149 (65.6) | 8 | 22 (35.5) | 40 (64.5) | 5 | 56 (34.4) | 107 (65.6) | 8 | .877 |
| Medical nursing | 64 (28.2) | 163 (71.8) | 9 | 16 (25.8) | 46 (74.2) | 8 | 48 (29.4) | 115 (70.6) | 9 | .624 |
| Psychiatric care | 54 (23.8) | 173 (76.2) | 10 | 19 (30.6) | 43 (69.4) | 7 | 35 (21.5) | 128 (78.5) | 10 | .164 |
| Elderly care | 42 (18.5) | 185 (81.5) | 11 | 12 (19.4) | 50 (80.6) | 9 | 30 (18.4) | 133 (81.6) | 11 | 1.0 |
Chi‐squared test, significance level of p < .05 (Bonferroni correction for significance p < .003).
4.2.3. The health‐related quality of life and personality traits
The health‐related quality of life measured with RAND‐36 and personality traits measured with BFI did not show any significant difference between the groups (Table 5).
TABLE 5.
RAND‐36 and BFI
| Total N = 227 | Transitory care N = 62 | Long‐term care N = 163 | p‐value a | |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| RAND‐36 | ||||
| Physical Functioning (PF) | 96.0 (8.4) | 97.7 (4.5) | 95.6 (9.1) | .093 |
| Role functioning/Physical (RP) | 88.1 (27.2) | 91.9 (22.1) | 87.1 (28.1) | .226 |
| Pain (Bodily Pain) (BP) | 83.7 (19.2) | 83.5 (18.3) | 84.1 (19.3) | .829 |
| General Health (GH) | 75.7 (17.9) | 78.3 (16.9) | 75.0 (17.9) | .209 |
| Energy/fatigue (Vitality) (VT) | 59.9 (19.6) | 60.7 (20.5) | 59.5 (19.3) | .678 |
| Social Functioning (SF) | 84.6 (20.0) | 86.3 (18.9) | 84.1 (20.2) | .466 |
| Role functioning/Emotional (RE) | 81.2 (30.2) | 81.2 (32.8) | 81.2 (28.7) | .926 |
| Emotional well‐being (Mental Health) (MH) | 75.5 (15.0) | 74.7 (17.2) | 75.8 (14.1) | .639 |
| Health Transition score (HT) | 56.6 (22.3) | 59.7 (24.1) | 55.5 (21.7) | .215 |
| BFI | ||||
| Extraversion | 28.2 (5.4) | 28.6 (5.1) | 28.1 (5.5) | .581 |
| Agreeableness | 38.8 (3.6) | 38.8 (3.9) | 38.9 (3.4) | .789 |
| Conscientiousness | 37.6 (4.3) | 37.5 (4.8) | 37.6 (4.2) | .869 |
| Neuroticism | 18.1 (5.1) | 17.6 (5.2) | 18.3 (5.1) | .320 |
| Openness to experience | 34.5 (6.1) | 34.1 (5.6) | 34.7 (6.3) | .534 |
T‐test, significance level of p < .05.
5. DISCUSSION
Morgenthaler (2009) described, similar to our results, that the nurses need to receive a value of the education such as new professional opportunities and higher wages to consider starting a specialist education, otherwise they might not feel that going to school for one more year is worth it. Most SN students in our study considered the opportunity for new tasks and additional responsibilities, intellectual challenges and higher wages to be the most important factors influencing their decision to pursue a specialist education. In both our and in Morgenthaler (2009) study, SN students were highly interested in additional responsibilities, while for nurse students and nurses in McCabe et al. (2005) this was not as important. In McCabe et al. (2005) showed instead that among nursing students and nurses intellectually challenging work was one of the most important factors when choosing a career. However, we observed a difference between the students in different specialization area types. SN students in specialization areas with transitory care rated challenges in practical skills and the occurrence of acute events as most important factors having affected their decision. According to McCabe et al. (2005) these preferences are related to the lower age among their students. We cannot in our study draw any age‐related conclusions as the significance level for age differences was just above the threshold.
Consistent with our findings, Cooley (2008) described nurses' reasons for studying to be expectation of receiving a personal development, expanding a formal competence, and getting access to one specific specialist specialization area. Harrison et al. (2014) showed similar results in their study that personal interest and experiences, challenges and stimulation, encouragement by others, workplace conditions and perceived benefits were important for decision‐making.
One of the key priorities for the SN students in our study was higher wages after finishing the education. This has also previously been seen for nursing students (Rognstad et al., 2004). However, both Rognstad and Aasland (2007) and McCabe et al. (2005) have established that this was not a priority when they started working as a nurse. Rognstad and Aasland (2007) showed that the appreciation of higher wages among nurses developed after some years of working.
Many of SN students' reasons for choosing to specialize that we saw in our study can also be found in Zhu et al.'s (2021) description of career plateau that have led to resignment. Zhu et al. (2021) included low possibility for additional responsibilities, for acquiring new skills and for promotion in their prescription of career plateau. Nurses did not feel getting value of working, were not motivated for learning, had no challenges or development possibilities, felt a lack of support from the organization, were dissatisfied with wages and had poor working conditions. All those factors were reasons for resigning and finding a new organization which could meet their requirements (Zhu et al., 2021).
The financial support during the studies given by the employer was an important motivating factor for 47% of the SN students in our study when deciding to start a specialist education. Morgenthaler (2009) saw financial concerns as a potential obstacle to pursuing an additional education. SN students often needed to consider the financial commitments to their families when deciding whether they can afford to study (Morgenthaler, 2009). In Sweden, it is possible to get a student aid comprising loans at low interest rate and grants by The Swedish Board of Student Finance. However, there are limitations of time and amount regarding the student loans (CSN, 2021). Therefore, some SN students in Sweden must face a specialist education without the possibility of financial support. In Sweden, average wages for SNs compared with Registered Nurses is less than 10% higher, and the difference between lowest and highest wages among SN is approximately 30% (Vårdförbundet, 2016). Therefore, SN education based on student aid or personal loan might not be economically beneficial, and wage benefits during the education are needed to attract the students.
There was a significantly higher number of male students in specialization areas with transitory care. Our findings are supported by Swedish statistics, where a higher number of male nurses are present in specialization areas as ambulatory care, anaesthesia and intensive care (The Swedish Occupational Register with statistics, 2017). Also, according to the study by Stanley et al. (2016) a higher number of men are working in areas like critical care and emergency care whereas they are underrepresented in specialization areas like elderly care or surgical nursing. Abrahamsen (2004) argues that male nurses more often transfer to areas with higher wages. This argument is only partly supported by Swedish statistics (Vårdförbundet, 2016) where anaesthesia and intensive care indeed have the highest wages among SN specialization areas, but ambulatory care instead has the lowest wages. We cannot draw any conclusions about gender from those statistics since they were not divided by gender. However, higher wages were one of the most important factors mentioned by all students in the current study and can therefore not be the only explanation of male nurses' higher interest in certain specialization areas. One other explanation might be that nurses in our study choosing transitory care specialization areas considered the challenge regarding practical skills as most important. Thus, one could draw the conclusions that specialization areas as ambulatory care, anaesthesia and intensive care are seen as more technical, which may be linked to the fact that work in technical fields often is more male‐dominated (The Swedish Occupational Register with statistics, 2017). Abrahamsen (2004) also suggested that male nurses might more often choose to leave specialization areas with bed‐ridden patients with a higher demand for nursing care.
A clear hierarchy between 11 defined specialization areas in Sweden was seen in our study. In previous studies among nurse students, specialization areas like psychiatric care and elderly care have been described to be least popular (Stevens & Crouch, 1995), and in our study they have the lowest status. Ambulatory care has had a strong increase in the number of specialist nurses in Sweden (The National Board of Health and Welfare, 2016) and is among the top‐rated specialization areas in our study. As an alternative for education in the current specialization area, students from the transitory care specialization areas considered anaesthesia, intensive care and ambulatory care. All those three specialization areas are also inside their own transitory care group and the have highest status. SN students in the long‐term care instead considered education outside of SN specialization areas as a top alternative followed by public health care and paediatric nursing. Since their top alternative for specialist education was an education outside the SN specialization areas, nurses in the long‐term care specialization areas seem to be at higher risk of leaving nursing as a career.
6. STRENGTHS AND LIMITATIONS
One challenge in this study was that face‐to‐face administration of paper surveys was not possible because of the overall distance education mode due to ongoing COVID‐19 pandemic. Students were contacted through the contact person at the nursing colleges only three times to answer the survey because of ethical considerations. This study's response rate of 40% is in line with the response rate described in other online surveys by Nulty (2008).
Learning platforms where an open link to the study was posted were only accessible through personal login with password. There by, the risk for undesirable participants were minimal. In addition, the survey included several questions that helped to ensure that no participants other than those who met the inclusion criteria participated. One person failed to provide the correct information confirming their eligibility for the study and was therefore excluded from the study. Other possible study biases such as repeated answering of the survey by the same person and randomly filling the answer were not possible to avoid with our method. On the other hand, participants did not benefit directly from having responded to the survey. Therefore, we consider it unlikely that anyone completed the survey more than once.
The convenience‐based sample size used in this study was adequate for the aim and for the chosen statistical methods. The aim of this study was to identify factors affecting nurses' decision to undergo specialist education and choose a specialty and to describe differences between specialization areas with different types of care. Also, the fact that participants where from three different nursing colleges not only from one is adding the strength to this study. We consider the results to have possibility to be representative of the views of specialist nursing students in Sweden.
There was a high number of significance tests conducted in this study to compare SN students in the transitory care and in the long‐term care specialization areas. The high number of tests risks giving results which are significant only because of chance, that is a high risk for type I error (Bland & Altman, 1995). Bonferroni correction was therefore used in our study to ensure that probability for false‐positive results was reduced.
7. CONCLUSION AND IMPLICATIONS
To make specialist education more attractive, employers might need to consider SNs' expectations on their organization. Although higher wages are important to make nurses feel that they receive a value of the education, there are also other important aspects that influence nurses' willingness to undergo a specialist education. This study shows that in addition to higher wages, SNs wish to achieve a personal and professional development, to be challenged intellectually and practically, to work with new tasks and to enter new areas of responsibilities. Furthermore, the choice of specialization area was not fully determined; instead, many nurses considered more than one specialist area as a possible alternative. This provides an opportunity for the employer to influence and guide the nurses' choice of specialist education by adapting the organization to the nurses' preferences. Therefore, to decrease the shortage of educated nurses, and with that associated patient mortality, there is a need to take into consideration the factors affecting nurses' decision to undergo specialist education and to choose a specialty. Currently, 10% of nurses are not working in health care anymore due to problems with the work environment and working conditions (Governmental inquiry, 2018), but if changes are made, they might return.
AUTHOR CONTRIBUTIONS
All authors have made substantial contributions to conception and design, to analysis and interpretation of the data; they have been involved in drafting the manuscript or review it critically for important intellectual content; they have approved the final version and agreed to be accountable for all aspects of the manuscript.
Funding information
The study was financed by unrestricted grants from the Swedish State under the Agreement Between the Swedish Government and the County Councils, the ALF‐Agreement (RS2019‐1089).
CONFLICT OF INTEREST
The authors have no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the manuscript.
ETHICAL APPROVAL
The Swedish Ethical Board approved this study (2020‐05194), and it was performed in accordance with the Helsinki Declaration (World Medical Association Declaration of Helsinki, 2013). Also, the heads of the participating nursing colleges approved this study. The web‐based survey was anonymous, and we did not gather any information which could identify the participants.
Supporting information
Appendix S1
Tiliander, A. , Olsson, C. , Kalèn, S. , Ponzer, S. S. , & Fagerdahl, A‐M (2023). Factors affecting nurses' decision to undergo a specialist education and to choose a specialty. Nursing Open, 10, 252–263. 10.1002/nop2.1300
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Abrahamsen, B. (2004). Career development and masculinities among male nurses. NORA ‐ Nordic Journal of Feminist and Gender Research, 12, 31–39. 10.1080/08038740410005749 [DOI] [Google Scholar]
- Aiken, L. H. , Sloane, D. , Griffiths, P. , Rafferty, A. M. , Bruyneel, L. , McHugh, M. , Maier, C. B. , Moreno‐Casbas, T. , Ball, J. E. , Ausserhofer, D. , & Sermeus, W. (2017). Nursing skill mix in European hospitals: Cross‐sectional study of the association with mortality, patient ratings, and quality of care. BMJ Quality and Safety, 26, 559–568. 10.1136/bmjqs-2016-005567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aiken, L. H. , Sloane, D. M. , Bruyneel, L. , Van den Heede, K. , Griffiths, P. , Busse, R. , Diomidous, M. , Kinnunen, J. , Kózka, M. , Lesaffre, E. , McHugh, M. D. , Moreno‐Casbas, M. T. , Rafferty, A. M. , Schwendimann, R. , Scott, P. A. , Tishelman, C. , van Achterberg, T. , & Sermeus, W. (2014). Nurse staffing and education and hospital mortality in nine European countries: A retrospective observational study. Lancet, 383, 1824–1830. 10.1016/s0140-6736(13)62631-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Audet, L. A. , Bourgault, P. , & Rochefort, C. M. (2018). Associations between nurse education and experience and the risk of mortality and adverse events in acute care hospitals: A systematic review of observational studies. International Journal of Nursing Studies, 80, 128–146. 10.1016/j.ijnurstu.2018.01.007 [DOI] [PubMed] [Google Scholar]
- Bexelius, T. S. , Olsson, C. , Järnbert‐Pettersson, H. , Parmskog, M. , Ponzer, S. , & Dahlin, M. (2016). Association between personality traits and future choice of specialization among Swedish doctors: A cross‐sectional study. Postgraduate Medical Journal, 92, 441–446. 10.1136/postgradmedj-2015-133478 [DOI] [PubMed] [Google Scholar]
- Bland, J. M. , & Altman, D. G. (1995). Multiple significance tests: The Bonferroni method. BMJ, 310, 170. 10.1136/bmj.310.6973.170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooley, M. C. (2008). Nurses' motivations for studying third level post‐registration nursing programmes and the effects of studying on their personal and work lives. Nurse Education Today, 28, 588–594. 10.1016/j.nedt.2007.11.002 [DOI] [PubMed] [Google Scholar]
- CSN . (2021). Student grants and loans for studies in Sweden . https://www.csn.se/languages/english/student‐grants‐and‐loans‐for‐studies‐in‐sweden.html
- Dury, C. , Hall, C. , Danan, J. L. , Mondoux, J. , Aguiar Barbieri‐Figueiredo, M. C. , Costa, M. A. , & Debout, C. (2014). Specialist nurse in Europe: Education, regulation and role. International Nursing Review, 61, 454–462. 10.1111/inr.12123 [DOI] [PubMed] [Google Scholar]
- Governmental inquiry . (2018). The specialist nurse of the future ‐ new role, new opportunities. (SOU 2018:77). https://www.regeringen.se/4ab6f6/contentassets/6f67c0e786f0491899a98579a002508c/framtidens‐specialistsjukskoterska‐‐ny‐roll‐nya‐mojligheter‐sou‐201877
- Harrison, C. A. , Hauck, Y. , & Hoffman, R. (2014). Choosing and remaining in mental health nursing: Perceptions of Western Australian nurses. International Journal of Mental Health Nursing, 23, 561–569. 10.1111/inm.12094 [DOI] [PubMed] [Google Scholar]
- Haryanto, M. (2019). Nursing shortage: Myth or fact? Orthopaedic Nursing, 38, 1–2. 10.1097/nor.0000000000000535 [DOI] [PubMed] [Google Scholar]
- Hays, R. D. , Sherbourne, C. D. , & Mazel, R. M. (1993). The RAND 36‐item health survey 1.0. Health Economics, 2, 217–227. 10.1002/hec.4730020305 [DOI] [PubMed] [Google Scholar]
- John, O. P. , & Srivastava, S. (1999). The big five trait taxonomy: History, measurement, and theoretical perspectives. In Pervin L. A. & John O. P. (Eds.), Handbook of personality: Theory and research (pp. 102–138). Guilford Press. [Google Scholar]
- Knap, M. , Ozga, D. , Krupa, S. , Penar‐Zadarko, B. , Medrzycka‐Dabrowska, W. , Witt, P. , & Friganovic, A. (2020). Position statement of the European specialist nurses organisation (ESNO) in specialist nursing as advanced practice nursing towards 2030. Pielegniarstwo xxi Wieku‐nursing in the 21. Century, 19(4), 274–280. 10.2478/pielxxiw-2020-0032 [DOI] [Google Scholar]
- Lindgren, B. M. , Lundman, B. , & Graneheim, U. H. (2020). Abstraction and interpretation during the qualitative content analysis process. International Journal of Nursing Studies, 108, 103632. 10.1016/j.ijnurstu.2020.103632 [DOI] [PubMed] [Google Scholar]
- Lowe, G. (2017). Nurse practitioners: Framing their professional identity. The Journal for Nurse Practitioners, 13(2), 175. 10.1016/j.nurpra.2016.12.021 [DOI] [Google Scholar]
- McCabe, R. , Nowak, M. , & Mullen, S. (2005). Nursing careers: What motivated nurses to choose their profession? Australian Bulletin of Labour, 31, 380–402. [Google Scholar]
- Morgenthaler, M. (2009). Too old for school? Barriers nurses can overcome when returning to school. AORN Journal, 89(335–337), 341–335. 10.1016/j.aorn.2008.09.004 [DOI] [PubMed] [Google Scholar]
- Nulty, D. D. (2008). The adequacy of response rates to online and paper surveys: What can be done? Assessment and Evaluation in Higher Education, 33, 301–314. 10.1080/02602930701293231 [DOI] [Google Scholar]
- O'Cathain, A. , & Thomas, K. J. (2004). "Any other comments?" open questions on questionnaires—A bane or a bonus to research? BMC Medical Research Methodology, 4, 25. 10.1186/1471-2288-4-25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olsson, C. , Järnbert‐Pettersson, H. , Ponzer, S. , Dahlin, M. , & Bexelius, T. (2019). Swedish doctors choice of medical speciality and associations with cultural capital and perceived status: A cross‐sectional study. BMC Medical Education, 19, 244. 10.1186/s12909-019-1691-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orwelius, L. , Nilsson, M. , Nilsson, E. , Wenemark, M. , Walfridsson, U. , Lundström, M. , Taft, C. , Palaszewski, B. , & Kristenson, M. (2017). The Swedish RAND‐36 health survey—Reliability and responsiveness assessed in patient populations using Svensson's method for paired ordinal data. Journal of Patient‐Reported Outcomes, 2, 4. 10.1186/s41687-018-0030-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ranchal, A. , Jolley, M. J. , Keogh, J. , Lepiesová, M. , Rasku, T. , & Zeller, S. (2015). The challenge of the standardization of nursing specializations in Europe. International Nursing Review, 62, 445–452. 10.1111/inr.12204 [DOI] [PubMed] [Google Scholar]
- Rognstad, M. K. , & Aasland, O. (2007). Change in career aspirations and job values from study time to working life. Journal of Nursing Management, 15, 424–432. [DOI] [PubMed] [Google Scholar]
- Rognstad, M. K. , Aasland, O. , & Granum, V. (2004). How do nursing students regard their future career? Career preferences in the post‐modern society. Nurse Education Today, 24, 493–500. 10.1016/j.nedt.2004.07.015 [DOI] [PubMed] [Google Scholar]
- Saager, L. , Ruetzler, K. , Turan, A. , Maheshwari, K. , Cohen, B. , You, J. , Mascha, E. J. , Qiu, Y. , Ince, I. , & Sessler, D. I. (2021). Do it often, do it better: Association between pairs of experienced subspecialty anesthesia caregivers and postoperative outcomes. A retrospective observational study. Anesthesia and Analgesia, 132, 866–877. 10.1213/ane.0000000000005318 [DOI] [PubMed] [Google Scholar]
- Scheffler, R. M. , & Arnold, D. R. (2019). Projecting shortages and surpluses of doctors and nurses in the OECD: What looms ahead. Health Economics, Policy, and Law, 14, 274–290. 10.1017/s174413311700055x [DOI] [PubMed] [Google Scholar]
- Stanley, D. , Beament, T. , Falconer, D. , Haigh, M. , Saunders, R. , Stanley, K. , Wall, P. , & Nielson, S. (2016). The male of the species: A profile of men in nursing. Journal of Advanced Nursing, 72, 1155–1168. 10.1111/jan.12905 [DOI] [PubMed] [Google Scholar]
- Stevens, J. , & Crouch, M. (1995). Who cares about care in nursing education? International Journal of Nursing Studies, 32, 233–242. 10.1016/0020-7489(95)00002-f [DOI] [PubMed] [Google Scholar]
- Swedish Higher Education Ordinance . (1993). Swedish Council for Higher Education. https://www.uhr.se/en/start/laws‐and‐regulations/Laws‐and‐regulations/The‐Higher‐Education‐Ordinance/
- The National Board of Health and Welfare . (2016). Availability of specialist nurses and radiological nurses in 2014. https://www.socialstyrelsen.se/globalassets/sharepoint‐dokument/artikelkatalog/statistik/2016‐11‐2.pdf
- The Swedish Occupational Register with statistics . (2017). Register of occupations with occupational statistics 2017 . https://www.scb.se/contentassets/1fe7f957920f4eaf97bddcc0270553f2/am0208_2017a01_sm_am33sm1901.pdf
- Vårdförbundet . (2016). Progress report on average pay, wage differentials and lifetime earnings for occupational groups in the Swedish Healthcare Workers' Union . https://www.vardforbundet.se/siteassets/engagemang‐och‐paverkan/sa‐paverkar‐vardforbundet/vardforbundets‐livsonerapport‐2016
- World Health Organization (WHO) . (2020). State of the world's nursing 2020: investing in education, jobs and leadership . https://www.who.int/publications/i/item/9789240003279
- World Medical Association Declaration of Helsinki . (2013). Ethical principles for medical research involving human subjects. JAMA, 310, 2191–2194. 10.1001/jama.2013.281053 [DOI] [PubMed] [Google Scholar]
- Zakrisson, I. (2010). Big five inventory (BFI): Testing for Swedish conditions. Social Science Reports from Mid Sweden University. [Google Scholar]
- Zhu, H. , Xu, C. , Jiang, H. , & Li, M. (2021). A qualitative study on the experiences and attributions for resigned nurses with career plateau. International Journal of Nursing and Health Sciences, 8, 325–331. 10.1016/j.ijnss.2021.05.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.