

Abstract
Background: Gated myocardial perfusion single-photon emission computed tomography (SPECT) has been used to non-invasively evaluate the left ventricular (LV) volume and function. This study aimed to measure the normal and range values for heart risk view-function (HRV-F) software using the Japanese Society of Nuclear Medicine Working Group (JSNM-WG) normal database and clarify the characteristics of the normal database.
Methods:We used 206 myocardial perfusion short-axis images from the normal database. Ejection fraction (EF), end-systolic volume (ESV), end-diastolic volume (EDV), peak filling rate (PFR), 1/3 mean filling rate (MFR), time to PFR (TTPF), and TTPF divided by RR interval (TPFR/RR) were calculated. Phase parameters of 95% histogram bandwidth and standard deviation were also computed using the phase analysis. The relationships among phase parameters, LV volumes, and body surface area (BSA) were evaluated in the age group of ≤65 years.
Results: Higher EF was observed in females than in males (p<0.0001). EDV and ESV were significantly higher in males than in females (p<0.0001). Additionally, PFR and 1/3 MFR significantly differed between sexes (p≤0.075). Phase parameters were higher in males than in females, and higher at stress than at rest. All diastolic parameters showed no significant differences between sexes in any age group, whereas differences have remained in phase values. Phase parameters were weakly correlated with EDV (r=0.31), ESV (r=0.43), and BSA (r=0.27), respectively.
Conclusions: Mean normal and range values of the normal database were determined using the HRV-F software. The normal and range values can help diagnose gated SPECT data in patients with cardiac diseases.
Keywords: 99mTc-sestamibi database, 99mTc-tetrofosmin database, Automatic quantification, Gated myocardial perfusion SPECT, Japanese Society of Nuclear Medicine (JSNM) working group, Normal database
Gated myocardial perfusion single-photon emission computed tomography (SPECT), using 99mTc-labeled radiopharmaceuticals, is one of the most common examinations in nuclear medicine, which can non-invasively evaluate the left ventricular (LV) function (1). In recent years, phase analysis in gated myocardial perfusion SPECT is considered important for the LV mechanical dyssynchrony evaluation, which helps diagnose and prognosticate patients with cardiac diseases (2).
Currently, quantitative analysis software, such as quantitative gated SPECT (QGS, Cedars-Sinai Medical Center, Los Angeles, CA, USA), heart risk view-function (HRV-F, Nihon Medi-Physics, Tokyo, Japan) (3), and cardioREPO (cREPO, FUJIFILM RI Pharma, Tokyo, Japan; PDRadiopharma, Tokyo, Japan, at present), have been used in clinical examinations in Japan. However, calculated cardiac functions differ depending on the software programs when gated myocardial perfusion SPECT is used. Moreover, patient sex affects cardiac functional values. Consequently, normal and range values have been reported to help the diagnosis as the baseline to discriminate between normal and abnormal conditions (4). We have determined normal and range values for QGS and cREPO software using the Japanese Society of Nuclear Medicine Working Group (JSNM-WG) database (5–7).
The Japanese assessment of cardiac events and survival study by gated SPECT (J-ACCESS) and a number of clinical studies using HRV-F software have been conducted and exhibited that the LV function and phase parameters were helpful for the diagnosis of coronary artery disease, prognostic risk stratification, and determination of subsequent treatments (8–10). However, few studies have reported the mean and range of normal values for HRV-F were to compare software differences (5, 7). Consequently, we tried to determine mean and range values for HRV-F software so that these values could aid the interpretation of LV function and phase parameters. This study aimed to measure the normal values and range for HRV-F software using the JSNM-WG and clarify the characteristics of the normal database.
Materials and methods
JSNM-WG normal database
A normal database of gated myocardial perfusion SPECT by JSNM-WG was used (5, 11). All patients underwent stress-rest 99mTc-sestamibi or 99mTc-tetrofosmin gated myocardial perfusion SPECT. A total of 206 short-axis images of 106 males and 100 females were used.
Sex differences were examined for diastolic and phase parameters in 206 patients. The younger age group was defined as ≤65 years (52 males and 45 females), and the details of the normal database have been published elsewhere (5, 6).
Data acquisition and image processing condition
The images were acquired with 64×64 matrices, R-R division number of 16, and 180° or 360° gamma camera rotation. All image data were reconstructed by a filtered back-projection method, without attenuation and scatter corrections. All images were acquired with a stress-preceding protocol.
LV ejection fraction (EF), end-systolic volume (ESV), end-diastolic volume (EDV), peak filling rate (PFR), 1/3 mean filling rate (MFR), time to PFR (TTPF), and TTPF divided by RR interval (TPFR/RR) were calculated. The 95% histogram bandwidth and phase standard deviation (SD) were also computed using the phase analysis of gated SPECT. All functional values were calculated for each sex using the H-RVF, QGS, and cREPO software.
Statistical analysis
Data were expressed as mean±SD. Continuous variables were compared usinga student t-test for parametric distribution and Wilcoxon signed-rank test for non-parametric distribution. Normal distribution was determined using the Shapiro-Wilk test. The Tukey-Kramer test was used for multiple comparisons in LV function and phase parameters. Pearson's correlation analysis was used to evaluate the relationship between two variables. All statistical tests were two-tailed, and p-values of <0.05 were considered significant. These analyses were performed using the JMP version 11.2.1 (SAS Institute Inc., Cary, NC, USA) software.
Results
Comparison between sexes
Table 1 shows the normal values of LV volumes, diastolic parameters, and phase parameters for stress and rest conditions in males and females. The EF was higher in females than in males (p<0.0001). Both EDV and ESV were significantly higher in males than in females (p<0.0001). Additionally, PFR and 1/3 MFR significantly differed between sexes (p=0.075). Both 95% bandwidth and phase SD were higher in males than in females, and higher at stress than at rest.
Table 1. Normal values and ranges for LV volume, diastolic, and phase parameters.
| Males Mean±SD (Mean −2SD to +2SD) |
Females Mean±SD (Mean −2SD to +2SD) |
p-value | |
|---|---|---|---|
| Stress condition | |||
| LV volume | |||
| EF (%) | 69.4±6.2 (57.0–81.8) | 73.8±6.6 (60.6–87.0) | <0.0001 |
| EDV (mL) | 81.3±20.0 (41.3–121.3) | 59.9±13.9 (32.1–87.7) | <0.0001 |
| ESV (mL) | 25.2±9.2 (6.8–43.6) | 15.7±5.5 (4.7–26.7) | <0.0001 |
| EDVI (mL/m2) | 48.3±11.4 (25.5–71.1) | 40.4±8.4 (23.6–57.2) | <0.0001 |
| ESVI (mL/m2) | 14.9±5.4 (4.1–25.7) | 10.6±3.6 (3.4–17.8) | <0.0001 |
| Diastolic parameters | |||
| PFR (per s) | 2.36±0.54 (1.28–3.44) | 2.59±0.64 (1.31–3.87) | 0.0205 |
| 1/3 MFR (per s) | 1.46±0.32 (0.82–2.10) | 1.60±0.36 (0.88–2.32) | 0.0060 |
| TTPF (ms) | 177±35 (107–247) | 168±31 (106–230) | n.s. |
| TTPF/RR interval | 0.20±0.06 (0.08–0.32) | 0.19±0.05 (0.09–0.29) | n.s. |
| Phase parameters | |||
| Bandwidth (degree) | 33.9±12.3 (9.3–58.5) | 26.5±10.7(5.1–47.9) | <0.0001 |
| Phase SD (degree) | 9.2±3.4 (2.4–16.0) | 7.2±2.8 (1.6–12.8) | <0.0001 |
| Rest condition | |||
| LV volume | |||
| EF (%) | 68.3±6.1 (56.1–80.5) | 72.6±6.2 (60.2–85.1) | <0.0001 |
| EDV (mL) | 81.6±19.6 (42.4–120.8) | 60.0±14.5 (30.9–89.1) | <0.0001 |
| ESV (mL) | 26.0±8.7 (8.6–43.4) | 16.4±5.8 (4.9–27.9) | <0.0001 |
| EDVI (mL/m2) | 48.5±10.9 (26.7–70.3) | 40.4±8.9 (22.6–58.2) | <0.0001 |
| ESVI (mL/m2) | 15.4±5.1 (5.2–25.6) | 11.1±3.7 (3.7–18.5) | <0.0001 |
| Diastolic parameters | |||
| PFR (per s) | 2.25±0.49 (1.27–3.23) | 2.50±0.57 (1.36–3.64) | 0.0023 |
| 1/3 MFR (per s) | 1.47±0.33 (0.81–2.13) | 1.61±0.38 (0.85–2.37) | 0.0122 |
| TTPF (ms) | 173±36 (101–245) | 170±39 (92–248) | n.s. |
| TTPF/RR interval | 0.19±0.06 (0.05–0.33) | 0.19±0.05 (0.09–0.29) | n.s. |
| Phase parameters | |||
| Bandwidth (degree) | 25.6±9.7 (6.2–45.0) | 20.8±8.0(4.8–36.8) | <0.0006 |
| Phase SD (degree) | 6.9±2.6 (1.7–12.1) | 5.7±2.2 (1.3–10.1) | <0.0017 |
EDV: end-diastolic volume, EF: ejection fraction, ESV: end-systolic volume, LV: left ventricular, MFR: mean filling rate, PFR: peak filling rate, SD: standard deviation, TTPF: time to PFR
The normal values were examined in two age groups, namely, ≤65 (n=97) and >65 years (n=109), and sex differences were compared for diastolic and phase parameters in the younger age group of ≤65 years (52 males and 45 females). Table 2 shows normal values and ranges of diastolic and phase parameters. All diastolic parameters showed no significant differences between sexes, whereas phase value differences have been observed between sexes. Moreover, phase value differences remained between stress and rest conditions, in males and females for 95% bandwidth (p<0.0001 and p<0.0001, respectively) and phase SD (p<0.0001 and p<0.0001, respectively). Although the diastolic parameters were comparable in the younger age group among the three software programs, TTPF showed no sex difference in HRV-F (177±35 vs. 168±31 for males and females, respectively). However, QGS and cREPO showed significant differences in TTPF between males and females (175±33 vs. 165±30, p=0.024; and 171±46 vs. 153±38, p=0.001; respectively).
Table 2. Normal values and ranges for diastolic and phase parameters in the age group of ≤65.
| Males Mean±SD (Mean −2SD to +2SD) |
Females Mean±SD (Mean −2SD to +2SD) |
p-value | |
|---|---|---|---|
| Stress condition | |||
| Diastolic parameters | |||
| PFR (per s) | 2.53±0.53 (1.47–3.59) | 2.64±0.52 (1.60–3.68) | n.s. |
| 1/3 MFR (per s) | 1.48±0.32 (0.85–2.11) | 1.59±0.35 (0.89–2.30) | n.s. |
| TTPF (ms) | 178±29 (119–237) | 174±28 (118–231) | n.s. |
| TTPF/RR interval | 0.21±0.06 (0.10–0.32) | 0.20±0.04 (0.12–0.28) | n.s. |
| Phase parameters | |||
| Bandwidth (degree) | 36.9±12.0 (13.0–60.8) | 25.6±8.1 (9.4–41.9) | <0.0001 |
| Phase SD (degree) | 10.1±3.3 (3.4–16.8) | 6.9±2.2 (2.6–11.3) | <0.0001 |
| Rest condition | |||
| Diastolic parameters | |||
| PFR (per s) | 2.44±0.50 (1.44–3.44) | 2.59±0.60 (1.40–3.79) | n.s. |
| 1/3 MFR (per s) | 1.56±0.36 (0.84–2.27) | 1.70±0.42 (0.87–2.54) | n.s. |
| TTPF (ms) | 171±33 (106–236) | 165±33 (99–231) | n.s. |
| TTPF/RR interval | 0.20±0.06 (0.08–0.31) | 0.18±0.03 (0.11–0.25) | n.s. |
| Phase parameters | |||
| Bandwidth (degree) | 27.0±9.7 (7.6–46.5) | 19.0±7.2 (4.5–33.4) | <0.001 |
| Phase SD (degree) | 7.2±2.6 (2.0–12.4) | 5.1±1.9 (1.4–8.9) | <0.001 |
MFR: mean filling rate, PFR: peak filling rate, SD: standard deviation, TTPF: time to PFR
Comparison of LV volume and phase parameters
Figure 1 shows the relationships of phase parameters and LV volumes; and of those depending on body habitus. The 95% bandwidth correlated with EDV (r=0.31), ESV (r=0.43), and body surface area (BSA, r=0.27). Phase SD also correlated with EDV (r=0.26) and ESV (r=0.39), and BSA (r=0.23).
Figure 1.
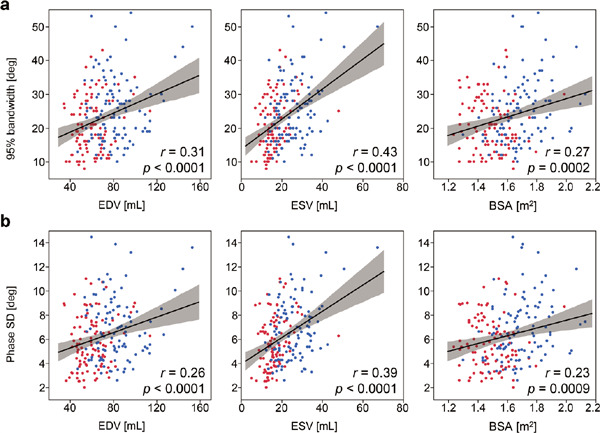
Relationships of phase parameters and LV volumes, and those depending on body habitus at rest condition.
a: Scatter plots of 95% bandwidth and EDV (left) and ESV (middle), and a scatter plot of that by BSA (right).
b: Scatter plots of phase SD and EDV (left) and ESV (middle), and a scatter plot of that by BSA (right).
Blue and red points indicate male and female data, respectively. The shaded area denotes a 95% confidence band around the fitted line.
BSA: body surface area, EDV: end-diastolic volume, ESV: end-systolic volume, LV: left ventricular, SD: standard deviation
The comparison of the normal values with the three software programs revealed similarities in phase values between QGS and HRV-F: 28.5±17.9 vs. 25.6±9.7 for males (p=n.s.) and 22.0±12.2 vs. 20.9±8.0 for females (p= n.s.) in bandwidth; and 8.8±7.4 vs. 6.9±2.6 for males (p= 0.0047) and 6.9±6.8 vs. 5.7±2.2 for females (p=n.s.) in phase SD, respectively. However, 95% bandwidth and phase SD of cREPO showed higher values (42.9±12.2 for males [p<0.001 for comparing HRV-F] and 36.8±9.1 for females [p<0.001]; and 10.6±2.6 [p<0.001] and 9.2±2.1[p<0.001], respectively).
Discussion
The mean and ranges of normal subjects were determined using the JSNM-WG normal database and HRV-F, and the main results are summarized as follows. EF was significantly higher in females, and both EDV and ESV were significantly higher in males. PFR and 1/3 MFR in the diastolic parameters were significantly different between sexes; however, TTPF and TTPF/RR were not significantly different between sexes. Phase values were higher at stress than at rest. Moreover, phase values for males are higher than those for females.
Previous studies by Nakajima et al. used the JSNM-WG database and QGS and cREPO software to determine normal values of LV volumes and diastolic parameters (5, 6). When compared with these studies, EF for HRV-F was nearly equivalent to those for QGS and cREPO. EDV and ESV volumes were similar between HRV-F and QGS. Regarding the diastolic parameters, we calculated normal values in the younger age group of <65 years, because the aged subjects show abnormal diastolic dysfunction, which caused a wide range of normal values (5). The diastolic parameters were comparable in the younger age group among the three software programs. However, TTPF was significantly higher in males than that in females in QPS and cREPO software. The characteristics of software programs should be taken into consideration in diagnosing gated SPECT data.
Phase parameters are affected by software, sex, and radiopharmaceutical dosage. The phase parameters based on sex differences have been reported (7), and a similar trend was found in this study. The differences in injected radiopharmaceutical dosage influence photon count statistics and image noise (12–14); thus, phase values would change depending on the stress and rest conditions in myocardial perfusion SPECT. Regarding the relationships among phase parameters, LV volume, and body habitus, the 95% bandwidth and phase SD were weakly correlated with EDV, ESV, and BSA. Such weak correlations between phase parameters and LV volumes were also observed in the previous study using the cREPO software program (6).
This study has several limitations. The JSNM-WG normal database was collected using clinically acceptable image quality and optimal image processing conditions, and the selection criteria were clearly defined. However, JSNM-WG normal database provides short-axis images, which include the differences in acquisition and image processing conditions, although acceptable image quality was confirmed during database accumulation. Lastly, the latest cardiac imaging cameras, such as cadmium-zinc-telluride cameras, were not included and required a new database.
Conclusions
Mean normal values and ranges of the JSNM-WG normal database were determined using the HRV-F software. Sex differences were exhibited in the LV volumes, diastolic parameters, and phase parameters except for TTPF and TTPF/RR. In future clinical researches using HRV-F software, the mean and normal ranges of this study can be applied to diagnostic and prognostic analyses. Moreover, when the mean and range of normal values for the LV function and phase parameters are incorporated into HRV-F software, automatic detection of abnormal parameters will be feasible, which is clinically convenient to help diagnose gated SPECT data in patients with cardiac diseases.
Acknowledgments
The authors thank physicians and technologists who contributed to the accumulation and generation of the JSNMWG normal database. The authors also thank Enago (www.enago.jp) for English language editing.
Sources of funding
None.
Conflicts of interest
K. Nakajima belongs to endowed department partly funded by Nihon Medi Physics, Tokyo, Japan; PDRadiopharma, Tokyo, Japan; and Siemens Healthcare Japan, Tokyo, Japan. Others have no conflict of interest to disclose.
References
- 1. JCS Joint WorkingGourp. Guidelines for clinical use of cardiac nuclear medicine (JCS 2010) – digest version –. Circ J 2012; 76: 761-7. [DOI] [PubMed] [Google Scholar]
- 2. Chen J, Garcia EV, Folks RD, Cooke CD, Faber TL, Tauxe EL, et al. Onset of left ventricular mechanical contraction as determined by phase analysis of ECG-gated myocardial perfusion SPECT imaging: development of a diagnostic tool for assessment of cardiac mechanical dyssynchrony. J Nucl Cardiol 2005; 12: 687-95. [DOI] [PubMed] [Google Scholar]
- 3. Kobayashi K, Tsukamoto K. Myocardial image analysis software heart risk view, heart score view and heart function view. The Japanese Journal of Nuclear Medicine Technology 2014; 34: 136-44. [Article in Japanese] [Google Scholar]
- 4. Nakae I, Hayashi H, Matsumoto T, Mitsunami K, Horie M. Clinical usefulness of a novel program “Heart Function View” for evaluating cardiac function from gated myocardial perfusion SPECT. Ann Nucl Med 2014; 28: 812-23. [DOI] [PubMed] [Google Scholar]
- 5. Nakajima K, Matsumoto N, Kasai T, Matsuo S, Kiso K, Okuda K. Normal values and standardization of parameters in nuclear cardiology: Japanese Society of Nuclear Medicine working group database. Ann Nucl Med 2016; 30: 188-99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Okuda K, Nakajima K. Normal values and gender differences of left ventricular functional parameters with cardioREPO software. Ann Nucl Cardiol 2017; 3: 29-33. [Google Scholar]
- 7. Nakajima K, Okuda K, Matsuo S, Kiso K, Kinuya S, Garcia EV. Comparison of phase dyssynchrony analysis using gated myocardial perfusion imaging with four software programs: Based on the Japanese Society of Nuclear Medicine working group normal database. J Nucl Cardiol 2017; 24: 611-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Sakatani T, Nakajima K, Nishimura T. Cardiovascular event risk estimated by myocardial perfusion SPECT combined with clinical data. J Cardiol 2022; 80: 64-71. [DOI] [PubMed] [Google Scholar]
- 9. Hatta T, Yoda S, Hayase M, Monno K, Hori Y, Fujito H, et al. Prognostic value of left ventricular dyssynchrony assessed with nuclear cardiology in patients with known or suspected stable coronary artery disease with preserved left ventricular ejection fraction. Int Heart J 2020; 61: 685-94. [DOI] [PubMed] [Google Scholar]
- 10. Fujito H, Yoda S, Hatta T, Hori Y, Hayase M, Miyagawa M, et al. Prognostic significance of left ventricular dyssynchrony assessed with nuclear cardiology for the prediction of major cardiac events after revascularization. Intern Med 2021; 60: 3679-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Nakajima K. Normal values for nuclear cardiology: Japanese databases for myocardial perfusion, fatty acid and sympathetic imaging and left ventricular function. Ann Nucl Med 2010; 24: 125-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Aljaroudi W, Koneru J, Heo J, Iskandrian AE. Impact of ischemia on left ventricular dyssynchrony by phase analysis of gated single photon emission computed tomography myocardial perfusion imaging. J Nucl Cardiol 2011; 18: 36-42. [DOI] [PubMed] [Google Scholar]
- 13. Mukherjee A, Singh H, Patel C, Sharma G, Roy A, Naik N. Normal values of cardiac mechanical synchrony parameters using gated myocardial perfusion single-photon emission computed tomography: Impact of population and study protocol. Indian J Nucl Med 2016; 31: 255-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kortelainen MJ, Koivumäki TM, Vauhkonen MJ, Hakulinen MA. Dependence of left ventricular functional parameters on image acquisition time in cardiac-gated myocardial perfusion SPECT. J Nucl Cardiol 2015; 22: 643-51. [DOI] [PubMed] [Google Scholar]