

Abstract
Background: Triglyceride deposit cardiomyovasculopathy (TGCV) is a rare intractable cardiovascular disorder (Orphanet ORPHAcode: 565612) in which defective intracellular lipolysis results in heart failure and coronary artery disease. Myocardial scintigraphy with 123I-β-methyl-p-iodophenylpentadecanoic acid (BMIPP) is useful to evaluate myocardial TG metabolism; its washout rate (WR) reflects myocardial lipolysis. This study reports the effects of CNT-01 (tricaprin), a developing orphan drug to facilitate lipolysis, on BMIPP-WR in patients with TGCV.
Methods: An investigator-initiated, multicenter, randomized, double-blind exploratory, trial (Phase IIa) was conducted (UMIN000035403). Seventeen patients with idiopathic TGCV were orally administered 1.5 g/day of CNT-01 or placebo for 8 weeks. Endpoints included delta BMIPP-WR and clinical parameters such as 6-minwalk distance and TGCV severity score.
Results: During the protocol, delta BMIPP-WRs were −0.26±3.28 and 7.08±3.28% (95% confidence intervals, −7.36 to 6.84 and −0.01 to 14.18) in the placebo and CNT-01 groups, respectively. The baseline-adjusted difference of delta BMIPP-WR between the two groups was significant (p=0.035) after one patient was excluded from the placebo group because of pseudonormalization of BMIPP-WR related to coronary bypass graft stenosis. Clinical parameters did not show significant changes.
Conclusions: This study proved the mechanism of CNT-01 to improve myocardial lipolysis in TGCV, as demonstrated by BMIPP scintigraphy.
Keywords: BMIPP, Randomized controlled trial, Rare disease, Triglyceride deposit cardiomyovasculopathy
Triglyceride deposit cardiomyovasculopat hy (TGCV) is a novel rare cardiovascular disorder we firstreport ed in 2008 in patients with severe heart failure (HF) requiring cardiac transplantation (Orphanet ORPHA code: 565612) (1–3). In the normal heart, long-chain fatty acid (LCFA) and its triglyceride (LCTG) is the major energy source (4). LCFA in plasma is taken up via cell surface receptors and re-esterified to produce LCTG, which is immediately hydrolyzed by intracellular lipases such as adipose triglyceride lipase (ATGL) (5), and released LCFA is oxidized in the mitochondria to produce ATP. In TGCV, the defective intracellular lipolysis of LCTG results in ectopic LCTG deposition and loss of LCFA supply, leading to lipotoxicity and energy failure in cardiomyocytes and vascular smooth muscle cells (1–3). As a result, patients with TGCV exhibit adult-onset HF and diffuse narrowing coronary artery disease (CAD). TGCV is classified into primary and idiopathic types with and without mutations of PNPLA2 encoding ATGL, respectively (3, 6).
β-methyl-p-iodophenylpentadecanoic acid (BMIPP) is an LCFA with the presence of a methyl group at the beta position, first developed by Knapp et al. Because of its high first-pass extraction and long retention in the myocardium, 123I-BMIPP is suitable for single-photon emission computed tomography (SPECT) imaging (7). Because earlier studies have indicated that the kinetics of 123I-BMIPP were similar to those of LCFA, 123I-BMIPP was approved in 1993 as an in vivo diagnostic radiotracer in Japan to evaluate the myocardial metabolism of LCFA and LCTG (8). Since 2015, we have reported that the washout rate of BMIPP (BMIPP-WR) was defective in both primary and idiopathic TGCV (I-TGCV) (3, 9), indicating that BMIPP-WR can reflect myocardial lipolysis. Based on these findings, we developed the diagnostic criteria for TGCV including the cutoff value of BMIPP-WR, as an essential item (10, 11).
Along with increases in the awareness of this disease and the cumulative number of clinically diagnosed patients, the severe prognosis of patients with TGCV has subsequently been clarified as follows: 1) The first registry data indicated that 8 of 20 cases registered were fatal (3), 2) TGCV patients with CAD were resistant to standard remedies including cholesterol-lowering drugs and percutaneous coronary intervention (12, 13), and 3) BMIPP-WR may be a prognostic factor for TGCV patients with heart failure (14). Therefore, the development of treatments targeting myocardial lipolysis in TGCV is urgent. Our study group has been performing academia-initiated development of a potential drug, CNT-01, for which the active ingredient is tricaprin, a class of medium-chain triglyceride (3). A preclinical study using a mouse model of TGCV indicated that CNT-01 had a potent ability to facilitate myocardial lipolysis, as demonstrated by reduced myocardial TG contents and increased BMIPP-WR; this subsequently improved cardiac function by cardiac CT scan (15). Thereafter, we confirmed the clinical safety of CNT-01 in phases I and I/IIa clinical trials.
Herein, we report the effect of CNT-01 on BMIPP-WR in myocardial scintigraphy in an investigator-initiated phase IIa randomized placebo-controlled clinical trial (RCT) in patients with I-TGCV. We further discuss the clinical significance and applications of BMIPP-WR in patients with heart diseases.
Study protocol and methods
Objectives
The aim of the present investigator-initiated clinical trial was to investigate the efficacy and safety of 8-week oral administration of CNT-01, which was developed by the Osaka University Hospital, in patients with TGCV in order to finally achieve the first drug approval for TGCV in Japan.
Study period
December 2018 to April 2019.
Decision of study protocol and oversight
All study protocol including duration and endpoints were decided after several round discussions between the Pharmaceuticals and Medical Devices Agency (PMDA), the regulatory authority in Japan, and investigators in academia. It should be noted that the above discussions were made based upon scientific knowledge of TGCV and CNT-01 before starting the clinical trial (December 2018). The trial was conducted in accordance with provisions of the Declaration of Helsinki, Good Clinical Practice (GCP) and applicable regulatory requirement. Prior to the conduct of study, institutional review board in each participating institution approved the contents of protocol and the appropriateness of the study. Written informed consents were obtained from all participants.
Developmental phase and study design
Multi-center, double-blinded, repeated-dose exploratoty Phase IIa study was conducted (UMIN000035403). Either 1.5 g per day of CNT-01 or placebo was orally administered for 8 weeks.
Patient population
As mentioned above, TGCV has two types. Primary TGCV is ultra-rare; only four survivors were identified at the start of this clinical trial, whereas I-TGCV is rare, but relatively larger. The number of clinically diagnosed cases was 131, of which 22 patients had already died (9). According to the discussion with PMDA, we decided that the participants for this study were patients with I-TGCV. The inclusion and exclusion criteria were as follows:
Inclusion criteria;
-
1.
Patients with the definite diagnosis of I-TGCV
-
2.
Patients whose BMIPP-WR is 5% or less
-
3.
Patients with a 6-minute walking distance (6MWD) less than 400 meters
-
4.
Patients who received and fully understood an adequate explanation for participation in the trial and who provided written informed consent
-
5.
Patients aged 20 years or older at the time of obtaining informed consent.
-
6.
Patients who are able to take the investigational products orally
Exclusion criteria;
-
1.
Patients who underwent coronary revascularization within 1 month prior to study participation
-
2.
Patients with fasting serum capric acid concentration of 10 µmol/L or higher
-
3.
Patients who have been on a diet containing medium-chain fatty acid at least once in the past
-
4.
Patients with diabetic ketoacidosis
-
5.
Women of childbearing potential, pregnant women, or lactating women
-
6.
Patients with New York Heart Association (NYHA) class IV
-
7.
Patients with acute coronary syndromes
-
8.
Patients with a history of drug addiction
-
9.
Patients allergic to any component of the investigational products
-
10.
Patients allergic to BMIPP or iodine
-
11.
Patients with a history of clinically significant drug allergy
-
12.
Patients with severe hepatic dysfunction (Child-Pugh classifications B and C). However, if the patient is taking anticoagulants (warfarin, dabigatran, ribaloxaban, apixaban, and edoxaban), that interfere with the prothrombin timemeasurement, the prothrombin time score should be classified as 2
-
13.
Patients who have participated in another clinical trial and received the investigation product (including placebo) within 3 months prior to participation in the current study
-
14.
Patients who are considered ineligible for the study based on the medical judgment of the principal investigator or subinvestigator
Among the survivors above, we obtained written informed consent from 17 patients with I-TGCV. They were screened for eligibility and randomized, with 9 participants assigned to the study drug group and 8 assigned to the control group (Figure 1A).
Figure 1.
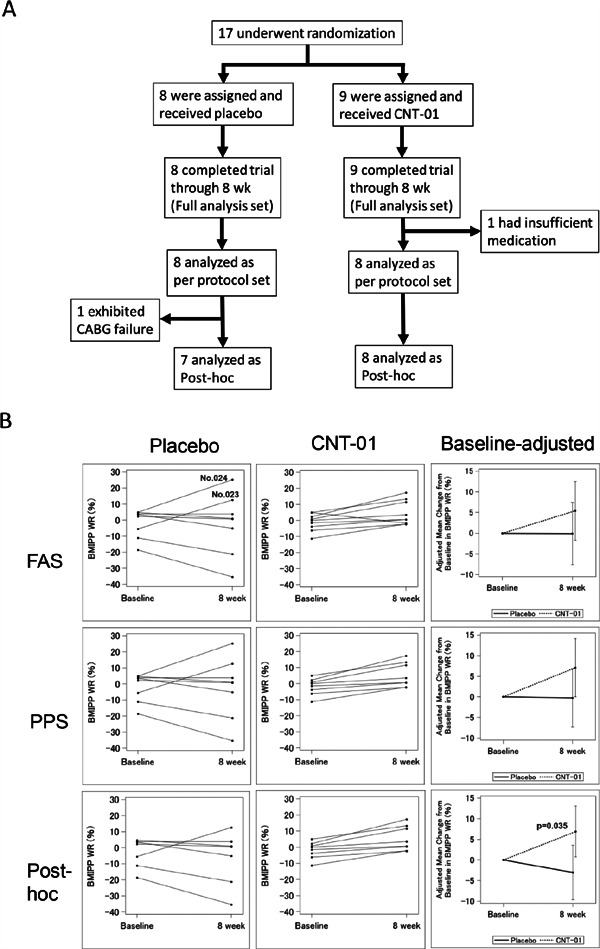
Flow chart of the clinical trial, data sets (A), and each graph of BMIPP-WR (B).
Clinical course of Cases No.023 and 024 are shown in Table 3 and in the Discussion. At the end of clinical trial, stenosis of CABG in Case No.024 was noted and excluded at posthoc analysis (Figure 1B).
BMIPP: β-methyl-p-iodophenylpentadecanoic acid, CABG: coronary artery bypass graft, FAS: full analysis set, PPS: per protocol set, WR: washout rate
The efficacy and safety analysis populations were defined as follows:
Full analysis set (FAS): A population consisting of participants enrolled in the study who received the investigational product, except participants with significant Good Clinical Practice violations.
Per protocol set (PPS): The full analysis set, but excluding participants with significant protocol violations and participants with the medication adherence rate of less than 80%. In this study, the compliance ratio was defined as the ratio of the number of days where the investigational product was taken three times daily to the planned number of days of administration.
After the observation period of the clinical trial, stenosis of coronary bypass graft was reported in one placebo participant. Because pseudonormalization of BMIPP-WR was reported in a TGCV patient with severe coronary artery stenosis (16), we decided to perform post-hoc analyses after excluding this case in the statistical analyses.
Exploratory endpoints
Endpoints were defined as any changes in the following parameters:
-
1.
BMIPP-WR
-
2.
6MWD and NYHA Class
-
3.
TGCV severity score as a patient-reported outcome, which was developed by us [10].
-
4.
Serum lipid levels and ATGL protein in peripheral leucocytes
-
5.
SF36
-
6.
Major cardiovascular events
-
7.
Frequency of sublingual nitroglycerin
-
8.
Vascular endothelial function
-
9.
Safety evaluation
BMIPP SPECT and WR calculation
In all participants, BMIPP scintigraphy was performed after overnight fasting. Only water intake was allowed by the timing of delayed images to minimize potential effects of food intake and changes in serum glucose or fatty acid levels on the uptake and WR of BMIPP. Following the protocol recommended by the Japanese Society of Nuclear Cardiology, after fasting for ≥12 h, 111 MBq of 123I-BMIPP (Cardiodine; Nihon Medi-Physics Co. Ltd., Tokyo, Japan) was intravenously injected at rest. Early and delayed images were obtained after 20 minutes and between 180 and 210 minutes, respectively. For the same participant, the allowance for the differences in the time interval between the early and delayed images at baseline and post 8-week tests was defined as within±5 min. BMIPP scintigraphy at baseline and 8-week was performed with same SPECT apparatus properly managed in the same hospital where each participant visited.
The WR was calculated as the ratio of left ventricular (LV) myocardial counts with time decay correction to early uptake as follows:
WR = [(mean LV count) early − (mean LV count) delayed × k] / (mean LV count) early × 100 (%), where k is a decay correction factor calculated by 1/0.5^(time/13.2).
In order to minimize the intra- and inter-observer variabilities, WR was computed using the myocardial SPECT analysis software Heart Risk View-S (Nihon Medi-Physics, Co. Ltd., Tokyo, Japan), which was approved by the Ministry of Health, Labour, and Welfare (MHLW) of Japan, based on the data of SPECT short-axis images (6, 10). The slices of analysis were carefully selected to determine exactly the same locations between pre- and post-intervention conditions. As mentioned above, this clinical trial was performed under double-blinded setting. The calculation of WR and data fixation was performed before the key open.
Efficacy and safety evaluation committee
A third party committee was established to evaluated the progress of the clinical trial, safety data, and, if necessary, efficacy data at an appropriate frequency, and to recommend continuation, change, or discontinuation of the clinical trial to investigators. This committee members included specialists for cardiovascular diseases, nuclear cardiology, metabolism, and statistics.
Statistical analyses
Continuous variables were summarized as mean±standard deviation, and categorical variables were presented as the number of participants. Baseline characteristics between groups were compared using two-sample t-test, Fisher's exact test, as appropriate. Between-group differences in the mean change from baseline in continuous variables were analyzed using analysis of covariance (ANCOVA) with a baseline covariate in the model, whereas Fisher's exact test was used for categorical variables. P-values of less than 0. 05 were considered to indicate significance. All analyses were performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA).
Results
Table 1 shows the baseline characteristics of each group. Consistent with previous reports (3, 6), patients in both groups showed normal serum lipid levels. Four patients in the placebo and two in the CNT-01 group had a medical history of ischemic heart disease.
Table 1. Baseline patient characteristics.
| Placebo (N=8) |
CNT-01 (N=9) |
p value | |
|---|---|---|---|
| Age (yr) | 68.6±11.9 | 70.1±14.5 | 0.82 |
| Sex (N) | 0.33 | ||
| Male | 4 | 7 | |
| Female | 4 | 2 | |
| Height (cm) | 158.4±11.7 | 162.4±8.4 | 0.43 |
| BW (kg) | 53.9±13.2 | 61.2±9.4 | 0.2 |
| Ischemic heart disease (N) | 4 | 2 | 0.33 |
| HbA1c (%) | 6.24±0.41 | 6.06±0.51 | 0.44 |
| 6MWD (m) | 248.6±105.3 | 275.1±118.1 | 0.63 |
| NYHA Class (N) | 0.32 | ||
| I | 0 | 2 | |
| II | 5 | 6 | |
| III | 3 | 1 | |
| IV | 0 | 0 | |
| BMIPP-WR (%) | −2.0±8.8 | −1.1±5.3 | 0.8 |
| TGCV severity score† | |||
| Symptom | 16.0±6.5 | 10.2±7.7 | 0.12 |
| ADL | 20.6±9.1 | 11.9±8.5 | 0.06 |
| Serum lipid (mmol/L) | |||
| TC | 4.50±1.1 | 4.21±0.83 | 0.55 |
| LDL-C | 2.54±0.65 | 2.39±0.80 | 0.68 |
| HDL-C | 1.44±0.02 | 1.37±0.27 | 0.69 |
| TG | 1.21±0.71 | 1.11±0.38 | 0.71 |
| ATGL protein mass (ng/mg of cell protein) | 3.90±3.4 | 6.39±3.9 | 0.19 |
Values are expressed as Mean±SD, or number of patients
The parameters and items were reported in Ref. 10.
6MWD: 6-min walk distance, ADL: activity of daily living, ATGL: adipose triglyceride lipase, BMIPP-WR: washout rate of β-methyl-iodopentadecanoic acid, BW: body weight, HDL-C: high-density lipoprotein-cholesterol, LDL-C: low-density lipoprotein-cholesterol, NYHA: New York Heart Association, TC: total cholesterol, TG: triglyceride, TGCV: triglyceride deposit cardiomyovasculopathy
One patient in the CNT-01 group was excluded from the FAS, because of inadequate dose status. Another patient in the placebo group (No.024 in Figure 1B) was excluded from the post-hoc analysis because of the occlusion of the coronary artery bypass during the study period. Based on the above, eight patients in the CNT-01 group and seven patients in the placebo group were included in the post-hoc analyses (Figure 1A).
In PPS, delta BMIPP-WRs were −0.26±3.28 and 7.08± 3.28% (95% confidence intervals: −7.36 to 6.84 and −0.01 to 14.18) in the placebo and CNT-01 groups, respectively. The BMIPP-WR was increased in all patients in the CNT-01 group. In the post-hoc analyses based on the ANCOVA, the change in BMIPP-WR from baseline was significant (p=0.035) between the two groups (Figure 1B) (representative SPECT images with additional follow-up are shown in Figure 2A). Clinical courses of No.024 and No.023 subjects after the clinical trial were discussed later.
Figure 2.
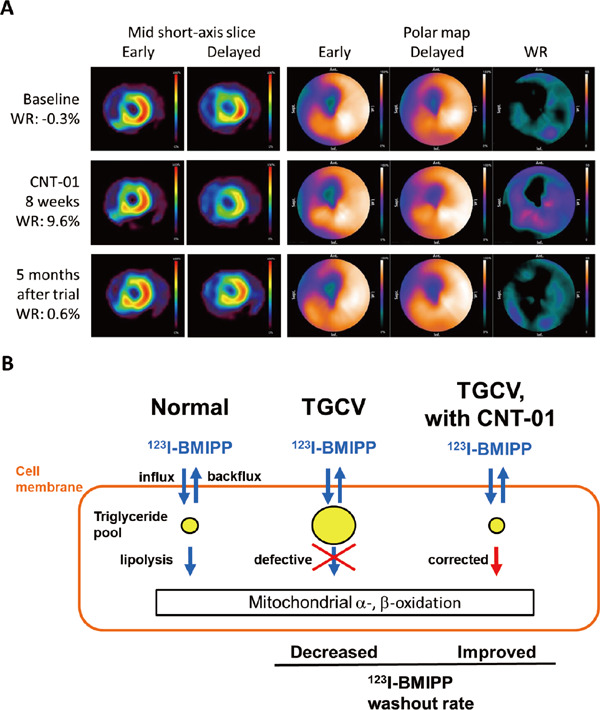
Representative images of BMIPP and Scheme of the present results.
A: Representative images of 123I-BMIPP at baseline and 8-week, and after CNT-01.
Time course of 123I-BMIPP SPECT images at baseline, at the end of 8-week CNT-01 administration, and 5 months after the end of clinical trial. The on and off effect of CNT-01 on BMIPP-WR is clearly shown.
It should be noted that the administration duration in this clinical trial was 8 weeks; in the current legislation in Japan, the compassionate use of investigation product is not allowed at the end of early phase clinical trial like the present study.
Short-axis images of the mid-portion of the LV (left), and polar map displays (right) are shown.
B: A scheme of 123I-BMIPP-WR and myocardial lipolysis representing the results of the present study.
Left: in the normal condition, the injected 123I-BMIPP is taken up via the CD36 receptor. The majority of them are reesterified and incorporated into the TG pool. The remaining, un-esterified 123I-BMIPP is immediately backfluxed into the blood. 123I-BMIPP in the TG pool is hydrolyzed by intracellular lipases including adipose triglyceride lipase. The hydrolyzed 123I-BMIPP is incorporated into the carnitine shuttle, where it is used by the mitochondria in α- and β-oxidation.
Middle: as intracellular lipolysis is defective in patients with TGCV, 123I-BMIPP is retained in the TG pool, which can be measured as defective BMIPP-WR.
Right: CNT-01 facilitates myocardial lipolysis and increases 123I-BMIPP-WR.
BMIPP: β-methyl-p-iodophenylpentadecanoic acid, LV: left ventricle, SPECT: single-photon emission computerized tomography, WR: washout rate
As shown in Table 2, 6MWDs, ATGL protein mass, NYHA class, and TGCV severity score were not significantly changed in either group, indicating that no apparent clinical benefits for patients could be observed during the 8-week observation period.
Table 2. Changes in 6MWD, ATGL protein, NYHA class, and TGCV severity score.
| Endpoint | Placebo | CNT-01 | |
|---|---|---|---|
| 6MWD (m)† | FAS | 34.3 (−6.0 to 74.7) | 34.1 (−3.9 to 72.1) |
| PPS | 34.3 (−8.0 to 76.5) | 35.9 (−6.3 to 78.2) | |
| ATGL protein mass (ng/mg of cell protein)† | FAS | 3.00 (−1.12 to 7.12) | 3.55 (−0.32 to 7.4) |
| PPS | 2.88 (−1.30 to 7.06) | 4.19 (0.01 to 8.37) | |
| NYHA class reduction (N)‡ | FAS | 1 | 0 |
| TGCV severity score, symptom (SUM)§ | FAS | −0.75 (−3.38 to 1.88) | −2.78 (−4.61 to −0.94) |
| TGCV severity score, ADL (SUM)§ | FAS | −0.88 (−3.30 to 1.55) | −2.67 (−6.47 to 1.14) |
Adjusted mean change from baseline (95% confidence intervals)
Number of patients with more than 1 class reduction
Mean change from baseline (95% confidence intervals)
6MWD: 6-min walk distance, ADL: activity of daily living, ATGL: adipose triglyceride lipase, FAS: full analysis set, NYHA: New York Heart Association, PPS: per protocol set, TGCV: triglyceride deposit cardiomyovasculopathy
Body weight, plasma glucose, serum lipids, and other endpoints were not changed in either group (data not shown).
Discussion
We successfully finished the first randomized placebo-controlled clinical trial for this orphan disease. Among the exploratory endpoints, we observed the apparent increase in BMIPP-WR (Figure 1B), which was consistent with preclinical data in the TGCV model mice (15) showing the improved myocardial lipolysis. Based on the data obtained, we have achieved a consensus with PMDA to proceed with the development of CNT-01 and MHLW designated CNT-01 as a SAKIGAKE pioneering drug in 2020. The development of CNT-01 was succeeded by a pharmaceutical company in Japan and another clinical trial with a longer observation period has been started to elucidate whether CNT-01 exerts beneficial clinical effects and can improve prognosis (jRCT 2051210177).
Thus far, the clinical significance of myocardial 123I-BMIPP scintigraphy has reportedly focused on its uptake only in the early image as follows: 1) the uptake of BMIPP is defective in patients with CD36 genetic deficiency, indicating that this fatty acid transporter is responsible for the myocardial uptake of BMIPP (17); 2) reduced uptake after severe ischemic condition, called “ischemic memory,” reflects prolonged damage of myocardial LCFA metabolism even after the normalization of perfusion (18). The mismatch between perfusion and fatty acid metabolism in the myocardium indicates the usefulness of BMIPP to detect myocardial ischemia and viable myocardium for revascularization in patients with acute coronary syndrome.
In contrast to this, previous kinetic studies in canine models (19, 20) have demonstrated that 1) 80%–90% of 123I-BMIPP taken up by cardiomyocytes is re-esterified into the LCTG pool, and non-esterified free BMIPP is immediately back fluxed into the blood; 2) BMIPP-WR was influenced by various experimental conditions including coronary artery ligation, pacing, and chemical modification; and 3) intracellular BMIPP is eventually alpha- and beta-oxidized in the mitochondria. In addition to the above animal studies, our series of studies in patients with TGCV, including the present randomized trial, clearly demonstrated that BMIPP-WR reflects myocardial lipolysis, proving the clinical significance of the measurement of BMIPP-WR.
The present study has the following limitations: First, a possible relationship between 123I-BMIPP kinetics and coronary events should be noted. Clinical studies conducted before the discovery of TGCV showed that an ischemic condition might increase the BMIPP-WR in patients with CAD. Our TGCV study group has observed a similar phenomenon in patients with TGCV called pseudonormalization of BMIPP-WR (16). As listed in Table 3, five patients with TGCV including two participants in the present clinical trial exhibited the pseudonormalization associated with coronary events. Even though the mechanism underlying the pseudonormalization remains unknown, it is at least necessary that, in the next phase clinical trial, patients with major cardiac events during the observation period should be excluded from the statistical set for evaluating 123I-BMIPP-WR; Second, it is of interest and required to investigate clinical implications of BMIPP scintigraphy in TGCV patients with and without CAD and the effect of severity of coronary atherosclerotic lesions on BMIPP imaging. Third, the molecular mechanism underlying the dynamics of 123I-BMIPP in cardiomyocytes still needs to be elucidated. In addition to basic science studies targeting recently identified proteins and enzymes for intracellular TG metabolism, detailed compartment analysis including TG pool and mitochondria would be of interest for understanding the pathophysiology of TGCV; Forth, patients with primary TGCV were not included in this trial because of the ultrararity of the disease. As the preclinical proof of concept with CNT-01 was obtained in the ATGL-knockout mice (15), CNT-01 warrants being tested for primary TGCV of which cause is the genetic ATGL deficiency (1, 3).
Table 3. Patients with idiopathic TGCV with pseudonormalization of BMIPP-WR.
| Age | Sex | Condition at pseudonormalization |
BMIPP-WR (%) | |||
|---|---|---|---|---|---|---|
| At diagnosis | Pseudonormalization | After treatment | ||||
| Case 1 | 81 | F | CABG failure | 4.1 | 25.2 | 8.9 |
| Case 2 | 75 | M | Frequentspast ic angina | −5.5 | 12.6 | 7.0 |
| Case 3 | 72 | F | Subtotal occlusion of LAD | ND | 24.3 | 5.0 |
| Case 4 | 43 | F | AMI (RCA #4) | 2.8 | 9.4 | 4.1 |
| Case 5 | 40 | M | CABG failure | 3.1 | 21.5 | ND |
Cases 1 and 2 are No. 024 and No. 023 paticipants, respectively, in the placebo group of the phase lla trial (please see Figure 1B).
Case 3 was reported previously by the Japan TGCV study group in the reference 16.
The principal investigator has obtained the information of cases 4–5 from the Japan TGCV study group after the phase lla trial was finished.
The pseudonormalization disappeared in Cases 1–4 after the revasculization or optimized medical therapy.
AMI: acute myocardial infarction, BMIPP: beta-methyliodophenylpentadecanoic acid, CABG: coronary artery bypass graft, LAD: left anterior descending branch, ND: not done, RCA: right coronary artery, TGCV: triglyceride deposit cardiomyovasculopathy, WR: washout rate
Conclusions
Following our previous reports showing defective 123I-BMIPP-WR in TGCV, we demonstrated that 123I-BMIPP-WR was increased by the administration of CNT-01 reflecting the improvement of lipolysis in the randomized controlled setting (Figure 2B). This study provided a clinical proof of the mechanism by which CNT-01 improves myocardial lipolysis in TGCV.
Acknowledgments
KH is the principal investigator for the Japan TGCV study group. KH and HM initiated and designed the study. KH and HM wrote the manuscript. HM, YN, KS, HY, CA, SF, and TA recruited the patients and collected data. MN and AN manufactured the academia-initiated drug, CNT-01, for the clinical trial. AM and TY evaluated the data and performed the statistical analysis. DN managed the project. KN supervised SPECT analysis. All authors critically contributed to the drafting manuscript and discussion, and approved the final manuscript.
Sources of funding
This work was supported by research grants for rare diseases from the Japan Agency of Medical Research and Development (AMED) (18ek0109335h001) and the Ministry of Health, Labour, and Welfare, Japan (20FC1008).
Conflicts of interest
Hirano holds the position of Joint Research Chair in collaboration with TOA EIYO LTD since February 2021 and medical adviser of TOA EIYO LTD since December 2021. Hirano received a research grant from Nihon Medi-Physics Co. Ltd. Nakajma belongs to the endowed department partly funded by Nihon Medi-Physics Co. Ltd. Others have no conflictt o declare.
Abbreviations
- ANCOVA
analysis of covariance
- ATGL
adipose triglyceride lipase
- BMIPP
β-methyl-p-iodophenylpentadecanoic acid
- FAS
full analysis set
- I-TGCV
idiopathic TGCV
- LCFA
long-chain fatty acid
- LCTG
long-chain triglyceride
- PMDA
Pharmaceuticals and Medical Devices Agency
- PPS
per protocol set
- RCT
randomized controlled trial
- SPECT
single photon emission computed tomography
- TGCV
triglyceride deposit cardiomyovasculopathy
- WR
washout rate
References
- 1. Hirano K, Ikeda Y, Zaima N, Sakata Y, Matsumiya G. Triglyceride depositcardiomyovasculopat hy. N Engl J Med 2008; 359: 2396-8. [DOI] [PubMed] [Google Scholar]
- 2. Hirano K. A novel clinical entity: triglyceride deposit cardiomyovasculopathy. J Atheroscler Thromb 2009; 16: 702-5. [DOI] [PubMed] [Google Scholar]
- 3. Li M, Hirano KI, Ikeda Y, Higashi M, Hashimoto C, Zhang B, etal. Triglyceride depositcardiomyovasculopat hy: a rare cardiovascular disorder. OrphanetJ Rare Dis 2019; 14: 134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Neubauer S. The failing heart—an engine outof fuel. N Engl J Med 2007; 356: 1140-51. [DOI] [PubMed] [Google Scholar]
- 5. Young SG, Zechner R. Biochemistry and pathophysiology of intravascular and intracellular lipolysis. Genes Dev 2013; 27: 459-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Miyauchi H, Iimori T, Hoshi K, Ohyama M, Hirano K, Kobayashi Y. Correlation perspectives for the diagnosis of idiopathic triglyceride deposit cardiomyovasculopathy. Ann Nucl Cardiol 2020; 6: 33-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Goodman MM, Kirsch G, Knapp FF Jr. Synthesis and evaluation of radioiodinated terminal p-iodophenyl-substituted α- and β-methyl-branched fatty acids. J Med Chem 1984; 27: 390-7. [DOI] [PubMed] [Google Scholar]
- 8. Tamaki N, Yoshinaga K. Novel iodinated tracers, MIBG and BMIPP, for nuclear cardiology. J Nucl Cardiol 2011; 18: 135-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Hirano K, Ikeda Y, Sugimura K, Sakata Y. Cardiomyocyte steatosis and defective washout of iodine-123-β-methyl iodophenyl-pentadecanoic acid in genetic deficiency of adipose triglyceride lipase. Eur Heart J 2015; 36: 580. [DOI] [PubMed] [Google Scholar]
- 10. Miyauchi H, Hashimoto C, Ikeda Y, Li M, Nakano Y, Kozawa J, et al. Diagnostic criteria and severity score for triglyceride depositcardiomyovasculopat hy. Ann Nucl Cardiol 2018; 4: 94-100. [Google Scholar]
- 11. Nakajima K. Triglyceride depositcardiomyovasculopat hy: how to recognize a new disease entity. Heart 2021; 107: 93-5. [DOI] [PubMed] [Google Scholar]
- 12. Nakano Y, Suzuki M, Hirano KI, Ando H, Takashima H, Takahashi H, et al. Association of triglyceride deposit cardiomyovasculopathy with drug-eluting stent restenosis among patients with diabetes. JAMA Netw Open 2020; 3: e2012583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Onishi T, Nakano Y, Hirano KI, Nagasawa Y, Niwa T, Tajima A, et al. Prevalence and clinical outcomes of triglyceride deposit cardiomyovasculopathy among hemodialysis patients. Heart2021; 107: 127-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Aoshima C, Fujimoto S, Kudo A, Kawaguchi YO, Takamura K, Matsue Y, et al. Clinical significance of 123I-BMIPP washout rate in patients with uncertain chronic heart failure. Eur J Nucl Med Mol Imaging 2022; 49: 3129-39. [DOI] [PubMed] [Google Scholar]
- 15. Suzuki A, Yamaguchi S, Li M, Hara Y, Miyauchi H, Ikeda Y, etal. Tricaprin rescues myocardial abnormality in a mouse model of triglyceride deposit cardiomyovasculopathy. J Oleo Sci 2018; 67: 983-9. [DOI] [PubMed] [Google Scholar]
- 16. Hirano K, Higashi M, Miyauchi H, Takagi A, Ikeda Y, Nakano Y, etal. Increased washoutof 123I-BMIPP in triglyceride deposit cardiomyovasculopathy (TGCV) with severe coronary stenosis: a pitfall of diagnosis for TGCV. Ann Nucl Cardiol 2019; 5: 47-9. [Google Scholar]
- 17. Tanaka T, Okamoto F, Sohmiya K, Kawamura K. Lack of myocardial iodine-123 15-(p-iodiphenyl) -3-R, S-methylpentadecanoic acid (BMIPP) uptake and CD36 abnormality—CD36 deficiency and hypertrophic cardiomyopathy. Jpn Circ J 1997; 61: 724-5. [DOI] [PubMed] [Google Scholar]
- 18. Dilsizian V, Bateman TM, Bergmann SR, Des Prez R, Magram MY, Goodbody AE, et al. Metabolic imaging with beta-methyl-p-[123I]-iodophenyl-pentadecanoic acid identifies ischemic memory after demand ischemia. Circulation 2005; 112: 2169-74. [DOI] [PubMed] [Google Scholar]
- 19. Hosokawa R, Nohara R, Fujibayashi Y, Okuda K, Ogino M, Hata T, et al. Myocardial kinetics of iodine-123-BMIPP in canine myocardium after regional ischemia and reperfusion: implications for clinical SPECT. J Nucl Med 1997; 38: 1857-63. [PubMed] [Google Scholar]
- 20. Fujibayashi Y, Nohara R, Hosokawa R, Okuda K, Yonekura Y, Tamaki N, et al. Metabolism and kinetics of iodine-123-BMIPP in canine myocardium. J Nucl Med 1996; 37: 757-61. [PubMed] [Google Scholar]