

Abstract
OBJECTIVES:
This laboratory study examined gender differences in upper extremity postures, applied forces, and muscle activity when a computer workstation was adjusted to individual anthropometry according to current guidelines.
METHODS:
Fifteen men and fifteen women completed five standardized computer tasks: touch-typing, completing a form, editing text, sorting and resizing graphical objects and navigating intranet pages. Subjects worked at a height-adjustable workstation with the keyboard on top of the work surface and the mouse to the right. Subjects repeated the text editing task with the mouse in two other locations: a “high” mouse position, which simulated using a keyboard drawer with the mouse on the primary work surface, and “central” mouse position with the mouse between the keyboard and the body, centered with the body’s center line. Surface electromyography measured muscle activity; electrogoniometric and magnetic motion analysis system measured wrist, forearm and upper arm postures; load-cells measured typing forces; and a force-sensing mouse measured applied forces.
RESULTS:
Relative forces applied to the keyboard, normalized muscle activity of two forearm muscles, range of motion for the wrist and shoulder joints and external rotation of the shoulder were higher for women (p<0.05). When subjects were dichotomized instead by anthropometry (either large/small shoulder width or arm length), the differences in forces, muscle activity of the shoulder and wrist posture and shoulder posture became more pronounced with smaller subjects having higher values. Postural differences between the genders increased in the high mouse position and decreased in the center mouse location.
CONCLUSIONS:
When a work station is adjusted per current guidelines differences in upper extremity force, muscle activity and postural factors still exist between genders. However, these were often stronger when subjects were grouped by anthropometry suggesting that perhaps the computer input devices themselves should be scaled to be more in proportion with the stature and strength of the user.
INTRODUCTION
Computer work has been associated with musculoskeletal disorders of the upper extremity (e.g. Punnett & Bergqvist, 1997; Gerr et al., 2002). The prevalence of upper extremity disorders related to computer work is higher among females (Punnett and Bergqvist, 1999; Gerr et al., 2002; Lassen et al., 2005). A recent review (Treaster and Burr, 2004) reported that the higher prevalence of MSD in females exists even controlling for work-factors. However, Punnett and Herbert’s review (1999) of the epidemiologic literature showed that, both in the general population and in workplace settings, the putative excess risk of upper extremity disorders among women was not impressive when differences in occupation and job demands were taken into account. Only a limited number of studies permitted such analysis, and even fewer examined potential differences in exposure between men and women within job titles, across similar tasks, and taking into account anthropometric differences.
Musculoskeletal disorders can occur when there is a mismatch between a worker’s capabilities and the job design. For example, Smet and Ghyselen (1998) found that musicians with smaller hands had more frequent musculoskeletal symptoms and overuse syndromes. Sauter et al (1991) reported that the relative height of the keyboard is associated with neck and shoulder disorders. Interventions thus should be aimed at matching the workstation with the anthropometry of the worker (OSHA, 1997). The relationship between gender and anthropometric dimensions is significant to note, as women, on average, have smaller anthropometric dimensions compared to men (Jurgens et al. 1990; National Health Survey, 1985). Hence, failure to implement ergonomic principles may have greater consequences for people with smaller anthropometry.
A small number of laboratory studies have examined gender and anthropometric differences in upper extremity biomechanics. Wahlstrom et al. (2000) reported that women used higher relative forces (percentage of maximum voluntary contraction) and more non-neutral postures than men when operating a computer mouse during a text selection and deletion task. Karlqvist and Bernmark (1998) examined mouse tasks and reported more extreme postures in female computer operators as well as in those with narrower shoulders and shorter height, suggesting that the higher exposures of female subjects resulted at least in part from their smaller stature requiring greater extremes of reach. These studies, however, have not examined multiple factors (force, muscle activity, wrist and shoulder postures) during tasks that span a wide range computer tasks (Dennerlein and Johnson, 2006a).
In addition to general recommendations for workstation setup, the positioning of the mouse is often utilized as an intervention for musculoskeletal symptoms. Dennerlein and Johnson (2006b) studied the biomechanical implications of four different mouse positions; the poorly positioned mouse yielded the least neutral posture and the highest level of muscle activity. Others have also studied alternative mouse positions, and the results have consistently shown that locating the pointing device close(r) to the midline of the body provides more neutral wrist and shoulder postures and reduces some muscle activity levels (Harvey and Peper, 1997; Sommerich et al., 2002; Cook and Kothiyal, 1998).
Our goal was to quantify differences in biomechanical measures (force, muscle activity and posture) between men and women in a controlled laboratory setting where the participants completed the same set of simulated work tasks at a workstation adjusted to fit each individual, with the mouse positioned to the right of the keyboard. This study tested the hypotheses that women utilize greater forces (absolute and relative), muscle activity and non-neutral wrist and shoulder postures. This study also sought to determine whether there was any correlation between these biomechanical parameters and the individuals’ anthropometry. The study hypothesized that smaller anthropometry leads to greater forces, muscle activities and non-neutral postures. Finally, this study also examined how these differences between genders were affected by workstation configuration.
METHODS
Subjects
Thirty subjects (15 males, 15 females) ranging in age from 21 to 39 years (mean = 26.9 years, standard deviation = 4.9 years), all of whom touch-typed at 40 words per minute or higher, were recruited through a temporary employment agency. Based on a typing test performed before the experiment, the net typing speed of the subjects ranged from 41 to 77 words per minute. Except for BMI, all anthropometric measurements were greater for men compared to women (Table 1). The Harvard School of Public Health Human Subjects Committee approved all protocols and consent forms.
Table 1:
Selected subject anthropometry and strength measures. Mean values (and standard deviations) across subjects within the gender groups are presented. Bolded values indicate p-values < 0.05 for student t-tests between genders.
| Parameter | Women (n=15) | Men (n=15) | p-value* |
|---|---|---|---|
| Height (cm) | 163 (5) | 179 (7) | <0.001 |
| Weight (Kg) | 59 (7) | 79 (12) | 0.001 |
| BMI (Kg/m2) | 22.3 (2.1) | 24.7 (3.5) | 0.03 |
| Shoulder width (cm) | 39.0 (2.5) | 44.4 (1.5) | <0.001 |
| Arm Length (cm) | 55.6 (2.7) | 60.7 (4.0) | <0.001 |
| Hand length (cm) | 17.5 (0.7) | 19.1 (1.5) | <0.001 |
| Index finger maximum voluntary | 52 (14) | 37 (7) | <0.001 |
| contraction (N) |
p-values from student t-tests
Experimental Protocol
The experiment consisted of subjects completing a series of five standardized computer tasks while seated at an adjustable workstation. The five different tasks were: typing (Type), text editing (Edit), completing a web based form (Form), a graphics manipulation task (Graphics), and web page browsing (Web). Each task designed to take approximately 5 minutes to complete and the five task required different combinations of mouse and keyboard interactions (Dennerlein and Johnson 2006a).
The workstation consisted of an adjustable chair without arms, an adjustable work surface for the keyboard and mouse, and a flat-panel monitor on an adjustable monitor stand. The chair height was adjusted such that with the participant’s feet flat on the ground their thighs were parallel to the ground. The height of the table was adjusted such that the surface was level with the resting elbow height for each individual while sitting for all experimental conditions. The keyboard was placed on the table surface near the edge of the workstation with the alphanumeric portion of the keyboard centered with the body’s centerline. Forearm and wrist supports were not provided. For all of the tasks the mouse was positioned to the right of the keyboard in a standard configuration.
Subjects repeated the text-editing task with the mouse positioned in two other locations. One location was with the mouse beyond the keyboard and elevated 5 cm above the surface of the keyboard (“high mouse”). This high mouse position emulated a workstation with a keyboard tray vertically adjusted to the individuals’ anthropometry with enough space for the keyboard only and the mouse is placed away from the user on the desk. The other location was with the keyboard pushed back 25 cm from the edge of the table and the mouse positioned between the keyboard and the user (“center mouse”). The order of the conditions for each subject was randomized.
Apparatus and Measurements
Strain gauge based sensors located under the keyboard and within the mouse measured the applied forces to the input devices during the tasks. The keyboard force sensing system consisted of a rectangular aluminum plate 3.18 mm thick with four 22 Newton load cells (model ELFS-B3–5L, Entran Devices Inc., Fairfield, NJ) mounted to the underside of the plate. The platform had a force sensitivity of 0.03 Newton’s (N) and could measure compressive forces up to 88 N. The mouse contained five miniature load cells (Model AIFP-PJ; Microstrain; Winooski, VT) with four load cells embedded between two stainless steel plates on the side of the mouse and one under the button providing a measure of thumb grip and finger forces, respectively (Johnson et al., 2000). Calibration of the mouse indicated the miniature side force sensing system had a sensitivity of 0.01 N, was linear (r = 0.996) with applied forces, and was accurate in measuring forces over the whole area of the side of the mouse. The side force-sensing system was also repeatable and had an average measurement error of 6.5% when 0.5 Newton was applied twenty times. The button force sensing system was linear (r = 0.983) with applied forces and moderately accurate in measuring forces over a 1.5 cm x 1.5 cm area (average absolute force measurement error over the area was 18.0%). Button force measurement was repeatable with an average error of 3.4% while measuring 0.5 Newton applied to the same location twenty times. The force signals were digitally recorded onto a personal computer at 200 samples per second and then digitally low-pass filtered at 20 Hz to remove high frequency noise and platform resonance (~100 Hz).
To normalize the force measurements as the percentage of a subject’s maximum capability, Maximum Voluntary Isometric Contractions (MVCs) were collected. To normalize the force results across subjects, three, five-second MVCs were collected to obtain the maximum forces the subjects could apply to the keyboard and mouse. For typing, subjects pressed as hard as they could on the J key of the keyboard with their index finger. For the mouse, subjects pressed as hard as they could with their index finger against a force transducer inserted into the mouse button and squeezed a force transducer mounted in the side of the mouse between the thumb and fingers, as described by Johnson et al. (2000). Participants rested for one minute between contractions. The force signals from these MVCs were smoothed with a one-second moving window average and the force MVC value was the highest amplitude from these three signals.
The electromyographic activity from four muscles of the right forearm and three muscles of the right shoulder were recorded during the tasks. The forearm muscles monitored were the flexor carpi radialis (FCR), the flexor carpi ulnaris (FCU), the extensor carpi ulnaris (ECU) and the extensor carpi radialis (ECR). The three shoulder muscles monitored were the anterior deltoid (AD), the medial deltoid (MD) and the upper trapezius (Trap) muscles. Surface electrodes (DE-2.1 Single Differential Electrode, Delsys, Boston, MA) were placed on top of the muscle bellies in accordance with the anatomical locations as identified by Perotto (1994). Placements were validated through palpation and signal response to isometric test contractions.
After amplification with a bandwidth of 20 to 450 Hz (Bagnoli-Eight Amplifier, Delsys, Boston, MA), the raw EMG signals were recorded onto a personal computer at 1000 samples per second. The EMG amplitude was represented by a root mean square (RMS) value calculated over a 0.2 second moving window. To normalize the EMG results across subjects, three, five-second maximum voluntary isometric contractions (MVCs) were collected for each muscle. The EMG MVC value was the highest amplitude from the three EMG signals for the identified muscle. For the MVCs, the experimenter manually restrained the movement of the joint that the muscle of interest articulates. For the four forearm muscles that articulate the wrist, the wrist was restrained and the subjects were instructed to push in the direction that each of the four muscles act as defined by Buchanan et al. (1993). For the anterior deltoid the experimenter resisted shoulder flexion and for the medial deltoid shoulder abduction was resisted. For the trapezius muscle, subjects attempted to lift/shrug their shoulders with the direction of the resistance being applied vertically downward at the acromion. For these exertions of the shoulder muscle the upper arm was near the neutral posture, vertically aligned with the torso.
The participants wore a two-channel, glove-based electrogoniometry system (Wristsystem, Greenleaf Medical; Palo Alto, CA) that measured wrist posture during the tasks from both the left and the right hand. The system measured wrist flexion and extension and ulnar and radial wrist deviation. The system has a resolution of 0.1 degrees and 2 degree accuracy over a ±90 degree range. It was calibrated using a wrist jig in accordance with the methods described in Jonsson and Johnson (2001). Postures were recorded continuously by a data logger at 20 samples per second during the tasks. Using the same methods of Jonsson and Johnson et al (2001), neutral radial/ulnar deviation was defined as the position where the third metacarpal was in alignment with the long axis of the forearm and neutral flexion/extension where the plane formed by the dorsal surface of the hand was in line with the plane formed by the dorsal surface of the forearm (Greene and Heckman, 1994).
For the first 15 participants, the right upper arm postural data were collected using a three-axis orientation sensor (Model 3DM; Microstrain, Inc.; Winooski, VT) placed on the lateral midpoint of the right humerus, defined as halfway between the lateral epicondyle and the acromiom process. The 3DM measured abduction (±70°) and flexion (±180°) using inclinometers, and rotation (±180) using a magnetometer. For the last 15 participants, an electro-magnetic motion analysis system (MiniBird, Ascension Technology, Burlington, VT) measured the orientation of the upper arm using two sensors, one placed on the forearm and one on the upper arm, midway on the humerus. The second system was introduced due to hardware failure. For both systems data were recorded through the serial port into a personal computer at 10 samples per second. The neutral position for the upper arm was defined as seated, shoulders relaxed with the elbows at the sides of the body and the palms of the hands resting on the subjects’ own thighs.
Upper extremity anthropometric measurements were taken using as the shortest distance between anatomical landmarks (Pheasant and Haslegrave, 2005). These measurements included shoulder width (distance across acromioclavicular joints), shoulder-elbow length (measured as acromioclavicular joint to olecranon process), elbow-wrist (distance from olecranon process to ulnar styloid), palm length (ulnar styloid to third metacarpophalangeal joint) and finger length (third metacarpophalangeal joint to the tip of the third digit). Arm length was calculated by adding the lengths of the upper arm and lower arm. Subjects self-reported their height and their weight.
Data and Statistical Analysis
Summary statistics for muscle activity and upper extremity postures included mean and standard deviation as well as the 10th, 50th, and 90th percentiles of signal amplitude (Jonsson, 1988). For the posture measures, the difference between the 90th and the 10th percentile provides a measure of the range of motion and the 50th percentile provides a measure of the median postural by definition These summary statistics were calculated for each subject and each task.
The mouse and keyboard force data were parsed into grip and typing episodes respectively. Grip episodes were defined when the force applied to the side of the mouse or the keyboard exceeded minimum and standard deviation force thresholds. A grip episode on the mouse was defined as any period where force applied to the side of the mouse was above 0.08 Newtons and a 100ms moving window of the force standard deviation exceeded 0.025 Newtons. For the keyboard force, the standard deviation of the force signal over a 150 millisecond second window had to be above a 0.45 Newton threshold, indicating dynamic activity; the maximum force for the episode had to exceed the activation force for the keyboard (0.65 N) and have a duration of over 150 milliseconds. Once an episode was identified, the average force and peak forces (95th percentile) as well as the duration of the episode were calculated. These force parameters were then averaged across episodes and the five tasks to provide a summary measure for each subject.
To test the hypothesis that women utilize greater forces (absolute and relative), muscle activity and non-neutral wrist and shoulder postures, repeated measures analysis of variance (ANOVA) models were fitted to each summary statistic (dependent parameter). The independent parameters in the model were gender, task and their interaction with subject set as a random variable and gender nested within the subject random effects variable. Post-hoc single sided t-tests were then used to compare values between the gender. To explore if anthropometry was also a factor, the subjects were categorized into two groups of 15 each, small and large. This was done twice, once based on shoulder width and once on arm length. The repeated measures model and post-hoc comparisons as described above were utilize with the anthropometry variable replacing the gender variable. Since the post-hoc t-test p-values and the p-value for the gender factor were the same, p-values for the post-hoc t-tests only are presented. Pearson correlation coefficients quantified the relationship between the subjects’ summary statistics and their anthropometry measures. To test the effects of different mouse positions the summary statistics were calculated within the text-edit task for the three mouse positions (standard, high and center) and compared between genders via two-sample t-test stratified by position. To test differences between genders across different workstation configuration, a repeated measures ANOVA was also fitted, with gender, position and their interaction as independent variables. Gender was nested within subject. Post-hoc single sided t-tests stratified within each workstation configuration tested if women had higher summary statistics compared to men. Statistical significance was defined as alpha ≤ 0.05.
RESULTS
While there was little to no difference between women and men in the absolute forces applied to keyboard and to the mouse during these five tasks, the normalized typing forces were consistently higher for women than for men (Table 2 and Table 3). The normalized median and 90th percentile keyboard forces were significantly higher (57% and 29%, respectively) for women than for men. The normalized mean forces applied to the button and to the side of the mouse were 36% and 24% higher, respectively, for women. Due to a mechanical and electrical failure of the mouse sensor during the experiment, mouse grip and button force data was collected successfully on only 6 women and 11 men; hence reducing our power to test for statistically significant differences in mouse forces.
Table 2:
Force applied to the keyboard during the text typing task. Mean values (standard deviations) across subjects within the gender groups are presented. Bolded values indicate p-values < 0.05 for student t-tests between genders.
| Parameter | Women (n=15) | Men (n=15) | p-value* |
|---|---|---|---|
| Median force (N) | 0.8 (0.4) | 0.7 (0.4) | 0.36 |
| 90th percentile force (N) | 2.1 (0.5) | 2.3 (0.4) | 0.11 |
| Median normalized force (%MVC) | 2.3 (1.5) | 1.5 (0.7) | 0.03 |
| 90th percentile normalized force (% MVC) | 6.1 (2.5) | 4.7 (1.3) | 0.03 |
p-values from student t-tests
Table 3:
Force applied to the mouse during all five tasks. Mean values (standard deviations) across subjects within the gender groups are presented.
| Parameter | Women (n = 6)** | Men (n = 11)** | p-value* |
|---|---|---|---|
| Mean side force (N) | 0.9 (0.4) | 1.0 (0.5) | 0.42 |
| Mean peak side force (N) | 2.1 (0.8) | 2.0 (0.8) | 0.41 |
| Mean button peak force (N) | 1.0 (0.2) | 1.0 (0.3) | 0.39 |
| Mean normalized side force (% MVC) | 1.3 (0.5) | 0.9 (0.4) | 0.06 |
| Mean normalized peak side force (% MVC) | 2.6 (1.1) | 1.9 (0.8) | 0.05 |
| Mean normalized button peak force (% MVC) | 2.8 (0.9) | 2.1 (1.1) | 0.07 |
p-values from post-hoc single sided student t-tests
due to hardware failure forces applied to the mouse were observed on only 6 women and 11 men.
Women had higher muscle activity for all muscles except the medial deltoid (Figure 1). In the forearm these greater values were statistically significant for the 10th and 50th percentile for the flexor carpi radialis (FCR) and the 50th and 90th for the extensor carpi radialis (ECR). No shoulder EMG values were significantly higher for women compared to men.
Figure 1.
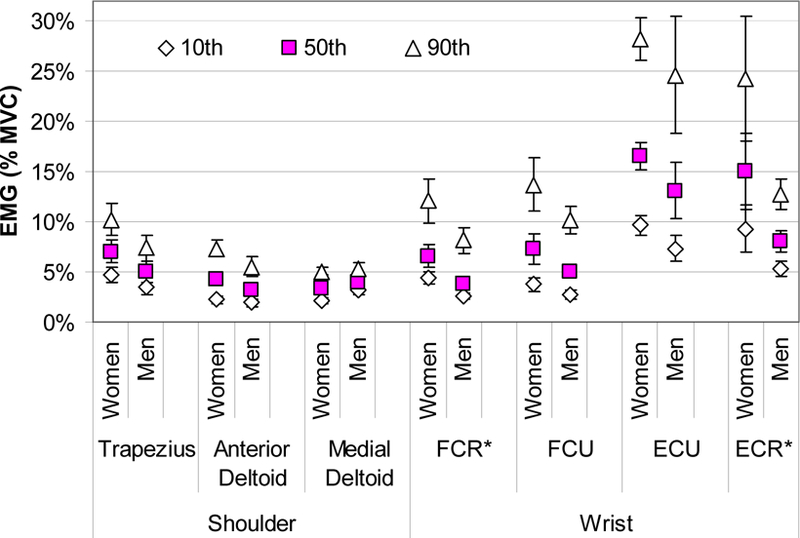
Average shoulder and forearm EMG amplitudes (10th (◊), 50th (□) and 90th (∆) percentile) grouped by gender for the standard workstation configuration. The error bars represent the standard error across subjects within the gender group. Females tended to have higher muscle activity in all but the medial deltoid muscle. Student t-tests compared the values between the subjects grouped by gender with significance found for the 10th and 50th percentile for FCR and the 50th and 90th percentile for the ECR.
Women adopted shoulder postures that were slightly less neutral than men (Figure 2). External rotation of the shoulder was significantly greater in woman than compared to men across all measures. The range of motion was also significantly greater for shoulder flexion for women compared to men by 5 degrees. While wrist extension was 5 degrees greater for men, the range of motion in wrist flexion/extension was significantly greater in the women and exceeded the men’s by 3 degrees. No significant differences were observed in wrist radial/ulnar deviation.
Figure 2.
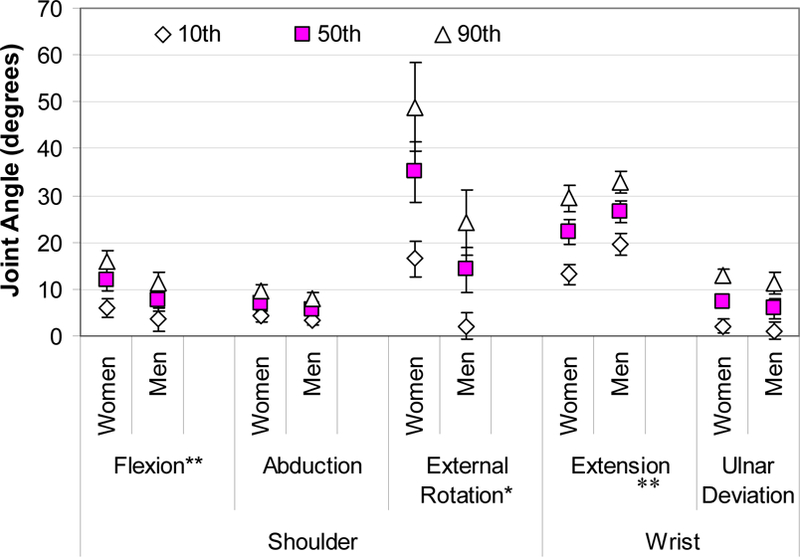
Average shoulder and wrist postures (10th (◊), 50th (□) and 90th (∆) percentile) grouped by genders for the standard workstation configuration. The error bars represent the standard error across subjects. For the shoulder and wrist ulnar deviation, women postures tended to be further from neutral than male postures Student t-tests compared the values between the subjects grouped by gender. (* p < 0.05 for the 10th, 50th and 90th percentiles, and ** p <0.05 for the range of motion being greater for women than for men).
Most anthropometric measures were negatively correlated with force, muscle activity and postural measurements (Table 4, Figure 3). Shoulder width and arm length had the highest number of significant correlations with the biomechanical parameters. Both were significantly correlated with normalized typing force, the range of motion in the wrist (both extension and ulnar deviation) and shoulder flexion and external rotation and with the amount of external rotation.
Table 4:
Correlation coefficients (and p values) between selected biomechanical and anthropometric parameters. Bolded values indicate p-values < 0.05
| Biomechanical Parameter | Gender* | Height | BMI | Shoulder Width | Arm Length | Hand Length |
|---|---|---|---|---|---|---|
| Median Typing Force (N) | −0.08 (0.69) | −0.19 (0.32) | −0.12 (0.52) | −0.20 (0.30) | −0.18 (0.34) | |
| Normalized Median Typing Force | X | −0.32 (0.09) | −0.34 (0.07) | −0.42 (0.02) | −0.40 (0.03) | −0.31 (0.10) |
| Mean Mouse Grip Force (N) | −0.50 (0.75) | 0.63 (0.01) | 0.11 (0.67) | −0.14 (0.60) | −0.15 (0.56) | |
| Normalized Mean Mouse Grip Force | −0.39 (0.12) | 0.26 (0.32) | −0.16 (0.54) | −0.38 (0.14) | −0.49 (0.05) | |
| 50th %tile FCR EMG | X | −0.49 (0.01) | −0.15 (0.42) | −0.27 (0.15) | −0.34 (0.07) | −0.49 (0.01) |
| 50th %tile FCU EMG | −0.43 (0.02) | −0.09 (0.65) | −0.11 (0.57) | −0.29 (0.13) | −0.26 (0.17) | |
| 50th %tile ECU EMG | −0.16 (0.41) | −0.24 (0.21) | −0.18 (0.34) | −0.01 (0.95) | −0.50 (0.00) | |
| 50th %tile ECR EMG | X | −0.20 (0.28) | −0.23 (0.23) | −0.42 (0.02) | −0.19 (0.33) | −0.03 (0.87) |
| 50th %tile Trapizeus EMG | −0.06 (0.76) | −0.09 (0.65) | −0.35 (0.05) | 0.00 (0.98) | −0.08 (0.67) | |
| 50th %tile Anterior Deltoid EMG | −0.19 (0.32) | 0.19 (0.31) | −0.15 (0.42) | −0.01 (0.97) | −0.21 (0.26) | |
| 50th %tile Medial Deltoid EMG | 0.31 (0.10) | 0.24 (0.21) | 0.20 (0.29) | 0.20 (0.28) | 0.36 (0.05) | |
| Median Wrist Extension | 0.02 (0.92) | 0.15 (0.43) | 0.14 (0.47) | −0.22 (0.24) | 0.35 (0.06) | |
| Range of Motion of Wrist Extension | X | −0.55 (0.00) | −0.31 (0.09) | −0.42 (0.02) | −0.48 (0.01) | −0.39 (0.04) |
| Median Wrist Ulnar Deviation | −0.18 (0.35) | −0.31 (0.09) | −0.18 (0.35) | −0.09 (0.62) | −0.28 (0.13) | |
| Range of Motion (ROM)of Wrist R/U | −0.31 (0.10) | −0.33 (0.08) | −0.39 (0.03) | −0.44 (0.01) | −0.32 (0.08) | |
| Median Shoulder Flexion | −0.35 (0.06) | 0.10 (0.61) | −0.22 (0.23) | −0.27 (0.16) | −0.10 (0.62) | |
| ROM Shoulder Flexion | X | −0.41 (0.02) | −0.45 (0.01) | −0.46 (0.01) | −0.59 (0.00) | −0.29 (0.12) |
| Median Shoulder Abduction | −0.35 (0.06) | −0.07 (0.70) | −0.17 (0.38) | −0.44 (0.02) | −0.26 (0.17) | |
| Median Shoulder External Rotation | X | −0.51 (0.00) | −0.35 (0.06) | −0.66 (0.00) | −0.67 (0.00) | −0.31 (0.10) |
| ROM Shoulder External Rotation | −0.35 (0.06) | −0.26 (0.16) | −0.47 (0.01) | −0.56 (0.00) | −0.29 (0.12) | |
X indicates parameters that are greater for women compare to men
Figure 3.
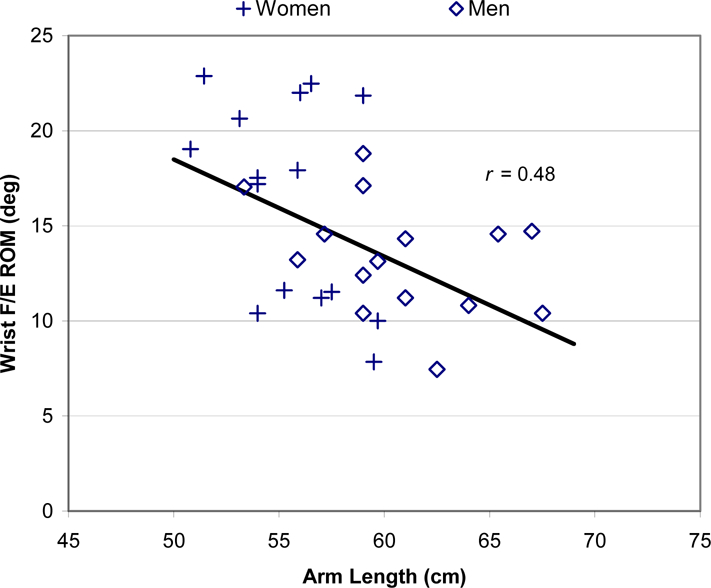
The range of motion of the wrist joint along the flexion extension (F/E) axis and the corresponding length of the subject’s arm.
The median values for shoulder width and arm length used to categorize the subjects by small and larger were 43 and 58 cm, respectively. Based on shoulder width, four subjects changed their grouping and based on arm length six subjects changed their grouping (i.e. three men were classified as small and three women were classified as large). The differences between small and large anthropometry, by either criterion, were similar to or more pronounced than those between men and women (Table 5). Some differences became statistically significant when categorized by anthropometry, such as the EMG amplitude of the Trapezius with shoulder width, and wrist range of motion and shoulder abduction with arm length.
Table 5:
Differences between subjects dichotomized by gender, shoulder width and arm length. Bold values indicate p-values < 0.05
| Parameter╲Dichotomized Variable | Gendera | Shoulder Widtha | Arm Lengtha | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Women | Men | p-valueb | Smaller (nf=13)c | Larger (nf=2)c | p-valueb | Smaller (nf=12)c | Larger (nf=3)c | p-valueb | |
| Mean keyboard Force (% MVC) | 2.8 (1.5) | 2.0 (0.7) | 0.04 | 2.9 (1.5) | 2.0 (0.7) | 0.02 | 2.9 (1.5) | 1.9 (0.6) | 0.02 |
| Median keyboard force (%MVC) | 2.3 (1.5) | 1.5 (0.7) | 0.03 | 2.3 (1.5) | 1.4 (0.7) | 0.02 | 2.3 (1.5) | 1.4 (0.7) | 0.02 |
| 90th percentile keyboard force (% MVC) | 6.1 (2.5) | 4.7 (1.3) | 0.03 | 6.2 (2.4) | 4.6 (1.3) | 0.01 | 6.2 (2.5) | 4.5 (1.0) | 0.01 |
| 50th %tile FCR EMG (% MVC) | 6.6 (1.1) | 3.8 (0.5) | 0.01 | 5.6 (0.6) | 4.8 (1.2) | 0.27 | 6.5 (1.2) | 3.9 (0.4) | 0.02 |
| 50th %tile ECR EMG(% MVC) | 15.0 (3.8) | 8.1 (1.0) | 0.05 | 14.9 (4.0) | 8.2 (1.0) | 0.05 | 14.9 (4.0) | 8.2 (0.9) | 0.05 |
| 50th %tile Trapezius EMG (% MVC) | 7.0 (1.1) | 5.0 (1.0) | 0.10 | 7.7 (1.3) | 4.4 (0.5) | 0.01 | 6.3 (1.2) | 5.8 (1.0) | 0.38 |
| Range of Motion of Wrist Extension (deg) | 16.3 (1.1) | 13.3 (1.1) | 0.04 | 15.9 (1.2) | 13.8 (1.2) | 0.13 | 16.7 (1.1) | 13.0 (1.1) | 0.03 |
| Range of Motion of Wrist R/U (deg) | 10.9 (0.8) | 10.0 (0.8) | 0.24 | 11.0 (0.8) | 9.9 (0.8) | 0.15 | 12.1 (0.7) | 8.8 (0.7) | 0.00 |
| Shoulder Flexion/Extension ROM (deg) | 9.9 (0.7) | 7.8 (0.8) | 0.02 | 10.0 (0.8) | 7.6 (0.6) | 0.00 | 10.3 (0.7) | 7.4 (0.7) | 0.00 |
| Shoulder Abduction 90th%tile (deg) | 9.6 (1.4) | 8.1 (1.3) | 0.21 | 9.4 (1.5) | 8.4 (1.4) | 0.3 | 10.4 (1.6) | 7.3 (1.0) | 0.05 |
| Median Shoulder External Rotation (deg) | 35.0 (6.5) | 14.2 (4.8) | 0.01 | 35.4 (6.4) | 13.8 (4.8) | 0.00 | 39.0 (6.5) | 10.1 (2.5) | 0.00 |
There were no significant differences between groups in terms of age and typing speed
p-values are from single sided student t-test testing if the values for women or smaller anthropometry were larger than values for men or larger anthropometry
nf = number of females in the group of 15 total.
For the text-editing task, the differences in parameters between women and men changed across different workstation configurations (Table 6). Differences between genders for both shoulder muscle activity and postural parameters were larger for the high mouse position compared to the standard mouse position. These gender differences were smaller for the centered mouse position compared to the standard mouse. Clear patterns across genders were not observed for forearm muscles or for wrist postural parameters between the three positions: Some parameters values increased while others decreased.
Table 6:
Mean values and (standard error) of selected biomechanical parameters between genders across three different workstation arrangements for the text edit task only.
| Biomechanical Parameter | Women | Standard Men | pd | Women | High Men | pe | Women | Center Men | pe |
|---|---|---|---|---|---|---|---|---|---|
| Median EMG (%MVC) | |||||||||
| FCR | 7.0 (1.4) | 3.8 (0.5) | 0.02 | 9.8 (2.4) | 4.4 (0.7) | 0.02 | 8.9 (2.5) | 3.8 (0.6) | 0.02 |
| FCU | 7.5 (1.8) | 5.4 (0.7) | 0.13 | 9.5 (2.2) | 7.8 (1.1) | 0.23 | 7.6 (1.8) | 3.8 (0.5) | 0.02 |
| ECU | 16.3 (1.7) | 12.3 (2.5) | 0.09 | 20.5 (3.6) | 14. (2.7) | 0.06 | 13.5 (1.8) | 11.0 (2.8) | 0.22 |
| ECR | 15.1 (4.3) | 8.0 (1.0) | 0.06 | 15.7 (4.1) | 7.9 (1.2) | 0.04 | 14.6 (3.4) | 8.0 (0.9) | 0.03 |
| Trapizeus | 8.3 (1.3) | 5.9 (1.1) | 0.08 | 11.9 (2.0) | 7.4 (1.4) | 0.03 | 8.3 (1.3) | 5.9 (1.1) | 0.16 |
| Ant. Deltoid | 4.3 (0.9) | 3.9 (0.8) | 0.34 | 8.4 (1.4) | 5.2 (1.1) | 0.04 | 3.6 (0.5) | 2.6 (0.05) | 0.09 |
| Med. Deltoid | 4.1 (0.5) | 4.4 (0.1) | 0.36 | 9.1 (2.0) | 6.2 (1.0) | 0.10 | 6.5 (2.1) | 4.1 (0.6) | 0.13 |
| Shoulder (°) | |||||||||
| 50th% Flexion | 8 (2) | 12 (3) | 0.17 | 31 (2) | 23 (3) | 0.01 | −1 (2) | 2 (3) | 0.22 |
| ROM Flexion | 15 (2) | 11 (1) | 0.03 | 36 (3) | 30 (2) | 0.04 | 21 (2) | 19 (2) | 0.18 |
| 50th% Ext. | 55 (11) | 24 (7) | 0.01 | 61 (13) | 23 (11) | 0.02 | 6 (5) | −4 (4) | 0.05 |
| Rotation (°) | |||||||||
p value for single sided student t-test testing if the values for women were larger than values for men the value across the gender groups stratified within each mouse position condition. Bolded vales indicate p<0.05
DISCUSSION
The goal of this laboratory study was to quantify differences in applied forces, upper extremity muscle activity and upper extremity posture between genders when working at a computer work-station adjusted for each individual’s anthropometry based on current guidelines. Since there were differences between genders the study also explored correlations of these upper extremity biomechanical measures with anthropometry. Significant differences were observed for normalized keyboard force, forearm muscle activity and shoulder postural measures across groups of individuals when grouped by gender and when dichotomized by anthropometry. In general, exposures were higher for women, and when dichotomized by anthropometry, for the smaller computer operators. Differences were more pronounced when groups were defined by anthropometry than by gender. Differences in shoulder postural and muscle activity measures were also greater when the work station was configured with the mouse in a non-optimal position, whereas these differences decreased when the mouse was positioned in the center of the work station, a potential intervention (Dennerlein and Johnson, 2006b).
The differences in normalized applied forces and muscle activity metrics across genders and their relationships with anthropometry may be due to differences of muscle strength. Both the force and the EMG signals were normalized to values obtained during maximum voluntary contractions, which were significantly higher in men than in women (Table 3). Since there were no differences in absolute force the relative force will have an inverse relationship with strength and thus this study observed that the normalized forces were greater in the women. They have to use a higher percentage of their strength to achieve the same absolute force as men. The relationships observed with anthropometry may also be related to strength, since strength is related to the size and cross sectional area of muscles (Zajac, 1989). Wahlstrom et al (2000) also observed a similar relationship for normalized mouse grip and button forces across genders but did not explore anthopometric relationships.
The differences in shoulder postures between genders and their associations with anthropometry may be due to the different kinematic demands of the upper extremity related to anthropometry. With the commonly used mouse position where the mouse is placed just beyond the right edge of the keyboard, the shoulder has to externally rotate so that the hand can reach the mouse. For those with narrow shoulders the base of this rotation is closer to the center of the keyboard and thus the operator with smaller stature has to externally rotate out more to reach the mouse. Karlqvist et al (1998) also hypothesized this relationship. The two other mouse positions tested support this hypothesis. For the high mouse position the mouse is further away relative to arm length and shoulder width and there were larger differences between genders. When the mouse is centered it is then close and there were smaller differences across genders. In addition Dennerlein and Johnson (2006b) reported that postures for both men and women are more neutral for a more centered mouse position.
These differences in factors may provide an explanation of why women have higher prevalence of musculoskeletal disorders compared to men. Given the exact same task and that the workstations were set up according to specific anthropometric guidelines for both men and women, women had less neutral shoulder postures, especially for external rotation. Since the degree of external rotation was highly related to anthropometry and women have smaller anthropometry, on average, these awkward postures may be a result of a poor fit for women compared to men in computer workstations.
The differences between genders become more pronounced when a workstation is not configured to standard guidelines. It is also worth noting the ubiquity of poor workstation design in the modern US workplace. A survey of 1000 workstations at various companies in the United States revealed that 75% of office workstations were not correctly set-up (Dennerlein and Johnson, 2003). The resultant biomechanical disadvantage that these improperly set-up workstations pose may also explain the high prevalence of musculoskeletal disorders.
Most ergonomic guidelines (e.g. OSHA, 1997) suggest vertical adjustments of workstations to match an operator’s anthropometry; however, guidelines suggest a standard keyboard and pointing device position within the horizontal worksurface without consideration for different subject anthropometries. These data along with the higher prevalence of MSD among women, who have smaller anthropometry, suggest that perhaps more attention should be paid to both the horizontal position of the mouse within the workstation and the size of the mouse and keyboard. Ergonomic products exist to bring the mouse closer to the center; however, most keyboards come with numeric key pads that push the mouse further to the right requiring more outward rotation. For computer operators that either do not use or minimally use the numeric keypad, one alternative would be to use a keyboard without numeric keypad or one that is detachable. This would bring the mouse closer to the body’s centerline (Harvey and Peper, 1997; Sommerich et al., 2002; Dennerlein and Johnson, 2006b). In addition, men have significantly greater strength capacities in the hands yet men and women use input devices which require the same activation force, irrespective of gender/strength. The data clearly demonstrates that women have to work at higher relative force capacities than men and this may also partially contribute to the higher prevalence of injuries among women. It is likely that certain exposures would be reduced if the computer input devices themselves were designed/scaled to be more in proportion with the stature and strength of the user intended to operate them. Sometimes this may prove useful. For instance, this study observed that women have less wrist extension than men contrary to what Wahlstrom et al (2000) observed. This difference may be explained by the different mice used, which in turn may have different effects on genders. Wahlstrom et al. used an Apple mouse that is flat and low profile whereas this study used a MicroSoft mouse that fills the hand. Men can generally anchor the wrist behind the MicroSoft mouse but not all women can; they instead tend to rest the hand on the mouse, resulting in less extension.
The differences between genders appear to be in part due to anthropometric differences between genders. As we grouped subjects based on anthropometry differences observed between genders were more pronounced. Some parameters that were not significant between genders became significant based on anthropometry. This study is limited in the overlap of anthropometry between women and men to fully test this further. If for example, one could examine the difference between a group of men and women that are not different in terms of key anthropometric measures. Such a study could add to our understanding in mechanisms leading to the observed differences in exposure between genders.
These conclusions have to be taken within the context of this study and within the limitations of this study. First these hypotheses were tested within a small population, limiting our power to detect differences and generalize the results. Unfortunately, the small sample size was partly due to equipment failure. Nonetheless there was statistical significance for many variables where the complete study population was sampled. .
While the average stature and hand length for our participants were similar to those for the general population of North America (Jurgens et al., 1990), there was a moderate overlap between genders in size/anthropometry. Four subjects (27%) changed categories for dichotomizing by shoulder width and 6 subjects (40%) for arm length. If the groupings were based on stature, only two subjects would change groups. Grouping subjects by anthropometry often provided stronger differences than group subjects by gender, but the numbers did not permit cross-tabulation by both gender and anthropometry simultaneously. In addition, the effects of mainly the lengths of limbs were studied. Other anthropometric variables may also influence our results.
In conclusion, when a work station is adjusted per current guidelines for computer workstations differences in upper extremity force, muscle activity and postural factors still exist between genders. However, these differences in biomechanical parameters were often stronger when subjects were grouped by anthropometry suggesting that perhaps the computer input devices themselves should be scaled to be more in proportion with the stature and strength of the user. Many of these correlations are the result of variable sized or computer operators which vary in strength using either fixed size devices or devices with fixed activation forces. In the interim, either using a smaller footprint keyboard without the numeric keypad, placing the mouse or using accessories to place the mouse closer to the center line will likely reduce some of the postural differences between men and women in computer operation.
ACKNOWLEDGEMENTS
Partial financial support to complete this study came from the National Institute for Occupational Safety and Health R010H03997, the Office Ergonomics Research Committee (www.oerc.org) and the Liberty Mutual Harvard Program for Occupational Safety and Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NIOSH. The authors thank Theodore Becker and others who assisted in the data collection, analysis and reporting.
Author Biography
Erik Won
Erik Won obtained his doctor of osteopathic medicine (DO) from Nova Southeastern University, in Ft. Lauderdale, FL in 1998. He interned at the U.S. Navel Medical Center in Portsmouth, Virginia in 1999. He has served as a Squadron Flight Surgeon at Camp Pendleton, CA before completing his residency in occupational and environmental medicine at the Harvard School of Public Health in 2004. He has held several clinical leadership positions including Chief Resident for the Occupational and Environmental Medicine Residency at the Harvard School of Public Health. Dr. Won is currently Physician, Medical Services, Boeing Corporation in Southern California.
Laura Punnett

Laura Punnett obtained a Doctor of Science degree from the Harvard School of Public Health in occupational health and epidemiology and completed her post-doctoral training in occupational ergonomics at The University of Michigan. She was a founding member of the Department of Work Environment at the University of Massachusetts Lowell, where she is now Professor of Occupational Epidemiology and Ergonomics. She is also Co-Director of the Lorin Kerr Ergonomics Institute (KEI) for Occupational Injury Prevention, Senior Associate at the Center for Women and Work, and Co-Director for the newly formed Center for the Promotion of Health in the New England Workplace. In 1996–1997 she was a Visiting Scientist, Division of Ergonomics, at the Swedish National Institute of Working Life, and in 2002–2003 she was Epidemiologist with the Industry-wide Studies Branch of the National Institute of Occupational Safety and Health. Dr. Punnett’s research interests include the epidemiology of work-related musculoskeletal disorders; the effect of ergonomic stressors on other health endpoints, such as pregnancy outcomes and acute injury risk; and methods for workplace measurement of ergonomic exposures, including the validity of worker self-assessments. She has also studied the factors influencing the effectiveness of ergonomic intervention programs and joint labor/management health and safety committees in industry.
Peter Johnson:
Peter Johnson obtained his PhD degree in Bioengineering from the University of California - Berkeley and San Francisco in 1998. He has worked as a researcher at the National Institutes of Occupational Health in the United States, Sweden and Denmark; as a Visiting Researcher in the Department of Occupational and Environmental Medicine at the Sahlgrenska Academy at Gothenburg University, Gothenburg, Sweden and as a Visiting Scientist at Harvard’s School of Public Health. Currently he is an Associate Professor in the Department of Environmental and Occupational Health Sciences at the University of Washington in Seattle. His research focuses on developing hardware and software systems for the assessment of physical exposures in the workplace and is also developing methods to measure muscle fatigue using electrical stimulation of the muscle.
Jack Dennerlein

Jack Dennerlein obtained his Ph.D, degree in from the University of California - Berkeley in 1996 and completed a post-doctoral training at the School of Engineering at Harvard University. Currently he is an Associate Professor in the Department of Environmental Health Sciences at the Harvard School of Public Health where he is also the co-director for the Occupational Injury Prevention Research Training Program supported by the United States National Institute for Occupational Safety and Health. From 2004 to 2005, Dr. Dennerlein was a visiting Scientist in the Faculty of Human Movement Sciences at the VU University, Amsterdam in the Netherlands. His primary research interests are in neuromuscular and occupational biomechanics with application in exposure assessment of work-related musculoskeletal disorders.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- Buchanan TS, Moniz MJ, Dewald JP, Zev Rymer W. Estimation of muscle forces about the wrist joint during isometric tasks using an EMG coefficient method. J. of Biomechanics, 1993; 26, 547–60. [DOI] [PubMed] [Google Scholar]
- Cook CJ, Kothiyal K. Influence of mouse position on muscular activity in the neck, shoulder and arm in computer users. Appl Ergon, 1998; 29, 439–43. [DOI] [PubMed] [Google Scholar]
- de Smet L, Ghyselen H, Lysens R. Incidence of overuse syndromes of the upper limb in young pianists and its correlation with hand size, hypermobility and playing habits. Chir Main 1998; 17(4):309–13. [DOI] [PubMed] [Google Scholar]
- Dennerlein JT, Johnson PW. Different computer tasks affect the exposure of the upper extremity to biomechanical risk factors. Ergonomics 2006a; 49(1): 45–61. [DOI] [PubMed] [Google Scholar]
- Dennerlein JT, Johnson P. Positions of the computer mouse within a thousand workstations, Human Factors and Ergonomics Society Conference, Denver, CO, 2003. [Google Scholar]
- Dennerlein JT, Johnson PW. Changes in upper extremity biomechanics across different mouse positions in a computer workstation. Ergonomics, 2006b; 49, 1456–69. [DOI] [PubMed] [Google Scholar]
- Gerr F, Marcus M, Ensor C, Kleinbaum D, Cohen S, Edwards A, Gentry E, Ortiz DJ, Monteilh C. A prospective study of computer users: I. Study design and incidence of musculoskeletal symptoms and disorders. Am J Ind Med 2002; 41(4):221–35. [DOI] [PubMed] [Google Scholar]
- Greene WB, Heckman JD. Clinical Measurement of Joint Motion. Amer Acad of Orthopaedic Surgeons, Rosemont, Illinois, 1994. [Google Scholar]
- Harvey R, Peper E. Surface electromyography and mouse use position. Ergonomics, 1997; 40, 781–9. [DOI] [PubMed] [Google Scholar]
- Johnson PW, Hagberg M, Hjelm EW, Rempel D. Measuring and characterizing force exposures during computer mouse use. Scand J Work Environ Health, 2000; 26, 398–405. [DOI] [PubMed] [Google Scholar]
- Jonsson B The static load components in muscle work. Eurp J Appl Physiol 1988; 57:305–310 [DOI] [PubMed] [Google Scholar]
- Jonsson P Johnson PW. Comparison of measurement accuracy between two types of wrist goniometer systems. Appl Ergon 2001; 32(6): 599–607 [DOI] [PubMed] [Google Scholar]
- Jurgens HW, Aune IA, Pieper U. International Data on Anthropometry, International Labour Office, Geneva, Switzerland, 1990 [Google Scholar]
- Karlqvist LK, Bernmark E, et al. (1998) Computer mouse position as a determinant of posture, muscular load and perceived exertion. Scan J Work Environ Health, 1998; 24(1): 62–73 [DOI] [PubMed] [Google Scholar]
- Lassen CF, Mikkelsen S, Kryger AI, Andersen JH. Risk factors for persistent elbow, forearm and hand pain among computer workers. Scand J Work Environ Health 2005; 31, 122–31. [DOI] [PubMed] [Google Scholar]
- OSHA. Working safely with Video Display Terminals, Revised (OSHA 3092) U.S. Department of Labor, Occupational Safety and Health Administration (OSHA), 1997. [Google Scholar]
- Perotto A Anatomical guide for the electromyographer: the limbs and trunk Thomas Charles C, Springfield, IL, 1994. [Google Scholar]
- Pheasant S, Haslegrave CM. Bodyspace: Anthropometry, Ergonomics and the Design of Work CRC Press, Taylor and Francis, Boco Raton, FL, 2005. [Google Scholar]
- Punnett L, Bergqvist U. Musculoskeletal disorders in visual display unit work: Gender and work demands. Occupational Medicine: State of the Art Reviews Cherniack MG. Philadelphia PA, Hanley & Belfus, Inc. 1999;14: 113–124. [PubMed] [Google Scholar]
- Punnett L, Bergqvist U. Visual display unit work and upper extremity musculoskeletal disorders. A review of epidemiological findings. Arbete och Hälsa 1997; 16, Solna, Sweden, National Institute of Working Life. [Google Scholar]
- Punnett L, Herbert R. Work-related Musculoskeletal Disorders: Is There a Gender Differential, and If So, What Does it Mean? In: Women and Health, eds. Goldman MB, Hatch M. Academic Press; San Diego CA, 1999. [Google Scholar]
- Rempel DM, Harrison RJ, Barnhart S. Work-related cumulative trauma disorders of the upper extremity. JAMA; 1992; 267(6):838–42. [PubMed] [Google Scholar]
- Sauter SL, Schleifer LM, Knutson SJ. Work posture, workstation design, and musculoskeletal discomfort in a VDT data entry task. Hum Factors, 1991; 33, 151–67. [DOI] [PubMed] [Google Scholar]
- Sommerich C, Starr H, Smith CA., Shivers C. Effects of notebook computer configuration and task on user biomechanics, productivity, and comfort. International Journal of Industrial Ergonomics, 2002; 30, 7–31. [Google Scholar]
- Treaster DE, Burr D. Gender differences in prevalence of upper extremity musculoskeletal disorders. Ergonomics, 2004; 47, 495–526. [DOI] [PubMed] [Google Scholar]
- Wahlstrom J, Svensson J, et al. , Differences between work methods and gender in computer mouse use. Scand J Work Environ Health 2000; 26(5):390–397. [DOI] [PubMed] [Google Scholar]
- Zajac FE. Muscle and tendon: properties, models, scaling, and application to biomechanics and motor control. Crit Rev Biomed Eng 1989; 17:359–411. [PubMed] [Google Scholar]