

Abstract
Background: RAD-140, one of the novel selective androgen receptor modulators (SARMs), has potent anabolic effects on bones and muscles with little androgenic effect. Despite the lack of approval for its clinical use, RAD-140 is readily accessible on the consumer market. Hepatotoxicity associated with the use of SARMs has only rarely been reported in the literature.
Case Report: A 24-year-old male presented with a 2-week history of diffuse abdominal pain, scleral icterus, pruritus, and jaundice. Prior to presentation, he had been taking the health supplement RAD-140 for muscle growth for 5 weeks. He had a cholestatic pattern of liver injury, with a peak total bilirubin of 38.5 mg/dL. Liver biopsy was supportive of a diagnosis of RAD-140–associated liver injury characterized pathologically by intracytoplasmic and canalicular cholestasis with minimal portal inflammation. Symptoms and liver injury resolved after cessation of the offending agent.
Conclusion: To date, only select descriptions of the potential hepatoxicity associated with the use of SARMs, including RAD-140, have been published. Given their potential hepatoxicity and ready availability on the consumer market, RAD-140 and other SARMs should be used judiciously and under close clinical supervision until further hepatic safety data become available.
Keywords: Chemical and drug induced liver injury, Enobosarm, LGD-4033, RAD140
INTRODUCTION
Nonsteroidal selective androgen receptor modulators (SARMs), including RAD-140, Enobosarm, and Ligandrol, promote anabolic effects on bones and muscles through binding to androgen receptors, similar to traditional anabolic-androgenic steroids such as testosterone.1-3 Unlike anabolic-androgenic steroids, SARMs do not have the unwanted androgenic effects because they are not metabolized to dihydrotestosterone by 5-alpha reductase or to estrogen by aromatase.2 Because of the high tissue selectivity of their anabolic actions, SARMs are being studied in several clinical applications, including sarcopenia, cancer-related cachexia, prostate cancer, breast cancer, and osteoporosis.1 Despite receiving a warning from the US Food and Drug Administration and being banned by the World Anti-Doping Agency, SARMs remain readily accessible in the online marketplace and are used as alternatives to anabolic-androgenic steroids for muscle and strength development.4-6 Unlike anabolic-androgenic steroids, which have a well-known hepatotoxic profile, only limited hepatic safety data are available for SARMs.3,7-12 We report a case of drug-induced liver injury caused by the use of the SARM RAD-140.
CASE REPORT
A previously healthy 24-year-old male presented to the emergency department (ED) with a 2-week history of diffuse abdominal pain, pruritus, scleral icterus, and jaundice. Approximately 2 months earlier, he had started taking up to 15 mg daily of RAD-140 for a total of 5 weeks for muscle growth. The only other medication that he took was acetaminophen 250 mg/aspirin 250 mg/caffeine 65 mg (used 4 times daily as needed for headache, no more than twice a week). He had stopped both medications 2 weeks prior to presentation as instructed by his primary care provider (PCP) because of the incidental finding of elevated liver chemistries (Table 1, Routine PCP office visit, +5 weeks).
Table 1.
Liver Test Results
| Timeline | Total Bilirubin, mg/dL (Reference, 0.2-1.2) | ALT, IU/L (Reference, 17-63) | AST, IU/L (Reference, 15-41) | ALP, IU/L (Reference, 32-91) | Platelet Count, × 109/L (Reference, 150-450) | INR (Reference, <1.0) | Albumin, gm/dL (Reference, 3.5-4.8) |
|---|---|---|---|---|---|---|---|
| Prior to RAD-140 use, –14 months | 1.0 | 48 | 26 | 82 | 152 | – | 4.6 |
| Started RAD-140 | – | – | – | – | – | – | |
| Routine PCP office visit, +5 weeks | 1.2 | 313 | 182 | 103 | 180 | 0.8 | 4.4 |
| Emergency department encounter, +7 weeks | 10.8 | 171 | 71 | 151 | 263 | 0.85 | 4.1 |
| Hepatology office visit, +8 weeks | 32.3 | 125 | 82 | 181 | 305 | 0.96 | 3.9 |
| Hepatology office visit, +10 weeks | 24.8 | 212 | 120 | 251 | 310 | 1.47 | 3.0 |
| Hospital day 1, +10 weeks, 2 days | 28.7 | 155 | 94 | 232 | 341 | 1.36 | 2.9 |
| Hospital day 2 | 26.1 | 134 | 76 | 203 | 312 | 1.46 | 2.5 |
| Hospital day 3 | 27.3 | 115 | 62 | 199 | 260 | 1.61 | 2.6 |
| Hospital day 4 | 24.3 | 117 | 79 | 194 | 268 | 1.69 | 2.5 |
| Postdischarge hepatology office visit, +11 weeks | 38.5 | 143 | 104 | 189 | 299 | 0.84 | 2.9 |
| Postdischarge hepatology office visit, +14 weeks | 24.6 | 120 | 118 | 187 | 261 | 0.89 | 2.9 |
| Postdischarge hepatology office visit, +18 weeks | 4.9 | 118 | 79 | 118 | 170 | 0.91 | 4.0 |
ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate aminotransferase; INR, international normalized ratio; PCP, primary care provider.
In the ED, the patient denied consuming alcohol or using any other supplements, over-the-counter or prescription medications, or recreational drugs. Physical examination was normal except for jaundice and scleral icterus. Laboratory data revealed total bilirubin of 10.8 mg/dL (reference range, 0.2-1.2 mg/dL), alkaline phosphatase of 151 IU/L (reference range, 32-91 IU/L), alanine aminotransferase of 171 IU/L (reference range, 17-63 IU/L), and aspartate aminotransferase of 71 IU/L (reference range, 15-41 IU/L). Gamma-glutamyl transpeptidase, international normalized ratio (INR), total protein, albumin, and complete blood count were within normal limits (Table 1, Emergency department encounter, +7 weeks). Hospital admission for further testing was recommended; however, the patient declined and left against medical advice.
A week after his index hospital encounter, the patient was seen in the hepatology clinic for follow-up, where he was noted to have worsening jaundice and pruritus. Blood work revealed total bilirubin of 32.3 mg/dL, alkaline phosphatase of 181 IU/L, alanine aminotransferase of 125 IU/L, aspartate aminotransferase of 82 IU/L, and INR of 0.96 (Table 1, Hepatology office visit, +8 weeks). Based on the patient's initial assessment, drug-induced liver injury from recent RAD-140 use was suspected. However, as he did not show any signs or symptoms concerning for acute liver failure that would warrant immediate hospitalization, further workup for his abnormal liver tests and short-interval follow-up were arranged. Two weeks later, he returned to the hepatology clinic, and blood work revealed total bilirubin of 24.8 mg/dL, alkaline phosphatase of 251 IU/L, alanine aminotransferase of 212 IU/L, aspartate aminotransferase of 120 IU/L, and INR of 1.47 (Table 1, Hepatology office visit, +10 weeks).
Given his significantly elevated liver tests and now elevated INR, he was urged to go to the ED, where he was admitted for closer monitoring and diagnostic evaluation. He did not display any signs or symptoms of encephalopathy. He denied any interval use of prescription or over-the-counter medications, supplements, alcohol, or recreational drugs. Serologic markers for viral hepatitis and autoimmune liver conditions were negative. Serum ferritin was significantly elevated at 1,523 ng/mL (reference range, 22-322 ng/mL), but transferrin saturation was only 21% (reference, ≤45%) and he was negative for C282Y/H63D mutations. Ceruloplasmin level was normal. Alpha-1 antitrypsin (AAT) level was normal, and AAT phenotype was Pi*MZ. Urine toxicology screen, alcohol screen, and acetaminophen level were negative. Doppler ultrasound of the liver was unremarkable. Abdominal axial computed tomography and magnetic retrograde cholangiogram revealed hepatomegaly and limited focal fatty infiltration with patent biliary tree and vasculature (Figure, A and B). Percutaneous liver biopsy revealed bile accumulation inside the hepatocytes and canaliculi (Figure, C) with minimal portal infiltrates of lymphocytes (Figure, D) and no significant steatosis, necrosis, fibrosis, stainable iron, or intracytoplasmic inclusions on periodic acid–Schiff stain, consistent with drug-induced cholestasis.
Figure.
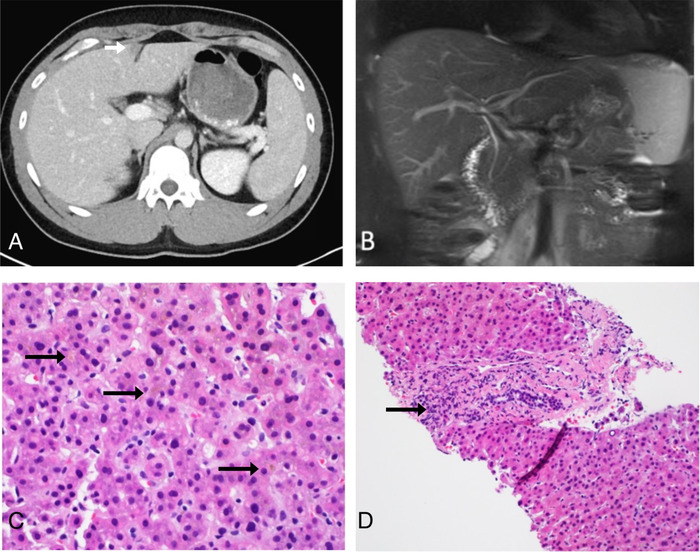
(A) Axial contrast-enhanced computed tomography image shows hepatomegaly and focal fatty infiltration (arrow). (B) Magnetic resonance cholangiopancreatography demonstrates patent biliary tree. (C) Liver histology illustrates hepatocellular and canalicular cholestasis (arrows) (hematoxylin and eosin [H&E] stain, magnification ×40). (D) Liver histology reveals minimal portal inflammation (arrow) (H&E stain, magnification ×20).
The patient had an unremarkable hospital course. Serial laboratory testing showed gradually improving liver chemistries and stable INR. As acute liver failure was not a concern, N-acetylcysteine was not given.
The patient was discharged on hospital day 4. He returned to the hepatology clinic for regular visits up to 5 months postdischarge. At his most recent clinic visit, his symptoms had entirely resolved, and his liver tests had markedly improved (Table 1, Postdischarge hepatology office visit, +18 weeks). The patient did not return for his next scheduled hepatology clinic visit and did not return calls to reschedule. Approximately 14 months postdischarge, he was seen at the PCP clinic for reasons unrelated to his liver injury. Routine blood work including liver tests was ordered but not completed.
DISCUSSION
This case of RAD-140–associated cholestatic liver injury had an assessed Drug-Induced Liver Injury Network causality score of 1 (probable) and a severity score of 3 (severe injury).8 To our knowledge, ours is the sixth case of SARM-associated drug-induced liver injury and the third case associated with RAD-140 use (Table 2).9-12 Similar to the previously reported cases, jaundice was the presenting symptom in our patient. Except for one case, SARM-related liver injury was either of mixed or cholestatic pattern.9-12 In our case, we observed a primarily cholestatic pattern of injury, with an initial moderate elevation in transaminases, followed by profound hyperbilirubinemia. We observed a latency period of approximately 6 weeks from cessation of the SARM to peak bilirubin levels, compared to Flores et al who reported a latency period of 5 weeks.9 Similar to Flores et al and Bedi et al, we observed a mild elevation in INR without fulminant liver failure.9,12 Liver biopsies typically demonstrate intracytoplasmic or canalicular cholestasis with minimal or nonexistent necrosis or inflammation. In all cases of SARM-related hepatoxicity to date, including ours, liver injury resolved with cessation of the offending agent. No patients developed fulminant liver failure, and no deaths occurred. While our patient did not receive any specific treatment for his liver injury, ursodeoxycholic acid may be beneficial in relieving cholestasis related to drug-induced liver injury, although data are largely lacking.13
Table 2.
Summary of Cases of Selective Androgen Receptor Modulator (SARM)-Associated Hepatotoxicity
| Study | SARM | Presenting Symptoms | Duration of SARM Use | Initial / Peak Bilirubin, mg/dL | Time to Peak Bilirubin After SARM Cessation | Initial ALT / AST / ALP, IU/L | Initial Platelet Count, × 109/L | INR | Liver Histology | Management |
|---|---|---|---|---|---|---|---|---|---|---|
| Flores et al, 20209 | Ligandrol | Jaundice, anorexia, nausea, lethargy, weight loss | 9 weeks | 6.78/6.78 | 5 weeks | 273/111/289 | 387 | 1 | – | SARM cessation, supportive care |
| Barbara et al, 202010 | Ligandrol | Jaundice, fatigue, pruritus, weight loss | 2 weeks | 35/38.2 | – | 229/91/88 | – | 1.1 | Cholestatic hepatitis with mild portal, periportal, and perisinusoidal fibrosis | SARM cessation, supportive care |
| Bedi et al, 202112 | Enobosarm | Jaundice, anorexia, weight loss, lethargy, diarrhea | 2 months | 19.9/43.0 | – | 112/69/268 | 313 | 1.3 | Moderate to severe cholestasis, very mild ductal damage | SARM cessation, supportive care |
| Flores et al, 20209 | RAD-140 | Jaundice, pruritus | 4 weeks and intermittent use thereafter | 17/20.2 | – | 44/61/286 | 347 | 1.2 | Moderate cholestasis, ductopenia, minimal fibrosis and inflammation | SARM cessation, supportive care |
| Barbara et al, 2020,11 | RAD-140 / Ligandrol | Jaundice, right upper quadrant pain, pruritus, diarrhea | 7 weeks | 34.5/34.5 | – | 46/36/529 | – | 1.0 | Diffuse canalicular cholestasis, ductal reaction, mild lobular inflammation with rare non-necrotizing epithelioid granuloma and mild portal and periportal fibrosis | SARM cessation, supportive care |
| Present case, 2022 | RAD-140 | Jaundice, abdominal pain, scleral icterus, pruritus | 5 weeks | 1.2/38.5 | 5 weeks, 6 days | 313/182/103 | 180 | 0.8 | Moderate intracytoplasmic and canalicular cholestasis, minimal portal inflammation | SARM cessation, supportive care |
ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate aminotransferase; INR, international normalized ratio.
Our patient had a history of using acetaminophen and salicylic acid prior to the onset of his liver injury. However, acetaminophen and/or salicylic acid–related hepatoxicity was deemed unlikely because of the small accumulated dosage, and more importantly, the lack of classic zone 3 necrosis/apoptosis and/or microvesicular steatosis. On the other hand, bland cholestasis, a pathologic feature commonly observed in anabolic-androgenic steroid–induced hepatotoxicity, highly suggests cholestatic injury from RAD-140.14
The molecular mechanisms underlying SARM-induced hepatotoxicity are largely speculative. The bland cholestasis seen in both anabolic-androgenic steroid– and RAD-140/Enobosarm–associated hepatotoxicity highly suggests involvement of androgen receptors in dysregulation of bile transport. In animal studies, the bile salt export pump (BSEP), an ATP-binding cassette subfamily B member 11 (ABCB11) transporter, was reported to be involved in anabolic-androgenic steroid–induced cholestatic injury.7,15,16 Whether the association of RAD-140 with androgen receptors regulates BSEP through receptor-associated signaling pathways remains to be defined. In humans, the ABCB11 mutation was reported to increase the genetic susceptibility of anabolic-androgenic steroid–induced cholestasis.17 Although we do not know if our patient has the ABCB11 mutation, he is heterozygous for alpha-1-antitrypsin Z (Pi*MZ), a phenotype reported to be a predisposing factor for liver disease and fibrosis.18 Whether Z heterozygosity contributes to drug-induced cholestasis remains to be determined.
CONCLUSION
The accumulating cases of drug-induced liver injury from SARMs raise concern about their hepatic safety and question the tissue selectivity of these agents. We caution the use of SARMs outside of clinical investigation and advocate for tighter regulation, close monitoring, and prompt reporting of adverse events associated with SARMs.
ACKNOWLEDGMENTS
This case was presented at the American College of Gastroenterology Scientific Meeting 2020 that took place virtually October 23-28, 2020. The authors have no financial or proprietary interest in the subject matter of this article.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
REFERENCES
- 1.Solomon ZJ, Mirabal JR, Mazur DJ, Kohn TP, Lipshultz LI, Pastuszak AW. Selective androgen receptor modulators: current knowledge and clinical applications. Sex Med Rev. 2019;7(1):84-94. doi: 10.1016/j.sxmr.2018.09.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Christiansen AR, Lipshultz LI, Hotaling JM, Pastuszak AW. Selective androgen receptor modulators: the future of androgen therapy? Transl Androl Urol. 2020;9(Suppl 2):S135-S148. doi: 10.21037/tau.2019.11.02 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Basaria S, Collins L, Dillon EL, et al. The safety, pharmacokinetics, and effects of LGD-4033, a novel nonsteroidal oral, selective androgen receptor modulator, in healthy young men. J Gerontol A Biol Sci Med Sci. 2013;68(1):87-95. doi: 10.1093/gerona/gls078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.FDA in brief: FDA warns against using SARMs in body building products. U.S. Food and Drug Administration. Published October 31, 2017. Accessed March 8, 2022. fda.gov/news-events/fda-brief/fda-brief-fda-warns-against-using-sarms-body-building-products
- 5.The prohibited list. World Anti-Doping Agency. Published January 1, 2022. Accessed March 8, 2022. wada-ama.org/en/prohibited-list
- 6.Van Wagoner RM, Eichner A, Bhasin S, Deuster PA, Eichner D. Chemical composition and labeling of substances marketed as selective androgen receptor modulators and sold via the internet [published correction appears in JAMA. 2018 Feb 20;319(7):724]. JAMA. 2017;318(20):2004-2010. doi: 10.1001/jama.2017.17069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Solimini R, Rotolo MC, Mastrobattista L, et al. Hepatotoxicity associated with illicit use of anabolic androgenic steroids in doping. Eur Rev Med Pharmacol Sci. 2017;21(1 Suppl):7-16. [PubMed] [Google Scholar]
- 8.Regev A, Seeff LB, Merz M, et al. Causality assessment for suspected DILI during clinical phases of drug development. Drug Saf. 2014;37 Suppl 1(Suppl 1):S47-S56. doi: 10.1007/s40264-014-0185-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Flores JE, Chitturi S, Walker S. Drug-induced liver injury by selective androgenic receptor modulators. Hepatol Commun. 2020;4(3):450-452. doi: 10.1002/hep4.1456 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Barbara M, Dhingra S, Mindikoglu AL. Ligandrol (LGD-4033)-induced liver injury. ACG Case Rep J. 2020;7(6):e00370. doi: 10.14309/crj.0000000000000370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Barbara M, Dhingra S, Mindikoglu AL. Drug-induced liver injury associated with Alpha Bolic (RAD-140) and Alpha Elite (RAD-140 and LGD-4033). ACG Case Rep J. 2020;7(6):e00409. doi: 10.14309/crj.0000000000000409 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bedi H, Hammond C, Sanders D, Yang HM, Yoshida EM. Drug-induced liver injury from enobosarm (ostarine), a selective androgen receptor modulator. ACG Case Rep J. 2021;8(1):e00518. doi: 10.14309/crj.0000000000000518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Robles-Díaz M, Nezic L, Vujic-Aleksic V, Björnsson ES. Role of ursodeoxycholic acid in treating and preventing idiosyncratic drug-induced liver injury. A systematic review. Front Pharmacol. 2021;12:744488. doi: 10.3389/fphar.2021.744488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bond P, Llewellyn W, Van Mol P. Anabolic androgenic steroid-induced hepatotoxicity. Med Hypotheses. 2016;93:150-153. doi: 10.1016/j.mehy.2016.06.004 [DOI] [PubMed] [Google Scholar]
- 15.Kullak-Ublick GA, Stieger B, Hagenbuch B, Meier PJ. Hepatic transport of bile salts. Semin Liver Dis. 2000;20(3):273-292. doi: 10.1055/s-2000-9426 [DOI] [PubMed] [Google Scholar]
- 16.Pauli-Magnus C, Meier PJ. Hepatobiliary transporters and drug-induced cholestasis. Hepatology. 2006;44(4):778-787. doi: 10.1002/hep.21359 [DOI] [PubMed] [Google Scholar]
- 17.El Sherrif Y, Potts JR, Howard MR, et al. Hepatotoxicity from anabolic androgenic steroids marketed as dietary supplements: contribution from ATP8B1/ABCB11 mutations? Liver Int. 2013;33(8):1266-1270. doi: 10.1111/liv.12216 [DOI] [PubMed] [Google Scholar]
- 18.Hakim A, Moll M, Qiao D, et al. Heterozygosity of the alpha 1-antitrypsin Pi*Z allele and risk of liver disease. Hepatol Commun. 2021;5(8):1348-1361. doi: 10.1002/hep4.1718 [DOI] [PMC free article] [PubMed] [Google Scholar]