

Abstract
Background and study aims Procedural sedation and analgesia (PSA) by trained non-anesthesiologist physicians and/or nurses is often performed during endoscopic procedures. Discharge from the recovery area after monitored observation is frequently based on fixed time parameters or subjective clinical assessment. In this study, the effect of implementation of the Aldrete score on recovery time after procedural sedation was analyzed in a real-life setting.
Patients and methods A prospective observational study of patients undergoing procedural sedation and analgesia during gastroscopy, colonoscopy or endoscopic ultrasound was performed. All procedures were randomly included to represent a real-life situation with different endoscopists, recovery nurses, endoscopy systems and indications. After a first observation period, all endoscopy nurses were trained to implement the Aldrete score when discharging patients, followed by a second observation period.
Results During the first observation period, the average time spent in the recovery area was 59 ± 22 minutes after procedural sedation. After implementation of the Aldrete score, the recovery time decreased significantly to 47 ± 25 minutes ( P < 0.01) with identical doses of procedural sedation and analgesia. The decrease in time was between 19 % and 35 % for the different endoscopic procedures.
Conclusions Implementation of the Aldrete score after procedural sedation and analgesia significantly reduces the time spent in the recovery area. The score can be used to safely implement a discharge policy that provides more efficient and standardized management for an endoscopy service.
Introduction
Because of the complexity of endoscopic procedures and/or the preferences of the endoscopist and/or patient, more and more procedures have been performed with procedural sedation and analgesia (PSA) in the last couple of years. PSA consists of administration of a sedative drug and/or analgesic drug as part of a procedure that is painful, causes stress and/or requires relative immobility (e. g. percutaneous gastrostomy placement). The purpose of PSA is twofold, namely, to make the procedure as comfortable as possible for the patient through optimal suppression of pain, stress and/or anxiety and to optimize conditions for diagnosis/therapy.
Increasing use of PSA results in new logistic challenges, especially in the recovery area, such as optimizing time planning and accurate monitoring of vital parameters until discharge. Frequently, discharge of patients is a decision based on subjective evaluation by the attending nurse or after a fixed period of time (e. g. 1 hour). International endoscopy societies, therefore, suggest use of post-anesthetic discharge scoring systems (PADSS) in analogy with the procedure after surgery and anesthesia in operating theaters [1]. Among the different PADSS, the Aldrete scoring system is being used commonly, evaluating activity, respiration, circulation, consciousness and oxygen saturation [2].
As part of a quality improvement project in endoscopy, it was hypothesized that implementation of the Aldrete scoring system could optimize time spent in the recovery area after PSA.
Patients and methods
A prospective observational study of patients undergoing procedural sedation and analgesia between November 21, 2019 and March 11, 2020 was performed. During the first observation period (November-December), recovery time after gastroscopy, colonoscopy and endoscopic ultrasound (EUS) with non-propofol non-anesthesiologist- administered procedural sedation and analgesia (midazolam + pethidine) was actively monitored in 231 patients. All procedures were consecutively included without interference by the observer to represent a real-life situation with different endoscopists, recovery nurses, endoscopy systems and indications. After this observation period, all endoscopy nurses were trained about how to implement the Aldrete score when discharging patients. After patient arrival in the recovery area, the Aldrete score was calculated every 10 minutes. After a minimum of 10 minutes, patients were discharged from the recovery area if they achieved an Aldrete score of 9 or more, accompanied by a responsible concomitance. Identical to the first observation period, recovery time after gastroscopy, colonoscopy and endoscopic ultrasound (EUS) with non-propofol non-anesthesiologist administered procedural sedation and analgesia (midazolam + pethidine) was actively monitored in 97 patients, identical to the first during the second observation period (February-March). The study was approved by the Educational Supervisory Committee on Medical Ethics (OBC) by delegation of Ethics Committee Research UZ/KU Leuven (OG032) and was performed in accordance with the Declaration of Helsinki. The primary endpoint was time spent in the recovery area after procedural sedation and analgesia until safe discharge and the secondary endpoint was time differences after different endoscopic procedures. Statistical analysis was performed using Student’s t -test.
Results
Based on subjective assessment by the nurse during the first observation period, the average time spent in the recovery area was 59 ± 22 minutes after procedural sedation with an average dose of 3.5 ± 1.3 mg midazolam and 30 ± 19 mg pethidine. After implementation of the Aldrete scoring system, the recovery time decreased significantly to 47 ± 25 minutes ( P < 0.01) with similar doses of procedural sedation (3.5 ± 1.2 mg midazolam and 32 ± 19 mg pethidine). No complications related to earlier discharge from the recovery area were observed and no readmissions to the Endoscopy Department or Emergency Department within 24 hours after sedation were recorded.
During the first observation period, the time spent in the recovery area had a Gaussian distribution, with the majority of patients spending between 41 and 50 minutes (average 59 minutes, median 60 minutes). After implementation of the Aldrete score, the Gaussian distribution shifted to the left with a more asymmetric time distribution and the majority of patients spent between 21 and 30 minutes (average 47 minutes, median 40 minutes) ( Fig. 1 ).
Fig. 1.
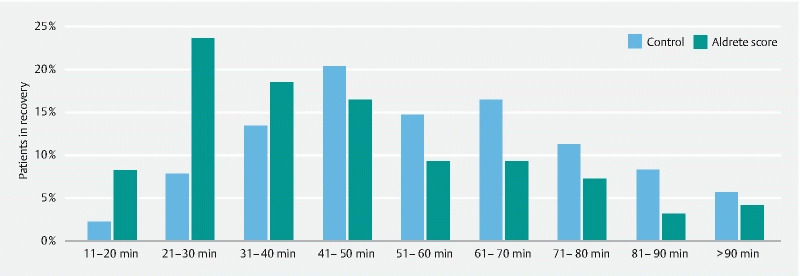
Patient distribution (%) in relation to time spent in the recovery area before (blue bars) and after implementation of Aldrete score (green bars)
The decrease in time was between 19 % and 35 % for the different endoscopic procedures, with significant gain of time after colonoscopy, therapeutic gastroscopy, and combined gastroscopy-colonoscopy ( Table 1 ).
Table 1. Average time spent in the recovery area after procedural sedation and analgesia (minutes + standard deviation) before and after implementation of Aldrete score.
| Control (min) | Aldrete score (min) | P value | |
| Endoscopic ultrasound | 54 ± 19 | 42 ± 25 | 0.06 |
| Diagnostic gastroscopy | 55 ± 19 | 45 ± 21 | 0.07 |
| Colonoscopy | 60 ± 24 | 50 ± 25 | < 0.05 |
| Colonoscopy + gastroscopy | 62 ± 17 | 40 ± 17 | < 0.05 |
| Therapeutic gastroscopy | 68 ± 28 | 47 ± 29 | < 0.05 |
| All procedures | 59 ± 22 | 47 ± 25 | < 0.01 |
Discussion
Endoscopic procedures with PSA are increasing in number and complexity, therefore, it is important to organize teaching and create protocols for safe post-procedure recovery. The length of time necessary to recover from PSA obviously depends on sedation depth, the patientʼs state of health, and the medication administered.
A significant number of (especially short-duration) endoscopic procedures with PSA result in complications in the recovery area. During the endoscopic procedure, stimuli are present, resulting in stressor responses stimulating ventilation while these stimuli are no longer present in the recovery area, leading to more shallow breathing and hypoxemia [3]. Therefore, time spent in the recovery area should not be too short, but discharge is often based on subjective assessment by the responsible nurse.
The Aldrete scoring system was created in 1970 [4] and it is analogous to the Apgar scoring system for neonates that was proposed in 1953 and currently still is in use worldwide [5]. The initial Aldrete scoring system was based on activity, respiration, circulation, and consciousness but also the more subjective parameter of color, namely pink, pale or cyanotic. With the invention of oxygen saturation monitoring, color has been replaced by oxygen saturation in the modified Aldrete scoring system [2]. The Aldrete scoring system does not take into account sedation depth or type of medication but compares the parameters at discharge with the pre-procedure parameters.
The Aldrete scoring system has been validated after general anesthesia, as well in the ambulatory surgical setting [6]. It has been assumed that PADSS like the Aldrete scoring system also can be used in discharge policy after endoscopic procedures with PSA. In the current observational study, this assumption was confirmed in a real-life endoscopic situation, resulting in more standardization and optimization of time management without lowering the quality of post-procedure care.
However, pain sensation or change in heart rate (as a surrogate marker for pain) is not included in the Aldrete scoring system. Discomfort or pain is a frequent finding after gastrointestinal endoscopy due to stomach or bowel distention, although the procedure is better tolerated after CO 2 insufflation that after air insufflation [7]. Also, the fact that patients are taking antihypertensive or antiarrhythmic medication (e. g. beta-blockers) is not included in the Aldrete scoring system.
In other specific situations, such as example ambulatory surgery, modified Aldrete scoring systems have been suggested to fulfil unmet needs such as monitoring of postoperative pain and bleeding [8]. Ideally a specific post-endoscopy discharge score should be created and validated, based on the Aldrete scoring system with additional relevant post-endoscopy parameters.
Pending a more dedicated post-endoscopy score, the current Aldrete scoring system can be easily implemented in the recovery area without major structural or logistic hurdles. Implementation of the Aldrete scoring system leads to a more standardized discharge policy after different diagnostic and therapeutic endoscopic procedures and provides clear guidelines to both responsible nurses and patients about criteria and estimated time of discharge. In a later phase, a more standardized discharge policy can optimize planning of different endoscopic procedures based on the number of beds in the recovery area and estimated time to discharge.
Conclusions
In conclusion, implementation of the Aldrete score after procedural sedation and analgesia is easy, safe, and significantly reduces the time spent in the recovery area.
Acknowledgement
We would like to thank Ramses Missotten, Emma Desmet and the entire Endoscopy E507 nursing staff for their support.
Footnotes
Competing interests Dr. Roelandt is supported by Clinical Mandate from Belgian Foundation against Cancer (Stichting tegen Kanker) and receives speaking and consultancy fees from MSD Belgium and Dr. Falk Pharma. Dr. Bisschops is supported by a research grant from Research Foundation Flanders (FWO) and receives speaking and consultancy fees from CDx Diagnostics, Cook, Fujifilm, GI Solutions, Ipsen, Medivators, Medtronic, Norgine and Pentax.
References
- 1.Dumonceau J M, Riphaus A, Schreiber F et al. Non-anesthesiologist administration of propofol for gastrointestinal endoscopy: European Society of Gastrointestinal Endoscopy, European Society of Gastroenterology and Endoscopy Nurses and Associates Guideline – Updated June 2015. Endoscopy. 2015;47:1175–1189. doi: 10.1055/s-0034-1393414. [DOI] [PubMed] [Google Scholar]
- 2.Aldrete J A. The post-anesthesia recovery score revisited. J Clin Anesth. 1995;7:89–91. doi: 10.1016/0952-8180(94)00001-k. [DOI] [PubMed] [Google Scholar]
- 3.Bisschops R, Saunders R, Dooms C et al. Implementing capnography to help improve patient safety during procedural sedation: quality improvement in a high-volume gastroenterology department. Eur J Gastroenterol Hepatol. 2021;33:e522–e528. doi: 10.1097/MEG.0000000000002144. [DOI] [PubMed] [Google Scholar]
- 4.Aldrete J A, Kroulik D. A postanesthetic recovery score. Anesth Analg. 1970;49:924–934. [PubMed] [Google Scholar]
- 5.Apgar V. A proposal for a new method of evaluation of the newborn infant. Curr Res Anesth Analg. 1953;32:260–267. [PubMed] [Google Scholar]
- 6.Aldrete J A. Modifications to the postanesthesia score for use in ambulatory surgery. J Perianesth Nurs. 1998;13:148–155. doi: 10.1016/s1089-9472(98)80044-0. [DOI] [PubMed] [Google Scholar]
- 7.DE-Quadros L G, Kaiser-Júnior R L, Felix V N et al. Colonoscopy: randomized comparative study of insufflation with carbon dioxide versus air. Arq Bras Cir Dig. 2017;30:177–181. doi: 10.1590/0102-6720201700030004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Marshall S I, Chung F. Discharge criteria and complications after ambulatory surgery. Anesth Analg. 1999;88:508–517. doi: 10.1097/00000539-199903000-00008. [DOI] [PubMed] [Google Scholar]