

A 40-year-old woman underwent piecemeal cold snare polypectomy (p-CSP) for a 25-mm sessile serrated lesion (SSL) in the ascending colon. The lesion was removed after acetic acid spraying and narrow-band imaging (NBI). The 6-month surveillance colonoscopy revealed a scar in the ascending colon ( Video 1 , Fig. 1 ). The remnant lesion was unclear on white light imaging. After 3 % acetic acid solution spraying, NBI showed a 1-mm white flat area at the center of the scar ( Fig. 2 ). Magnified NBI demonstrated a serrated structure in the white area ( Fig. 3 ). The diminutive lesion was diagnosed as a remnant SSL and removed using cold forceps polypectomy. Histopathological examination revealed serrated tissue similar to the initially resected SSL ( Fig. 4 ).
Fig. 1 .
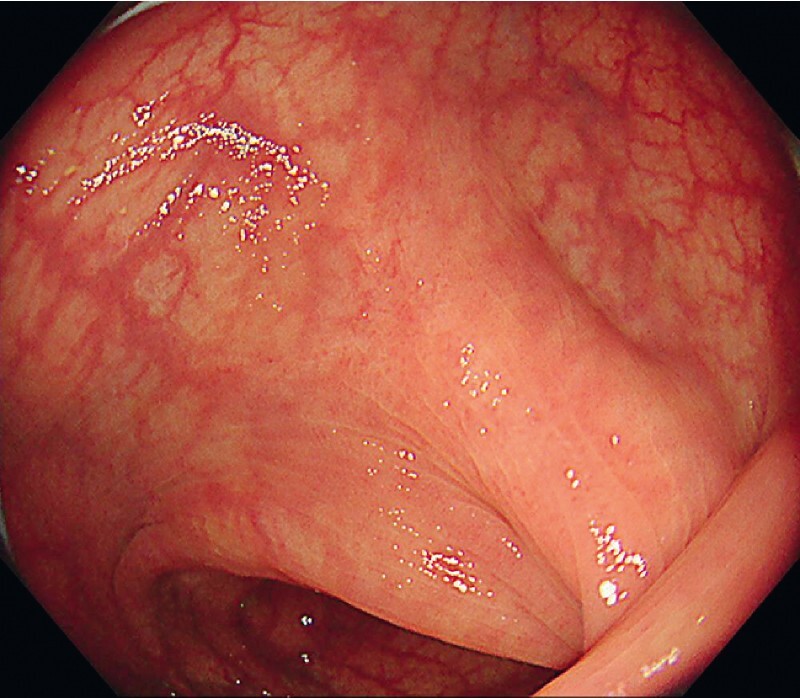
Surveillance colonoscopy after piecemeal cold snare polypectomy for sessile serrated lesions revealing a scar in the ascending colon of a 40-year-old woman.
Fig. 2 .

After 3 % acetic acid solution spraying, narrow-band imaging reveals a 1-mm flat white area at the center of the scar.
Fig. 3 .
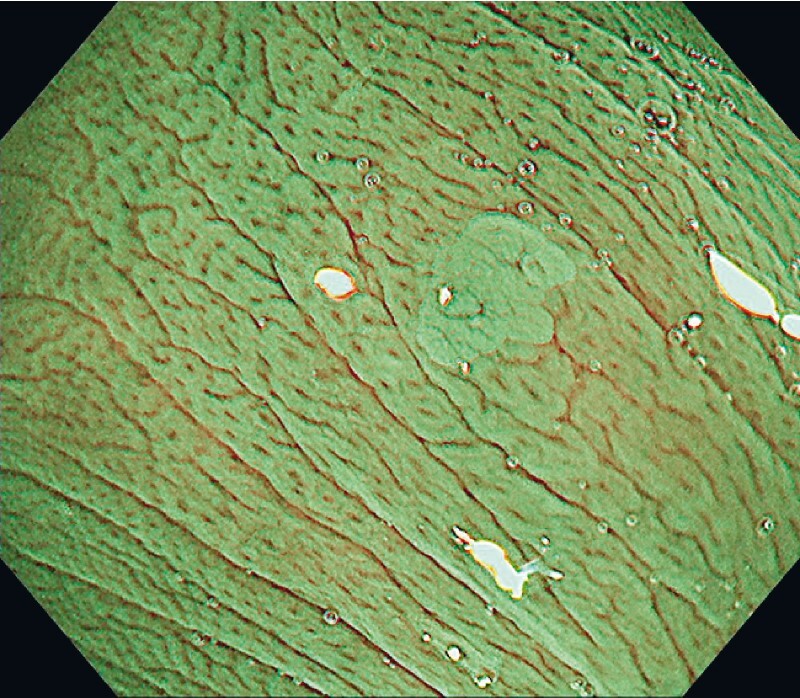
Magnifying narrow-band image showing the serrated structure of the white area.
Fig. 4 .
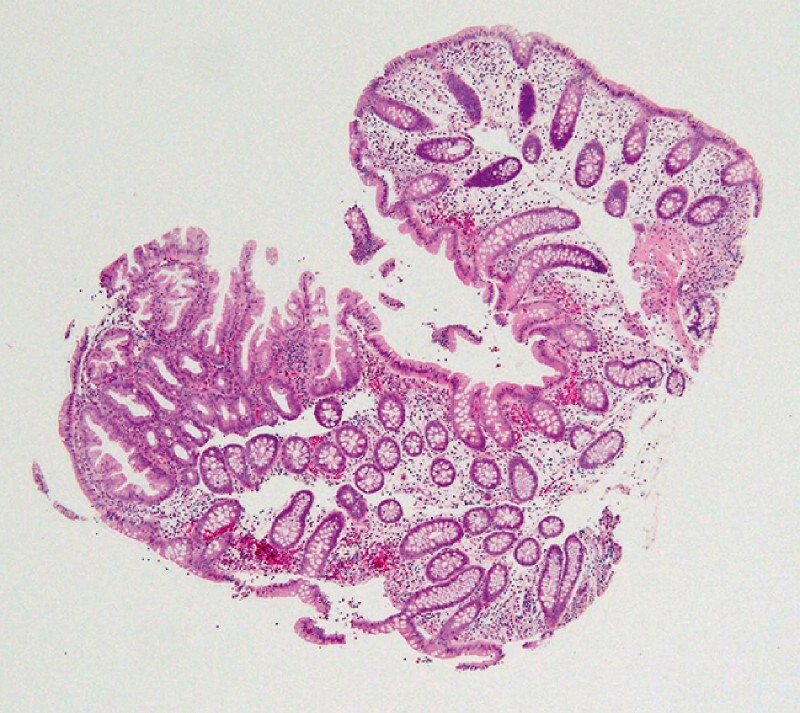
Histopathology examination revealing serrated tissue similar to the initially resected sessile serrated lesion.
Video 1 A remnant sessile serrated lesion after piecemeal cold snare polypectomy was detected using acetic acid spraying and narrow-band imaging. Video text: Colonoscopy showed a 25-mm sessile serrated lesion in the ascending colon. Acetic acid was sprayed over the lesion. The lesion was removed by piecemeal cold snare polypectomy. Surveillance colonoscopy showed a scar in the ascending colon. The remnant lesion was unclear on white light imaging and narrow-band imaging. Acetic acid was sprayed over the scar. A diminutive flat white lesion was detected at the center of the scar. Magnifying narrow-band imaging showed that the white lesion had a serrated structure. The remnant lesion was removed by cold forceps polypectomy. Histopathology revealed serrated tissue.
SSL is a recognized precursor of colorectal cancer through the serrated pathway 1 and requires removal, and p-CSP is reportedly a safe and effective endoscopic resection technique for it 2 3 . However, piecemeal endoscopic removal carries the risk of recurrence. Moreover, the long-term outcome after p-CSP for SSL remains unknown. Despite the use of NBI, few remnant SSLs may be overlooked, and the recurrence rate after p-CSP may be underestimated due to difficulty of detection 4 . The usefulness of acetic acid spray and NBI for removing SSL was previously reported 5 . Acetic acid spray and NBI enable distinction of the SSL from the surrounding normal mucosa by the acetowhitening reaction, resulting in efficient endoscopic delineation. In our case, a diminutive residual SSL was successfully detected using NBI after acetic acid spraying. The use of acetic acid and NBI after the identification of the scar after piecemeal endoscopic removal of SSL can improve the detection of residual tumour.
Footnotes
Competing interests The authors declare that they have no conflict of interest.
References
- 1.Nguyen L H, Goel A, Chung D C. Pathways of colorectal carcinogenesis. Gastroenterology. 2020;158:291–302. doi: 10.1053/j.gastro.2019.08.059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kimoto Y, Sakai E, Inamoto R et al. Safety and Efficacy of cold snare polypectomy without submucosal injection for large sessile serrated lesions: a prospective study. Clin Gastroenterol Hepatol. 2022;20:e132–e138. doi: 10.1016/j.cgh.2020.10.053. [DOI] [PubMed] [Google Scholar]
- 3.van Hattem W A, Shahidi N, Vosko S et al. Piecemeal cold snare polypectomy versus conventional endoscopic mucosal resection for large sessile serrated lesions: a retrospective comparison across two successive periods. Gut. 2021;70:1691–1697. doi: 10.1136/gutjnl-2020-321753. [DOI] [PubMed] [Google Scholar]
- 4.Jung Y, Moon J R, Jeon S R et al. Usefulness of narrow-band imaging for the detection of remnant sessile-serrated adenoma (SSA) tissue after endoscopic resection: the KASID multicenter study. Surg Endosc. 2021;35:5217–5224. doi: 10.1007/s00464-020-08016-2. [DOI] [PubMed] [Google Scholar]
- 5.Yabuuchi Y, Hosotani K, Morita S et al. Effective endoscopic delineation with acetic acid spray and narrow band imaging in underwater endoscopic mucosal resection for sessile serrated lesion. Am J Gastroenterol. 2022;117:840. doi: 10.14309/ajg.0000000000001694. [DOI] [PubMed] [Google Scholar]