

Abstract
Background and study aims Training in endoscopy is a key objective of gastroenterology residency. There is currently no standardized or systematic training approach. This study evaluated and compared the current status of gastrointestinal endoscopy training programs in all teaching hospitals in the Netherlands from a resident perspective.
Materials and methods A national online survey with open and closed questions on gastrointestinal endoscopy training was administered to all gastroenterology residents (N = 180) in the eight educational regions in the Netherlands.
Results One hundred residents who had already started endoscopy training were included in the analyses. Sixty-five residents (65 %) were satisfied with their endoscopy training program. Participation in a preclinical endoscopy course was mandatory in seven of eight educational regions. Residents from the region without a mandatory endoscopy training course were significantly less likely to be satisfied with their endoscopy training program (32 %, P = .011). Criteria used to determine the level of supervision differed greatly between teaching hospitals (e. g. assessed endoscopy competence, predefined period of time or number of procedures). Only 26 residents (26 %) reported uniformity in teaching methods and styles between different supervising gastroenterologists in their teaching hospital.
Conclusions Although most gastroenterology residents were satisfied with the endoscopy training program and endoscopy supervision in their teaching hospital, this study identified considerable local and regional variability. Future studies should be conducted to evaluate the trainers’ perspective and trainers’ behavior during endoscopy training sessions, which might eventually lead to the development of best practices regarding endoscopy training, including standardization of training programs and supervision methods.
Introduction
During the past decades, the field of gastrointestinal endoscopy has been developing rapidly. In this fast-moving field, effective endoscopy training is essential to achieve resident competency in performing endoscopy. In the teaching of procedural skills in gastrointestinal endoscopy, the focus is gradually moving worldwide from the use of threshold numbers toward an individualized, competency-based approach 1 .
In 2018 the Netherlands Society of Gastroenterology and Hepatology developed a new, national, competency-based gastroenterology curriculum 2 . This curriculum has been implemented in all eight educational regions in the Netherlands. The duration of gastroenterology residency is variable, ranging from 65 to 72 months, including 20 months of internal medicine training, and depending on the residents’ individual competencies. Entrustable Professional Activities (EPAs) are the cornerstone of this new curriculum, and are defined as units of professional practice that capture essential competencies. Residents must become proficient before undertaking these activities independently 3 . An entrustment decision to certify for an endoscopy-related EPA is based on several Direct Observation of Procedural Skills (DOPS) evaluations of individual endoscopic procedures and made by multiple endoscopy trainers 2 4 .
Residents start performing basic endoscopic procedures in the first year of gastroenterology residency. There is currently no standardized or systematic teaching approach toward endoscopy training 1 . Despite its well-established value in practical skills development in the early training phase 1 5 , simulation-based training in endoscopy is currently not incorporated in the national gastroenterology training curriculum 2 . Residents usually learn to perform endoscopic procedures on patients under direct supervision and feedback from different attending gastroenterologists. After completing a specified level of training, residents are declared capable of performing endoscopic procedures under indirect supervision (EPA level 3). Although the national gastroenterology curriculum does provide criteria for determining the required level of endoscopy supervision, based on EPA levels 2 , the extent and manner of which these subjective criteria are used in clinical practice are currently unclear.
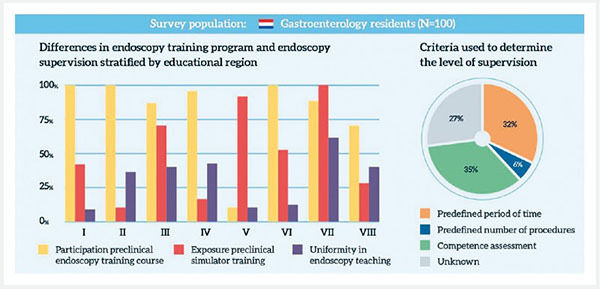
To provide a starting point for developing future best practices regarding endoscopy training, the present study aimed to evaluate and compare the current status of gastrointestinal endoscopy training programs in all teaching hospitals in the Netherlands from a resident perspective. Second, this study examined the satisfaction of gastroenterology residents with their endoscopy training program and endoscopy supervision ( infographic ).
Materials and methods
Design, procedure and participants
All first- (GRY-1), second- (GRY-2), third- (GRY-3) and fourth gastroenterology residency year (GRY-4) trainees in the Netherlands were invited to participate in an online survey during the annual National Resident Education Program in January 2021. The survey was built and study data were collected using REDCap (Research Electronic Data Capture), which is a secure web application for building and managing online databases and surveys. All residents received an email with a link to the survey. After a single reminder 2 weeks after the initial invitation, data collection ceased 4 weeks later.
Survey
A 56-item survey (Appendix) was developed by the research team with input from gastroenterologists specialized in endoscopy teaching and from experts in postgraduate medical education. Survey questions were formulated considering the current national gastroenterology curriculum, implemented in 2018, and applicable EPAs 2 . Questions were open- and closed-ended and were presented as single answer, multiple choice, 5-point Likert scale (ranging from 1 – “strongly disagree” to 5 – “strongly agree”), and free-text questions. The survey focused on the following domains: demographic characteristics, current endoscopy training program, and perceived quality of endoscopy supervision. The survey was reviewed and approved for distribution by the Medical Ethical Committee of Isala Hospital, Zwolle, the Netherlands (study number: 201125). All participants gave written informed consent.
Statistical analysis
Unanswered questions were regarded as missing data in the analyses. For the questions with a 5-point Likert scale, the data were dichotomized with “agree” and “strongly agree” taken as positive, and “neutral,” “disagree” and “strongly disagree” taken as negative. Pearson’s χ 2 test and one-way ANOVA test were used to compare quantitative variables between the eight educational regions in the Netherlands. P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS Statistics version 26 (IBM, New York, United States).
Results
The survey was distributed to 180 gastroenterology residents. All 26 teaching hospitals in the Netherlands were represented, except one. Nineteen residents had not started formal endoscopy training yet; for those residents the questionnaire ended after question 8. One hundred participants who had already started their endoscopy training program were included in the analyses. Baseline characteristics are summarized in Table 1 . To ensure participant anonymity, educational regions are presented as Roman numbers (I-VIII). Mean (standard deviation) participant age was 33.1 (2.5) years; 68 % were female. The group comprised 15 %, 36 %, 26 % and 23 % from GRY-1, GRY-2, GRY-3 and GRY-4, respectively.
Table 1. Demographic characteristic of participants performing gastrointestinal endoscopy stratified by educational region.
| Total (N = 100) |
I (N = 13) |
II (N = 10) |
III (N = 11) |
IV (N = 15) |
V (N = 19) |
VI (N = 15) |
VII (N = 6) |
VIII (N = 11) |
P
value |
|
| Mean age, years (SD) | 33.1 (2.5) | 32.5 (3.0) | 33.6 (1.3) | 32.9 (2.4) | 34.2 (3.4) | 32.8 (2.6) | 32.4 (1.4) | 34.0 (2.0) | 32.8 (2.2) | .457 |
| Female, N (%) | 68 (68) | 9 (69) | 9 (90) | 8 (73) | 9 (60) | 11 (58) | 10 (67) | 4 (67) | 8 (73) | .801 |
| Year of training, N (%) | ||||||||||
|
15 (15) | 3 (23) | 3 (30) | 2 (18) | 1 (7) | 3 (16) | 2 (13) | 1 (17) | 0 (0) | |
|
36 (36) | 5 (39) | 2 (20) | 5 (46) | 3 (20) | 6 (32) | 7 (47) | 1 (17) | 7 (64) | |
|
26 (26) | 3 (23) | 3 (30) | 3 (27) | 6 (40) | 5 (26) | 2 (13) | 2 (33) | 2 (18) | |
|
23 (23) | 2 (15) | 2 (20) | 1 (9) | 5 (33) | 5 (26) | 4 (27) | 2 (33) | 2 (18) | |
|
Statistics: Pearson’s χ
2
test and one-way ANOVA test.
N, number of participants; SD, standard deviation; GRY, gastroenterology residency year. | ||||||||||
Current endoscopy training program
Almost all participants performed esophagogastroduodenoscopies (98 %) and colonoscopies (93 %) in the first phase of endoscopy training ( Table 2 ). Seventy-two residents (72 %) reported to have performed sigmoidoscopies in this phase. Overall, the large majority of residents (65 %) “agreed” (Likert scale 4–5) that they were satisfied with the endoscopy training program offered by their teaching hospital. The most mentioned positive aspects were the high exposure of endoscopic procedures and the approachability of endoscopy trainers. Frequently mentioned points for improvement were the lack of discussion between the trainer and resident before and after the endoscopy training, and the lack of uniformity between different endoscopy trainers, using variable teaching methods and styles. The highest satisfaction rate was seen in educational region VIII (91 %). Residents in educational region V were significantly less likely to be satisfied compared to the other regions (32 %, P = .011). Seventy-six residents (76 %) had participated in a 2-day preclinical endoscopy course. Almost all of these course participants (96 %) “agreed” (Likert scale 4–5) that such a preclinical endoscopy course was useful in preparing them for performing endoscopic procedures on patients. Participation in a preclinical endoscopy course was mandatory in all educational regions, except for residents in region V. In this region, only two residents (11 %) attended an endoscopy course prior to hands-on training, compared to 73 % to 100 % in the other regions ( P < .001). The free-text responses revealed that lacking a preclinical endoscopy course was the most mentioned point for improvement regarding the endoscopy training program by residents in educational region V. This point was not mentioned by residents from the other educational regions. Fifty-one gastroenterology residents (51 %) had exposure to preclinical simulator training apart from a formal training course, most of whom (73 %) performed ≤ 20 simulator procedures. Exposure to simulator training apart from a formal training course was significantly more common in educational regions III (72 %), V (89 %), and VII (100 %), compared to other regions (ranging 10 % to 53 %, P < .001). Thirty-six participants who had had this training (71 %) perceived it as beneficial for developing endoscopy skills prior to endoscopy training on patients.
Table 2. Differences in endoscopy training program stratified by educational region.
|
Total
(N = 100) |
I
(N = 13) |
II
(N = 10) |
III
(N = 11) |
IV
(N = 15) |
V
(N = 19) |
IV
(N = 15) |
VII
(N = 6) |
VIII
(N = 11) |
P
value |
|
| First 50 endoscopies 1 | ||||||||||
|
98 (98) | 12 (92) | 10 (100) | 11 (100) | 15 (100) | 18 (95) | 15 (100) | 6 (100) | 11 (100) | |
|
72 (72) | 11 (85) | 7 (70) | 5 (45) | 14 (93) | 6 (32) | 15 (100) | 4 (67) | 10 (91) | |
|
93 (93) | 13 (100) | 7 (70) | 10 (91) | 15 (100) | 17 (89) | 15 (100) | 5 (83) | 11 (100) | |
| Satisfaction endoscopy training program 2 | 65 (65) | 11 (85) | 8 (80) | 9 (82) | 8 (53) | 6 (32) | 9 (60) | 4 (67) | 10 (91) | .011 |
| Participation preclinical endoscopy course 1 | 76 (76) | 13 (100) | 10 (100) | 9 (82) | 14 (93) | 2 (11) | 15 (100) | 5 (83) | 8 (73) | < .001 |
| Satisfaction preclinical endoscopy course 2 | 73 (96) | 13 (100) | 10 (100) | 8 (89) | 14 (100) | 2 (100) | 14 (93) | 4 (80) | 8 (100) | .446 |
| Exposure preclinical simulator training 1 | 51 (51) | 5 (39) | 1 (10) | 8 (72) | 3 (20) | 17 (89) | 8 (53) | 6 (100) | 3 (27) | < .001 |
| Number of simulator procedures 1 | ||||||||||
|
17 (33) | 3 (60) | 0 (0) | 3 (38) | 3 (100) | 0 (0) | 5 (63) | 1 (17) | 2 (67) | |
|
20 (39) | 1 (20) | 0 (0) | 1 (13) | 0 (0) | 9 (53) | 3 (38) | 5 (83) | 1 (33) | |
|
13 (26) | 1 (20) | 1 (100) | 4 (50) | 0 (0) | 7 (41) | 0 (0) | 0 (0) | 0 (0) | |
|
1 (2) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (6) | 0 (0) | 0 (0) | 0 (0) | |
| Satisfaction simulator training 2 | 36 (71) | 3 (60) | 1 (100) | 6 (75) | 1 (33) | 12 (71) | 5 (63) | 6 (100) | 2 (67) | .594 |
|
Statistics: Pearson’s χ
2
test; N = number of participants
EGD, esophagogastroduodenoscopy. | ||||||||||
Number (percentage) of participants the statement applied to.
Number (percentage) of participants that ‘agreed’ (Likert scale 4–5) with the statement.
Perceived quality of endoscopy supervision
The overall perception of the quality of endoscopy supervision was positive: 72 % of the residents “agreed”’ (Likert scale 4–5) that they were satisfied with the endoscopy supervision of attending gastroenterologists in their teaching hospital ( Table 3 ). The satisfaction rate was lowest in region V (47 %). Regional differences were not statistically significant ( P = .131). The most reported characteristics of an excellent endoscopy teacher were: calm, patient, approachable, motivating and able to instruct verbally without taking over the scope. Seventy-three residents (73 %) perceived attending gastroenterologists in their teaching hospital capable of teaching gastrointestinal endoscopic skills, despite considerable variation in teaching methods and styles; only 26 % reported uniformity in endoscopy supervision between supervisors from their teaching hospital. The approachability of endoscopy supervisors varied between the educational regions. According to residents in the educational regions IV and V, supervisors were significantly less approachable for questions (67 % and 63 %, respectively) compared to the other regions (84.0 %, P = .033). Criteria used to determine the level of supervision differed considerably between teaching hospitals. Most residents reported that the transition from direct (EPA level 2) to indirect supervision (EPA level 3) was based on assessment of endoscopic competence (35 %) or a predefined period of time (32 %). The predefined period of direct supervision varied between teaching hospitals (median 12 weeks; interquartile range 10 to 18 weeks). Only six residents (6 %) noted that the period of direct supervision was based on threshold numbers (median 50 procedures; interquartile range 40–50 procedures). Moreover, 27 participants (27 %) did not know the exact criteria used for determining the level of supervision. Most participants (56 %) reported that supervising gastroenterologists rarely observed a complete procedure once the resident was allowed to perform gastrointestinal endoscopies under indirect supervision. Only a few participants (8 %) experienced to go beyond the limits of their capacities during endoscopic procedures. A discussion between the supervisor and resident prior to an endoscopy training session to determine the endoscopic experience and knowledge of the resident and setting learning goals and objectives, was reported by 23 % of the participants when directly supervised and 20 % when indirectly supervised. Only nine residents (10 %) evaluated predefined learning objectives after the endoscopy during a debriefing with the attending gastroenterologist.
Table 3. Differences in endoscopy supervision stratified by educational region.
|
Total
(N = 100) |
I
(N = 13) |
II
(N = 10) |
III
(N = 11) |
IV
(N = 15) |
V
(N = 19) |
VI
(N = 15) |
VII
(N = 6) |
VIII
(N = 11) |
P
value |
|
| Satisfaction endoscopy supervision 1 | 72 (72) | 12 (92) | 7 (90) | 9 (82) | 11 (73) | 9 (47) | 10 (67) | 4 (67) | 10 (91) | .131 |
| Endoscopic skills improvement | 73 (73) | 10 (77) | 7 (70) | 9 (82) | 13 (87) | 8 (42) | 12 (80) | 6 (100) | 8 (73) | .055 |
| Uniform teaching methods 1 | 26 (26) | 1 (8) | 3 (30) | 4 (36) | 6 (40) | 2 (11) | 2 (13) | 4 (67) | 4 (36) | .053 |
| Supervisor approachability 1 | 84 (84) | 12 (92) | 9 (90) | 10 (91) | 10 (67) | 12 (63) | 15 (100) | 6 (100) | 10 (91) | .033 |
| Transition direct to indirect supervision 2 | ||||||||||
|
32 (32) | 9 (69) | 1 (10) | 0 (0) | 6 (40) | 4 (21) | 3 (20) | 5 (83) | 4 (36) | |
|
6 (6) | 1 (8) | 2 (20) | 1 (9) | 0 (0) | 1 (5) | 1 (7) | 0 (0) | 0 (0) | |
|
35 (35) | 3 (23) | 2 (20) | 5 (46) | 5 (33) | 7 (37) | 7 (47) | 1 (17) | 5 (46) | |
|
27 (27) | 0 (0) | 5 (50) | 5 (46) | 4 (27) | 7 (37) | 4 (27) | 0 (0) | 2 (18) | |
| Endoscopy observation indirect supervision 1 | 56 (56) | 6 (46) | 6 (60) | 5 (46) | 8 (53) | 13 (68) | 7 (47) | 4 (67) | 7 (64) | .879 |
| Beyond the limit of capacities 1 | 8 (8) | 0 (0) | 0 (0) | 1 (9) | 2 (14) 3 | 2 (11) | 2 (13) | 0 (0) | 1 (9) | .778 |
| Pre-discussion direct supervision 1 | 22 (23) | 3 (25) 3 | 3 (30) | 4 (36) | 3 (21) 3 | 1 (6) 3 | 2 (13) | 1 (17) | 5 (46) | .244 |
| Pre-discussion indirect supervision 1 | 19 (20) | 4 (33) 3 | 3 (30) | 2 (18) | 1 (7) 3 | 4 (22) 3 | 3 (20) | 0 (0) | 2 (18) | .670 |
| Debriefing 1 | 9 (10) | 2 (17) 3 | 1 (10) | 3 (27) | 1 (7) | 0 (0) 3 | 2 (13) | 0 (0) | 0 (0) 3 | .242 |
Statistics: Pearson’s χ 2 test.
N, number of participants.
Number (percentage) of participants that “agreed” (Likert scale 4–5) with the statement.
Number (percentage) of participants the statement applied to.
Missing data.
Discussion
In this national survey assessing perceptions of Dutch gastroenterology residents on their endoscopy training, most residents were satisfied with the endoscopy training program and endoscopy supervision in their teaching hospital, despite the presence of considerable local and regional variability. The main differences we observed concerned: 1. participation in a preclinical endoscopy training course; 2. exposure to endoscopy simulator training; 3. criteria used to determine the level of supervision; and 4. lack of uniformity in teaching methods and styles between different endoscopy supervisors in the same hospital.
Participation in a preclinical endoscopy training course, consisting of didactic lectures on basic endoscopic techniques followed by simulator training sessions, was mandatory in seven of eight educational regions. Although the exact impact of the COVID-19 pandemic is unclear, we assume that under normal circumstances endoscopy course participation would have been higher than currently reported in these regions. Almost all participants found a preclinical endoscopy course useful in preparing them for performing endoscopic procedures on patients. Gastroenterology residents in the educational region without a mandatory endoscopy training course, region V, were significantly less likely to be satisfied with their endoscopy training program. Although there are many factors that influence residents’ satisfaction, based on the free-text responses we assume that the lower satisfaction in region V was mainly caused by the lack of a preclinical endoscopy course. Only a few studies investigated the impact of a preclinical endoscopy training course in preparation for performing endoscopic procedures on patients. Theoretical knowledge, endoscopy performance 6 7 8 and DOPS scores 6 7 improved after training course completion.
Although the utility of simulation-based training in the early phase of gastrointestinal endoscopy learning is well established 1 5 9 , our findings demonstrate that access to simulator training apart from a formal training course is limited. Due to the high costs of endoscopy simulators, training facilities are only available in a few teaching hospitals. Compared to trainees in most other regions, participants in educational region V, the region without a mandatory endoscopy course, had significantly higher exposure to preclinical simulator training apart from a formal endoscopy training course. Most participants, however, performed ≤ 20 simulator procedures. One study demonstrated that the learning effect of simulator training ceased after 60 simulator colonoscopies 10 , indicating that most residents in educational region V presumably did not reach their learning plateau. It is unclear to what extent residents who performed simulator procedures apart from a formal training course received augmented feedback and instruction. Such feedback has been identified as a critical feature for effective learning in a simulation-based setting 5 11 12 . To overcome regional disparities in the development of basic endoscopic skills for novice gastrointestinal endoscopists, we propose that preclinical simulator training, including providing structured feedback, should be incorporated in the national gastroenterology training curriculum.
The criteria used to determine the level of supervision differed considerably between teaching hospitals, and some are still focused on a predefined period of time or minimum number of performed procedures. Notably, a considerable proportion of the participants did not know the exact criteria used for determining the level of supervision, which may implicate that local criteria are not always specified. The current competency-based gastroenterology curriculum, however, recommends the use of DOPS to assess the level of endoscopy competence. A few endoscopy programs in the United Kingdom 13 and the United States 14 15 also describe an integrated direct observation assessment tool in their curricula 16 , although the extent to which these tools are used in clinical practice is unclear. Possible barriers to widespread usage of competence-assessment tools such as DOPS may be supervisors’ lack of time, resistance to change, and scheduling difficulties. Since the use of threshold numbers is considered a poor surrogate marker for competence 1 , endoscopy training programs should be encouraged to identify and overcome possible barriers and use competence-assessment tools in clinical practice to enhance individualized learning 16 .
Within the current endoscopy training programs, residents are primarily trained one-on-one according to the traditional apprenticeship model. The lack of uniformity in endoscopy supervision and the absence of a standardized teaching approach to procedural training, identified in this study, may lead to conflicting messages that create confusion in learners 17 . The Dreyfus model of skill acquisition postulates that when individuals acquire a skill through external instruction and practice, they normally progress through five developmental stages, from novice to expert 18 . The beginning and intermediate stages are characterized by analytical decision making based on strict rules and context, which should be applied uniformly by supervisors. With experience, residents develop more intuition in decision making, gradually shifting to unconscious performance that relies on implicit knowledge 18 . In a recent Delphi consensus study, endoscopy education experts identified 10 essential gastrointestinal endoscopy teaching competencies 19 . Essential competencies included discussing patient history and plans before a procedure, reviewing the procedure afterwards and providing structured feedback to the resident. Our results indicate that these teaching competencies are rarely applied in clinical endoscopy supervision practice. Although future research is needed to determine its impact in clinical endoscopy supervision practice, it is likely that uniform teaching methods and styles can contribute to improvement of the quality of endoscopy training in gastroenterology residency.
The strengths of this study include the high response rate and the nationwide design, with participation of residents from all educational regions in the Netherlands. We acknowledge the following limitations. Firstly, this survey does not cover the trainers’ perspective on endoscopy teaching which would be interesting to compare with the residents’ point of view. Second, in the free-text response fields some residents noted that the limited number of endoscopic procedures in their teaching hospital negatively affected the development of their endoscopic skills. Because our survey did not collect information about the number of performed endoscopic procedures, we cannot make a comparative analysis between the different regions with regard to the number of procedures per trainee. Finally, the survey population was limited to gastroenterology residents in the Netherlands. As in some countries different training models are used extrapolation of the results may not always be possible 20 . A survey among gastroenterology physicians in 16 European countries revealed considerable differences both among and within the countries. One of the recommendations of this study was that national regulatory authorities should promote greater standardization of educational programs 20 . In our opinion, this emphasizes the importance of evaluating endoscopy training programs, both at an international and a national level.
Conclusions
In conclusion, this national survey identified considerable local and regional variability in gastrointestinal endoscopy training programs and teaching methods used in teaching hospitals in the Netherlands. Future studies should be conducted to evaluate the trainers’ perspective and the trainers’ behavior during endoscopy training sessions, which might eventually lead to the development of best practices regarding endoscopy training, including standardization of training programs and supervision methods.
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Supplementary material :
References
- 1.Ekkelenkamp V E, Koch A D, de Man R A et al. Training and competence assessment in gastrointestinal endoscopy: a systematic review. Gut. 2016;65:607–615. doi: 10.1136/gutjnl-2014-307173. [DOI] [PubMed] [Google Scholar]
- 2.Uitgave van de Nederlandse Vereniging voor Maag-Darm-Leverartsen NOVUM Landelijk Opleidingsplan Voor De Specialistenopleiding Maag-Darm-Leverziekten 2018https://www.knmg.nl/web/file?uuid=6b17510e-03c7-4c31-b9af-1587ae868ae9&owner=5c945405-d6ca-4deb-aa16-7af2088aa173&contentid=73016&elementid=2178494Accessed 2022 Apr 14
- 3.Ten Cate O. Entrustability of professional activities and competency-bases training. Med Educ. 2005;39:1176–1177. doi: 10.1111/j.1365-2929.2005.02341.x. [DOI] [PubMed] [Google Scholar]
- 4.Barton J R, Corbett S, van der Vleuten C P. The validity and reliability of a Direct Observation of Procedural Skills assessment tool: assessing colonoscopic skills of senior endoscopists. Gastrointest Endosc. 2012;75:591–597. doi: 10.1016/j.gie.2011.09.053. [DOI] [PubMed] [Google Scholar]
- 5.Khan R, Plahouras J, Johnston B C et al. Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy. Cochrane Database Syst Rev. 2018:CD008237. doi: 10.1002/14651858.CD008237.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Suzuki N, Thomas-Gibson S, Vance M et al. Efficacy of an accelerated colonoscopy training week: audit from one national colonoscopy training center in the UK. Dig Endosc. 2006;18:288–293. [Google Scholar]
- 7.Thomas-Gibson S, Bassett P, Suzuki N et al. Intensive training over 5 days improves colonoscopy skills long-term. Endoscopy. 2007;39:818–824. doi: 10.1055/s-2007-966763. [DOI] [PubMed] [Google Scholar]
- 8.Götzberger M, Rösch T, Geisenhof S et al. Effectiveness of a novel endoscopy training concept. Endoscopy. 2011;43:802–807. doi: 10.1055/s-0030-1256372. [DOI] [PubMed] [Google Scholar]
- 9.Walsh C M, Sherlock M E, Ling S C et al. Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy. Cochrane Database Syst Rev. 2012;6:CD008237. doi: 10.1002/14651858.CD008237.pub2. [DOI] [PubMed] [Google Scholar]
- 10.Koch A D, Ekkelenkamp V E, Haringsma J et al. Simulated colonoscopy training leads to improved performance during patient-based assessment. Gastrointest Endosc. 2015;81:630–636. doi: 10.1016/j.gie.2014.09.014. [DOI] [PubMed] [Google Scholar]
- 11.Mahmood T, Darzi A. The learning curve for a colonoscopy simulator in the absence of any feedback: no feedback, no learning. Surg Endosc. 2004;18:1224–1230. doi: 10.1007/s00464-003-9143-4. [DOI] [PubMed] [Google Scholar]
- 12.Hatala R, Cook D A, Zendejas B et al. Feedback for simulation-based procedural skills training: a meta-analysis and critical narrative synthesis. Adv Health Sci Educ Theory Pract. 2014;19:251–272. doi: 10.1007/s10459-013-9462-8. [DOI] [PubMed] [Google Scholar]
- 13.Mehta T, Dowler K, McKaig B et al. Development and roll out of the JETS e-portfolio: a web based electronic portfolio for endoscopists. Frontline Gastroenterol. 2011;2:35–42. doi: 10.1136/fg.2010.003269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Patel S G, Keswani R, Elta G et al. Status of competency-based medical education in endoscopy training: a nationwide survey of US ACGME-accredited gastroenterology training programs. Am J Gastroenterol. 2015;110:956–962. doi: 10.1038/ajg.2015.24. [DOI] [PubMed] [Google Scholar]
- 15.Han S, Obuch J C, Duloy A M et al. Prospective multicenter study evaluating endoscopy competence among gastroenterology trainees in the era of the next accreditation system. Acad Med. 2020;95:283–292. doi: 10.1097/ACM.0000000000002885. [DOI] [PubMed] [Google Scholar]
- 16.Khan R, Zheng E, Wani S B et al. Colonoscopy competence assessment tools: a systematic review of validity evidence. Endoscopy. 2021;53:1235–1245. doi: 10.1055/a-1352-7293. [DOI] [PubMed] [Google Scholar]
- 17.Huang C, Hopkins R, Huang K et al. Standardizing endoscopy training: a workshop for endoscopy educators. MedEdPORTAL. 2020;16:11015. doi: 10.15766/mep_2374-8265.11015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dreyfus S E. The five-stage model of adult skill acquisition. Bull Sci Technol Soc. 2004;24:177–181. [Google Scholar]
- 19.Kumar N L, Smith B N, Lee L S et al. Best practices in teaching endoscopy based on a Delphi survey of gastroenterology program directors and experts in endoscopy education. Clin Gastroenterol Hepatol. 2020;18:574–579. doi: 10.1016/j.cgh.2019.05.023. [DOI] [PubMed] [Google Scholar]
- 20.Maida M, Alrubaiy L, Bokun T et al. Current challenges and future needs of clinical and endoscopic training in gastroenterology: a European survey. Endosc Int Open. 2020;8:E525–E533. doi: 10.1055/a-1093-0877. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.