

ABSTRACT
Objective:
This study proposes to systematically review the literature and compare data on (1) function, (2) pain, (3) return to sport, and (4) complications after anterior cruciate ligament (ACL) reconstruction with quadriceps tendon autograft (QT) and hamstring tendon autograft (HT).
Methods:
In June 2021, a systematic review of the EMBASE, MEDLINE/PubMed, Cochrane Central Register of Controlled Trials, and LILACS databases was performed, based on PRISMA guidelines. The search strategy included the keywords: “Previous Cruciate Ligament Reconstruction,” “ACL reconstruction,” “quadriceps tendon autograft,” “quadriceps graft,” “Hamstring-Tendon Autografts.” Meta-analyses were performed using Review Manager software (RevMan Web).
Results:
There were no significant differences between the two groups regarding function according to Lysholm score (MD 3.01; CI-0.30, 6.33, p = 0.08), the presence of pain (RR 0.89; CI-0.57, 1.39, p = 0.60), and re-rupture (RR 0.60; IC-0.19, 1.88, p = 0.38).
Conclusion:
QT and HT autografts show comparatively good results in ACL reconstruction without significant differences regarding function, pain, and rupture after surgical intervention. Level of Evidence II, Systematic Review of Level II Studies.
Keywords: Anterior Cruciate Ligament, Hamstring Tendons, Quadriceps Muscle, Tendons
RESUMO
Objetivo:
Revisar sistematicamente a literatura e comparar dados sobre função, dor, retorno ao esporte e complicação após a reconstrução de ligamento cruzado anterior (LCA) com autoenxerto do tendão do quadríceps (TQ) e autoenxerto do tendão dos músculos isquiotibiais (TF).
Métodos:
Em junho de 2021, foi realizada revisão sistemática das bases de dados EMBASE, MEDLINE/PubMed, Cochrane Central Register of Controlled Trials e LILACS, baseada nas diretrizes do Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). A estratégia de pesquisa incluiu as palavras-chave: “Anterior Cruciate Ligament Reconstruction”, “ACL reconstruction”, “quadriceps tendon autograft”, “quadriceps graft” e “Hamstring-Tendon Autografts”. As metanálises foram realizadas usando o software Review Manager (RevMan Web).
Resultados:
Não houve diferenças significativas entre os dois grupos com relação à função pelo escore de Lysholm (MD 3,01; IC-0,30, 6,33, p = 0,08), presença de dor (RR 0,89; IC-0,57, 1,39, p = 0,60) e re-ruptura (RR 0,60; IC-0,19, 1,88, p = 0,38).
Conclusão:
Os autoenxertos de TQ e TF apresentam resultados comparativamente bons na reconstrução do LCA sem diferenças significativas com relação à função, dor e ruptura após a intervenção cirúrgica. Nível de Evidência II, Revisão Sistemática de Estudos de Nível II.
Descritores: Ligamento Cruzado Anterior, Tendões dos Músculos Isquiotibiais, Músculo Quadríceps, Tendões
INTRODUCTION
Anterior cruciate ligament (ACL) injuries are the most common ligament injury to occur in the knee after twisting and rotation, especially during sports activity. 1 ),( 2 ACL injury compromises neuromuscular control and proprioceptive acuity of the knee and may contribute to an increased risk of a secondary injury. 3
After an ACL lesion, the treatment goals are for the patient to return to sports and daily activities without further damage. 1 ),( 2 Treatment may be conservative (physiotherapy or medications) or surgical, with ACL reconstruction using autograft. 1 ),( 2 ),( 4 ),( 5 The choice of treatment depends mainly on factors such as age, sex, level of activity, degree of injury or concomitant lesions and degree of instability. 1 ),( 2 ),( 5
The choice of graft for ACL reconstruction remains a subject of interest among orthopedic surgeons since the ideal graft has not yet been found and this remains a prevalent research topic. 6 ),( 7 Autologous grafts of the hamstrings (TF) and patellar tendon (PT) are the most commonly used for ACL reconstruction. 8 However, as the use of quadriceps tendon (QT) as grafts increases, so does its interest as a topic of scientific research. 6 ),( 8 For these reasons, QT grafts have been proposed as a promising alternative to common grafts in ACL injury surgery. 8
Despite technical advances in ACL reconstruction surgery, there is still a need to improve postoperative results and understand which type of grafts result in lower failure rates and risk of complications and which results in better function, less pain, and shorter return time to sport. 6 ),( 8 Therefore, the objective of this systematic review and meta-analysis is to compare the available evidence on (1) function, (2) pain, (3) return to sport, and (4) complications after reconstruction of the anterior cruciate ligament with autograft of the quadriceps tendon (QT) and hamstring tendon (HT).
METHODS
A systematic review was conducted, in June 2021, based on the recommendations of The Cochrane Handbook of Interventions Reviews 9 ),( 10 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses - PRISMA. A review protocol was published in the International Prospective Register of Systematic Reviews (PROSPERO CRD42021260308).
Data sources and research
One of the researchers (T.N.A.) developed the protocol and defined the research strategies for the databases EMBASE, MEDLINE/PubMed, Cochrane Central Register of Controlled Trials, and LILACS. Data were collected on June 10, 2021. Subsequently, the reference lists of eligible studies were analyzed.
To conduct the search for intervention studies, a strategy was developed with the acronym PICO that focuses on population, intervention, comparison, and outcomes. 11 Thus: P = adults over 18 years of age with complete anterior cruciate ligament injuries; I = quadriceps tendon autograft; C = hamstring autograft; and O = the primary outcome of interest includes pain, function, and re-rupture. Secondary outcomes were: return to sport and complications.
Identification of studies
To search the studies within the databases, the following combinations of keywords were used with the Boolean operators AND and OR:
“Anterior Cruciate Ligament Reconstruction” [Mesh] OR “ACL reconstruction”;
“quadriceps tendon autograft” OR “quadriceps graft”;
“Hamstring-Tendon Autografts.”
Inclusion criteria
Inclusion criteria were as follows: (1) studies performed with humans; (2) adults without previous surgical procedures for anterior cruciate ligament injury; (3) aged over 18 years; (4) randomized clinical trials and cohort studies; (5) clinical studies on ACL reconstruction using quadriceps tendon autograft, single- or double-bundle reconstruction, with or without bone block (quadriceps autograft without bone plug); (6) studies comparing the results of quadriceps tendon autograft versus hamstring autograft (femoral biceps, semitendinosus, and semimembranosus); (7) all procedures were primary ligament reconstructions performed for acute symptoms or chronic ACL deficiency, with or without meniscus injury; (8) articles in English, Spanish, or Portuguese; (9) published between January 2000 and June 2021.
Case reports, expert opinion, registration of clinical trials, reviews, unpublished data, animal or in vitro experiments, and studies conducted on human cadavers were excluded, in addition to studies with less than 12 months of follow-up and studies investigating results after reconstruction of other ligaments.
Data extraction
The stages of the screening of the articles were performed using Rayyan software. 12 Analysis of titles and abstracts and the full reading were performed by two researchers (T.N.A. & J.B.M.C.) independently; any divergences were resolved among the members of the research team. After reading the articles, the following information was collected: author, year, and place of publication; study design and follow-up time of the intervention; details about ACL injury, intervention (QT autograft versus HT); measures of outcomes or results.
Evaluation of the quality and risk of bias
The quality of the studies was evaluated for each outcome investigated using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE - https://gradepro.org/). 13 ),( 14 The quality of the evidence was classified into four categories: high, moderate, low, or very low. 13 ),( 14 The risk of bias in the included studies of the meta-analysis was performed using the ROBINS tool for Risk of Bias in Randomized Trials and Risk of Bias in Non-Randomised Studies.
Statistical analysis
We calculated the risk ratio and mean difference with a 95% confidence interval using the random effect model. Heterogeneity was classified based on the values of I 2 : 25%, low heterogeneity; 50%, moderate heterogeneity; and 90%, high heterogeneity. 10 All statistical analyses were performed with the Review Manager (RevMan Web) software.
RESULTS
Searches in the three databases resulted in 350 articles, and two additional articles were retrieved by manual search in Google Scholar. After removing 59 duplicates, we read 39 articles in full, of which 13 were included 8 ),( 15 )-( 26 (Figure 1). Supplementary Material 2 shows the list of excluded articles and their respective justification.
Figure 1. Flowchart of the screening of the articles.

Table 1 shows the characteristics of the included studies. Four randomized clinical trials 15 ),( 18 ),( 23 ),( 26 and nine cohort studies 8 ),( 16 ),( 17 ),( 19 )-( 22 ),( 24 ),( 25 were included. Studies were conducted in Romania, 15 ),( 25 Germany, 8 ),( 17 ),( 18 Denmark, 23 Mexico, 26 Switzerland, 16 Australia, 19 Korea, 20 Austria, 21 ),( 22 and Turkey. 24 A total of 879 adults with anterior cruciate ligament injury participated in this study. Of these, 422 underwent ACL reconstruction with QT autograft and 457, with HT autograft.
Table 1. Characteristics of the studies on quadriceps tendon autograft versus hamstring autograft for anterior cruciate ligament reconstruction.
| Author, year | Type of study and follow-up | Sample size/sex/age (years) | Surgical technique | Intervention/placebo or control | Outcomes | Adverse events or complications | Approval of the ethics committee |
|---|---|---|---|---|---|---|---|
| CLINICAL TRIALS | |||||||
| Buescu et al., 17 2017 | Parallel randomized clinical trial | N = 48 | Anatomical arthroscopic reconstruction of the ACL in single-bundle | (1) QT (n = 24 patients). | Pain: VAS - patients who required complementary analgesia (n/%) | None | Yes |
| (1) QT 0-1 2h: 12 (50%) | |||||||
| Male: 45 | QT 25-48 h: 4 (16.66%) | ||||||
| Romania | Average follow-up: 0-48 h | Female: 3 | (1) HT (n = 24 patients). | (2) HT 0-1 2h: 18 (75%) | |||
| Age: 28.35 ± 7.19 | HT 25-48 h: 9 (37.50%) | ||||||
| (p = 0.002). | |||||||
| Horstmann et al., 18 2022 | Randomized, controled clinical trial | N = 51 | Press-fit fixation techniques without implant. | (1) QT (n = 24 patients). | Functional results by Lysholm: | Yes | Yes |
| (1) QT Preoperative: 72.3 ± 13.2 | |||||||
| Sex: | QT two years postoperatively: | ||||||
| 90.4 ± 11.9 | |||||||
| Follow-up: 2 years | Male/Female | (2) HT Preoperative: 60.4 ± 18.5 | |||||
| (1) QT: 21/3 | HT two years postoperatively: | ||||||
| Germany | (2) HT: 12/15 | (1) HT (n = 27 patients). | 83.5 ± 17.4 | ||||
| Age: | p < 0.131 | ||||||
| Evaluation: 3, 6, 12, and 24 months after surgery. | (1) QT:24.1 ± 3.6 | Return to sport (in days): | |||||
| (1) QT: 82.1 ± 45.6 | |||||||
| (2) HT:32.7 ± 11.4 | (2) HT: 95.2 ± 45.5 | ||||||
| p < 0.131 | |||||||
| Sinding et al., 23 2020 | Randomized, controled clinical trial | N = 85 | ACL Reconstruction | (1) QT (n = 42 patients). | Function: When comparing the two groups of patients with autograft, 4%-11% less muscle strength was observed during knee extensor at 0 degrees/s (isometric, MVIC) and 60 degrees/s (concentric dynamics) in QT vs. HT, along with knee extensor 4% lower RFD200ms. | NR | Yes |
| Sex: | |||||||
| Male/Female | |||||||
| (1) QT: 25/17 | |||||||
| Denmark | Follow-up: 1 year | (2) HT: 23/20 | (1) HT (n = 43 patients). | Functional Capacity (single leg hop distance - SHD): There was no difference in SHD between HT and QT. | |||
| Age: | |||||||
| (1) QT:28.7 ± 6.4 | |||||||
| (2) HT: 28.3 ± 6.2 | |||||||
| Vilchez-Cavazos et al., 26 2020 | Randomized clinical trial | N = 28 | ACL Reconstruction | (1) QT (n = 14 patients). | Functional results by Lysholm (median and interquartile range): | NR | Yes |
| (1) QT baseline: 75.0 (61.5-83.5) | |||||||
| Sex: | QT 12 months: 95.0 (91.0-100.0) | ||||||
| Male/Female | (2) HT baseline: 61.0 (37.0-74.0) | ||||||
| Follow-up: | (1) QT: 11/2 | HT 12 months: 98.0 (90.0-100.0) | |||||
| Mexico | 2 weeks and 1, 3, 6 and 12 months. | (2) HT: 12/3 | (1) HT (n = 14 patients). | Pain (VAS) (median and interquartile range): | |||
| Age: | (1) QT baseline: 3.0 (1.5-7.0) | ||||||
| (1) QT: 30.64 ± 8.71 | QT 12 months: 0.0 (0.0-1.5) | ||||||
| (2) HT: 28.60 ± 6.74 | (2) HT baseline: 4.0 (3.0-7.0) | ||||||
| HT 12 months: 0.0 (0.0-1.0) | |||||||
| OBSERVATIONAL STUDIES | |||||||
| Akoto et al., 8 2019 | Retrospective cohort study | N = 82 | Isolated ACL reconstruction | (1) QT (n = 41 patients). | Functional results by IKDC scores: | Graft failure: | Yes |
| (1) QT: 86.4 ± 14.2 | (1) QT: n = 3 | ||||||
| Male: 64 | (2) HT: 86.7 ± 10.9 | (2) HT: n = 4 | |||||
| Female: 18 | p = 0.9 | Contralateral ACL rupture: | |||||
| Germany | Follow-up: 12 months | Age: | (1) HT (n = 41 patients). | Functional tests | (1) QT: n = 1 | ||
| (1) QT: 29 ± 10 | (One-Leg Hop test): | (2) HT: n = 2 | |||||
| (1) QT: 96.2 ± 8.5 | Infection: | ||||||
| (2) HT: 28 ± 10 | (2) HT: 95.5 ± 8.5 | (1) QT: n = 1 | |||||
| p = 0.8 | (2) HT: n = 2 | ||||||
| Cavaignac et al., 16 2017 | Cohort study | N = 86 | Isolated ACL reconstruction | (1) QT (n = 45 patients). | Functional results by Lysholm: | QT group, there was 1 re-rupture | Yes |
| (1) QT: 89 ± 6.9 | |||||||
| Male: 45 | (2) HT: 83.1 ± 5.3 | ||||||
| Female: 41 | p < 0.05 | ||||||
| Switzerland | Average follow-up: 3.6 6 0.4 years, and the minimum follow-up was 3 years | Age: | (1) HT (n = 41 patients). | Pain: | In the HT group, there were 2 cases of graft rupture. | ||
| (1) QT: 32.1 ± 8 | (1) QT: 90 ± 6.8 | ||||||
| (2) HT: 30.9 ± 9 | (2) HT: 86 ± 7.2 | ||||||
| p = 0.23 | |||||||
| Häner et al., 17 2016 | Cohort study | N = 51 | ACL Reconstruction homologous autograft (HT and QT) | (1) QT (n = 25 patients). | Functional results by Lysholm: | No rerupture occurred during postoperative follow-up. No early superficial or meniscal infection. | Yes |
| (1) QT: 88 | |||||||
| Sex: | (2) HT: 78.1 | ||||||
| p = 0.06 | |||||||
| Male/Female | |||||||
| Pain: | |||||||
| (1) QT: 17/8 | When kneeling | ||||||
| (1) QT: 7 | |||||||
| Germany | Average follow-up: 24 months | (2) HT: 18/8 | (1) HT (n = 26 patients). | (2) HT: 11 | Lesion was found in either group. | ||
| When squatting | |||||||
| Age: | (1) QT: 7 | ||||||
| Climb stairs | |||||||
| (1) QT: 35.9 ± 10.4 | (1) QT:4 | ||||||
| (2) HT: 4 | |||||||
| (2) HT: 35.8 ± 13.1 | In squats | ||||||
| (2) HT:8 | |||||||
| Johnston et al., 19 2021 | Cohort study | N = 111 | Arthroscopy-assisted ACL reconstruction with femoral tunnel perforated via anteromedial portal | (1) QT (n = 37 patients). | Previous knee pain: | NR | Yes |
| Sex: | (1) QT: 67% | ||||||
| Male/Female | (2) HT: 63% | ||||||
| (1) QT: 29/8 | p = N.S. | ||||||
| Australia | Follow-up: 6 months | (2) HT: 58/16 | (1) HT (n = 74 patients). | Active knee flexion amplitude while standing (p < 0.001), active knee flexion amplitude measured in lateral decubitus (p < 0.001), and passive knee flexion amplitude (p = 0.016) in the HT Group when compared with the QT group. | |||
| Age: | |||||||
| (1) QT: 20.0 (15-34) | |||||||
| (2) HT: 20.5 (15-32) | |||||||
| Lee et al., 20 2016 | Cohort study | N = 96 | ACL Reconstruction | (1) QT (n = 48 patients). | Lysholm scores: | NR | Yes |
| Sex: | (1) QT Preoperative: 70.2 ± 9.6 | ||||||
| Male/Female | QT final follow-up: 92.1 ± 8.7 | ||||||
| (1) QT: 44/4 | (2) HT Preoperative: 69.4 ± 18.0 | ||||||
| Korea | Follow-up: 2 years | (2) HT: 44/4 | (1) HT (n = 48 patients). | HT final follow-up: 88.4 ± 11.9 | |||
| Age: | p = 0.30 | ||||||
| (1) QT: 31.1 (17-57) | The recovery of flexor muscle strength was better in the quadriceps group (86.6% vs. 92.2% at 60 degrees/s, p = 0.22; 87.1% vs. 99.6% at 180 degrees/s, p = 0.01). | ||||||
| (2) HT: 29.9 (17-58) | |||||||
| Ortmaier et al., 21 2021 | Retrospective cohort study | N = 45 patients | ACL Reconstruction homologous autograft (HT and QT) | (1) QT (n = 20 patients). | Knee pain (VAS): Subjective assessments of pain during and after sports worsened significantly for almost all parameters with no significant difference between pre- and postoperative groups. | NR | Yes |
| Sex: | |||||||
| Male/Female | |||||||
| Austria | Follow-up: 12 months | (1) QT: 17/8 | (1) HT (n = 25 patients). | ||||
| (2) HT: 12/8 | Rate of return to sports was 91.3%. | ||||||
| Age (average): 33.4 years | |||||||
| Runer et al., 22 2018 | Prospective cohort study | N = 80 patients | ACL Reconstruction homologous autograft (HT and QT) | (1) QT (n = 40 patients). | Lysholm scores: | During the QT graft collection process, no joint capsule opening or patellar fracture was observed. Postoperatively, no major quadriceps bleeding or hematoma was reported or observed. | Yes |
| (1) QT Preoperative: 94.7 ± 8.2 | |||||||
| Sex: | QT final follow-up: 93.4 ± 7.5 | ||||||
| Male/Female | (2) HT Preoperative: 94.1 ± 9.9 | ||||||
| (1) QT: 23/17 | HT final follow-up: 93.4 ± 8.7 | None of the QT patients reported tenderness, numbness, or irritation at the graft collection site. | |||||
| Austria | Follow-up: 6, 12, and 24 months after surgery. | (2) HT: 23/17 | (1) HT (n = 40 patients). | Pain (VAS): | |||
| Age (average): | (1) QT Preoperative: 0.90 ± 1.1 | Rerupture: Over the 2 years of follow-up, one graft rupture occurred in the HT group, while no further ruptures were recorded in the QT group (n.s.). The re-rupture occurred as a result of the player's contact during a football game. | |||||
| (1) QT: 34.6 ± 11.0 | QT final follow-up: 0.6 ± 1.0 | ||||||
| (2) HT: 34.4 (± 11.0) | (2) HT Preoperative: 0.8 ± 1.0 | ||||||
| HT final follow-up: 0.8 ± 1.2 | |||||||
| Sofu et al., 24 2013 | Retrospective cohort study | N = 44 patients | ACL Reconstruction homologous autograft (HT and QT) | (1) QT (n = 23 patients). | Lysholm scores < 64 (poor): | NR | Yes |
| Sex: | |||||||
| Male/Female | (1) QT Preoperative: 22 (95.6%) | ||||||
| (1) QT: 21/02 | QT final follow-up: 1 (4.3%) | ||||||
| Turkey | Follow-up: 37.6 months | (2) HT: 21/0 | (1) HT (n = 21 patients). | (2) HT Preoperative: 19 (90.5%) | |||
| Age (average): | |||||||
| (1) QT: 26.8 | HT final follow-up: 0 (0%) | ||||||
| (2) HT: 28.6 | |||||||
| Todor et al., 25 2019 | Retrospective cohort study | N = 72 patients | ACL Reconstruction homologous autograft (HT and QT) | (1) QT (n = 39 patients). | Lysholm scores: | In both groups, there were no readmissions or reoperations due to complications. There was one patient in the QT group with a lateral difference of 5 mm in the KT-1000 test and was considered a failure. No patient in the HT group had a difference of more than 3 mm. | Yes |
| Sex: | |||||||
| Male/Female | (1) QT Post-operative: 89.20 ± 9.97 | ||||||
| (1) QT: 26/13 | |||||||
| Romania | Follow-up: 24 months | (2) HT: 23/10 | (1) HT (n = 33 patients). | (1) HT Post-operative: 91.33 ± 6.65 | 5 patients in the QT group (12.82%) reported an unsatisfactory aesthetic appearance of the suprapatellar incision and 8 patients in the HT group (24.24%) reported mild numbness in the anteromedial face of the leg. | ||
| Age (average): | |||||||
| (1) QT: 30.64 ± 8.71 | p = 0.299 | ||||||
| (2) HT: 28.60 ± 6.74 | |||||||
VAS: visual analog scale; QT: quadriceps tendon; HT: hamstring tendons; NR: not reported; IKDC: International Knee Documentation Committee.
RESULTS
Function
Ten studies showed results on knee function after QT autograft and HT autograft. 8 ),( 16 )-( 18 ),( 20 ),( 22 )-( 26 ACL reconstruction with QT autograft presented clinical outcomes similar to those of the HT autograft in terms of stability and knee function. 8 ),( 17 ),( 23 ),( 26 Of the studies included, only one demonstrated that the autograft of the quadruple tendon of the HT is superior to the autograft of the QT in arthroscopic ACL reconstruction surgery. 24
Furthermore, one year after ACL reconstruction, it was found that the autograft of HT led to impairments of the extensor and flexor bilateral muscle strength, while the autograft of QT resulted in more pronounced impairments only in the extensor bilateral muscle strength. The functional capacity reported by the patient was not affected by the type of autograft. 23
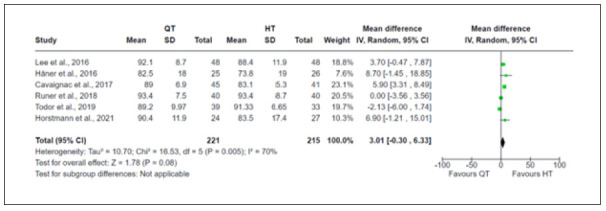
We conducted a meta-analysis of six studies with data on knee function analyzed by the Lysholm score. 16 )-( 18 ),( 20 ),( 22 ),( 25 The meta-analysis results indicated that there were no differences in knee function between the QT autograft and the HT autograft (MD 3.01; CI-0.30, 6.33, p = 0.08), and there was evidence of moderate heterogeneity among the studies (I² = 70%, Chi² = 16.53). Figure 2 presents the Funnel plot results for the Lysholm score.
Figure 2. Funnel plot showing the mean difference in Lysholm scores between quadriceps tendon and hamstring tendon autografts.
Pain
Eight studies showed results on the presence of pain after ACL reconstruction surgery. 15 )-( 17 ),( 19 ),( 21 ),( 22 ),( 24 ),( 26
Vilchez-Cavazos et al. 26 reported that no significant differences were observed regarding pain between the groups of QT and HT autograft, in the pre and postoperative periods. However, Buescu et al. 15 reported that the percentage of individuals who required supplementary analgesics was 38% higher in the group with HT autograft, when compared with the group with QT autograft. In the study by Ortmaier et al., 21 the subjective assessments of pain during and after sports activity reported a significant worsening in almost all parameters with no significant difference between pre- and postoperative groups.
We performed two meta-analyses on the differences in pain after ACL reconstruction with QT and HT autograft. In the first meta-analysis conducted with four studies that contained data on the total amount of pain, the result indicated that there were no differences between the groups analyzed after intervention (RR 0.89; CI-0.57, 1.39, p = 0.60) and there was low evidence of heterogeneity among the studies (I² = 36%, Chi² = 4.68). 15 ),( 17 ),( 19 ),( 24 Additionally, the other meta-analysis with mean and standard deviation of the presence of pain after reconstruction also indicated that there were no differences between the groups analyzed after intervention (MD 1.63; CI-2.45, 5.72, p = 0.43) 16 ),( 17 (Figure 3).
Figure 3. Funnel plot showing the proportion of risk (A) and mean difference (B) of pain after surgical intervention for reconstruction with autografts of the quadriceps tendon and hamstring tendon.

Return to sport
Two studies reported data on return to sport. 18 ),( 21 Horstmann et al. 18 indicated that the time of return to sport was 82 days in the QT autograft group and 95.2 days in the HT autograft group, and there were no differences between the groups. Furthermore, the study by Ortmaier et al. 21 reported that the rate of return to sports was 91.3% and there were no significant differences (p ≥ 0.05) in the number of sports modalities and in the time of return to sport between groups.
Complication and adverse events
Table 1 shows information on adverse events or complications reported in the studies. Horstmann et al. 18 conducted a randomized controlled trial with a 2-year follow-up period. The authors reported that in the HT group, there was one graft delay, which was treated with revision ACL reconstruction with QT. There was also residual anteromedial instability of the knee, which was treated with the reconstruction of the medial collateral ligament of the knee and revision of the ACL graft. In the QT autograft group, there was one early infection, which was treated with antibiotic transplant retention and arthroscopic lavage and three ACL graft retentions, which were treated with ACL graft revision (two revision reconstructions with thigh tendon graft and a healing response).
Cavaignac et al. 16 described that in the QT autograft group, there was one re-rupture after a new sports injury (contact sport) after 3.7 years of follow-up. There were three reoperations: one for a cyclops lesion (at 5.7 months), one to remove the femoral screw (at 13.1 months), and one for a grade 3 medial condyle cartilage lesion (microfracture at 25.2 months). In the HT group, there were two cases of graft rupture. One patient was re-operated at 15.3 months for arthroscopic arthrolysis.
Akoto et al. 8 reported that the graft failure rate was 7.3% in the QT autograft group and 9.8% in the HT autograft group and there was no statistical difference between the groups. Furthermore, no statistical difference was found between the two groups in terms of infection, contralateral rupture of the ACL or lesions associated with meniscus and cartilage. During the 2-year follow-up, in a cohort study, none of the patients with QT autograft reported tenderness, numbness, or irritation at the graft collection site. 22
Re-rupture
One study reported cases of contralateral ACL rupture 8 and two studies reported graft re-rupture. 16 ),( 22 The meta-analysis of the three studies showed no differences in rupture following QT or HT autograft (RR 0.60; CI-0.19, 1.88, p = 0.38), and there was no evidence of heterogeneity among the studies (I² = 0%, Chi² = 0.28). Figure 4 shows the results of rupture following QT or HT autograft.
Figure 4. Funnel plot showing the proportion of risk of ruptures after surgical intervention for reconstruction with autografts of the quadriceps tendon and hamstring tendon.

Quality assessment
Table 2 shows the analysis of the methodological quality of the studies. Figure 5 shows the bias risk analysis for both randomized and non-randomized studies.
Table 2. Quality assessment.
| Summary of findings: | ||||||
|---|---|---|---|---|---|---|
| Quadriceps tendon autograft compared with hamstring tendon autograft for anterior cruciate ligament reconstruction | ||||||
| Patient or population: anterior cruciate ligament reconstruction | ||||||
| Setting: | ||||||
| Intervention: Quadriceps tendon autograft | ||||||
| Comparison: hamstring tendon autograft | ||||||
| Outcomes | Anticipated absolute effects * (95% CI) | Relative effect (95% CI) | Nº of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with hamstring tendon autograft | Risk with Quadriceps tendon autograft | |||||
| Function follow-up: mean 3 years | The mean function was 89.43 | mean 85.59 higher (0 to 0) | - | 436 (6 RCTs) | ⨁⨁⨁◯ MODERATE | There were no differences in knee function between quadriceps tendon autograft and hamstring autograft (p = 0.08). |
| Pain follow-up: range 48 Years to 24 months | 383 per 1.000 | 341 per 1.000 (218 to 533) | RR 0.89 (0.57 to 1.39) | 254 (4 RCTs) | ⨁⨁⨁◯ MODERATE | There were no differences in pain between the groups analyzed after the intervention (p = 0.60). |
| Return to sport follow-up: median 2 years | The mean return to sport was 82.1 | mean 95.2 higher (0 to 0) | - | 51 (1 RCT) | ⨁⨁⨁⨁ HIGH | There were no significant differences (p < 0.131) in time to return to sport between groups. |
| Complications - Re-rupture follow-up: range 12 months to 3 years | 11 per 1.000 | 0 per 1.000 (0 to 0) | no estimates | 371 (5 observational studies) | ⨁⨁◯◯ LOW | There were no differences in rupture following quadriceps tendon autograft and hamstring autograft (p = 0.38). |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). | ||||||
| CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence | ||||||
| High certainty: We are very confident that the true effect lies close to that of the estimate of the effect | ||||||
| Moderate certainty: We are moderately confident in the estimated effect: The true effect is likely to be close to the estimated effect, but there is a possibility that it is substantially different | ||||||
| Low certainty: Our confidence in the estimated effect is limited: The true effect may be substantially different from the estimated effect | ||||||
| Very low certainty: We have very little confidence in the estimated effect: The true effect is likely to be substantially different from the estimated effect | ||||||
Figure 5. Assessment of the risk of bias from (A) randomized clinical trials and (B) non-randomized trials.

DISCUSSION
This systematic review included 13 studies, nine of which were included in the meta-analysis comparing the reconstruction of ACL rupture with QT autograft and HT autograft. The total sample of adult participants was 879. The main finding of this systematic review and meta-analysis is that there were no statistically or clinical differences between the two reconstructions in relation to functionality (Lysholm score), 16 )-( 18 ),( 20 ),( 22 ),( 25 pain (VAS), 15 ),( 17 ),( 19 ),( 24 and rupture following reconstruction. 8 ),( 16 ),( 22 In addition, there were no differences between the groups regarding rates of graft failures and infections. 8
Although there is another meta-analysis on functional results between reconstruction for ACL rupture with QT autograft and HT autograft, 27 our review included a greater number of studies and with new results. Moreover, our review has the differential of presenting meta-analysis results on pain and re-rupture between the two interventions.
The systematic review and meta-analysis mentioned above was published in February 2019. 27 The authors compared the QT Autograft versus HT and patellar tendon (bone-tendon-bone) autograft. 27 They concluded that the QT autograft had comparable clinical and functional results and graft survival rate when compared with the patellar tendon (bone-tendon-bone) and HT autograft. The QT autograft, however, showed significantly less pain at the site of collection than the patellar tendon autograft (bone-tendon-bone) and better functional results than the HT autograft. 27
Another recent systematic review and meta-analysis of randomized clinical trials was performed to compare autografts of the patellar tendon (bone-tendon-bone) with HT autografts. The authors also identified that no recommendation can be made on the optimal choice of graft when using, as a primary metric, the return to baseline level of physical activity and/or participation in sports. 28
When comparing autograft and synthetic graft interventions in participants with ACL injury, a recent systematic review concluded that patellar tendon autografts (bone-tendon-bone) were associated with better results regarding ACL integrity and stability in the pivot shift and Lachman tests, better degrees of IKDC function, and lower complication rates than synthetic grafts. 29
As a strength of this review, we highlight the development of a comprehensive research strategy and the accuracy in the selection of studies. As possible limitations of our study, we highlight the heterogeneity between the studies, identified by the presentation of the different outcomes, methods of comparison, and intervention and follow-up period for ACL reconstruction. The evidence is not very robust according to the evaluation of methodological quality, this is mostly due to the small sample size in most of the studies. Thus, we highlight the importance of conducting future research, including high-quality clinical trials and cohort studies, with large sample size and follow-up time; these will help in deciding the best surgical intervention. In future updates to this review, the addition of evidence from ongoing studies and new robust studies should help inform on the optimal treatment for anterior cruciate ligament injuries. These studies should not only evaluate and report results that are important for patients with ACL rupture but should also consider factors such as standardization of interventions, period of follow-up, and assessment methods of pain, functions, and complications that create additional challenges in the design, conduction, and interpretation of clinical trials and cohort studies.
CONCLUSION
We found evidence that there is no difference in the postoperative period of surgical treatment of ACL reconstruction with QT autograft and HT autograft regarding the results of function, pain, and re-rupture. Therefore, one technique is not superior to another considering functionality, pain, and ruptures after ACL reconstruction.
SUPPLEMENTARY MATERIAL 1.
SEARCH STRATEGIES USED IN DATABASES.
| Databases | Search Strategy |
|---|---|
| MEDLINE/PubMed | Search: ((((Anterior Cruciate Ligament Reconstruction) OR (ACL reconstruction)) AND (quadriceps tendon autograft)) OR (quadriceps graft)) AND (Hamstring-Tendon Autografts) Filters: from 2000 - 2021 |
| 06/10/2021 | Total: 197 |
| EMBASE | 1 (Anterior Cruciate Ligament Reconstruction or ACL reconstruction).mp. [mp=title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading word, candidate term word] 16283 |
| 2 (quadriceps tendon autograft or quadriceps graft).mp. [mp=title, abstract, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword, floating subheading word, candidate term word] 156 | |
| 3 anterior cruciate ligament/ or anterior cruciate ligament reconstruction/ or tendon graft/ or Hamstring-Tendon Autografts.mp. or hamstring/ or hamstring tendon/ | |
| 06/10/2021 | 30642 |
| 41 and 2 and 3 | |
| Total: 119 | |
| Cochrane Central Register of Controlled Trials | (Anterior Cruciate Ligament Reconstruction OR ACL reconstruction) AND (quadriceps tendon autograft OR quadriceps graft) AND (Hamstring-Tendon Autografts) |
| 06/10/2021 | Total: 34 |
SUPPLEMENTARY MATERIAL 2.
EXCLUDED ARTICLES AND REASON FOR EXCLUSIONS.
| Number | Title | Reason for exclusion |
|---|---|---|
| 1 | Hamstring tendon autograft versus quadriceps tendon autograft for anterior cruciate ligament reconstruction: a randomised controlled trial [Internet]. Hoboken: Cochrane Central Register of Controlled Trials (CENTRAL); 2018 [accessed on 2022 Oct 24]. Available from: https://trialsearch.who.int/Trial2.aspx?TrialID=ACTRN12618001520224 | 1 |
| 2 | A randomized controlled trial comparing the outcomes of quadriceps autograft vs. hamstring autograft in acl reconstruction [Internet]. Hoboken: Cochrane Central Register of Controlled Trials (CENTRAL); 2019 [accessed on 2022 Oct 24]. Available from: https://trialsearch.who.int/Trial2.aspx?TrialID=ACTRN12619001396112 | 1 |
| 3 | Cristiani R, Mikkelsen C, Wange P, Olsson D, Stålman A, Engström B. Autograft type affects muscle strength and hop performance after ACL reconstruction. A randomised controlled trial comparing patellar tendon and hamstring tendon autografts with standard or accelerated rehabilitation. Knee Surg Sports Traumatol Arthrosc. 2021;29(9):3025-3036. | 2 |
| 4 | Feller JA, Webster KE. A randomized comparison of patellar tendon and hamstring tendon anterior cruciate ligament reconstruction. Am J Sports Med. 2003;31(4):564-73. | 2 |
| 5 | Gupta R, Kapoor D, Kapoor L, Malhotra A, Masih GD, Kapoor A, Joshi S. Immediate post-operative pain in anterior cruciate ligament reconstruction surgery with bone patellar tendon bone graft versus hamstring graft. J Orthop Surg Res. 2016;11(1):67. | 2 |
| 6 | Comparing two surgical techniques for anterior cruciate ligament (ACL) reconstruction [Internet]. Hoboken: Cochrane Central Register of Controlled Trials (CENTRAL); 2020 [accessed on 2022 Oct 24]. Available from: https://trialsearch.who.int/Trial2.aspx?TrialID=ISRCTN55542036 | 1 |
| 7 | A double blind randomized comparative study of two autografts in arthroscopic ACL reconstruction [Internet]. SICOT 40th Orthopaedic World Congress; 2019; Muscat. Hoboken: Cochrane Central Register of Controlled Trials (CENTRAL); 2019 [accessed on 2022 Oct 24]. Available from: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-02072196/full | 4 |
| 8 | Kondo E, Yasuda K, Miyatake S, Kitamura N, Tohyama H, Yagi T. Clinical comparison of two suspensory fixation devices for anatomic double-bundle anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2012;20(7):1261-7. | 3 |
| 9 | Martin-Alguacil JL, Arroyo-Morales M, Martin-Gómez JL, Lozano-Lozano M, Galiano-Castillo N, Cantarero-Villanueva I. Comparison of knee sonography and pressure pain threshold after anterior cruciate ligament reconstruction with quadriceps tendon versus hamstring tendon autografts in soccer players. Acta Orthop Traumatol Turc. 2019;53(4):260-5. | 3 |
| 10 | Anterior cruciate ligament-reconstruction: quadriceps tendon or hamstrings tendon? A prospective randomised controlled trial [Internet]. Bethesda: NML; 2019 [acessed on 2022 Oct 24]. Available from: https://clinicaltrials.gov/show/NCT02173483 | 1 |
| 11 | Comparative study of anterior cruciate ligament reconstruction (quadriceps versus hamstring tendon) [Internet]. Bethesda: NML; 2018 [acessed on 2022 Oct 24]. Available from: https://clinicaltrials.gov/ct2/show/NCT02832791 | 1 |
| 12 | Recovery of soccer players after anterior cruciate ligament reconstruction [Internet]. Bethesda: NML; 2021 [acessed on 2022 Oct 24]. Available from: https://clinicaltrials.gov/ct2/show/NCT04742868 | 1 |
| 13 | Setuain I, Izquierdo M, Idoate F, Bikandi E, Gorostiaga EM, Aagaard P, et al. Differential effects of 2 rehabilitation programs following anterior cruciate ligament reconstruction. J Sport Rehabil. 2017;26(6):544-55. | 2 |
| 14 | Tashiro T, Kurosawa H, Kawakami A, Hikita A, Fukui N. Influence of medial hamstring tendon harvest on knee flexor strength after anterior cruciate ligament reconstruction. A detailed evaluation with comparison of single- and double-tendon harvest. Am J Sports Med. 2003;31(4):522-9. | 2 |
| 15 | Wipfler B, Donner S, Zechmann CM, Springer J, Siebold R, Paessler HH. Anterior cruciate ligament reconstruction using patellar tendon versus hamstring tendon: a prospective comparative study with 9-year follow-up. Arthroscopy. 2011;27(5):653-65. | 2 |
| 16 | Yoo SH, Song EK, Shin YR, Kim SK, Seon JK. Comparison of clinical outcomes and second-look arthroscopic findings after ACL reconstruction using a hamstring autograft or a tibialis allograft. Knee Surg Sports Traumatol Arthrosc. 2017;25(4):1290-7. | 2 |
| 17 | Chen CH, Chen WJ, Shih CH. Arthroscopic reconstruction of the posterior cruciate ligament: a comparison of quadriceps tendon autograft and quadruple hamstring tendon graft. Arthroscopy. 2002;18(6):603-12. | 2 |
| 18 | Chen CH, Chen WJ, Shih CH, Jiang CC. Quadriceps tendon-patellar bone autograft for arthroscopic anterior cruciate ligament reconstruction. Journal of Surgical Association Republic of China. 1998;31(3):166-72. | 5 |
| 19 | A study comparing two grafts for treatment of knee instability [Internet]. Hoboken: Cochrane Central Register of Controlled Trials (CENTRAL); 2019 [acessed on 2022 Oct 24]. Available from: https://trialsearch.who.int/Trial2.aspx?TrialID=CTRI/2017/03/008098 | 1 |
| 20 | Is quadriceps tendon a better choice than hamstring tendons for repairing anterior cruciate ligament lesion? [Internet]. Hoboken: Cochrane Central Register of Controlled Trials; 2019 [acessed on 2022 Oct 24]. Available from: https://trialsearch.who.int/Trial2.aspx?TrialID=ISRCTN12967309 | 1 |
| 21 | Ouabo EC, Gillain L, Saithna A, Blanchard J, Siegrist O, Sonnery-Cottet B. Combined anatomic anterior cruciate and anterolateral ligament reconstruction with quadriceps tendon autograft and gracilis allograft through a single femoral tunnel. Arthrosc Tech. 2019;8(8):e827-34. | 6 |
| 22 | Sanada T, Iwaso H, Fukai A, Honda E, Yoshitomi H, Inagawa M. Anatomic anterior cruciate ligament reconstruction using rectangular bone-tendon-bone autograft versus double-bundle hamstring tendon autograft in young female athletes. Arthrosc Sports Med Rehabil. 2021;3(1):e47-55. | 2 |
| 23 | Shibata Y, Matsushita T, Araki D, Kida A, Takiguchi K, Ueda Y, et al. Prediction of quadriceps strength recovery after anterior cruciate ligament reconstruction with a hamstring autograft: decision tree analysis. J Orthop Sci. 2019;24(2):301-5. | 3 |
| 24 | Fischer F, Fink C, Herbst E, Hoser C, Hepperger C, Blank C, Gföller P. Higher hamstring-to-quadriceps isokinetic strength ratio during the first post-operative months in patients with quadriceps tendon compared to hamstring tendon graft following ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2018;26(2):418-25. | 3 |
| 25 | Shaieb MD, Kan DM, Chang SK, Marumoto JM, Richardson AB. A prospective randomized comparison of patellar tendon versus semitendinosus and gracilis tendon autografts for anterior cruciate ligament reconstruction. Am J Sports Med. 2002;30(2):214-20. | 2 |
| 26 | Martin-Alguacil JL, Arroyo-Morales M, Martín-Gomez JL, Monje-Cabrera IM, Abellán-Guillén JF, Esparza-Ros F, et al. Strength recovery after anterior cruciate ligament reconstruction with quadriceps tendon versus hamstring tendon autografts in soccer players: a randomized controlled trial. Knee. 2018;25(4):704-14. (e-mail sent to authors) | 7 |
| 1Clinical trial record; 2Another comparison; 3Another outcome; 4Summary of congress; 5Another language; 6Article of revision of surgical technique; 7Incomplete data - deleted after contact with authors. | ||
Footnotes
The study was conducted at Hospital Israelita Albert Einstein.
REFERENCES
- 1.Monk AP, Davies LJ, Hopewell S, Harris K, Beard DJ, Price AJ. Surgical versus conservative interventions for treating anterior cruciate ligament injuries. Cochrane Database Syst Rev. 2016;4(4):CD011166–CD011166. doi: 10.1002/14651858.CD011166.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Prentice HA, Lind M, Mouton C, Persson A, Magnusson H, Gabr A. Patient demographic and surgical characteristics in anterior cruciate ligament reconstruction a description of registries from six countries. Br J Sports Med. 2018;52(11):716–722. doi: 10.1136/bjsports-2017-098674. [DOI] [PubMed] [Google Scholar]
- 3.Strong A, Arumugam A, Tengman E, Röijezon U, Häger CK. Properties of knee joint position sense tests for anterior cruciate ligament injury a systematic review and meta-analysis. Orthop J Sports Med. 2021;9(8):23259671211007878–23259671211007878. doi: 10.1177/23259671211007878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mehran N, Damodar D, Shu Yang J. Quadriceps tendon autograft in anterior cruciate ligament reconstruction. J Am Acad Orthop Surg. 2020;28(2):45–52. doi: 10.5435/JAAOS-D-19-00032. [DOI] [PubMed] [Google Scholar]
- 5.Spindler KP, Wright RW. Clinical practice Anterior cruciate ligament tear. New Engl J Med. 2008;359(20):2135–2142. doi: 10.1056/NEJMcp0804745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Heffron WM, Hunnicutt JL, Xerogeanes JW, Woolf SK, Slone HS. Systematic review of publications regarding quadriceps tendon autograft use in anterior cruciate ligament reconstruction. Arthrosc Sports Med Rehabil. 2019;1(1):e93–e99. doi: 10.1016/j.asmr.2019.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marín Fermín T, Hovsepian JM, Symeonidis PD, Terzidis I, Papakostas ET. Insufficient evidence to support peroneus longus tendon over other autografts for primary anterior cruciate ligament reconstruction a systematic review. J ISAKOS. 2021;6(3):161–169. doi: 10.1136/jisakos-2020-000501. [DOI] [PubMed] [Google Scholar]
- 8.Akoto R, Albers M, Balke M, Bouillon B, Höher J. ACL reconstruction with quadriceps tendon graft and press-fit fixation versus quadruple hamstring graft and interference screw fixation - a matched pair analysis after one year follow up. BMC Musculoskelet Disord. 2019;20(1):109–109. doi: 10.1186/s12891-019-2499-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928–d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Milner KA, Cosme S. The PICO Game an innovative strategy for teaching step 1 in evidence-based practice. Worldviews Evid Based Nurs. 2017;14(6):514–516. doi: 10.1111/wvn.12255. [DOI] [PubMed] [Google Scholar]
- 12.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210–210. doi: 10.1186/s13643-016-0384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J. GRADE guidelines 3. rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–406. doi: 10.1016/j.jclinepi.2010.07.015. [DOI] [PubMed] [Google Scholar]
- 14.Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J. GRADE guidelines 1. introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi: 10.1016/j.jclinepi.2010.04.026. [DOI] [PubMed] [Google Scholar]
- 15.Buescu CT, Onutu AH, Lucaciu DO, Todor A. Pain level after ACL reconstruction a comparative study between free quadriceps tendon and hamstring tendons autografts. Acta Orthop Traumatol Turc. 2017;51(2):100–103. doi: 10.1016/j.aott.2017.02.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cavaignac E, Coulin B, Tscholl P, Nik Mohd Fatmy N, Duthon V, Menetrey J. Is quadriceps tendon autograft a better choice than hamstring autograft for anterior cruciate ligament reconstruction A comparative study with a mean follow-up of 3.6 years. Am J Sports Med. 2017;45(6):1326–1332. doi: 10.1177/0363546516688665. [DOI] [PubMed] [Google Scholar]
- 17.Häner M, Bierke S, Petersen W. Anterior cruciate ligament revision surgery ipsilateral quadriceps versus contralateral semitendinosus-gracilis autografts. Arthroscopy. 2016;32(11):2308–2317. doi: 10.1016/j.arthro.2016.03.020. [DOI] [PubMed] [Google Scholar]
- 18.Horstmann H, Petri M, Tegtbur U, Felmet G, Krettek C, Jagodzinski M. Quadriceps and hamstring tendon autografts in ACL reconstruction yield comparably good results in a prospective, randomized controlled trial. Arch Orthop Trauma Surg. 2022;142(2):281–289. doi: 10.1007/s00402-021-03862-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Johnston PT, Feller JA, McClelland JA, Webster KE. Strength deficits and flexion range of motion following primary anterior cruciate ligament reconstruction differ between quadriceps and hamstring autografts. J ISAKOS. 2021;6(2):88–93. doi: 10.1136/jisakos-2020-000481. [DOI] [PubMed] [Google Scholar]
- 20.Lee JK, Lee S, Lee MC. Outcomes of anatomic anterior cruciate ligament reconstruction bone-quadriceps tendon graft versus double-bundle hamstring tendon graft. Am J Sports Med. 2016;44(9):2323–2329. doi: 10.1177/0363546516650666. [DOI] [PubMed] [Google Scholar]
- 21.Ortmaier R, Fink C, Schobersberger W, Kindermann H, Leister I, Runer A. Return to sports after anterior cruciate ligament injury a matched-pair analysis of repair with internal brace and reconstruction using hamstring or quadriceps tendons. Sportverletz Sportschaden. 2021;35(1):36–44. doi: 10.1055/a-1019-0949. [DOI] [PubMed] [Google Scholar]
- 22.Runer A, Wierer G, Herbst E, Hepperger C, Herbort M, Gföller P. There is no difference between quadriceps- and hamstring tendon autografts in primary anterior cruciate ligament reconstruction a 2-year patient-reported outcome study. Knee Surg Sports Traumatol Arthrosc. 2018;26(2):605–614. doi: 10.1007/s00167-017-4554-2. [DOI] [PubMed] [Google Scholar]
- 23.Sinding KS, Nielsen TG, Hvid LG, Lind M, Dalgas U. Effects of autograft types on muscle strength and functional capacity in patients having anterior cruciate ligament reconstruction a randomized controlled trial. Sports Med. 2020;50(7):1393–1403. doi: 10.1007/s40279-020-01276-x. [DOI] [PubMed] [Google Scholar]
- 24.Sofu H, Sahin V, Gürsu S, Yildirim T, Issin A, Ordueri M. Use of quadriceps tendon versus hamstring tendon autograft for arthroscopic anterior cruciate ligament reconstruction a comparative analysis of clinical results. Eklem Hastalik Cerrahisi. 2013;24(3):139–143. doi: 10.5606/ehc.2013.31. [DOI] [PubMed] [Google Scholar]
- 25.Todor A, Nistor DV, Caterev S. Clinical outcomes after ACL reconstruction with free quadriceps tendon autograft versus hamstring tendons autograft A retrospective study with a minimal follow-up two years. Acta Orthop Traumatol Turc. 2019;53(3):180–183. doi: 10.1016/j.aott.2019.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Vilchez-Cavazos F, Dávila-Martínez A, Garza-Castro S, Simental-Mendía M, Garay-Mendoza D, Tamez-Mata Y. Anterior cruciate ligament injuries treated with quadriceps tendon autograft versus hamstring autograft a randomized controlled trial. Cir Cir. 2020;88(1):76–81. doi: 10.24875/CIRU.19001001. [DOI] [PubMed] [Google Scholar]
- 27.Mouarbes D, Menetrey J, Marot V, Courtot L, Berard E, Cavaignac E. Anterior cruciate ligament reconstruction a systematic review and meta-analysis of outcomes for quadriceps tendon autograft versus bone-patellar tendon-bone and hamstring-tendon autografts. Am J Sports Med. 2019;47(14):3531–3540. doi: 10.1177/0363546518825340. [DOI] [PubMed] [Google Scholar]
- 28.Bergeron JJ, Sercia QP, Drager J, Pelet S, Belzile EL. Return to baseline physical activity after bone-patellar tendon-bone versus hamstring tendon autografts for anterior cruciate ligament reconstruction a systematic review and meta-analysis of randomized controlled trials. Am J Sports Med. 2021;50(8):2292–2303. doi: 10.1177/03635465211017522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Fan D, Ma J, Zhang L. Patellar tendon versus artificial grafts in anterior cruciate ligament reconstruction a systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):478–478. doi: 10.1186/s13018-021-02624-x. [DOI] [PMC free article] [PubMed] [Google Scholar]