

Abstract
Introduction: Endoscopic Denker’s approach involves complete exposure of the anterior, inferior and lateral walls of the maxillary sinus providing access to both infratemporal and pterygopalatine fossa. Open approaches to maxillary sinus may lead to a high chance of cranial nerve dysfunction, trismus and wound healing issues. Surgical methods differ based on pathology, exposure, visualization and extent of clearance of the pathology.
Method: The technique and surgical steps of Endoscopic Reverse Denker’s approach are presented.
Results: Critical steps include inferior turbinectomy, uncinectomy, followed by mega middle meatal antrostomy. For exposure drilling is started from the anterior margin of middle meatal antrostomy up to the pyriform aperture anteriorly till the anterior wall of the maxilla is visualized and the nasolacrimal duct can be visualized and transected. This method preserves the pyriform aperture and anterior wall similar to inside-out mastoidectomy tracing the pathology with less bone removal, faster and less morbidity.
Conclusion: Endoscopic Reverse Denker’s is a 2-handed or 4-handed endoscopic technique for proper exposure, visualization and clearance of the maxillary pathology of the anterolateral and anterior wall. Olfaction is preserved and crusting is less as there is less bone removal with no atrophic nasal changes. It preserves the pyriform aperture thereby preventing alar collapse.
Keywords: Endoscopic, Anterior, Reverse Denker’s, Maxillary Sinus
Introduction
Denker’s approach was initially described by Alfred Denker in 1916, later it was reported as an endoscopic technique by Sturmann and Canfield [1, 2]. This approach involves complete exposure of the anterior, inferior and lateral walls of the maxillary sinus. The endoscopic Denker’s approach provides access to both infratemporal and pterygopalatine fossa [3]. Open approaches to maxillary sinus may lead to a high chance of cranial nerve dysfunction, trismus and wound healing issues [4]. These complications are considerably less with endoscopic Denker’s approach. The need for extremely angled endoscopes and instrumentations as well as Denker’s approach, is a valuable surgical procedure for addressing pathology in the anterior maxillary sinus and infratemporal fossa. Here we represent a new surgical technique, called reverse Denker’s approach for maxillary sinus.
How I do it
This procedure is done for anterior maxillary and infratemporal pathology similar to modified endoscopic denker’s approach but in a retrograde approach with 0 degree and 70 degree angled endoscope.This technique is useful in cases which cannot be managed with the conventional functional endoscopic sinus surgery (FESS) approach. Initial steps include inferior turbinectomy, uncinectomy, followed by mega middle meatal antrostomy. With a straight / angled handpiece with a drill ( cutting or coarse diamond burr); drilling is started from the anterior margin of middle meatal antrostomy up to the pyriform aperture anteriorly till the anterior wall of the maxilla is visualized (maxillary pathology may vary from individual to individual depending on pneumatization of maxilla). This method preserves the pyriform aperture and anterior wall. An Angled endoscope and handpiece for drilling can help in proper exposure, visualization and clearance of the pathology. While drilling retrograde from the posterior to anterior approach, one may encounter the nasolacrimal duct which can be adequately visualized and transected with scissors or Surgical Scalpel Blade Number 11. This technique can also be performed for infratemporal tumours. This technique preserves the pyriform aperture and anterior wall of the maxilla thus avoiding alar collapse as a possible postoperative complication.
Reverse Denker’s approach is just like the inside-out mastoidectomy tracing the pathology with less bone removal, faster and less morbidity. In this procedure, the anterior facial skeleton is preserved thereby preventing alar collapse which may lead to postoperative facial deformity. [Figure 1]
Discussion
Radical surgeries to treat chronic maxillary sinus causes distressing symptoms due to trauma of the soft tissue of the cheek and extensive destruction of the anterior maxillary wall [1]. Spontaneous healing of the maxillary sinus after an open procedure is usually delayed and cases chances of secondary sinusitis are more [2]. The Anteroinferior and anterolateral aspect of the maxillary sinus is difficult to reach through a purely transnasal approach [3]. The complexity of skull base surgeries lies between technical demands for maximum exposure, visualization and the nature of skull base anatomy [4].
The maxillary sinus is divided into five zones of access by Harvey et al. [5]. They are the nasal cavity (zone 1), medial to the infraorbital nerve (zone 2), lateral to the infraorbital nerve (zone 3), anterior maxilla (zone 4), and premaxillary tissue (zone 5). Zone 3, 4, and 5 are identified as the most difficult areas to access endoscopically. A variety of endoscopic procedures have been developed recently to increase instrumental accessibility to the maxillary sinus. Exposure of maxillary sinus is more in modified endoscopic medial maxillectomy than standard middle meatal antrostomy.
Non-opposing septal incisions are used by Robinson et al. to facilitate endoscopic tumour resection [6]. Ramakrishnan et al. identified that septal dislocation provides more anterolateral reach over total endoscopic medial maxillectomy [7].
Endoscopic Denker’s approach is a soft tissue approach similar to radical endoscopic medial maxillectomy. Here mucosal flap is raised anterior to the inferior turbinate head with exposure of frontal process of maxilla & bony dissection is taken laterally over the face of the maxilla [8]. Adequate exposure through an endoscopic anterior maxillotomy without the need for a sublabial incision is one of the advantages of Denker’s approach [9]. For the management of extensive sinonasal tumours, this approach is appropriate but it is associated with the risk of damage to the infraorbital nerve, alar collapse and nasolacrimal duct injury [10].
Crusting will be there like any extended maxillary procedures; in the Endoscopic reverse denkers approach the nasal crusting is significantly less as there is less bone removal. Regular follow-up on an outpatient clinic basis for 6 months to 1 year by diagnostic nasal endoscopy for nasal crusting and its removal is minimal as bone removal is minimal. On Endoscopic assessment, during follow-up, there were no atrophic nasal changes in the mucosa and underlying bones. Olfaction is preserved as the working surgical approach is well below the olfactory area. This surgical approach is indicated for maxillary pathology of anterolateral and anterior wall sites which are not accessible through large Middle meatal antrostomy and infratemporal pathologies.
Endoscopic denker’s surgery is a four-hand technique (to retract soft tissue) whereas Endoscopic Reverse Denker’s approach is a 2-handed or 4-handed technique. In the Endoscopic Denkers approach, there is alar collapse secondary to the loss of the pyriform ridge [11]. In Reverse Denker’s approach, the pyriform ridge being intact, alar collapse is unlikely.
During the COVID-19 pandemic, covid associated mucormycosis was on the rise, in our Clinical practice prolonged surgical time increases the risk of exposure and transmission of Covid-19 to surgeons, assistants and operation theatre technicians. This led to an innovative surgical approach to address maxillary sinonasal mucormycosis to alleviate such risk during the covid-19 pandemic.
Complications
In Reverse denker’s approach, the possible complications include nasal crusting, epiphora, epistaxis, Long term follow-up, the maxillary sinus ciliary mechanism being lost, and the goblet cell of the maxillary sinus continuing to secrete mucus, which may result in stasis, an additional factor. These patients would require removal of secreting maxillary sinus mucosa and regular postoperative saline nasal douching.
Limitations
The surgical approach by reverse denker’s approach may be challenging in certain anatomical variations of the maxillary sinus.
Conclusion
Endoscopic Reverse Denker’s is a 2-handed or 4-handed endoscopic technique for proper exposure, visualization and clearance of the maxillary pathology of the anterolateral and anterior wall. Olfaction is preserved and crusting is less as there is less bone removal with no atrophic nasal changes. It preserves the pyriform aperture thereby preventing alar collapse.
Fig. 1.
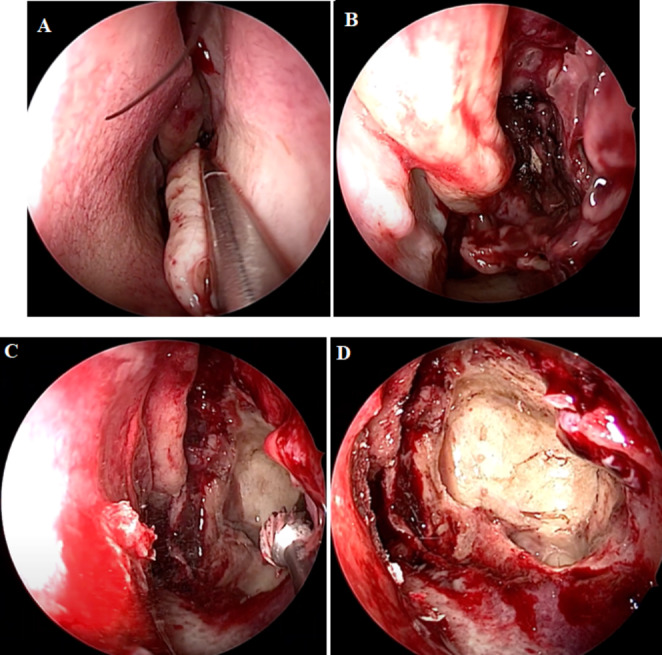
Critical steps in Endoscopic Reverse Denker’s approach
A. Inferior Turbinectomy
B. Maxillary pathology visualized after uncinectomy
C. Widening the maxillary sinus os using drill from posterior to anteriorly
D. All walls of maxillary sinus seen after reverse denker’s approach
Compliance with Ethical Standards
Source of Support (Financial or Non-Financial)
Nil.
Disclosure of Potential Conflicts of Interest
None declared.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from individual participant included in the study.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Nagalingeswaran Ahilasamy, Email: nahilasamy@yahoo.com.
Veerasigamani Narendrakumar, Email: drnarenent@gmail.com.
Rajendran Dinesh Kumar, Email: dinuraj1186@gmail.com.
Arya N Baby, Email: aryaannababy@gmail.com.
Manoj Kumar N, Email: manoj.jagu93@gmail.com.
References
- 1.Canfield RB. The submucous resection of the lateral nasal wall in chronic empyema of the antrum, ethmoid and sphenoid. J Am Med Assoc. 1908;51:1136–1141. doi: 10.1001/jama.1908.25410140018002e. [DOI] [Google Scholar]
- 2.Sturmann D. Die intranasale Eröffnung der Kieferhöhle. Berliner Klinische Wochenschrift. 1908;45:1273–1274. [Google Scholar]
- 3.Lee JT, Suh JD, Carrau RL, Chu MW, Chiu AG Endoscopic Denker’s approach for resection of lesions involving the anteroinferior maxillary sinus and infratemporal fossa.Laryngoscope. 2017Mar; 127(3):556–560. doi: 10.1002/lary.26237. Epub 2016 Sep 19. PMID: 27640815. [DOI] [PubMed]
- 4.Janecka IP Classification of facial translocation approach to the skull base. Otolaryngol Head Neck Surg. 1995 Apr;112(4):579 – 85. doi: 10.1177/019459989511200412. PMID: 7700665 [DOI] [PubMed]
- 5.Harvey RJ, Sheehan PO, Debnath NI, Schlosser RJ (2009) Jul-Aug;23(4):426 – 32 Transseptal approach for extended endoscopic resections of the maxilla and infratemporal fossa. Am J Rhinol Allergy. doi: 10.2500/ajra.2009.23.3333. PMID: 19671261 [DOI] [PubMed]
- 6.Robinson S, Patel N, Wormald PJ (2005) Oct;115(10):1818-22 Endoscopic management of benign tumors extending into the infratemporal fossa: a two-surgeon transnasal approach. Laryngoscope. doi:10.1097/01.mlg.0000174956.90361.dc. PMID: 16222202 [DOI] [PubMed]
- 7.Ramakrishnan VR, Suh JD, Chiu AG, Palmer JN (2011) Mar-Apr;25(2):128 – 30 Septal dislocation for endoscopic access of the anterolateral maxillary sinus and infratemporal fossa. Am J Rhinol Allergy. doi: 10.2500/ajra.2011.25.3559. PMID: 21679518 [DOI] [PubMed]
- 8.Ashman A, Psaltis AJ, Wormald PJ, Tan NC (2020 Jun) Extended endoscopic approaches to the maxillary sinus. J Laryngol Otol 134(6):473–480 [DOI] [PubMed]
- 9.Stavrakas M, Karkos PD, Tsinaslanidou Z, Constantinidis J (2021) Jul;131(7):1458–1462 Endoscopic Denker’s Approach for the Treatment of Extensive Sinonasal Tumors: Our Experience. Laryngoscope. doi: 10.1002/lary.29235. Epub 2020 Nov 3. PMID: 33140854 [DOI] [PubMed]
- 10.El-Sayed I, Pletcher S, Russell M, McDermott M, Parsa A (2011) Apr;121(4):694-8 Endoscopic anterior maxillotomy: infratemporal fossa via transnasal approach. Laryngoscope. doi: 10.1002/lary.21469. PMID: 21433014 [DOI] [PubMed]
- 11.Prosser JD, Figueroa R, Carrau RI, et al. Quantitative analysis of endoscopic endonasal approaches to the infratemporal fossa. Laryngoscope. 2011;121:1601–1605. doi: 10.1002/lary.21863. [DOI] [PubMed] [Google Scholar]