

Abstract
Objective
The present research compared the effectiveness of the monopolar radiofrequency method with that of bipolar method in the facial skin of women in selected age groups.
Methods
The study included 150 women with good general health and healthy skin. The first group comprised 75 female participants who received monopolar radiofrequency electromagnetic field treatment (RFM) and 75 women who were treated using the bipolar method (RFB). In both the RFM and RFB groups, five age groups were distinguished: Group I (20–29 years), Group II (30–39 years), Group III (40–49 years), Group IV (50–59 years), and Group V (60–69 years). Transepidermal water loss (TEWL) was measured using tewametry to determine stratum corneum barrier function and corneometry was used to measure epidermal hydration. Tewametric and corneometric measurements of the facial skin were performed to determine its condition following radiofrequency electromagnetic field therapy and to assess the sustainability of the obtained results after four months of therapy. The follow-up measurement was performed prior to the first treatment session and the subsequent ones after one month, and four months following the first measurement.
Results
The best results, indicating an improvement in epidermal hydration were observed for bipolar radiofrequency method in the age group 40-49 years and group 50-59 years.
Keywords: Radiofrequency, skin, woman, hydration, TEWL
There are a number of factors influencing the condition of the skin, such as ethnicity, color, thickness, which are essential for assessing the effectiveness and sustainability of the results.1,2 Each method of non-invasive skin rejuvenation is based on its regeneration which, in turn, indicates its time-consuming character, while the effects are distributed over time.3 In the radiofrequency method, a non-ablative tissue tightening is observed, as well as an improvement of skin tone occur by means of its remodeling in the process of neocolagenesis and elastogenesis following deep volumetric heating. The immediate response is tissue shortening which stems from breaking the intermolecular cross-linking bonds, thus, leading to the development of the triple helix. Although the energy emitted does not cause ablation, it generates thermal energy in the target tissue which may cause conformational changes. As a result of the partial denaturation of collagen fibers, antigenic determinants are exposed, which digest damaged collagen, whereas the degradation products stimulate fibroblasts to synthesize collagen.4,5,6 Skin defects result from a decrease in the lipid levels and in the skin hydration, as reported by Berardesca et al7 and Firooz et al8. Additionally, Man et al9 found a correlation between the sebum content and the degree of hydration of the stratum corneum in women, although it was not observed in the studied group of men. Depending on the skin area, the highest values were found on the forehead and cheeks, as well as within the area of joint bends, whereas the lower values were found on the forearms and shins.10–13 Moreover, an increased epidermis hydration is observed in the summer, which is accompanied by a decrease in the transepidermal water loss (TEWL).
Cravello et al14 showed the influence of the environment temperature and humidity on hydration and TEWL. In fact, epidermis hydration increases due to higher temperature and humidity, whereas TEWL depends on the temperature increase, and it decreases at high humidity.
Tewametry is the measurement of the barrier function in the stratum corneum. Water loss via the epidermis occurs mainly as a result of two mechanisms: 1) evaporation, by passive diffusion, and 2) secretion by eccrine glands. Since it is not possible to assess the condition of the skin directly, it can be evaluated by measuring the degree of water evaporation. This method employs an electric hygrometer to measure the amount of water lost from the body via the stratum corneum. The parameter describing this skin condition is TEWL, which describes the amount of water evaporated from 1m2of skin within one hour. The measurement of TEWL is used to evaluate the efficiency of skin barrier function, where lower values indicate better skin hydration. In normal conditions, which do not involve an increased sweat secretion, TEWL fluctuates between 85–170mL per day, although with a well-functioning epidermal barrier, it does not exceed 25g/m2/h. In the case of damage to the stratum corneum, the degree of water loss through the epidermis may amount to 70g/m2/h.15 Nevertheless, this factor may be affected by various parameters, including age, sex, body area, skin temperature, sweating, or emotional state. Corneometry constitutes another research method providing information with regard to the state of hydration in the stratum corneum, which is based on the assessment of the electrical capacity of a dielectric medium. Changes in the dielectric constant, associated with skin hydration, alter the electrical capacity. The greater the amount of water in the tissue, the lower the electrical resistance and current conduction. The measurement result is given in the arbitrary units corresponding to 0.02mg of water/cm2of the stratum corneum.16 In the presented research, the functional parameters of the facial skin were evaluated using the Multi Skin Test Centre MC 750 analyzer by Courage and Khazaka Electronic, due to its non-invasiveness and the potential to avoid damage to the epidermal barrier.
METHODS
Research objectives. The aim of the present research was to assess the influence of monopolar and bipolar radiofrequency treatments on the condition of the facial skin and on the durability of the obtained results. This was achieved by measuring the degree of epidermal hydration (corneometry), as well as by measuring the stratum corneum barrier function (tewametry) over the course of a four-month period in women in the selected age groups. Additionally, the effectiveness of the monopolar radiofrequency method was compared to the bipolar radiofrequency method.
Research group. The tests were non-invasive, the participants were informed about the details of the procedure, and they signed an informed consent form. Moreover, a treatment report containing information regarding age, date of the tests, method, and environmental conditions was provided. It was used to conduct a cosmetic interview for the purpose of a diagnosis, as well as to exclude the possible contraindications. Random allocation to groups were implemented. The Bioethics Committee at Poznań University of Medical Sciences approved the research (resolution number 1091/16). Subsequently, the study participants were divided into two groups.
The first group consisted of 75 women who received the monopolar radiofrequency (RFM) treatment. In this group, the following age groups were distinguished, with 15 women in each group: Group I (20–29 years of age), Group II (30–39 years of age), Group III (40–49 years of age), Group IV (50–59 years of age), Group V (60–69 years of age). The results were recorded before and after the procedure, and the subjects underwent the first measurement before and after the procedure (t0). The subsequent data according to the same pattern were collected one month (t1), and four months following the first treatment (t2).
The second group included 75 women who received the bipolar radiofrequency (RFB) therapy, and the following age groups were distinguished, with 15 women in each group: Group I (20–29 years), Group II (30–39 years), Group III (40–49 years), Group IV (50-59 years), Group V (60-69 years). The data were recorded before and after the procedure. The subjects underwent the first measurement before and after the procedure (t0). The subsequent measurements according to the same pattern were performed one month (t1) and four months following the first treatment (t2).
Treatment and measurement methods. The measurements were performed in the same environment, temperature, and relative air humidity. The skin of each participant was acclimatized in order to calm the blood circulation and to reduce skin perspiration. A 10-minute break between the treatment and the measurement to level the skin temperature was preserved following RF application. The probe was applied vertically to the cheek with its entire surface, with a simultaneous control of stability and pressure. Nevertheless, the measurement of the hydration below the zygomatic bone was not conducted, due to the fact that the lack of bone support for the probe may have resulted in the lack of repeatable results. Patients were recommended to refrain from applying makeup on the day of the test, as well as not to use creams and washing products two hours prior to the test.
In the course of the monopolar radiofrequency therapy, the BN-300 radiofrequency device (Beauty System, Wrocław, Poland) was used. The following parameters were used: frequency: 1-5MHz; power: 3W/cm2;l probe diameter: 2cm; maximum skin temperature 40°C, wave: constant, application time: 15 minutes.
In the course of bipolar radiofrequency therapy, the Mimarii (Mimari, Wrocław, Poland) device was used. Treatment parameters were as follows: frequency: 1-5MHz; power: eye area 1-42W/cm2; face 1-64W/cm2; probe diameter: 2cm; maximum skin temperature 40°C; wave: constant; application time: 15 minutes.
Statistical analysis. Statistical analysis was performed using the Grubbs test, which verified the presence of outliers (±3SD); the Shapiro-Wilk test was applied to test the normal distribution, whereas the Mauchly's test was used to evaluate the sphericity assumption. Despite slight deviations from the normal distribution of the studied variables, after verifying the variance homogeneity in the subgroups, the analysis of variance (ANOVA) model with repeated measures was used in the statistical analysis. The study involved variance analysis to explore observations which are dependent on one or more factors operating simultaneously. This method allowed to estimate the probability with which the identified factors may account for the differences between the observed group averages. The effect size was determined using η2partial. The power observed for each effect was also calculated. The significance of the differences between pairs of means was verified using the Newman-Keuls test, which compares all possible pairs of means. Moreover, Pearson's linear correlation coefficients (rxy) were calculated for the selected variables, which indicate the level of linear dependence between random variables. Statistical analyses to test the research hypotheses were performed using the Statistica package. Statistical inference was based on the calculated p-value, comparing it with the level of significance α=0.05 adopted for the purpose of the study. Statistical parameters used in the analysis were as follows: F-distribution, the result of variance analysis, M-arithmetic means of the difference of the measurements before and after the treatment, N-size of the study group, η2partial-effect size, p-value-probability level, (α =0.05)-observed power, (±95% PU)-confidence interval.
RESULTS
Tewametric assessment of the barrier function of the stratum corneum. Epidermal barrier was evaluated on the basis of TEWL before and after the radiofrequency treatment. Subsequently, on the basis of the difference between these measurements, it was estimated whether a decrease (weakening of the barrier= negative values), or an increase (strengthening of the barrier=positive values) was observed in a given test following the procedure. The results of RFB therapy were different, and the initial deterioration was followed by an improvement in the last measurement. In contrast, the epidermal parameters were worse in subjects undergoing the RFM therapy following four months of the treatment in comparison with the RFB therapy results evaluated both after one month of the therapy and after its completion. If TEWL prior to the treatment was 2.2, and following the treatment it was 2.0, epidermal barrier strengthening was recorded. This, in turn, allowed for the evaluation of its function changes in relation to the treatment duration, as well as for the comparison of the two therapies. Interestingly, a significant effect of the age group was found, as well as an interaction between the treatment type (RFM and RFB) and treatment duration (study start - 0, after the one month and after the four months). The p-value was compared with α=0.05 level of significance adopted for the purpose of the study (Table 1).
TABLE 1.
TEWL before and after treatment—ANOVA with repeated measures
| ANALYZED PARAMETERS | F | P-VALUE | η2PARTIAL | POWER OBSERVED (α=0.05) |
|---|---|---|---|---|
| Method | 2.22 | 0.1388 | 0.02 | 0.32 |
| Age group | 3.75 | 0.0062 | 0.10 | 0.88 |
| Method * Age group | 2.40 | 0.0528 | 0.06 | 0.68 |
| Month of measurement | 0.02 | 0.9775 | <0.01 | 0.05 |
| Month of measurement * Method | 5.81 | 0.0034 | 0.04 | 0.87 |
| Month of measurement * Method * Age group | 1.27 | 0.2615 | 0.03 | 0.58 |
In RFM therapy group, skin parameters improved in the initial measurements, on average by 0.03. Conversely, with the treatment duration, skin parameters deteriorated at the subsequent measurements, on average by -0.05 and -0.08. In contrast, the effects of the RFB therapy were different: after the initial deterioration (-0.06), an improvement was observed, from 0.04 to 0.05 in the last measurement. Furthermore, after four months of therapy, epidermal parameters were worse in the subjects who received RFM therapy, as compared to the results of RFB therapy evaluated both after one month and at the end of the treatment.
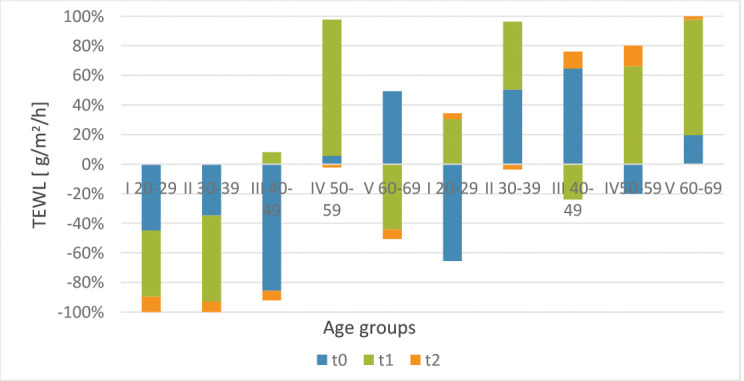
Moreover, a correlation was found between the age group, the type of therapy (RFM, RFB) and therapy duration. In the age Group I (20-29 years) and the age Group II (30-39 years), a significant increase in TEWL was recorded for the monopolar method, affecting the deeper epidermal structures, which indicates that this method is not beneficial for young individuals (as well as for the elderly). There was a statistically significant difference between the treatment method and the therapy duration. In terms of the monopolar method (RFM), in the age Group I (20-29 years) and II (30-39 years), a significant increase in TEWL was observed following the second application (t1), which may indicate that this method is not beneficial for young individuals. Additionally, a slight increase in TEWL was noted after the third application (t2). In the case of this method, in the age Group III (40–49 years) after the third application (t2) TEWL increased with age. In the age Group IV (50–59 years), major changes in hydration level were observed after applications in a fixed time schedule. In the age Group V (60–69 years) for the monopolar method, no significant changes in the improvement of the epidermal barrier were found following the therapy (Figure 1).
FIGURE 1.
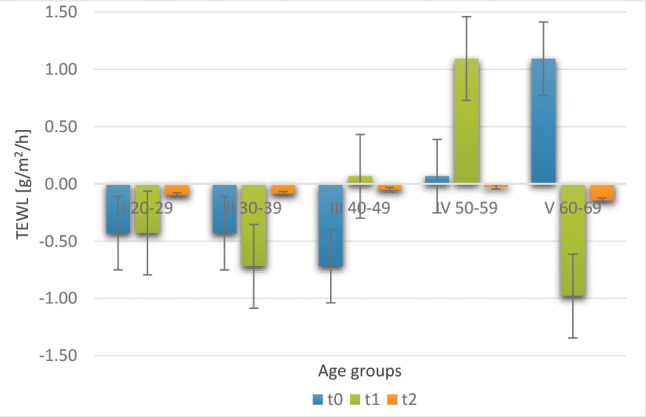
Average results of measuring the barrier function of the stratum corneum according to the investigated time points, age groups, and method (RFM)
In terms of RFB, following an initial deterioration, an improvement was observed in the last measurement. The epidermis parameters were poorer in individuals who underwent RFM after four months of the treatment as compared to the results of bipolar therapy both after one month and at the end of the treatment. Following a four-month therapy with radiofrequency using the RFM and the RFB method, a significant correlation was observed between the TEWL measurement and the method applied. A reduction in TEWL for the bipolar method indicates that the method is suitable for the age Group IV (40-49 years) and age Group V (50-59 years) (Figure 2).
FIGURE 2.
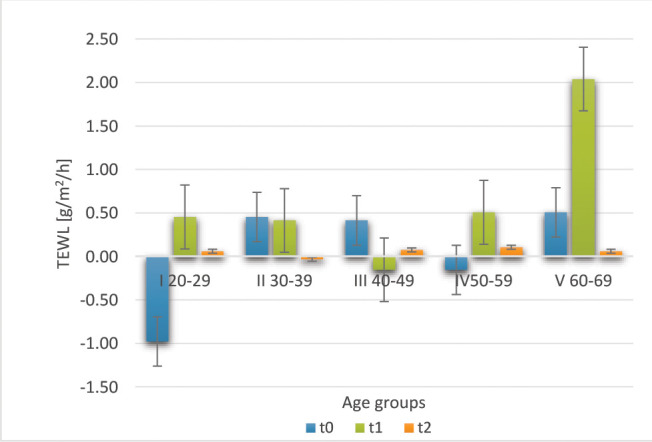
Average results of the stratum corneum barrier function measurement according to the investigated tim points, age groups, and method (RFB)
Corneometric assessment of stratum corneum hydration. The water content in the stratum corneum was measured using corneometry. The effect of radiofrequency therapy constitutes the difference between the post-treatment corneometric measurement and the corneometric measurement prior to the radiofrequency treatment. On the basis of the difference between the earlier and later measurements, it was estimated whether an increase or a decrease in the water content resulted from the therapy. The impact of the method employed, age group, and time of the measurement on the average differences in epidermal hydration prior to and following the treatment was observed.
Subsequently, on the basis of the difference between the later and the earlier measurement, it was estimated whether a decrease in water content (negative values) or an increase (positive values) followed post-treatment. For instance: if the corneometric measurement before the procedure was 32.2; and after it amounted to 34.92, an increase in the epidermal hydration by 2.7 units was noted. The method, the age group and the time of the measurement significantly affected the mean differences in the epidermal hydration, both prior to and following the treatment (Table 2).
TABLE 2.
Corneometric measurements before and after therapy– ANOVA with repeated measurements
| ANALYZED PARAMETERS | F | P-VALUE | η2PARTIAL | POWER OBSERVED (α=0.05) |
|---|---|---|---|---|
| Method | 13.08 | 0.0004 | 0.09 | 0.95 |
| Age group | 2.63 | 0.0368 | 0.07 | 0.72 |
| Method * Age group | 0.77 | 0.5474 | 0.02 | 0.24 |
| Month of measurement | 3.32 | 0.0377 | 0.02 | 0.63 |
| Month of measurement * Method | 1.46 | 0.2341 | 0.01 | 0.31 |
| Month of measurement * Method * Age group | 1.84 | 0.0690 | 0.05 | 0.78 |
The RFB method was more effective, regardless of the treatment duration and the age group. The applied method significantly increased the epidermis hydration in all studied age groups. In fact, the age group exerted a significant impact the moisturizing effects. Moreover, the initial hydration level increased with the therapy duration, which indicates the effectiveness of the therapy. An increase in the epidermal hydration was observed following the application of therapy using both methods. The best effects were observed in Group III (40-49 years) and Group IV (50-59 years).
In terms of the monopolar method, in the age Group I (20-29 years), the hydration level remained constant or slightly increased. In the age Group II (30-39 years), a decrease in hydration after application was observed in the oldest female participants in the group, which could be associated with an increase in TEWL and a natural decrease in the epidermal water content in women at the age of 40.
As far as the age Group III (40–49 years) is concerned, a considerable increase in hydration was observed after the third application (t2) using the same method. In the age Group IV (50–59 years), significant changes in hydration were observed after applications in a fixed time schedule. In the age Group V (60–69), no significant changes in hydration following the therapy were observed for the monopolar method (Figure 3).
FIGURE 3.
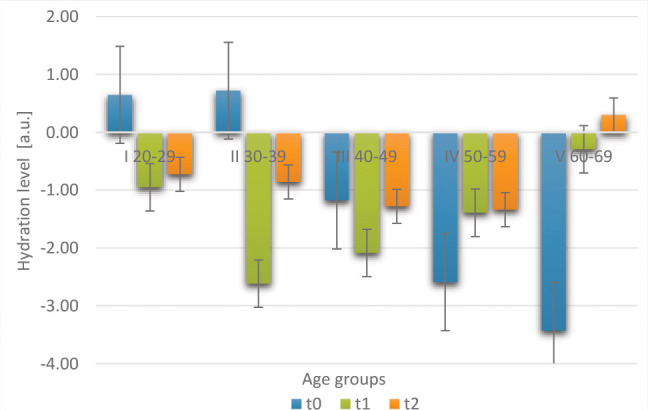
Average results of the corneometric measurement, according to the investigated time points, age groups, and the method (RFM)
In the case of the bipolar method, epidermal hydration was maintained at or within the limits in the age group I (20–29 years). In the age Group II (30–39 years), a constant increase in hydration was observed. In group (40–49 years), an increase in hydration was observed laterally (t2) at application III. In Group IV (50–59 years), a leveling of epidermal hydration occurred in the investigated time-points. In the age group V (60–69 years), low water content in the structures was accompanied by a post-therapy compensation in hydration. The best results following the bipolar strategy were obtained in the age Group III (40–49 years) and IV (50–59 years) (Figure 4).
FIGURE 4.
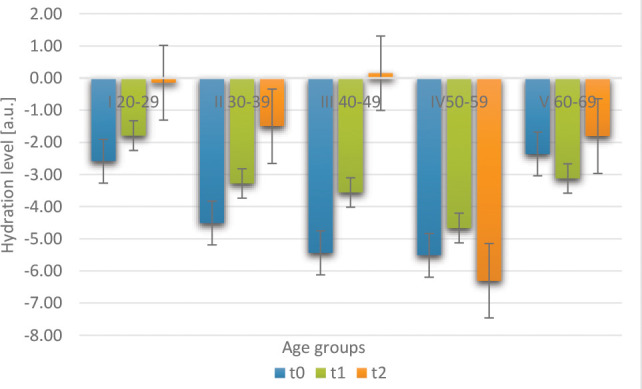
Average results of corneometric measurement, according to the investigated time points, age groups, and the method (RFB)
FIGURE 5.
Average results of the stratum corneum barrier function measurement at the investigated time-points and the age groups for the monopolar (RFM) and bipolar (RFB) methods
FIGURE 6.

Average results of corneometric measurement at the investigated time-points and the age groups for the monopolar method (RFB) and the bipolar method (RFB)
The comparison of monopolar (RFM) and bipolar (RFB) methods, an improvement in facial skin tension was obtained, expressed as a statistically significant increase in the epidermal hydration and a decrease in TEWL. The tewametric measurement was compared in terms of the monopolar and the bipolar method at the studied timepoints (t1, after one month; t2, after four months of therapy) for the selected age groups (I, II, III, IV, V). The same diagram compares the corneometric measurement for the monopolar radiofrequency method and for the bipolar radiofrequency method at the tested timepoints for the selected age groups. The method significantly affected the hydration results. The RFB method was more effective, regardless of the therapy duration and the age group.
In the groups who received RFM, in age Group I (20–29), the hydration level remained stable or slightly increased. A slight increase was also observed in TEWL after the third application (t2). On the other hand, in the age Group II (30–39 years) receiving RFM, a considerable decrease in hydration after the application was observed in the oldest patients in the RFM group. Using the same method, a significant increase in hydration after the third application (t2) was observed in the age Group III (40–49 years). Additionally, as in the previous group, the TEWL increased with age and hydration rapidly decreased in patients over 45 years of age. A decrease in TEWL was also observed in the oldest women. In the age Group IV (50–59 years), considerable changes in the hydration level were observed after applications in a fixed time schedule. In the age Group V (60–69 years of age) for the monopolar method with low water content in skin structures, no significant changes in hydration after therapy were observed. In the bipolar method, in the age Group I (20–29 years), the level of epidermal hydration remained stable or increased slightly, and was the highest of all the studied age groups, although a slight increase in the transepidermal water loss was observed following the second application (t2).
In the groups who received RFB, in the age Group II (30–39 years), a stable increase in hydration and a decrease in TEWL was observed. In the age Group III (40–49 years) in the same method, a significant increase in hydration after the third application (t2) was noted. The highest values indicating an increase in hydration following treatment were observed in the oldest women in this group. Nevertheless, unlike the monopolar method, the TEWL coefficient decreased with age, although notably it increased after the second application, which was not a beneficial phenomenon. In the age Group IV (50–59 years), a decrease in epidermal hydration was observed in a fixed-time distribution. In the age Group V (60–69 years) undergoing the bipolar method yielded a slight improvement in hydration. However, the best effects after the monopolar therapy were observed in the age Group III (40–49 years), where hydration was maintained at 60 percent. In Group I (RFM) and (RFB), an improvement of facial skin tone was found, which was demonstrated by a statistically significant increase of the epidermis hydration and a decrease of TEWL.
DISCUSSION
The aim of the present research was to determine whether radiofrequency therapy with the mono- and bipolar method increased the hydration level of the epidermis, as well as whether it maintained the facial structures tone for a longer period of time. The positive influence of radiofrequency therapy on the proper functioning of the epidermal barrier, the hydration of the epidermis, remodeling of the dermis structures by changing the tension of collagen fibers was confirmed. Moreover, discrepancies were indicated between the measurements in age groups following the application of different test methods performed at time intervals. A significant element was an attempt to correlate the monitoring of the radiofrequency therapy effects with the period of hydration and the volumetric effect of the facial skin, which has not yet been reported in the literature.
The results demonstrated that radiofrequency therapy not only significantly increased both facial skin tone and density, but also persisted post-treatment in the selected age groups. Therefore, the results of both the mono- and bipolar methods contributed to the improvement which persisted until the last follow-up, which may indicate the long-term effectiveness of this method.
CONCLUSION
The application of radiofrequency, both in terms of monopolar and bipolar therapy, resulted in a decrease in TEWL and, therefore, in the increased hydration of the epidermal structures and resulting in better facial skin tension. Differences were shown between values in different age groups, with the best treatment effects observed for the bipolar method in the age Group III (40–49 years) and IV (50–59 years), following the second wave emission. Non-invasive biophysical methods of assessing the facial skin parameters, including the measurement of the barrier function of stratum corneum (tewametry) and the measurement of epidermal hydration (corneometry), constitute a reliable method for the evaluation of a 4-month radiofrequency therapy.
The analysis of skin impedance measurements conducted on a large group of respondents confirmed the assumptions of other researchers regarding the possibility of using research methods in monitoring the effects after non-invasive radiofrequency treatment.17–21 In fact, radiofrequency therapy not only significantly increased facial skin tension and density, but also persisted following its completion in the selected age groups. Summing up, the effects obtained in the course of the therapy, both with the mono- and bipolar method, resulted in an improvement which lasted until the last follow-up examination and one month after the end of the therapy. Therefore, the research demonstrated that the therapy involving electromagnetic field with radiofrequency improved facial skin hydration in women of different age groups.
REFERENCES
- el-Domyati M, el-Ammawi TS, Medhat W et al. Radiofrequency facial rejuvenation: Evidence-based effect. Acad Dermatol. 2011;64(3):524–535. doi: 10.1016/j.jaad.2010.06.045. Mar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sukal SA. Thermage, the nonablative radiofrequency for rejuvenation. Clin Derm. 2008;26(6):602–607. doi: 10.1016/j.clindermatol.2007.09.007. [DOI] [PubMed] [Google Scholar]
- Yokohama Y, Akita H, Hesegawa S et al. Histologig study of collagen and stem cells after radiofreqency treatment for aging skin. Dermatol Surg. 2014;40:390–397. doi: 10.1111/dsu.12443. [DOI] [PubMed] [Google Scholar]
- Paasch U, Bodendorf M, Grunewald S et al. Skin rejuvenation radiofrequency therapy: methods, effects and risk. J Dtsch Dermatol. 2009;7:196–203. doi: 10.1111/j.1610-0387.2008.06780.x. [DOI] [PubMed] [Google Scholar]
- Shapiro S, Eros Y, Abrahami Y et al. Evaluation of safety and efficacy of the TriPollar technology for treatment of wrinkles. Lasers Surg Med. 2012;44:453–458. doi: 10.1002/lsm.22044. [DOI] [PubMed] [Google Scholar]
- Elsaie ML. Cutaneous remodelling and photorejuvenation using radiofrequency devices. Indian J Dermatol. 2009;930:283–294. doi: 10.4103/0019-5154.55625. May; 33. Epub 2009 May 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Addor FA, Aoki V. Skin barrier in atopic dermatitis. An Bras Dermatol. 2010;85(2):184–194. doi: 10.1590/s0365-05962010000200009. Mar-Apr. [DOI] [PubMed] [Google Scholar]
- Firooz A, Sadr B, Babakoohi S Variation of biophysical parameters of the skin with age, gender and body region. 2012. p. 386936. Scientific World Journal. [DOI] [PMC free article] [PubMed]
- Man MQ, Xin SJ, Song SP. Variation of skin surface pH, sebum content and stratum corneum hydration with age and gender in large Chinese population. Skin Pharma. Physiol. 2009;22(4):190–199. doi: 10.1159/000231524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tagami H. Location-related differences in structure and function of the stratum corneum with special emphasis on those of the facial skin. Int J Cosmet Sci. 2008;30:413–434. doi: 10.1111/j.1468-2494.2008.00459.x. [DOI] [PubMed] [Google Scholar]
- Kleesz P, Darlenski R, Fluhr JW. Full-body skin mapping for six biophysical parameters: baseline values at 16 aatomical sites in 125 human subjects. Skin Pharmacol Physiol. 2012;25(1):25–33. doi: 10.1159/000330721. [DOI] [PubMed] [Google Scholar]
- Mayrovitz HN, Bernal M, Brlit F et al. Biopysical measures of skin tissue water: variations within and among anatomical sites and correlations between measures. Skin Res Technol. 2013;19:47–54. doi: 10.1111/srt.12000. [DOI] [PubMed] [Google Scholar]
- Mohammed D, Matts PJ, Hadgraf J, Lane MF. Variation of stratum corneum biophysical and molecular properties with anatomic site. AAPS J. 2012;14(4):806–812. doi: 10.1208/s12248-012-9400-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cravello B, Ferri A. Relationships between skin properties and environmental parameters. Skin Res Technol. 2008;14:180–186. doi: 10.1111/j.1600-0846.2007.00275.x. [DOI] [PubMed] [Google Scholar]
- O’Goshi K, Serup J, Inter-instrumental variation of skin capacitance measured with the Corneometer. Skin Res Technol. 2005;11(2):107–109. doi: 10.1111/j.1600-0846.2005.00086.x. [DOI] [PubMed] [Google Scholar]
- Machado M, Hadgraft J, Lane ME. Assessment of the variation of skin barrier function with anatomic site, age, gender and ethnicity. Int J Cosmet Sci. 2010;32:397–409. doi: 10.1111/j.1468-2494.2010.00587.x. [DOI] [PubMed] [Google Scholar]
- Alster TS, Tanzi E. Improvement of neck and cheek laxity with a nonablative radiofrequency device: a lifting experience. Dermatol Surg. 2004;30:503–507. doi: 10.1111/j.1524-4725.2004.30164.x. [DOI] [PubMed] [Google Scholar]
- Ruiz-Esparza J. Nonablative radiofrequency for facial and neck rejuvenation. A faster, safer, and less painful procedure basedon concentrating the heat in key areas: the ThermaLift concept. J Cos Dermatol. 2006;5:68–75. doi: 10.1111/j.1473-2165.2006.00226.x. [DOI] [PubMed] [Google Scholar]
- Alster TS, Lupton JR. Nonablative cutaneous remodeling using radiofrequency devices. Clin Dermatol. 2007;25:487–491. doi: 10.1016/j.clindermatol.2007.05.005. [DOI] [PubMed] [Google Scholar]
- Atiyeh BS, Dibo SA. Nonsurgical nonablative treatment of aging skin: radiofrequency technologies between aggressive marketing and evidence-based efficacy. Aesthetic Plast Surg. 2009;33:283–294. doi: 10.1007/s00266-009-9361-9. [DOI] [PubMed] [Google Scholar]
- Bogle MA, Ubelhoer N, Weiss RA et al. Evaluation of the multiple pass, low fluence algorithm for radiofrequency tightening of the lower face. Lasers Surg Med. 2007;39:210–217. doi: 10.1002/lsm.20472. [DOI] [PubMed] [Google Scholar]