

Abstract
Objectives
Research and evidence‐based medicine (EBM) education are important elements of emergency medicine (EM) residency training; however, curricular time is limited and integrating novel strategies to engage learners and improve understanding of complex concepts is challenging. We sought to develop a unique research escape hunt educational experience to teach EM residents basic research and EBM skills using an active‐learning, team‐based strategy.
Methods
A nine‐station escape room–scavenger hunt was designed around educational content including (1) predictive statistics and diagnostic test characteristics, (2) interpretation of data and statistical analysis, (3) study design, (4) informed consent for research, and (5) the ethical principles guiding research. Stations required participants to use a variety of strategies to solve puzzles, with a correct response required to progress through the escape hunt. Teams worked together to solve each station's puzzles, with opportunities to reinforce the content in real time. Subsequent sessions were presented in a virtual format using Zoom breakout rooms over the past 2 years.
Results
Postactivity assessments were grounded in Kirkpatrick's model and focused on participants' reactions, learning, and behavior. Participants reported high levels of satisfaction (100% [21/21] “satisfied” or “extremely satisfied”) and engagement (95% [20/21] “engaged” or “very engaged”) with the activity, as well as increased comfort with the research and EBM concepts covered (91% [19/21] “agree” or “strongly agree” increased comfort), and demonstrated improvements in knowledge across each content area presented (91% [19/21]).
Reflective Discussion
This practical, team‐based curriculum was found to be a successful way to engage residents with research methodology and EBM content. This curriculum is feasible for both in‐person and virtual formats and we will continue to use this as a component of our EM residency program moving forward.
NEED FOR INNOVATION
Research and evidence‐based medicine (EBM) education are important parts of emergency medicine (EM) residency training and the Accreditation Council for Graduate Medical Education (ACGME) identifies scholarly activity as a core requirement for EM; however, curricular time is limited and integrating novel strategies to engage learners and improve understanding of complex concepts is challenging. Likewise, EM milestones call for an evidence‐based practice and the ability to critically appraise evidence. 1 However, no standardized approach is used to deliver this vital content. 2 , 3 , 4 , 5 We hypothesized that a more interactive format would increase engagement from our learners and allow us to reinforce concepts that had appeared elsewhere in the curriculum.
BACKGROUND
EM training programs take a variety of approaches to addressing the requirement for education related to research and EBM and there is not a standard, widely accepted curriculum available. 2 , 3 , 4 , 5 When presented in a typical lecture format, we found that engagement from our learners was quite limited. We are aware of EM and other training programs where an escape hunt has been used to present educational content; however to date we do not believe that this format has been applied to these topics. 6 , 7 , 8
OBJECTIVE OF INNOVATION
We sought to develop and pilot a research escape hunt to teach EM residents: (1) predictive statistics and diagnostic test characteristics, (2) interpretation of data and statistical analysis, (3) study design, (4) informed consent for research, and (5) the ethical principles guiding research. These content domains were chosen by senior EM faculty with extensive research and EBM experience including our research director (TDS), director of quality improvement, and department chair. Escape hunts have demonstrated efficacy for other EM content, and we anticipated that this learning format would support our educational goals.
DEVELOPMENT PROCESS
To encourage resident engagement with research and EBM educational content, we considered ways to incorporate active, participatory learning experiences. Participatory learning experiences engage adults both cognitively and affectively. 8 David Kolb's Experiential Learning Theory posits that adults are experiential learners who learn through active participation in and reflection on an activity or experience. 9 Kolb describes four stages of experiential learning, including concrete experience, observations and reflections, formalization/generalization of concepts, and testing concepts in new situations. We hypothesized that active participation in an escape room–scavenger hunt experience would provide our residents with an educational experience that they would identify as both an engaging and a satisfying way to learn this material. Topics were identified by the research division within our department as those most amenable to this educational modality as well as those which residents had previously shown the most difficulty understanding. A nine‐station escape room–scavenger hunt hybrid was developed around the content. Each station focused on one topic, for example, on understanding diagnostic test characteristics or on identifying and applying the principles of the Belmont Report. Stations required participants to use a variety of strategies to solve a puzzle or series of puzzles, with correct responses contributing toward unlocking the station's combination lock. Examples of strategies used include completing mathematical computations, responding to multiple choice questions, completing crossword puzzles, and participating in black light–invisible ink pen activities. Successfully “cracking the code” and unlocking each station's lock revealed a small reward (e.g., chocolate) and provided the team with a station‐completed “ticket” and location of the team's next station. Content within each domain was designed to be challenging for junior residents and those with minimal prior exposure to clinically oriented research.
IMPLEMENTATION PHASE
One week prior to the event, participants were provided with preparatory educational materials to review including summary sheets and podcast links, with instructions to review the material prior to the event. The escape hunt was held as the last session on our didactic day. Participants were instructed to come to our administrative office building and divide up into teams of no more than five players. Teams included representation from across postgraduate year (PGY) of training. Faculty members were present in the building, where nine spaces (e.g., faculty offices, conference rooms) had been set up as individual stations. To begin the game, each team was provided with a score sheet and an envelope containing the location of their first station. Teams worked together to solve each station's puzzles, rotating through each station as the escape hunt progressed. Faculty members were present to help guide teams through the stations and to reset stations and locks with each successful completion. The first team to successfully complete all nine stations, accumulating the most points for correct responses, was declared the game winner and received a prize.
Following the event, learners participated in a debriefing, including a review of the rationale for all correct puzzle responses. Postactivity assessments were grounded in Kirkpatrick's evaluation model and focused on participants' reactions, learning, and behavior. 10 To assess reactions to the event, participants were asked to respond to Likert‐type items focused on satisfaction with the event, engagement with the event and material, and comfort with the research and EBM concepts covered during the event. Individual participants self‐reported acquisition of new knowledge across each covered domain using Likert‐type items, for example, “I gained knowledge about interpreting visual displays of data through this event” (strongly agree through strongly disagree response options). To assess later behavioral change, participants were asked to provide examples of how they applied the knowledge gained in practice. In addition, we assessed the degree to which residents found that the escape hunt activity mirrored aspects of clinical practice, such as working as a team, delegating tasks, and brainstorming. 8 This project was exempted by the MaineHealth Institutional Review Board.
A COVID‐impacted event was held in 2 subsequent years utilizing Zoom breakout rooms. The preparatory materials were presented in a similar format utilizing Canvas, our learning management software. During the session, teams were placed into assigned breakout rooms to ensure each team had a mix of PGY, rotating medical student, and prior research training experience levels. A Google Form was then used to present questions and supporting materials to the group (Figure 1). The Google Form was created so that the group could not proceed until a correct answer to the question was identified. A Google Sheet was also used to create a crossword puzzle allowing for free‐text entry of appropriate answers. New questions and case‐based scenarios were used for each event to keep content fresh and prior participants challenged. Downloadable versions of our virtual escape hunt and an exemplar crossword puzzle are available at: https://www.dropbox.com/sh/vxllzjntx11wiqf/AADFYOzEffc3kXJIVdKMYIuwa?dl=0
FIGURE 1.
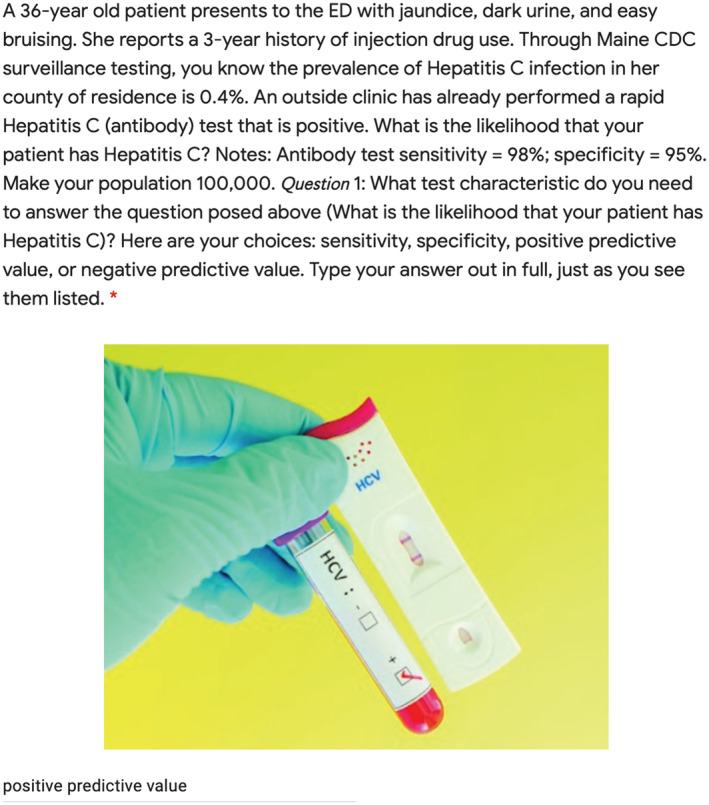
Google Form used to present question on test characteristics.
OUTCOMES
Twenty‐one EM resident physicians (six PGY‐1 [29%], seven PGY‐2 [33%], eight PGY‐3 [38%]) participated in the initial escape hunt event for which a postparticipation survey was completed. Participants reported high levels of satisfaction (100% [21/21] “satisfied” or “extremely satisfied”) and engagement (95% [20/21] “engaged” or “very engaged”) with the activity, reported increased comfort with the research and EBM concepts covered (91% [19/21] “agree” or “strongly agree” increased comfort), and demonstrated improvements in knowledge across each content area presented (91% [19/21]). In addition, participants reported that skills and strategies used during the escape hunt were similar to those used in clinical practice including “working as a team,” “task switching,” “task delegation,” “brainstorming,” and “solving complex problems together.” In response to query about how knowledge gained in the event was applied in practice, open‐ended responses included “I used the calculations we practiced to determine the negative predictive value of my patient's negative COVID rapid test” and “I was able to apply what we learned about interpreting forest plots to understanding one of our journal club articles this month.” Additionally, we were able to demonstrate that an escape‐hunt format was possible using a virtual format.
REFLECTIVE DISCUSSION
While we are aware of prior implementation of escape room and escape hunt models for the delivery of EM content, to date we do not believe that this format has been used to present concepts related to research methodology and EBM. Prior attempts at teaching this material have been unable to engage our residents and did not offer them the opportunity to work with the concepts at the time of instruction. The team‐based structure of an escape hunt allowed our residents to engage with the content in an interactive way, discussing among themselves, asking questions of the faculty member, and calculating predictive statistics and test characteristics. The response from our trainees was that they found this format to be a significant improvement over a more traditional lecture‐based curriculum.
Limitations do exist. Although we have presented the research escape hunt three times, once in person and two times via Zoom, we were only able to collect participant survey data following the initial in person session. While we demonstrated that residents found the format engaging and perceived it to be educational, we did not have a means of assessing their long‐term knowledge retention. Curricular design challenges included the time necessary to develop the escape hunt materials, costs associated with first‐time purchase of materials, limitations on the space available to optimize the flow of the event, and the number of faculty required to ensure game progression. We now have a materials bank of curriculum and physical problem stimuli that can be used in the future for in person events, and we have successfully taught a COVID‐safe virtual event on two occasions demonstrating the adaptability and reproducibility of this format. Future work will focus on demonstrating knowledge acquisition and retention. We are happy to share our materials for other interested in implementing an in‐person or virtual research escape hunt.
CONFLICT OF INTEREST
The authors declare no potential conflict of interest.
Supporting information
Appendix S1. Supporting Information
Fallon TS, Germann CA, Anderson RS, Strout TD. The research escape hunt: An escape room–scavenger hunt for resident education. AEM Educ Train. 2022;6:e10833. doi: 10.1002/aet2.10833
Supervising Editor: Dr. Daniel Runde.
REFERENCES
- 1. ACGME . ACGME program requirements for graduate medical education in emergency medicine, effective July 1, 2019 . Available at: https://www.acgme.org/Specialties/Program‐Requirements‐and‐FAQs‐and‐Applications/pfcatid/7/Emergency. Accessed June 8, 2020.
- 2. Kirkpatrick A, Doran T, Mullins D, Gnugnoli D, Ashurst J. A national evaluation of scholarly activity requirements in osteopathic EM residency programs: survey of EM program directors. South Med J. 2019;112(5):259‐262. [DOI] [PubMed] [Google Scholar]
- 3. Oliver JJ, Ross JM, Davis WT, et al. The development of an emergency medicine resident research program in the United States military. Milit Med. 2019;184(11/12):e622‐e625. [DOI] [PubMed] [Google Scholar]
- 4. Geyer BC, Kaji AH, Katz ED, Jones AE, Bebarta VS. A national evaluation of the scholarly activity requirement in residency programs: a survey of emergency medicine program directors. Acad Emerg Med. 2015;22(11):1337‐1344. [DOI] [PubMed] [Google Scholar]
- 5. Kane BG, Totten VY, Kraus CK, et al. Creating consensus: revisiting the emergency medicine resident scholarly activity requirement. West J Emerg Med. 2019;20(2):369‐375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Zhang XC, Diemer G, Lee H, Jaffe R, Papanagnou D. Finding the ‘QR’ to patient safety: applying gamification to incorporate patient safety priorities through a simulated ‘escape room’ experience. Cureus. 2019;11(2):e4014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Diemer G, Jaffe R, Papanagnou D, Zhang XC, Zavodnick J. Patient safety escape room: a graduate medical education simulation for event reporting. MedEdPORTAL. 2019;15:10868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Zhang XC, Lee H, Rodriguez C, Rudner J, Chan TM, Papanagnou D. Trapped as a group, escape as a team: applying gamification to incorporate team‐building skills through an ‘escape room’ experience. Cureus. 2018;10(3):e2256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kolb DA. Experiential learning: experience as the source of learning and development. Prentice Hall; 1984. [Google Scholar]
- 10. Kirkpatrick DL. Evaluating training programs: the four levels. Berrett‐Koehler; 1994. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Supporting Information