

The risk of lymph node metastases from invasive submucosal (T1b) colorectal cancers > 1000 µm deep is 1.3 % according to the Japanese guideline 1 . Over 98 % of stage T1b cancers without evidence of lymphovascular invasion, poor differentiation, or budding have no associated lymph node metastases. Achieving an endoscopic R0 resection allows curative resection of the majority of stage T1b cancers. Although magnifying colonoscopy can diagnose stage T1b cancers, pathological evaluation using specimens from an R0 resection is more reliable. If a cancer is diminutive and possibly a stage T1b cancer, total excision for pathological evaluation may avoid surgical resection but, to be justified, must be safe and reasonable. Although endoscopic submucosal dissection is reliable for R0 resection, Fukuda et al. recently showed that underwater endoscopic mucosal resection (UEMR) can completely resect stage T1b lesions 2 . Endoscopic ultrasound (EUS) demonstrates the submucosa under the tumor, which facilitates decision-making about UEMR.
A 73-year-old man was referred because of a cecal lesion that was suspected to be an adenocarcinoma after biopsy. An outpatient colonoscopy revealed a 7-mm sessile cecal tumor. Magnifying narrow-band imaging using an EC-760ZP-W/M colonoscope (Fujifilm, Tokyo, Japan) with distal attachment (D-201-14304; Olympus, Tokyo, Japan) suggested a T1b cancer ( Fig. 1 ; Video 1 ). EUS (EU-ME1; Olympus) clearly demonstrated residual submucosa under the tumor. When the cecum contracted, the muscularis became recessed circumferentially, with a thickened submucosa on EUS imaging. This transformed the lesion into a floating subpedunculated tumor in the underwater endoscopic view ( Fig. 2 ), which suggested that complete endoscopic resection using UEMR for complete pathological evaluation would be both safe and feasible on an outpatient basis. UEMR was completed without complications ( Fig. 3 ). Pathologic evaluation revealed a submucosal invasive adenocarcinoma with negative margins ( Fig. 4 ).
Fig. 1.
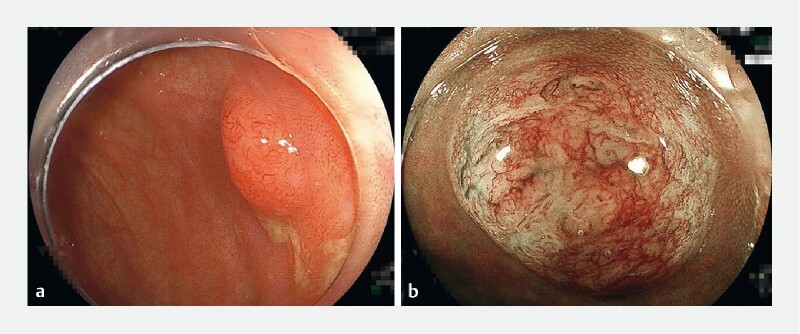
Images from magnifying narrow-band imaging (NBI) of a cecal lesion showing: a a 7-mm sessile tumor without a demarcated depressed area, which initially resembled a sessile serrated lesion and was suspected to be an adenocarcinoma on a previous biopsy; b under blue light, a vascular pattern with both interruption of thick vessels and loose vascular areas, and a surface pattern with amorphous areas, which was classified as type 3 (the Japan NBI Expert Team classification), consistent with a diagnosis of deep submucosal invasive cancer.
Fig. 2.
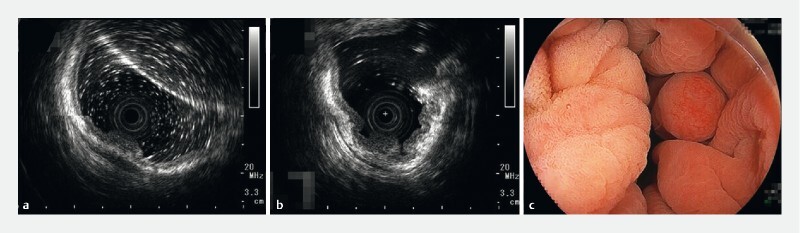
Endoscopic ultrasound using a 20-MHz miniature probe showing: a a high echoic submucosal layer between the tumor and the muscularis during insufflation; b when the cecum contracted while still under water, the muscularis becoming circumferentially recessed and the submucosa becoming thicker, with the tumor appearing to float on the submucosa. c On underwater endoscopic view, the tumor was transformed from a sessile tumor to a floating subpedunculated tumor.
Fig. 3.
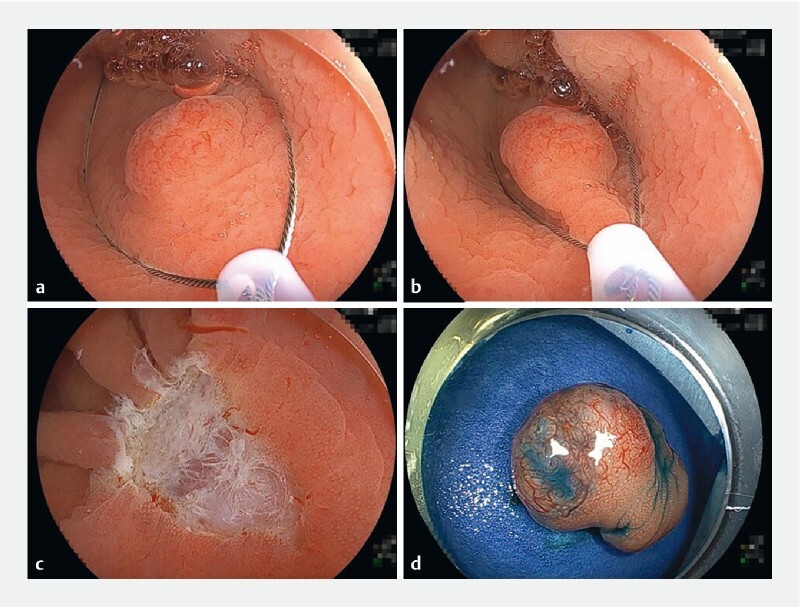
Sequential pictures of the underwater endoscopic mucosal resection of the tumor showing: a the tip of the snare (15-mm Rota snare; Medi-Globe GmbH, Achenmühle, Germany) securely placed on the normal mucosa beyond the tumor with a sufficient proximal margin; b the snare being gradually closed, while confirming it was capturing the entire tumor with its surrounding normal mucosa and aspirating the water, with the completely captured tumor then cut with pure cut mode diathermy (ESG-100; Olympus); c no residual lesions around the mucosal defect, meaning endoscopic en bloc resection had been achieved, and the mucosal defect was closed with a reopenable clip (Sureclip Plus; Micro-Tech Co. Ltd., NanJing, China) and endoclips (EZ-clip; Olympus); d the resected specimen.
Fig. 4.
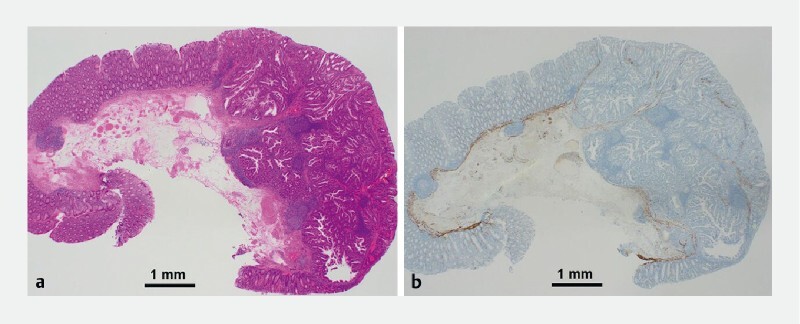
Histopathological views (× 40 magnification) showing: a on hematoxylin and eosin staining, a well-to-moderately differentiated deeply invasive submucosal adenocarcinoma, with no lymphovascular invasion and a negative vertical margin; b on desmin staining, absence of the muscularis mucosa, with submucosal invasion to a depth of 3 mm.
Video 1 Underwater endoscopic mucosal resection is performed for an endoscopically identified deeply invasive cancer after it has been confirmed to be both safe and feasible on endoscopic ultrasound.
This patient demonstrates that a stage T1b cancer can be safely and completely resected with UEMR after first confirming the submucosal characteristics using EUS. Indiscriminate EMR and/or cold snare polypectomy should be avoided for such lesions.
Endoscopy_UCTN_Code_TTT_1AQ_2AD
Footnotes
Competing interests H. Yamamoto is a consultant for Fujifilm Corporation and has received honoraria, a grant, and royalties from the company. The remaining authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Hashiguchi Y, Muro K, Saito Y et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol. 2020;25:1–42. doi: 10.1007/s10147-019-01485-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fukuda H, Takeuchi Y, Shoji A et al. Curative value of underwater endoscopic mucosal resection for submucosally invasive colorectal cancer. J Gastroenterol Hepatol. 2021;36:2471–2478. doi: 10.1111/jgh.15513. [DOI] [PubMed] [Google Scholar]