

Abstract
Primary leptomeningeal medulloblastoma (PL-MB) in adults is a rare disease with a severe prognosis. A 35-year-old woman presented with headaches, diplopia, and gait ataxia, with triventricular hydrocephalus and descent of the cerebellar tonsils beyond the foramen magnum. Endoscopic third ventriculostomy was performed. Six months later, headaches recurred. Dilatation of the supratentorial ventricular system and massive cerebellar swelling without contrast-enhancing nodularities were reported. Occipitocervical decompression with duraplasty was performed. A bioptic diagnosis of PL-MB was made. Craniospinal irradiation and chemotherapy were administered. After 18 months, no recurrence was observed.
Few cases of PL-MB have been reported: patients die before treatment or within a few days after surgery. Our long-term survival could be ascribable to a slow clinical presentation and an early diagnosis that allowed surgical treatment and the administration of a combined chemoradiotherapy protocol. Cerebellar swelling, even without associated enhancing lesions, with or without hydrocephalus, should be a neuroradiological alarm sign, and PL-MB should be considered.
Keywords: Chiari-like malformation, endoscopic third ventriculostomy, obstructive hydrocephalus, occipitocervical decompression, primary leptomeningeal medulloblastoma
Key Messages
PL-MB is a rare disease with a severe prognosis. Cerebellar swelling, independent of the presence of nodular enhancing lesions and hydrocephalus, should be considered a neuroradiological alarm sign. Although uncommon, in the case of leptomeningeal involvement, MB should be considered as a differential pathological diagnosis.
Introduction
Medulloblastoma (MB) is a malignant neuroepithelial tumor that originates from primitive neuroectodermal tissue. 1 2 In most cases, it occurs as a mass lesion in the vermis or hemispheres of the cerebellum. 1 3 Although MB commonly metastasizes along the cerebrospinal fluid (CSF) pathway 4 and subarachnoid seeding is found in up to one-third of patients at diagnosis, 5 primary leptomeningeal medulloblastoma (PL-MB) without any evidence of a tumor mass is exceedingly rare, 5 and only a few cases have been reported in the literature. 4 5 6 7 8 9 10 11 12
Herein, we report the unusual occurrence of a pathologically-confirmed PL-MB in an adult woman, focusing on the differential diagnosis implications and on the good clinical outcome compared with other reports in the literature.
Case History
A 35-year-old woman experienced headaches and diplopia over the course of 2 years. Due to the onset of gait ataxia and worsening of the headaches (that became continuous and invalidating), she underwent magnetic resonance imaging (MRI). This study demonstrated the presence of triventricular hydrocephalus with transependymal transudation and downward displacement of the cerebellar tonsils beneath the foramen magnum into the cervical spinal canal with obstruction of the fourth ventricle, similar to a Chiari malformation ( Fig. 1 ). The patient underwent endoscopic third ventriculostomy (ETV) through a right-sided burr hole. Postoperative computed tomography (CT) scans excluded any complications, and the patient was discharged 3 days after the endoscopic procedure with prompt amelioration of her presenting symptoms. The neuroradiological follow-up 1 month later demonstrated a decrease in the size of the third and lateral ventricles, with resolution of the transependymal transudation and reduction in the cerebellar ectopia ( Fig. 2 ). Fast spin-echo sequences revealed the patency of the stoma on the floor of the third ventricle and the regular flow void inside it. Six months after surgery, the patient lamented the onset of mild headache. The neuroradiological investigations documented mild dilatation of the supratentorial ventricular system, downward displacement of the cerebellar tonsils, and widened cerebellar folia. Some areas of hyperintensity were identified in fluid-attenuated inversion recovery (FLAIR) sequences, but no contrast enhancement was documented ( Fig. 3 ). Thus, although atypical and infrequent, a Lhermitte-Duclos disease with involvement of both cerebellar hemispheres and vermis was suspected, and occipitocervical decompression with duraplasty was performed. Intraoperatively, the cerebellum was found to be extremely swollen, but no gross tumor mass was observed. Multiple biopsies were taken from both cerebellar tonsils and both cerebellar hemispheres. Histological examination of the tumor fragments from all the sampled areas showed a dense population of atypical small cells arranged in loosely cohesive sheets located within the subarachnoid space, extending through the Virchow-Robin spaces, and focally infiltrating the subjacent cerebellar parenchyma ( Fig. 4A ). The tumor cells exhibited moderately pleomorphic round to ovoid hyperchromatic nuclei with scant cytoplasm, and many mitotic figures were observed ( Fig. 4B ). Immunohistochemical staining revealed positivity for microtubule-associated protein-2 (MAP2) and synaptophysin ( Fig. 4C ), and negativity for CKAE1/AE3, glial fibrillary acid protein (GFAP), P53, transcription thyroid factor-1 (TTF-1), and CD45 in the neoplastic cells. The Ki-67 labelling index was approximately 30% ( Fig. 4D ). Considering the morphologic and immunohistochemical profile of the leptomeningeal infiltrate, the lesion was considered consistent with a classic MB. Two weeks after surgery, an examination of the CSF was performed, and no neoplastic cells were found and no abnormalities in physicochemical parameters were recorded. After the exclusion of areas of FLAIR-hyperintensity and contrast enhancement on whole-spine MRI, the patient was referred for adjuvant therapy. She was treated with irradiation at a dose of 32.4 Gy to the craniospinal axis followed by a 23.4 Gy boost to the posterior fossa (1.8 Gy/fr). Postradiation MRI showed persistent cerebellar hyperintensity, and six courses of platinum/etoposide-based chemotherapy were administered. Eighteen months later, the patient did not have any symptoms, and no neuroradiological recurrence was observed ( Fig. 5 ).
Fig. 1.
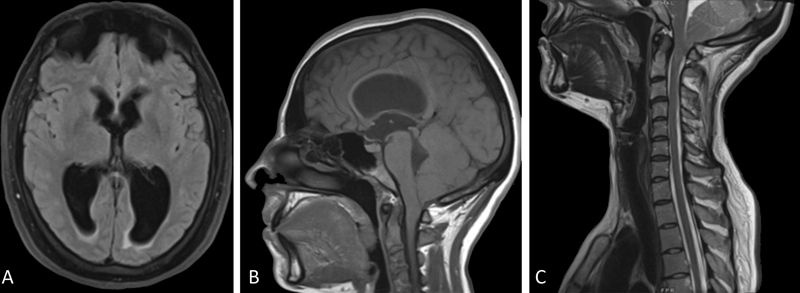
Preendoscopic third ventriculostomy magnetic resonance imaging. The neuroradiological investigations documented triventricular hydrocephalus with signs of transependymal transudations ( A ). On the sagittal scans, a mild dilatation of the aqueduct ( B ) and downward displacement of the cerebellar tonsils beyond the foramen magnum with obstruction of the fourth ventricle ( C ) were evidenced.
Fig. 2.
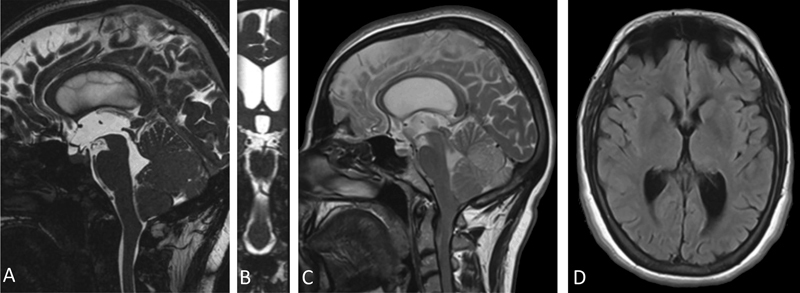
Postendoscopic third ventriculostomy magnetic resonance imaging. The postoperative images documented the patency of the stoma on the floor of the third ventricle ( A, B ), with a regular flow inside it ( C ) and a reduction in the dilatation of the lateral ventricles with resolution of the transependymal transudation ( D ).
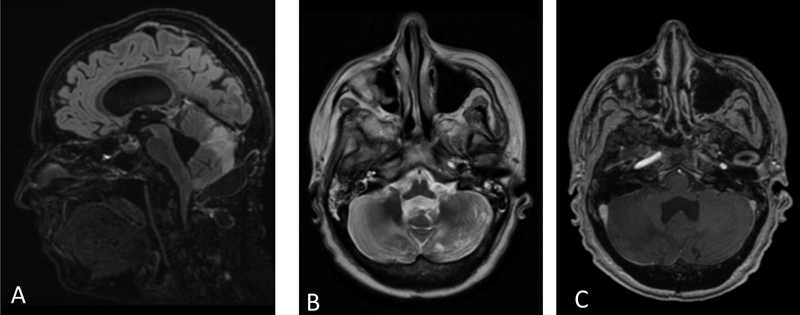
Fig. 3.
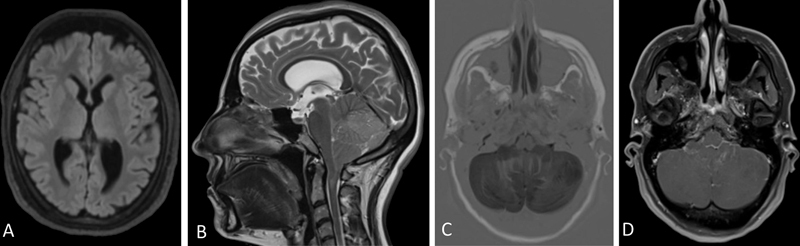
Magnetic resonance imaging at 6 months. Mild triventricular dilatation ( A ) and downward displacement of the cerebellar tonsils ( B ) were associated with areas of hyperintensity in both cerebellar hemispheres and vermis and diffuse cerebellar swelling ( C ). No contrast enhancement was documented ( D ).
Fig. 4.
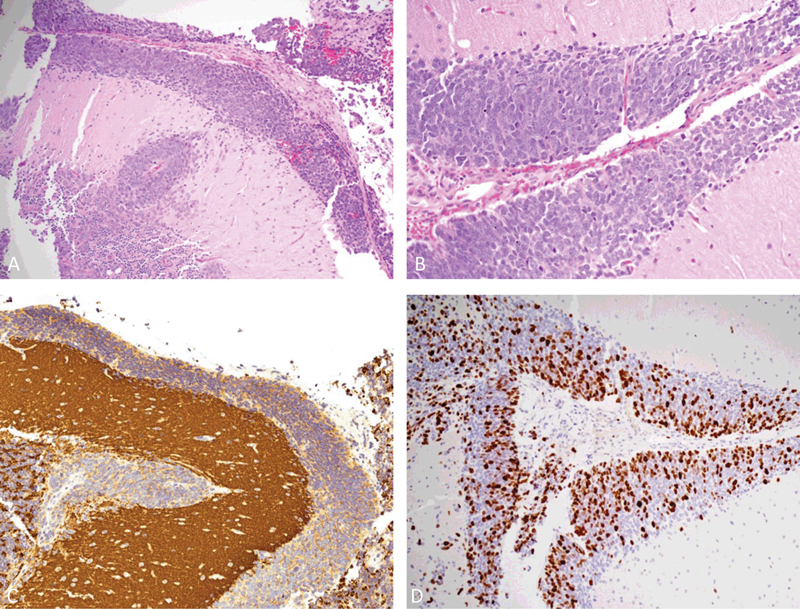
Histological and immunohistochemical specimens. The hematoxylin and eosin-stained section ( A ) showed the neoplastic infiltrate within the subarachnoid space (original magnification 100 × ). A higher magnification ( B ) revealed the neoplastic cells with large, round-oval nuclei, and scant cytoplasm (original magnification 400 × ). The immunohistochemical staining documented the positivity for synaptophysin ( C ) and a high proliferation index ( D ).
Fig. 5.
Follow-up magnetic resonance imaging. The patient underwent craniospinal irradiation and subsequent chemotherapy. The sagittal scans ( A ) documented a resolution of the downward displacement of the cerebellar tonsils with enlargement of the fourth ventricle and distension of the cerebellar folia. No evolution of the cerebellar hyperintensities was documented ( B ). No area of contrast enhancement was evidenced ( C ).
Discussion
MB is a posterior fossa embryonal tumor that represents the most common brain malignancy in children. 1 2 3 It accounts for 12 to 25% of central nervous system (CNS) neoplasms in childhood and 1% in adults. 1 2 3 Three-quarters of MB arise from the cerebellar vermis and tend to protrude into the fourth ventricle, although the site of origin in adults is commonly the cerebellar hemispheres. 13 Of all primary CNS tumors, MB has the greatest propensity for local, regional, and distant spread. 14 It may spread locally to adjacent structures (brainstem, upper spinal cord, midbrain, and cerebellar surface) or invade the subarachnoid space to form an icing-like layer of neoplastic cells on the pial surface. 14 Metastases, through the CSF pathway, manifest as supratentorial implants, spinal cord lesions, and malignant cells within the CSF. 14 15 Dissemination of tumor cells can occur at any time. 5 In most cases, it appears to be secondary to the primary mass. 7 16 Although subarachnoid seeding is common, occurring in approximately 33% of MB at the time of diagnosis, 5 purely diffuse leptomeningeal tumor spread without mass lesion in an adult patient is rare, 4 5 6 7 8 9 10 11 12 17 and has, to the best of our knowledge, been only reported few times in the literature, 4 5 6 7 8 9 10 11 12 and all the described patients had very unfavorable prognosis. 4 5 6 7 8 9 10 11 12
Generally, PL-MB manifests with headache 4 6 8 10 12 18 and visual abnormalities 4 6 8 10 18 lasting a few months, and may also result in rapid neurologic deterioration. 8 9 11 12 In particular, Hankey et al 4 described the case of a 39-year-old woman presenting with a month-long history of headaches, slurred speech, ataxia, memory impairment, and olfactory and auditory hallucinations. Headache and blurred vision lasting a few months were reported in an 8-year-old boy 10 and in a 22-year-old man. 6 In both patients, MRI revealed an intense leptomeningeal enhancement of the cerebellar folia and cerebral convexities, and a suboccipital craniotomy was performed. 6 10 A more rapid neurological deterioration, following several weeks of premonitory signs, such as headache and vomiting, 12 neck pain, 11 diplopia, and tinnitus, 8 has been reported in other cases. 8 9 11 12 This difference in symptom progression could explain the difference in overall survival between our patient and the others. In particular, our subject presented with a long story of headaches and diplopia and did not present any episodes of consciousness reduction. Thus, we initially treated her for chronic triventricular hydrocephalus, similar to the authors who used a ventriculoperitoneal shunt. 8 16 In contrast, in subjects with rapid neurological deterioration, Rushing et al 11 preferred an external ventricular drainage for an acute-onset hydrocephalus, while Ferrara et al 7 and Guo et al 8 opted for an emergent posterior fossa decompression.
Contemporary evaluation procedures in MB include MRI of the brain and spinal cord, histological examination of biopsy or resected tumor specimens, and analysis of CSF cytology. 14 On MRI, MB appears as a heterogeneous enhancing well-defined mass lesion, 5 13 16 often with surrounding cystic degeneration of necrosis. 5 It is generally iso- or hyperintense on FLAIR and T2-weighted sequences, and commonly appears heterogeneous because of cyst formation, calcification, and necrosis. 13 Diffusion-weighted imaging shows restricted diffusion, while spectroscopy demonstrates elevated choline peaks and decreased creatinine and N-acetylacetate peaks, with occasional elevation in lactic acid and lipid contents. 13 However, in rare cases, leptomeningeal enhancement without a detectable intraparenchymal mass is apparent. 7 9 10 11 12 Gadolinium-enhanced T1-weighted and FLAIR sequences have been suggested. 11 19 While some authors have demonstrated the presence of contrast-enhancing leptomeninges on CT 4 7 and MRI, 6 8 9 10 12 in our case, no variation was recognized after contrast administration both before and after the endoscopic procedure. Our neuroradiological investigations demonstrated only a Chiari-like malformation 11 16 with triventricular hydrocephalus 6 11 16 and nonspecific cerebellar swelling with some hyperintensities in FLAIR and T2-weighted sequences. 9 11
Excluding an autoptic pathological diagnosis in a 30-year-old male, 11 a bioptical sample was obtained. 4 6 7 8 9 10 12 The differential diagnosis of a lesion that involves only the leptomeninges is quite wide and includes metastasis (meningeal carcinomatosis), especially in adults, primary brain tumors (gliomas and mixed glioneuronal tumors such as the recently described diffuse leptomeningeal glioneuronal tumor), and infectious and noninfectious meningitis. 1 Histologically, in a case showing this morphology ( Fig. 4 ) and occurring in an adult patient, the diagnosis of a metastatic small cell lung cancer or lymphoma has to be ruled out; negative immunostaining for cytokeratins, TTF-1, and CD45 excluded these entities.
In meningeal pathology without mass formation, CSF cytology studies are considered the most useful step in clinical diagnosis. 20 Some authors have demonstrated the presence of neoplastic cells in the CSF. 7 10 18 Similar to others, 4 6 9 in our case, no neoplastic cells were identified in the CSF sample.
Despite advances in multimodal therapy, the 5-year survival rate of patients with MB still ranges from 50 to 70%. 5 Subjects with PL-MB generally die a few days after surgery 4 10 12 or deteriorate before any treatment. 9 11 Only Guo et al 8 reported a case of a 21-year-old man who underwent craniospinal irradiation and died 6 months after diagnosis. No long-term survivor was described, with the exception of our patient, who underwent both craniospinal irradiation and chemotherapy. Our good outcome could be attributed to the slow progression of the symptoms. This allowed for early identification of cerebellar swelling before the onset of any contrast-enhancing nodularity. Thus, the patient was referred to an early combined chemoradiotherapy protocol.
In conclusion, PL-MB is a rare disease with a severe prognosis. Contemporary evaluation should include cranial and spinal MRI with and without contrast administration and CSF analysis. Our experience underlines the importance of maintaining a degree of suspicion for leptomeningeal tumors in patients with Chiari-like neuroradiological images, cerebellar swelling, and obstructive hydrocephalus. Moreover, cerebellar swelling, independent of the presence of nodular enhancing lesions and hydrocephalus, should be considered a neuroradiological alarm sign. Even if subarachnoid neuroepithelial neoplasm is an extremely uncommon presentation, in the case of leptomeningeal involvement, MB should be considered as a differential pathological diagnosis.
Footnotes
Conflict of Interest None declared.
References
- 1.Louis D N, Perry A, Reifenberger G. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(06):803–820. doi: 10.1007/s00401-016-1545-1. [DOI] [PubMed] [Google Scholar]
- 2.Roberts R O, Lynch C F, Jones M P, Hart M N. Medulloblastoma: a population-based study of 532 cases. J Neuropathol Exp Neurol. 1991;50(02):134–144. doi: 10.1097/00005072-199103000-00005. [DOI] [PubMed] [Google Scholar]
- 3.Blessing M M, Alexandrescu S. Embryonal tumors of the central nervous system: an update. Surg Pathol Clin. 2020;13(02):235–247. doi: 10.1016/j.path.2020.01.003. [DOI] [PubMed] [Google Scholar]
- 4.Hankey G J, Khangure M S, Spagnolo D, Quinlan M F. Adult onset medulloblastoma cerebelli with leptomeningeal dissemination and coincidental primary hyperparathyroidism. Australas Radiol. 1989;33(01):111–115. doi: 10.1111/j.1440-1673.1989.tb03249.x. [DOI] [PubMed] [Google Scholar]
- 5.David K M, Casey A T, Hayward R D, Harkness W F, Phipps K, Wade A M. Medulloblastoma: is the 5-year survival rate improving? A review of 80 cases from a single institution. J Neurosurg. 1997;86(01):13–21. doi: 10.3171/jns.1997.86.1.0013. [DOI] [PubMed] [Google Scholar]
- 6.Asadollahi M, Shayanfar N, Rezaiyan B, Hasibi M. A rare presentation of medulloblastoma in adults as primary leptomeningeal involvement. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3829233/ Iran J Neurol. 2012;11(01):30–33. [PMC free article] [PubMed] [Google Scholar]
- 7.Ferrara M, Bizzozero L, Fiumara E, D'Angelo V, Corona C, Colombo N. “Primary” leptomeningeal dissemination of medulloblastoma. Report of an unusual case. https://pubmed.ncbi.nlm.nih.gov/2795197/ J Neurosurg Sci. 1989;33(02):219–223. [PubMed] [Google Scholar]
- 8.Guo X, Zhong D, Ma W. Primary leptomeningeal medulloblastoma: a rare case. Clin Neurol Neurosurg. 2012;114(08):1181–1184. doi: 10.1016/j.clineuro.2012.02.042. [DOI] [PubMed] [Google Scholar]
- 9.McGlacken-Byrne S M, Gorman K M, Lagan N K, Robinson I, Farrell M, King M D. Identification of leptomeningeal medulloblastoma with contrast-enhanced magnetic resonance imaging: a devastating differential of acute disseminated encephalomyelitis. J Paediatr Child Health. 2018;54(08):929–930. doi: 10.1111/jpc.14094. [DOI] [PubMed] [Google Scholar]
- 10.Mehta R I, Cutler A R, Lasky J L., III “Primary” leptomeningeal medulloblastoma. Hum Pathol. 2009;40(11):1661–1665. doi: 10.1016/j.humpath.2009.04.024. [DOI] [PubMed] [Google Scholar]
- 11.Rushing E J, Smith A B, Smirniotopoulos J G, Douglas A F, Zeng W, Azumi N. Occult leptomeningeal large cell medulloblastoma in an adult. Clin Neuropathol. 2009;28(03):188–192. doi: 10.5414/npp28188. [DOI] [PubMed] [Google Scholar]
- 12.Suman R, Santosh V, Anandh B A. Primary leptomeningeal medulloblastoma. Pediatr Neurosurg. 2007;43(06):544–545. doi: 10.1159/000108806. [DOI] [PubMed] [Google Scholar]
- 13.Millard N E, De Braganca K C. Medulloblastoma. J Child Neurol. 2016;31(12):1341–1353. doi: 10.1177/0883073815600866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ayan I, Kebudi R, Bayindir C, Darendeliler E. Microscopic local leptomeningeal invasion at diagnosis of medulloblastoma. Int J Radiat Oncol Biol Phys. 1997;39(02):461–466. doi: 10.1016/s0360-3016(97)00083-7. [DOI] [PubMed] [Google Scholar]
- 15.Rutka J T, Hoffman H J. Medulloblastoma: a historical perspective and overview. J Neurooncol. 1996;29(01):1–7. doi: 10.1007/BF00165513. [DOI] [PubMed] [Google Scholar]
- 16.Noiphithak R, Mektripop N, Thamwongskul C. Rapidly progressive medulloblastoma initially mimicking idiopathic intracranial hypertension and Chiari I malformation: a case report. Int J Surg Case Rep. 2021;85:106147. doi: 10.1016/j.ijscr.2021.106147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Packer R J. Childhood medulloblastoma: progress and future challenges. Brain Dev. 1999;21(02):75–81. doi: 10.1016/s0387-7604(98)00085-0. [DOI] [PubMed] [Google Scholar]
- 18.Kajtazi N I, Nahrir S, Al Shakweer W, Al Ghamdi J, Al Fakeeh A, Al Hameed M. Malignant idiopathic intracranial hypertension revealed a hidden primary spinal leptomeningeal medulloblastoma. BMJ Case Rep. 2021;14(07):e243506. doi: 10.1136/bcr-2021-243506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Griffiths P D, Coley S C, Romanowski C AJ, Hodgson T, Wilkinson I D. Contrast-enhanced fluid-attenuated inversion recovery imaging for leptomeningeal disease in children. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8148663/ AJNR Am J Neuroradiol. 2003;24(04):719–723. [PMC free article] [PubMed] [Google Scholar]
- 20.Budka H, Pilz P, Guseo A. Primary leptomeningeal sarcomatosis. Clinicopathological report of six cases. J Neurol. 1975;211(01):77–93. doi: 10.1007/BF00312466. [DOI] [PubMed] [Google Scholar]