

Abstract
Introduction and importance
Primary cardiac sarcoma is a rare malignancy with a poor prognosis because of diagnostic delay, therapeutic difficulties, and high metastatic potential. The therapeutic approach includes surgery, chemotherapy, and radiation therapy, alone or in combination. However, there is a lack of evidence to guide the treatment.
Case presentation
We present a case of primary cardiac sarcoma. Our patient was presented in the department of emergency medicine (ED) in our institute with shortness of breath on exertion associated with orthopnea. Based on the history and cardiovascular examination, he underwent an echocardiogram, which revealed a sizeable echogenic density in the right ventricular outflow tract. He underwent surgical resection of the cardiac mass via median sternotomy and total cardiopulmonary bypass approach. The patient was eventually diagnosed with primary cardiac sarcoma, confirmed by tissue biopsy after surgical intervention.
Clinical discussion
Through this report, we highlight the rarity of primary cardiac sarcomas, the importance of multidisciplinary tumor board (MDT) discussion and provide evidence of surgical excision being the treatment of choice, followed by systemic chemotherapy in selected cases.
Conclusion
Cardiac sarcoma is a rare but highly malignant tumor with a poor prognosis. However, early diagnosis and surgical resection of a primary cardiac sarcoma can significantly increase the patient's survival and quality of life. Therefore, physicians should keep a high suspicion of a patient with clinical features suggestive of cardiac sarcoma, and echocardiography should be the diagnostic modality of choice in such patients.
Keywords: Cardiac sarcoma, Malignancy, Surgery, Chemotherapy
Highlights
-
•
Primary Cardiac Sarcoma is a rare malignancy with a poor prognosis because of its highly malignant potential.
-
•
Evidence to guide treatment should be based on multidisciplinary tumor board (MDT) discussion.
-
•
Surgical excision followed by chemotherapy may improve survival and quality of life.
1. Introduction
Primary cardiac sarcoma is a rare and malignant tumor representing only 20 % of all primary cardiac tumors originating in the heart [1]. It has a very low incidence of 0.0017 to 0.0019 [2]. Its presentation depends on which cardiac chambers are involved. The right side of the heart is usually affected by these rare malignant tumors and is commonly identified by transthoracic echocardiography [3]. Most patients with cardiac sarcomas present with chest pain, fatigue, and dyspnea. Tumors with deep infiltration can cause superior vena cava syndrome or dysphonia because of recurrent laryngeal nerve palsy [4].
Elective cardiac sarcoma therapy consists of complete surgical excision, followed by radiation and a chemotherapeutic regimen [5]. The prognosis of cardiac sarcomas is poor, with median survival ranging from 9.6 to 16.5 months [6]. All the work has been reported in line with the SCARE 2020 criteria [7].
2. Case presentation
A 63-year-old gentleman with a history of hypertension and gastroesophageal reflux disease presented initially in the emergency department of our hospital with shortness of breath. Detailed history and physical examination were performed. His vital parameters showed a heart rate of 88 beats per minute, blood pressure of 134/82 mmHg, respiratory rate of 22 breaths per minute and temperature of 98 F. Cardiovascular examination revealed a pan-systolic murmur heard in the fourth intercostal space along the right sternal border. The rest of the systemic examination was unremarkable. Due to severe financial constraints and lack of funding and insurance, he refused any relevant investigation; hence he was managed conservatively. He then lost to follow-up and later presented in the clinic with shortness of breath on exertion, which had gradually worsened over the last six months. It was accompanied by mild to moderate nocturnal dyspnea. General physical examination was unremarkable at this time with the persistent cardiac murmur, appreciated on cardiovascular assessment.
He underwent clinically relevant limited laboratory investigations, which were within the normal reference ranges, except for his haemoglobin level, which was 9.6 g/dl. His echocardiography performed outside our institute showed a normal ejection fraction of 55–60 % with a moderately dilated right atrium and ventricle with severe tricuspid regurgitation. A large echogenic density was noted at the right ventricular outflow tract, extending into the main pulmonary artery, obstructing the pulmonary valve. Conventional angiography showed a large fixed mass at the posterior wall of the right ventricular outflow tract protruding into the main pulmonary artery (measuring 32 × 21.5 mm). Based on the history, physical examination, and imaging findings, we strongly suspected a primary cardiac tumor.
He underwent surgical resection of the tumor. Median sternotomy and total cardiopulmonary bypass approach was used with pulmonary valve repair under general anesthesia. A 2x2cm mass was removed, involving the pulmonary valve, but some tissue was left behind because of its invasion into the pulmonary artery wall. Histopathology of the samples taken from the mass showed a malignant neoplasm characterized by elongated cells exhibiting a moderate-to-severe degree of nuclear pleomorphism and hyperchromasia and frequent normal and abnormal mitotic figures (Fig. 1). The history, physical examination, and histopathological findings were conclusive of primary cardiac sarcoma of undifferentiated type.
Fig. 1.

Low power view of the tumor with pleomorphic cells showing abnormal mitotic figures (arrow). Hematoxylin and Eosin (H&E) stain 10 × 10.
A positron emission tomography (PET) performed four weeks after surgery showed a residual tumor in the right ventricle with a standardized uptake value of 6.4 (Fig. 2), and postoperative echocardiography showed a normal ejection fraction of 55–60 %, moderate tricuspid regurgitation, and moderate to severe pulmonary artery hypertension.
Fig. 2.
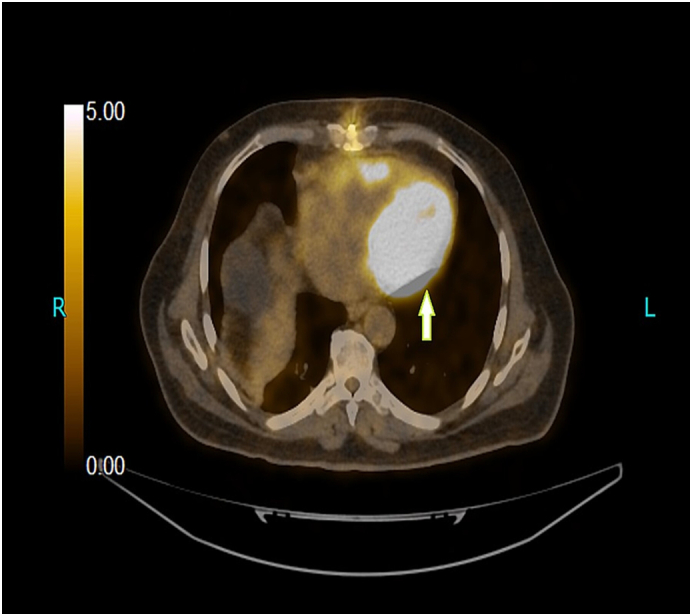
Positron emission tomography (PET) scan performed after surgery shows a hypermetabolic focus seen over the right ventricular wall with SUV-max of 6.4 (residual tumor). Non-homogeneous uptake is seen over the mediastinum, consistent with surgical intervention.
The patient's case was discussed in a multidisciplinary tumor (MDT) board meeting, and he was offered a single agent systemic chemotherapy i-e ifosfamide, with a dose of 2.5 g/m2 every three weeks. The patient has received a total of twenty-two cycles of systemic chemotherapy. A routine assessment was performed every three months, which includes history and physical, echocardiogram and imaging study. His recent scans showed improvement in the disease process, and his echocardiography showed marked improvement with a decrease in pulmonary artery hypertension and mild tricuspid regurgitation. His Eastern Cooperative Oncology Group (ECOG) score was one post-operatively which remained the same throughout his clinic follow-ups. Our management plan involved the continuation of palliative chemotherapy with a follow-up assessment at three months. However, after a year, the patient succumbed to COVID-19 pneumonia, developed multi-organ failure, and was put on comfort measures. Written informed consent was obtained from the patient's next kin for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
3. Discussion
Cardiac sarcomas, being rare malignant tumor of the heart with diverse symptoms and lack of awareness, usually have a late presentation. Although there has been advancement in modern technology to diagnose and treat the disease, it most frequently is detected in an advanced stage, contributing to the poor prognosis [8]. The most frequent cardiac sarcomas include liposarcomas, rhabdomyosarcoma, fibrosarcoma, leiomyosarcomas, angiosarcomas, synovial sarcomas, and undifferentiated sarcomas. The most common type is angiosarcoma arising in the right atrium with frequent pulmonary and distant metastases. Another tumor that involves the left atrium locally in an advanced state is an undifferentiated sarcoma [8].
Cardiac sarcomas are usually asymptomatic. However, when symptomatic, the most common findings are dyspnea, chest pain, and generalized fatigue. Precordial examination most commonly reveals a pansystolic murmur with a classic “tumor plop” sound during auscultation when it involves the mitral valve [9]. Diagnostic and staging modalities for assessing the tumor presence and local invasion include echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI). A study by Alam et al. suggests that a trans-oesophagal echocardiogram can be more helpful than a trans-thoracic echocardiogram in establishing the precise location of the tumor and its degree of extension. However, a chest CT scan can be used to visualize extra cardiac attachments. MRI can give a detailed view of myocardial and great vessel invasion assessment. After the tumor is suspected in imaging studies, a tissue biopsy is the standard gold test for diagnosis [10]. Early diagnosis and prompt treatment are associated with a good prognosis and greater chances of survival for up to 25 months [11]. Sometimes these rare tumors in the first phase of their growth can be misdiagnosed as other more known and frequent forms and therefore recur after initial treatment [12]. Hence such cases should be discussed in multidisciplinary tumor board meetings, whenever encountered.
Metastatic cardiac sarcomas are associated with a lower survival rate as compared to non-metastatic cardiac sarcomas, as reported by a case series by Simpson et al. of 34 cardiac sarcoma patients, in which the median survival period of patients without metastasis was found to be 15 months compared to patients with a metastatic disease which was only five months [13]. In addition, higher mortality is observed in patients with metastatic disease or who develop heart failure [14].
Surgery is the treatment of choice in early-stage disease and is used in the diagnostic evaluation of the tumor by obtaining a biopsy. Surgery also plays a palliative role in late-stage disease [15]. Centofanti et al. suggest an increase in the median survival rate in cardiac sarcoma patients in patients who have undergone complete resection of the tumor compared to incomplete resection or metastatic disease [16].
Research studies have shown no agreement on the efficacy of postsurgical therapy. However, chemotherapy is recommended even after total tumor resection because there is a chance of missed microscopic aggressive tumor cells and recurrence. Radiotherapy has not shown any benefits in patients having positive remnants after surgical resection, mitigation of localized disease or distant recurrence [16], [17].
4. Conclusion
Cardiac sarcoma is a rare but highly malignant tumor with a poor prognosis. However, early diagnosis and surgical resection of a primary cardiac sarcoma can significantly increase the patient's survival and quality of life. Therefore, physicians should keep a high suspicion of a patient with clinical features suggestive of cardiac sarcoma, and echocardiography should be the diagnostic modality of choice in such patients.
Ethical approval
The institution does not require ethical approval for this case report and images.
Funding
None.
Guarantor
Corresponding author is the Guarantor of this case report.
Research registration number
Not applicable.
Consent for publication
Written informed consent was obtained from the patient's next kin for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Patient's perspective
As per the patient's next kin, patient was very satisfied with his surgical procedure and the multidisciplinary tumor board meeting decisions and over all treatment. He paid kind regards to the whole team, involved in his treatment.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Declaration of competing interest
None declared.
Contributor Information
Saqib Raza Khan, Email: saqib.raza31@yahoo.com.
Saad Nasir, Email: saad.nasir@aku.edu.
Yasmin Abdul Rashid, Email: yasmin.rashid@aku.edu.
Adnan Abdul Jabbar, Email: adnan.jabbar@zu.edu.pk.
References
- 1.Kim M.P., Correa A.M., Blackmon S., et al. Outcomes after right-side heart sarcoma resection. Ann. Thorac. Surg. 2011;91(3):770–776. doi: 10.1016/j.athoracsur.2010.09.079. [DOI] [PubMed] [Google Scholar]
- 2.Devbhandari M.P., Meraj S., Jones M.T., Kadir I., Bridgewater B. Primary cardiac sarcoma: reports of two cases and a review of current literature. J. Cardiothorac. Surg. 2007;2(1):1–5. doi: 10.1186/1749-8090-2-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Neragi-Miandoab S., Kim J., Vlahakes G. Malignant tumours of the heart: a review of tumour type, diagnosis and therapy. Clin. Oncol. 2007;19(10):748–756. doi: 10.1016/j.clon.2007.06.009. [DOI] [PubMed] [Google Scholar]
- 4.Steger C.M., Hager T., Ruttmann E. International Scholarly Research Notices. Vol. 2012. 2012. Primary cardiac tumours: a single-center 41-year experience. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nakamura-Horigome M., Koyama J., Eizawa T., et al. Successful treatment of primary cardiac angiosarcoma with docetaxel and radiotherapy. Angiology. 2008;59(3):368–371. doi: 10.1177/0003319707308212. [DOI] [PubMed] [Google Scholar]
- 6.Deyrup A., Weiss S. Grading of soft tissue sarcomas: the challenge of providing precise information in an imprecise world. Histopathology. 2006;48(1):42–50. doi: 10.1111/j.1365-2559.2005.02288.x. [DOI] [PubMed] [Google Scholar]
- 7.Agha R.A., Franchi T., Sohrabi C., Mathew G., Kerwan A., Thoma A., Beamish A.J., Noureldin A., Rao A., Vasudevan B., Challacombe B. The SCARE 2020 guideline: updating consensus surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2020 Dec;1(84):226–230. doi: 10.1016/j.ijsu.2020.10.034. [DOI] [PubMed] [Google Scholar]
- 8.Shanmugam G. Primary cardiac sarcoma. Eur. J. Cardiothorac. Surg. 2006;29(6):925–932. doi: 10.1016/j.ejcts.2006.03.034. [DOI] [PubMed] [Google Scholar]
- 9.Shapira O.M., Korach A., Izhar U., et al. Radical multidisciplinary approach to primary cardiac sarcomas. Eur. J. Cardiothorac. Surg. 2013;44(2):330–336. doi: 10.1093/ejcts/ezt029. [DOI] [PubMed] [Google Scholar]
- 10.Auger D., Pressacco J., Marcotte F., Tremblay A., Dore A., Ducharme A. Cardiac masses: an integrative approach using echocardiography and other imaging modalities. Heart. 2011;97(13):1101–1109. doi: 10.1136/hrt.2010.196006. [DOI] [PubMed] [Google Scholar]
- 11.Alam M., Rosman H.S., Grullon C. Transesophageal echocardiography in evaluation of atrial masses. Angiology. 1995;46(2):123–128. doi: 10.1177/000331979504600205. [DOI] [PubMed] [Google Scholar]
- 12.Dell’Amore A., Asadi N., Caroli G., Dolci G., Bini A., Stella F. Recurrent primary cardiac osteosarcoma: a case report and literature review. Gen. Thorac. Cardiovasc. Surg. 2014 Mar;62(3):175–180. doi: 10.1007/s11748-013-0236-2. [DOI] [PubMed] [Google Scholar]
- 13.SLKSO S.H., SHPLB J.C., Moynihan T. Malignant primary cardiac tumors. Cancer. 2008;112:2440–2446. doi: 10.1002/cncr.23459. [DOI] [PubMed] [Google Scholar]
- 14.Raaf H.N., Raaf J.H. Wiley Online Library; 1994. Sarcomas related to the heart and vasculature; pp. 374–382. [DOI] [PubMed] [Google Scholar]
- 15.Hamidi M., Moody J.S., Weigel T.L., Kozak K.R. Primary cardiac sarcoma. Ann. Thorac. Surg. 2010;90(1):176–181. doi: 10.1016/j.athoracsur.2010.03.065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Centofanti P., Di Rosa E., Deorsola L., et al. Primary cardiac tumors: early and late results of surgical treatment in 91 patients. Ann. Thorac. Surg. 1999;68(4):1236–1241. doi: 10.1016/s0003-4975(99)00700-6. [DOI] [PubMed] [Google Scholar]
- 17.Pessotto R., Silvestre G., Luciani G.B., et al. Primary cardiac leiomyosarcoma: seven-year survival with combined surgical and adjuvant therapy. Int. J. Cardiol. 1997;60(1):91–94. doi: 10.1016/s0167-5273(97)02956-2. [DOI] [PubMed] [Google Scholar]