

Abstract
Rationale.
Although perceived obligations to meet the expectations of family, friends, and society can be detrimental to physical health, much research in this area has thus far been conducted exclusively on Western samples. Cross-cultural research importantly suggests that positive health can be dependent on whether one engages in modes of being that are sanctioned by one’s culture. Specifically, studies show that better health is predicted when people from cultures that value independence are able to exercise their personal autonomy and when people from cultures that value interdependence are able to maintain relational harmony (Kitayama, Karasawa, Curhan, Ryff, & Markus, 2010).
Objective.
Based on these lines of research, as the fulfillment of perceived obligations can facilitate relational harmony but infringe on personal autonomy, we posit that culture will moderate the impact of perceived obligations on health outcomes. To gain further insight, we additionally examined people’s goal disengagement tendency as an individual difference that may influence their likelihood of shunning perceived obligations in order to avoid associated stressors.
Method.
Drawing from the parallel biomarker projects of Midlife in the United States (MIDUS) and Midlife in Japan (MIDJA), we examined the interaction between perceived obligations and goal disengagement tendency on health among American and Japanese middle-aged adults. Health outcomes were indexed by biomarkers of inflammation (interleukin-6 and C-reactive protein levels) and cardiovascular risk (systolic blood pressure and total/high-density lipoprotein cholesterol).
Results.
We found that a higher tendency to disengage from stressful social obligations is associated with better health for Americans. In contrast, we found poorer health outcomes amongst Japanese participants who tend to disengage from their perceived obligations.
Conclusion.
Our results highlight the importance of examining how perceived obligations influence physical health from a cultural perspective. The current study supports the hypothesis that culturally distinct pathways underlie health outcomes.
Keywords: culture, perceived obligation, goal disengagement, inflammation and cardiovascular risk, personal control, stress, United States, Japan
Introduction
Do obligations stifle us, or do they give us a sense of purpose? Regardless of how we feel about obligations, they are ubiquitous in life—many people have been in relationships where they felt either morally or legally bound to meet the needs and expectation of others. Many people also feel obliged to contribute to society at large, such as the public community, the country, or even the world. As obligations are driven by factors external to the self, such as normative expectations or indebtedness, perceived obligations are often accompanied by feelings of constraint in terms of autonomy and personal control (Ayalon, 2016; Ross & Mirowsky, 2013). In light of the stressful tensions that may arise between individual autonomy and perceived obligations (Johnson & Acabchuk, 2018), it becomes imperative to examine the impact of perceived obligations on critical life outcomes, such as physical health. Indeed, several recent studies in the United States have consistently found perceived obligation to be associated with negative physical consequences (Kim, Knight, & Longmire, 2007; Losada et al., 2010; Sayegh, & Knight, 2010). For example, in a probability sample of 65 White and 95 African American dementia caregivers, Kim et al. (2007) reported that familial obligations are associated with poorer health as indexed by blood pressure, heart rate, and self-reported general health.
As much of the research on the health-related implications of obligations is based primarily on Western samples, the impact of perceived obligations on health in other cultural contexts remains unclear. In the present research, we adopt the perspective of cultural influence as normative influence. That is, rather than assuming that all members in a culture endorse the same collectivistic or individualistic values—an approach that has been questioned empirically (Oyserman, Coon, & Kemmelmeier, 2002)—we posit that a culture exerts its influence when its members comply with culturally normative values, or values they perceive to be accepted by most other members of the culture. To the extent that people perceive certain values as highly endorsed by their culture (i.e., normative values), those values can guide people’s thoughts and behaviors even when they do not necessarily endorse the values themselves. For instance, in one study, Hong Kong Chinese and American participants were first asked to indicate whether they approach their goals mostly by avoiding mistakes or by doing what is needed without being too concerned about making mistakes (Zou et al., 2009; Study 3). Next, they read a scenario with a disappointing outcome where the protagonist missed a flight. When asked to think of what the protagonist could have done differently to avoid the negative outcome, the Chinese participants tended to think about how the protagonist’s mistakes could have been avoided whereas the American participants thought about what else the protagonist could have done to make it for the flight. The researchers found no group difference in personal endorsement of goal attainment approaches. However, in line with the main findings, American participants perceived that most Americans would not be too concerned about making mistakes while Hong Kong Chinese participants perceived that most Hong Kong Chinese individuals would put more emphasis on avoiding mistakes. In other words, participants’ thoughts were guided by perceptions of what their cultural fellows would endorse. Indeed, not only do normative values guide personal behavior and thinking; they also influence what parents tend to inculcate in their children—parents were found to teach not only the values they endorsed themselves but also what they perceived to be the normative values in their society (Tam & Lee, 2010; Tam & Chan, 2015). In view of documented variations in people’s endorsements of their own culture’s tenets (e.g., Oyserman et al., 2002), we opted to qualify our cultural descriptors by referring to the preferred values of the cultural mandates in question. Thus, we will be referring to our target cultures as either “collectivism-preferred” or “individualism-preferred” throughout this paper.
Based on the findings of earlier-mentioned studies on perceived obligations and physiological outcomes (e.g., Kim et al., 2007; Losada et al., 2010) as well as the studies on cultural normative influence, it seems reasonable to assume that people from collectivism-preferred cultures (e.g., Japan) that value relational harmony would experience worse health problems due to the greater burdens they face while fulfilling social responsibilities relative to people from individualism-preferred cultures (e.g., the United States) that prize autonomy and personal control more (Markus & Kitayama, 2001). However, Kitayama, Karasawa, Curhan, Ryff, and Markus (2010) suggest that collectivism-preferred cultures may, counterintuitively, have better health when faced with more perceived obligations, not less. Their study on “modes of being” revealed that people can achieve positive health outcomes by acting in accordance with their cultural mandates. In general, individualism-preferred cultures tend to sanction an independence-driven mode of being, which is a motivational orientation to pursue personal control and autonomy, whereas collectivism-preferred cultures tend to sanction an interdependence-driven mode of being, which constitutes a motivational orientation to maintain relational harmony and show concern for others. As culturally distinct pathways based on either independence or interdependence may underlie people’s positive health outcomes, it is therefore possible that the health-related impact of constrained autonomy and personal control will vary as a function of differences in cultural modes of being. Indeed, Kitayama and colleagues found that being able to exert personal control was the strongest predictor of positive health outcomes (e.g., subjective health, number of chronic health problems, frequency of somatic symptoms, sensitivity to unpleasant sensations) in the United States but not in Japan. In contrast, maintaining relational harmony was the strongest predictor of positive health outcomes in Japan but not in the United States.
These and other recent studies demonstrating culturally distinct pathways to health (e.g., Kitayama et al., 2010; Park et al., 2013) highlight the importance of accounting for culturally valued modes of being when examining the impact of perceived obligations on health (Hardin, Robitschek, Flores, Navarro, & Ashton, 2014). Kitayama et al.’s (2010) study suggests that culture will moderate the link between perceived obligation and health such that for individualism-preferred cultures, perceived obligation will have a negative health impact as it conflicts with cultural mandates of independence and undermines personal autonomy (e.g., Sayegh, & Knight, 2010), whereas for collectivism-preferred cultures, perceived obligation will have a positive health impact as it aligns with cultural mandates of interdependence and facilitates relational harmony (Kim, Sherman, Ko, & Taylor, 2006; Li, Zou, Liu, & Zou, 2014; Xu, 2019).
In addition to culture, individual differences in goal disengagement tendency (GDT) may also impose a moderating effect on perceived obligation and health (Kannan, Brown, Kunitz, & Chapman, 2019; Wrosch, Scheier, Miller, Schulz, & Carver, 2003). As the fulfillment of obligations can be a stressful goal to accomplish, some individuals may have more will to persist while others may abandon the goal to relieve themselves of associated stressors. Research on coping styles and control strategies has indeed established that individuals vary in GDT such that, when faced with obligations and commitment is stressful or difficult, high GDT individuals are more likely than low GDT individuals to disengage and avoid fulfillling their obligations (Wrosch et al., 2003). By disengaging from one’s perceived obligations, a person can retain his or her autonomy and personal control but harm his or her relational harmony with the beneficiary of the obligation. In contrast, individuals with low GDT are especially likely to persist in fulfillling difficult obligations, which may constrain their autonomy and personal control but strengthen their relational harmony. Thus, a consideration of individual differences in GDT will add another important dimension to our understanding of how perceived obligations affect health outcomes alongside the influence of culture.
Based on the foregoing analysis, the current study aimed to investigate the links between perceived obligation and physical health risks as moderated by culture and GDT. The parallel biomarker projects of Midlife in the United States (MIDUS) and Midlife in Japan (MIDJA) offer an immensely valuable opportunity to examine these links with large samples and objective measures of biological health risk in the domains of perceived familial and public community obligations among middle-aged Americans (representing the individualism-preferred culture; n = 1,054) and Japanese (representing the collectivism-preferred culture; n = 382). The cross-cultural comparison is critical since research has shown that Americans tend to perceive individualism to be widely shared in the United States but not collectivism (Zou et al., 2009), while most Japanese expect other Japanese to hold stronger collectivistic than individualistic values (Hashimoto & Yamagishi, 2015). Participants from both countries completed identical questionnaires. The Japanese version of the questionnaire was translated from and back-translated to English and adjusted by native speakers to ensure equivalent meaning. Participants also stayed overnight in a clinical research center in their respective countries to provide their biomarker data. Each type of biomarker was then shipped on dry ice to the same testing laboratory for analysis.
In accordance with Kitayama et al.’s distinct pathways to positive health hypothesis, we predict that culture and GDT would moderate the link between perceived obligations and biological health risk. Specifically, if acting in line with an independence mode of being (i.e., personal control and autonomy) is associated with positive health outcomes among individuals from an individualism-preferred culture, then perceived obligation would be positively associated with biological health risk (i.e., greater inflammation and cardiovascular risk) among Americans with low GDT. In contrast, if acting in line with an interdependence mode of being (i.e., relational harmony) is associated with positive health outcomes among individuals from a collectivism-preferred culture, then perceived obligation would be negatively associated with biological health risk among Japanese with low GDT. Conversely, we hypothesize that these predicted associations would be reversed for participants with high GDT when faced with stressors. In this case, among individuals with high GDT, perceived obligation would be negatively associated with biological health risk in Americans but positively associated with biological health risk among the Japanese.
Method
Participants
The MIDUS and MIDJA biomarker projects consisted of 1,054 American and 382 Japanese participants2, which is a subset of a randomly selected sample of 4,244 and 1,027 adults in the United States and Tokyo metropolitan area, respectively. One participant from MIDUS was excluded due to missing data in almost all measurements. The American participants in the MIDUS biomarker project were invited to an overnight hospital stay at one of three clinical research centers in the United States (University of California, Los Angeles; Georgetown University; and University of Wisconsin-Madison) for a biological assessment that included the collection of a fasting blood sample before breakfast on the second day of the participant’s hospital stay (Love, Seeman, Weinstein, & Ryff, 2010). The location of the assigned center was based on the region (West Coast, Midwest, East Coast, respectively) in which the participants lived. Likewise, the Japanese participants in the MIDJA biomarker project were invited to visit a medical clinic (Yuki Medical Clinic) near the University of Tokyo to participate in similar biological assessments (Coe et al., 2011).
Eligibility criteria for the MIDUS and MIDJA biomarker project included completing the initial MIDUS and MIDJA survey and interest in further participation in the biomarker project. Participants who eventually participated in the MIDUS and MIDJA biomarker project had similar characteristics to those who only participated in the initial survey but not the biomarker project. For MIDJA, as demonstrated by Boylan, Tsenkova, Miyamoto, and Ryff (2017), there was no significant difference between Japanese participants who participated in the biomarker project and those who did not in terms of demographic characteristics (e.g., age, educational attainment, family size, marital status, economic status) and health characteristics (e.g., number of chronic diseases, number of prescription medications taken, number of physician visits in the prior year), except that the Japanese who participated in the biomarker project had a higher proportion of females and were less likely to smoke. Similarly, for MIDUS, as demonstrated by Love et al. (2010), there was no significant difference between American participants who participated in the biomarker project and those who did not in terms of demographic characteristics (e.g., age, sex, race, marital status, economic status) and health characteristics (e.g., number of chronic diseases, number of physician visits in the prior year), except that Americans who participated in the biomarker project were more educated and less likely to smoke. Table 1 presents the descriptive statistics for demographics and key variables for each cultural group. The data collection was approved by the Health Sciences IRBs at the University of Wisconsin-Madison, University of California, Los Angeles, and Georgetown University for MIDUS biomarker project, as well as the University of Tokyo for MIDJA biomarker project. Data and materials from the MIDUS and MIDJA are freely available from the Inter-university Consortium for Political and Social Research (http://www.icpsr.umich.edu).
Table 1.
Descriptive Statistics for Demographic and Key Variables in American (MIDUS) and Japanese (MIDJA) participants
| Americans (MIDUS) |
Japanese (MIDJA) |
|||
|---|---|---|---|---|
| n | M (SD) | n | M (SD) | |
| Demographic | ||||
| Mean age (years) | 1,053 | 58.05 (11.63)a | 382 | 55.47 (14.04)b |
| Gender (% of female) | 1,053 | 55%a | 382 | 56%a |
| Education1 | 1,050 | 4.96 (1.61)a | 378 | 4.42 (1.64)b |
| Occupational status2 | 1,053 | 1.79 (0.93)a | 379 | 1.74 (0.79) |
| Subjective social status3 | 1,041 | 6.59 (1.72)a | 374 | 6.24 (2.04)b |
| Health Status | ||||
| Number of chronic diseases | 1,053 | 2.30 (2.34)a | 377 | 2.31 (2.02)a |
| Waist-to-hip ratio | 1,052 | 0.89 (0.10)a | 382 | 0.83 (0.08)b |
| Health behaviors | ||||
| Non-smoker (%) | 1,053 | 56.89%a | 356 | 51.97%b |
| Former smoker (%) | 1,053 | 32.48%a | 356 | 25.00%b |
| Current smoker (%) | 1,053 | 10.64%a | 356 | 23.03%b |
| Alcohol consumption (drinks per week) | 1,051 | 3.14 (5.53)a | 379 | 7.24 (11.75)b |
| Emotionality | ||||
| Anger expression4 | 1,052 | 12.79 (3.13)a | 381 | 12.25 (3.63)b |
| Experience of negative emotions5 | 1,049 | 1.49 (0.55)a | 381 | 1.70 (0.65)b |
| Personality6 | ||||
| Neuroticism | 1,049 | 2.03 (0.63)a | 381 | 2.13 (0.58)b |
| Openness to experience | 1,044 | 2.96 (0.52)a | 381 | 2.46 (0.66)b |
| Conscientious | 1,049 | 3.48 (0.43)a | 381 | 2.73 (0.54)b |
| Extraversion | 1,049 | 3.13 (0.57)a | 381 | 2.46 (0.66)b |
| Agreeableness | 1,049 | 3.44 (0.50)a | 381 | 2.69 (0.63)b |
| Perceived obligations7 | ||||
| Family and close friends | 1,051 | 5.04 (1.07)a | 370 | 5.02 (0.93)a |
| Public community | 1,051 | 5.43 (1.15)a | 370 | 5.62 (0.90)b |
| Goal disengagement tendency8 | 1,053 | 2.59 (2.99)a | 377 | 2.37 (0.52)b |
| Biological health risk factor score | ||||
| Interleukin-6 (pg/ml) | 1,044 | 2.79 (2.79)a | 382 | 1.64 (2.11)b |
| C-reactive protein (ug/ml) | 1,040 | 2.70 (4.28)a | 382 | 0.76 (2.00)b |
| Systolic blood pressure (mm Hg) | 1,053 | 131.01 (17.87)a | 382 | 121.64 (19.95) b |
| Total/HDL cholesterol | 1,043 | 3.75 (1.43)a | 382 | 3.15 (1.15)b |
Note. SDs are shown in parentheses. Means in the same row with different superscript letters differ significantly (p < .05)
Education attainment was rated on a scale of 1 (8th grade, junior high school) to 7 (attended or graduated from graduate school)
Occupational status was rated on a three-point Likert scale (1 = manual, blue-collar, or service, 2 = non-manual, white-collar, or clerical, 3 = managerial or professional)
Subjective social status was measured with a ladder scale (1st rung = lowest, 10th rung = highest; Adler, Epel, Castellazza, & Ickovics, 2000)
Anger expression was computed by summing scores from 8 items (Spielberger, 1996) rated on a four-point Likert scale (1 = almost never, 4 = almost always), with higher scores indicating greater anger expression.
Negative affect was computed by averaging scores from 6 items (Mroczek & Kolarz, 1998) rated on a five-point Likert scale (1 = none of the time, 5 = all of the time), with higher scores indicating greater negative affect.
Each personality score was computed by averaging the respective personality items (Rossi, 2001), which were rated on a four-point Likert scale (1 = not at all, 4 = a lot) with higher scores indicating a higher amount of that particular personality dimension (e.g., greater neuroticism).
Perceived obligation in each domain was computed by averaging scores from 3 items (Rossi, 2001) rated on a seven-point Likert scale (1 = strongly disagree, 7 = strongly agree), with higher scores indicating greater perceived obligations.
Goal disengagement tendency was computed by averaging scores from 6 items (Wrosch, Heckhausen, Lachman, 2000) rated on a four-point Likert scale (1 = not at all, 4 = a lot), with higher scores indicating greater goal disengagement tendency.
Measures
Biological health risk.
Based on Kitayama et al. (2015), biological health risk was conceptualized as inflammation and cardiovascular risk indexed by interleukin-6, C-reactive protein (CRP) levels, systolic blood pressure, and total/high-density lipoprotein (HDL) cholesterol. Blood samples were collected between 0900 and 1145 for over 95 % of the Japanese sample and between 0500 and 0700 for the entire American sample. For the American sample, the tubes were filled in the following order: (1) three 10-millilitre serum separator tubes, (2) two 4-millilitre EDTA tubes, and (3) one 4-millilitre or 2.7-millilitre citrated tube. For the Japanese sample, the tubes were filled in the following order: (1) three 8.5-millilitre serum separator tubes, (2) two 1.8-millilitre citrated tubes, (3) one 2-millilitre FNa tube, and (4) one 2-millilitre EDTA2k tube. Frozen samples were then stored in a −60°C to −80°C freezer before being shipped on dry ice to the MIDUS Biocore Lab at the University of Wisconsin-Madison. Samples were subsequently stored in a −65°C freezer until assayed. Interleukin-6, CRP, and cholesterol in both MIDUS and MIDJA were assayed in the MIDUS Biocore Laboratory, the Laboratory for Clinical Biochemistry Research (University of Vermont, Burlington, VT), and the Meriter Labs (Madison, WI) respectively.
Interleukin-6 was measured using the Quantikine® High-sensitivity enzyme-linked immunosorbent assay (ELISA) kit #HS600B (R&D Systems, Minneapolis, MN) with an assay range of 0.156 to 10 pg/mL. All samples were tested in duplicate. The laboratory intra-assay and inter-assay coefficients of variance for interleukin-6 were 3.2% and 12.3%, respectively. The reference range spanned from 0.45 to 9.96 pg/mL. CRP was measured by BNII nephelometer (N Antiserum to Human Fibrinogen; Dade Behring Inc., Deerfield, IL) using a particle-enhanced immunonepholometric assay ranging from 0.175-1100 ug/mL. For CRP, the laboratory intra-assay coefficients of variance ranged from 2.3% to 4.4% and the laboratory inter-assay coefficients of variance ranged from 2.1% to 5.7%. The reference range was < 3 ug/mL.
Blood pressure was assessed during a large-scale physical examination after participants sat quietly and rested for 5 minutes. While participants were seated, three consecutive blood pressure readings were taken by nurses using a Finometer beat-to-beat blood pressure monitor (Finapres Medical Systems BV, BT Arnhem, The Netherlands) with a 30-second interval between each assessment. Systolic blood pressure was computed by taking the average of the second and third systolic blood pressure measurements while in the sitting position. The intercorrelations between blood pressure readings for the sample within each culture ranged from .84 to .97, suggesting that these readings were reliable. Similar procedures were used for both American and Japanese samples. Cholesterol was measured using the Cobas Integra Analyser (Roche Diagnostics, Indianapolis, IN) with assays ranging from 0-800 mg/dL for total cholesterol and 0-155 mg/dL for HDL cholesterol. For total cholesterol, the laboratory intra-assay coefficients of variance ranged from 0.51% to 0.81% and the laboratory inter-assay coefficients of variance was 2.65%. The reference range was < 200 mg/dL. For HDL cholesterol, the laboratory intra-assay coefficients of variance ranged from 1.1% to 1.4% and the laboratory inter-assay coefficients of variance was 6.52%. The reference range was > 40 mg/dL.
All indices were winsorized to 3 SDs within each culture to reduce the influence of extreme outliers and were log-transformed to reduce skewness. From a total of 1,053 participants in MIDUS, we winsorized 21 data points for interleukin-6, 22 data points for CRP, 6 data points for systolic blood pressure, and 13 data points for total/HDL cholesterol. From a total of 382 Japanese participants in MIDJA, we winsorized 8 data points for interleukin-6, 8 data points for CRP, 2 data points for systolic blood pressure, and 7 data points for total/HDL cholesterol.
As all four indices (i.e., interleukin-6, CRP, systolic blood pressure, and total/HDL cholesterol) were positively correlated within each culture, we followed the approach adopted by Kitayama et al. (2015) and conducted principal component analyses to examine whether the indices can be analyzed as a single factor. The principal component analyses showed that the four indices highly loaded on a single factor (see Supplementary Materials for factor loadings and zero-order correlations). Confirmatory factor analysis also showed that the single-factor model had an acceptable fit, χ 2(1, n=1,419)= 27.70, p<.001; CFI=.970, TLI=.911, RMSEA=.095 [90% CI=.066, .128]. Furthermore, the single-factor model had a significantly better fit than an alternative model assuming four distinct variables (p<.001). Hence, we used the factor score from the single-factor model as our indicator of biological health risk, with higher values indicating greater inflammation and cardiovascular risk.
Perceived obligation.
Perceived obligation was assessed in two social domains, 1) family and close friends and 2) public community, using a shortened version of Rossi’s (2001) social obligation scale. Participants rated their agreement with a series of statements about their sense of obligation towards others on a seven-point Likert scale (1=strongly disagree, 7=strongly agree). There were three items in the domain of family and close friends (e.g., “I feel obligated to drop plans when members of my family seem very troubled”; αMIDUS=.65 and αMIDJA=.46) and three items in the domain of public community (e.g., “I feel obligated to volunteer time or money to social causes I support”; αMIDUS=.72 and αMIDJA =.68). It is important to note that the original Rossi’s (2001) Social Obligation Scale consisted of 8 items for perceived obligation in the domain of family and close friends and 4 items for perceived obligation in the domain of public community. However, MIDUS and MIDJA only administered the shortened version of the Social Obligation Scale, which consisted of 4 items for perceived obligation in the domain of family and close friends and 3 items for the domain of public community. In the domain of public community, we used all 3 items that were administered in MIDUS and MIDJA. In the domain of family and close friends, we used all the items except for “I feel obligated to take my divorced or unemployed adult child back into my home” since the scenario was not relevant or applicable to most of our participants.
Goal disengagement tendency.
GDT was measured with Wrosch, Heckhausen, and Lachman’s (2000) six-item goal disengagement scale. Participants rated how much they tended to disengage from their goals (e.g., “I often remind myself that I can’t do everything”; when something I wanted did not work out, I try not to think about it too much”) on a four-point Likert scale (1=not at all, 4=a lot; αMIDUS=.73 and αMIDJA =.69).
Data Analysis
The main goal of the current study is to examine the moderating effects of culture and GDT on the relation between perceived obligation (across the domains of family and close friends as well as community) and objective biological health risks. To test our hypotheses, we conducted three-way interaction analyses in each domain of perceived obligation using the SPSS PROCESS macro (model 3; Hayes, 2012) to determine the significance of the interaction between and among an independent variable (i.e., perceived obligation) and two moderators (i.e., culture and GDT). The PROCESS macro uses ordinary least squares regression to estimate the coefficients of each predictor and their interactions. Perceived obligation was included as the independent variable, culture was included as the first moderator, and GDT was included as the second moderator. Continuous variables that were included with interaction terms were mean-centered. A significant perceived obligation × culture × GDT interaction would support the hypothesized three-way interaction model. Simple slopes were computed, followed by slope difference tests to examine the two-way interactions of perceived obligation × culture at each level of GDT.
We conducted three separate analyses, each with an additional set of covariates, to ensure the robustness of the hypothesized three-way interaction. In the first model, as per previous cross-cultural studies on biological health risk (e.g., Kitayama et al. 2015), we controlled for demographics, health status, and health behaviors that have been linked with inflammation and cardiovascular risk (O’Connor et al., 2009). For demographics, the covariates consisted of age, gender, education, occupational status, and subjective social status as measured by the MacArthur Scales of Subjective Social Status (Adler, Epel, Castellazzo & Ickovics, 2000). The scale uses an image of a ladder and participants were instructed to rate their social status by choosing the rung on the ladder (1st rung=lowest, 10th rung=highest) that corresponds most to their self-perceived social standing in their community. We standardized education attainment across cultures with a 7-point scale (1=8th grade, junior high school, 2=some high school, no diploma, 3=graduated from high school, 4=attended colleage, degree, 5=graduated from two years college or vocational school, 6= graduated from four or five years college (bachelor’s degree), 7=attended or graduated from graduate school) and occupational status with a 3-point scale (1=manual, blue-collar, or service, 2=non-manual, white-collar, or clerical, 3=managerial or professional; Kitayama et al., 2015). For health status, the number of chronic diseases (e.g., diabetes) experienced in the past 12 months and obesity as indexed by waist-to-hip ratio were included as covariates. For health behaviors, we controlled for behaviors that have been previously documented to be associated with inflammation and cardiovascular risk, which included smoking experience and alcohol consumption.
In the second model, we additionally controlled for emotionality-related variables that have previously been shown to influence biological health risk (Curhan et al., 2014; Kitayama et al., 2015; Park et al., 2013), which consisted of anger expression (Spielberger, 1996) and negative affect (Mroczek & Kolarz, 1998). We also included the interaction terms of these emotionality variables with culture as past studies have demonstrated that culture moderates the influence of anger expression and negative affect on biological health risk (Curhan et al., 2014; Kitayama et al., 2015). Therefore, Model 2 allowed us to test whether the hypothesized three-way interaction is unique or simply due to specific aspects of emotionality that have been found to be moderated by culture in previous studies.
In the third model, we further included the Big Five personality traits as covariates (extraversion, conscientiousness, agreeableness, neuroticism, and openness to experience; Rossi, 2001) to ensure that the influences of perceived obligation on health are not confounded by the influence of personality traits (Friedman, Kern, & Reynolds, 2010; Marshall, Wortman, Vickers, Kusulas, & Hervig, 1994).
Following established statistical recommendations (Nguyen, Strazdins, Nicholson, & Cooklin, 2018; Sidi & Harel, 2018), we conducted missing data imputation to minimize bias. In our main analyses, missing data (less than 1% of total values and on any given variable) were imputed using an expectation-maximization algorithm (Dempster, Laird, & Rubin, 1977), with missing at random as our assumption. We also reanalyzed our data with multiple imputations using a Markov chain Monte Carlo algorithm with a fully conditional specification procedure to create five imputed datasets (Rubin, 1987). As recommended by Von Hippel (2007), we employed the multiple-imputation-then-deletion (MID) procedure in which missing criterion variables were excluded from the analysis subsequent to the imputation. Results from both imputation techniques were consistent (see Supplementary Materials).
Results
Family and Close Friends
The three-way interaction analyses in the domain of family and close friends for all three models are summarized in Table 2. As predicted, there are significant two-way interactions of perceived obligation × culture on biological health risk across all three models (ps<.01). More importantly, the perceived obligation × culture × GDT interaction is significant across all three models (ps<.01), suggesting a robust three-way interaction even when controlling for demographic factors, health status, health behaviors, emotionality-related variables, and personality traits.
Table 2.
Three-way Interactions of Perceived Obligation in the Domain of Family and Close Friends, Culture, and GDT on Biological Health Risk in Three Separate Models
| Model 1 |
Model 2 |
Model 3 |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE | t | B | SE | t | B | SE | t | |
| Main effect | |||||||||
| Perceived obligation | −0.02 | .02 | −0.99 | −0.02 | .02 | −1.05 | −0.04 | .02 | −1.61 |
| Culture | −0.89 | .05 | −17.23*** | −0.88 | .05 | −16.90*** | −0.87 | .07 | −12.91*** |
| GDT | −0.07 | .04 | −1.79† | −0.07 | .04 | −0.55 | −0.03 | .05 | −0.58 |
| Two-way interaction | |||||||||
| Perceived obligation × Culture | 0.19 | .05 | 3.81*** | 0.18 | .05 | 3.58*** | 0.18 | .05 | 3.65*** |
| Perceived obligation × GDT | −0.06 | .04 | −1.42 | −0.06 | .04 | −1.51 | −0.12 | .04 | −2.68** |
| Culture × GDT | −0.18 | .09 | −1.96† | −0.16 | .09 | −1.82† | −0.27 | .09 | −2.34† |
| Three-way interaction | |||||||||
| Perceived obligation × culture × GDT | 0.24 | .09 | 2.50* | 0.24 | .09 | 2.49* | 0.22 | .09 | 2.35* |
| Control | |||||||||
| Age | 0.02 | .00 | 8.89*** | 0.02 | .00 | 8.60*** | 0.02 | .00 | 8.51*** |
| Gender | 0.18 | .06 | 3.07** | 0.18 | .06 | 3.17** | 0.14 | .06 | 2.39* |
| Education | −0.06 | .01 | −4.21*** | −0.06 | .01 | −4.17*** | −0.05 | .01 | −3.81*** |
| Occupational status | 0.07 | .03 | 2.65* | 0.06 | .03 | 2.60** | 0.07 | .03 | 2.87** |
| Subjective social status | −0.02 | .01 | −1.51 | −0.02 | .01 | −1.36 | −0.02 | .01 | −1.49 |
| Number of chronic diseases | 0.03 | .01 | 3.62** | 0.03 | .01 | 3.30** | 0.03 | .01 | 3.24** |
| Waist-to-hip ratio | 3.69 | .29 | 12.62*** | 3.68 | .29 | 12.63*** | 3.55 | .29 | 12.07*** |
| Former smoker | −0.06 | .05 | −1.19 | −0.06 | .05 | −1.36 | −0.06 | .05 | −1.22 |
| Current smoker | 0.17 | .07 | 2.65* | 0.17 | .07 | 2.64** | 0.17 | .07 | 2.63* |
| Alcohol | −0.00 | .00 | −0.34 | −0.00 | .00 | −0.14 | −0.00 | .00 | −0.07 |
| Anger expression | 0.02 | 2.68** | 0.03 | .01 | 3.17** | ||||
| Experience of negative emotions | 0.00 | .05 | 0.01 | 0.03 | .06 | 0.58 | |||
| Anger expression × culture | −0.04 | .01 | −2.95** | −0.04 | .01 | −2.85** | |||
| Experience of negative emotions × culture | −0.04 | .08 | −0.54 | −0.05 | .08 | −0.58 | |||
| Agreeableness | 0.16 | .05 | 3.25*** | ||||||
| Openness to experience | −0.06 | .05 | −1.34 | ||||||
| Neuroticism | −0.06 | .04 | −1.46 | ||||||
| Extraversion | −0.03 | .05 | −0.68 | ||||||
| Conscientiousness | −.04 | .05 | −0.83 | ||||||
Note: Culture was dummy coded with the United States as reference. Gender was coded with male as reference. Former and current smoker were coded with non-smoker as reference.
p<.10,
p<.05,
p<.01,
p<.001.
GDT = goal disengagement tendency.
As the three-way interactions are all significant, we conducted simple slopes analyses for the association between perceived obligation and biological health risk on each culture and level of GDT in the full model. As shown in Figure 1, when GDT is high, the association between perceived obligation and biological health risk is significantly negative among Americans, b = −0.10, t = −3.30, p < .001, but significantly positive among the Japanese, b= 0.20, t=2.82, p=.005. Moreover, the slopes differential test confirmed that the interaction between perceived obligation and culture is significant when GDT is high, b= 0.30, F=15.08, p<.001. The link between perceived obligation and biological health risk became weaker when GDT is moderate. Here, the association between perceived obligation and biological health risk is not significant among Americans, b=−0.04, t=−1.61, p= .108, but is significantly positive among the Japanese, b=0.15, t=3.24, p=.001. The slopes differential test confirmed that the interaction between perceived obligation and culture is significant when GDT is moderate, b=0.18, t=3.65, p< .001. Lastly, when GDT is low, perceived obligation is unrelated with biological health risk in both Americans, b=0.02, t=.67, p=.504, and the Japanese, b=.09, t=1.78, p=.075. Consistently, the slopes differential test confirmed that the interaction between perceived obligation and culture is not significant when GDT is low, b=0.07, t=1.25, p=.263. The significance patterns did not change when we further conducted simple slopes analyses on Models 1 and 2.
Figure 1.
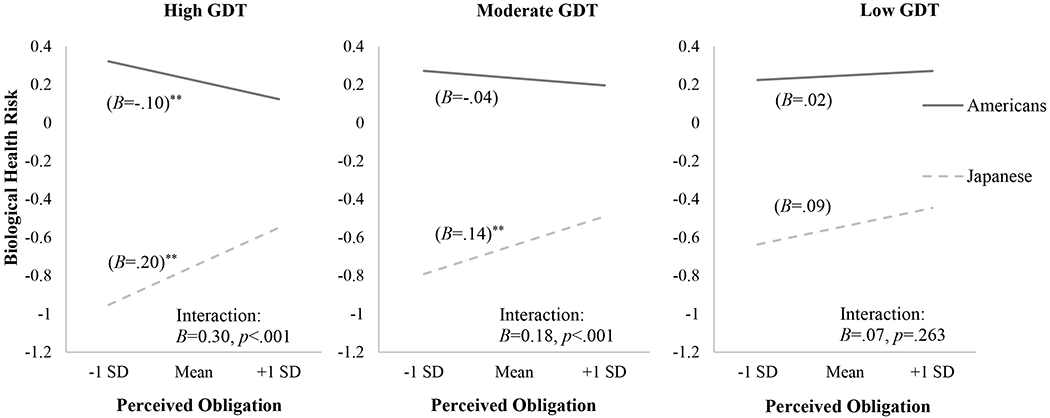
Simple slopes (i.e., unstandardized coefficients) of perceived obligation in the domain of family and close friends predicting biological health risk at 1 SD above the mean and 1 SD below the mean across culture when GDT is high, moderate, and low. Higher biological health risk values indicate greater inflammation and cardiovascular risk, * p<.05, ** p<.01. GDT = goal disengagement tendency.
Public Community
The three-way interaction analyses in the domain of public community for all three models are summarized in Table 3. Consistent with the results for the domain of family and close friends, there are significant two-way interactions of perceived obligation × culture on biological health risk across all three models (ps<.01). However, the three-way interaction of perceived obligation × culture × GDT is not significant across all three models for public community.
Table 3.
Three-way Interactions of Perceived Obligation in the Domain of Public Community, Culture, and GDT on Biological Health Risk in Three Separate Models
| Model 1 |
Model 2 |
Model 3 |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE | t | B | SE | t | B | SE | t | |
| Main effect | |||||||||
| Perceived obligation | −0.05 | .02 | −2.18* | −0.05 | .02 | −2.08* | −0.05 | .02 | −2.19* |
| Culture | −0.89 | .05 | −16.88*** | −0.89 | .05 | −16.56*** | −0.87 | .07 | −12.52*** |
| GDT | −0.03 | .05 | −0.69 | −0.03 | .05 | −0.64 | −0.03 | .05 | −0.73 |
| Two-way interaction | |||||||||
| Perceived obligation × Culture | 0.13 | .05 | 2.48* | 0.12 | .05 | 2.39* | 0.12 | .05 | 2.27* |
| Perceived obligation × GDT | −0.06 | .04 | −1.38 | −0.05 | .04 | −1.31 | −0.05 | .04 | −1.26 |
| Culture × GDT | −0.17 | .09 | −1.89† | −0.16 | .09 | −1.77† | −0.16 | .09 | −1.80† |
| Three-way interaction | |||||||||
| Perceived obligation × culture × GDT | 0.12 | .09 | 1.40 | 0.13 | .09 | 1.45 | 0.13 | .09 | 1.43 |
| Control | |||||||||
| Age | 0.02 | .00 | 9.13*** | 0.02 | .00 | 8.75*** | 0.02 | .00 | 8.62*** |
| Gender | 0.17 | .06 | 3.02** | 0.18 | .06 | 3.13** | 0.14 | .06 | 2.41* |
| Education | −0.05 | .01 | −3.74*** | −0.05 | .01 | −3.71*** | −0.05 | .01 | −3.39*** |
| Occupational status | 0.06 | .03 | 2.50* | 0.06 | .03 | 2.45* | 0.07 | .03 | 2.69** |
| Subjective social status | −0.01 | .01 | −1.10 | −0.01 | .01 | −1.05 | −0.02 | .01 | −1.19 |
| Number of chronic diseases | 0.03 | .01 | 3.62** | 0.03 | .01 | 3.41** | 0.03 | .01 | 3.36** |
| Waist-to-hip ratio | 3.69 | .29 | 12.59*** | 3.68 | .29 | 12.60*** | 3.58 | .30 | 12.11*** |
| Former smoker | −0.06 | .05 | −1.17 | −0.06 | .05 | −1.31 | −0.06 | .05 | −1.18 |
| Current smoker | 0.18 | .07 | 2.77** | 0.18 | .07 | 2.80** | 0.18 | .07 | 2.78** |
| Alcohol | −0.00 | .00 | −0.39 | −0.00 | .00 | −0.18 | −0.00 | .00 | −0.06 |
| Anger expression | 0.02 | .01 | 2.63** | 0.03 | .01 | 3.20** | |||
| Experience of negative emotions | −0.01 | .05 | −0.29 | 0.02 | .06 | 0.37 | |||
| Anger expression × culture | −0.04 | .01 | −3.10** | −0.04 | .01 | −2.98** | |||
| Experience of negative emotions × culture | −0.03 | .08 | −0.36 | −0.04 | .08 | −0.45 | |||
| Agreeableness | 0.15 | .05 | 3.16*** | ||||||
| Openness to experience | −0.06 | .05 | −1.28 | ||||||
| Neuroticism | −0.07 | .04 | −1.62 | ||||||
| Extraversion | −0.04 | .05 | −0.82 | ||||||
| Conscientiousness | −0.03 | .05 | −0.52 | ||||||
Note: Culture was dummy coded with the United States as reference. Gender was coded with male as reference. Former and current smoker were coded with non-smoker as reference.
p<.10,
p<.05,
p<.01,
p<.001.
GDT = goal disengagement tendency.
Nevertheless, to maintain consistency with the analysis for the domain of family and close friends, we also conducted simple slopes analyses for the link between perceived obligation and biological health risk in the domain of community on each culture and level of GDT in the full model. As shown in Figure 2, when GDT is high, the correlation between perceived obligation and biological health risk is significantly negative in Americans, b=−0.07, t=−2.62, p=.009, but not significant among the Japanese, b= 0.11, t=1.51, p=.130. The slopes differential test confirmed that the interaction between perceived obligation and culture is significant when GDT is high, b= 0.18, F=5.73, p=.017. Similarly, when GDT is moderate, the association between perceived obligation and biological health risk is significantly negative in Americans, b=−0.05, t=−2.19, p=.023, but not significant among the Japanese, b=.07, t=1.44, p=.149. The slopes differential test showed that the interaction between perceived obligation and culture is still significant when GDT is moderate, b= 0.11, F=5.15, p=.023. Lastly, when GDT is low, the association between perceived obligation and biological health risk became insignificant for both Americans, b=−0.02, t=.70, p=.485, and the Japanese, b=0.03, t=.55, p=.585. Consistently, the slopes differential test confirmed that the interaction between perceived obligation and culture is not significant when GDT is low, b=0.05, F= 0.71, p=.401. These significance patterns did not change when we further conducted simple slopes analyses on Models 1 and 2.
Figure 2.

Simple slopes (i.e., unstandardized coefficients) of perceived obligation in the domain of public community predicting biological health risk at 1 SD above the mean and 1 SD below the mean across culture when GDT is high, moderate, and low. Higher biological health risk values indicate greater inflammation and cardiovascular risk, † p<.10, * p<.05, ** p<.01. GDT = goal disengagement tendency.
Discussion
Our study is the first to provide empirical evidence showing that the links between biological health risk and perceived obligation across the domains of family, close friends, and community depend crucially on culture, or more specifically whether one acts in accordance with one’s cultural mandates. Thus, obligations do not straightforwardly result in poorer health, as some previous studies might suggest, once cultural contexts are taken into account. We also found that cultural variations in the associations between perceived obligation and biological health risks are further moderated by GDT. Specifically, for people with high GDT, higher perceived obligation is linked with better heath as indexed by lower inflammation (interleukin-6, CRP levels) and cardiovascular risk (systolic blood pressure and total/HDL cholesterol) in Americans but poorer health in the Japanese. Furthermore, this association was weakened at moderate levels of GDT and became non-significant at low levels of GDT (see Figure 1).
The significant three-way interaction in the domain of family and close friends provide support for the hypothesis that positive health occurs through culturally distinct pathways (Kitayama et al., 2010; Park et al., 2013). As individualism-preferred cultures especially value personal control and sense of autonomy while collectivism-preferred cultures especially value relational harmony, we hypothesized that positive health outcomes can be achieved partly through aligning oneself with the dominant cultural mandates of one’s cultural group. We found that a higher tendency to disengage from perceived obligations in the domain of family and close friends is associated with better health outcomes for Americans. This suggests that although relational harmony may suffer when people from individualism-preferred cultures try to avoid the stifling constraints of perceived obligations, they get to engage in their culturally sanctioned independence mode of being, and the freedom to uninhibitedly exercise autonomy and personal control may lead to better health outcomes for them. On the flipside, the poorer health outcomes amongst Japanese participants who tend to disengage from their perceived obligations in the domain of family and close friends suggest that people from collectivism-preferred cultures who fail to abide by their cultural mandates of interdependence, such as putting in the effort to contribute to relational harmony or helping others, may suffer from stressors (e.g., being seen as selfish) despite maintaining their own personal autonomy. These findings lend support to the importance of congruence between prevailing cultural modes of being and psychological propensities on physical health.
However, our hypothesis that the link between perceived obligation and biological health risk would be positive for Americans and negative for the Japanese among those low in GDT was not supported. Specifically, among participants with low GDT, there were no associations between perceived obligation and biological health risk across both cultures. This indicates that the tendency to disengage from perceived obligations has a stronger cross-cultural differential influence on physical health than the tendency to engage in perceived obligations. The null associations between perceived obligation and biological health risks may be attributable to a negativity bias in obligation fulfillment, whereby asymmetries exist between the consequences of fulfillling and not fulfillling the same obligations (Conway, Guest, & Trenberth, 2011; De Jong, Clinton, Rigotti, & Bernhard-Oettel, 2015; Taylor, 1991). Specifically, when people disengage from perceived obligations, their failure to fulfill obligations may trigger stronger emotional reactions from both the self and others compared with their fulfilllment of obligations. This may be due to the fact that obligations are mostly driven by normative expectations. For instance, fulfillling family obligations may not significantly enhance familial relational harmony for collectivism-preferred individuals as meeting these obligations is regarded as a norm and is thus already expected. In contrast, failure to meet family obligations could trigger strong negative consequences for familial relations due to its undesirable and unexpected nature, especially for collectivism-preferred cultures where expectations to maintain relational harmony are particularly intense. Similarly, for people from individualism-preferred cultures, the persistence to fulfill family obligations may not impact one’s personal control and autonomy as much as the liberating act of choosing not to meet family expectations (Peeters, 2002).
Importantly, our results in the domain of family and close friends were not entirely consistent with those in the domain of public community. In particular, the three-way interaction was significant for family and close friends but not for public community, which suggests that the moderating role of GDT on the impact of perceived obligation might be more relevant in situations that involve people who are closer to us. That is, we may not be as concerned or bothered if we withdrew help or support for individuals from the broader community as compared to doing the same with kin and close acquaintances. Given that those who are closer to us play a more significant role in our lives, whether we persist in fulfilling our obligations towards them is more likely to conjure stronger emotional reactions, such as feeling bad or guilty when we fail to meet expectations. Conversely, obligations in the domain of community, such as the duty to vote during elections or giving time or money to social causes, often carry some degree of diffusion of responsibility as they are perceived as more remote, detached from us, and hence less visceral (Rossi, 2001). These results therefore indicate that closeness matters where the personal ramifications of disengagement is concerned.
It is noteworthy that our findings do not contradict existing research that found positive associations between volunteerism, helping behaviors, and physical health outcomes (Post, 2005). A growing literature has demonstrated that acts of helping within the context of volunteerism are associated with numerous health benefits, such as lower risk of cardiovascular disease (Burr, Han, & Tavares, 2015) and even lower mortality rates (Okun, Yeung, & Brown, 2013). Interestingly, the positive associations between volunteerism and health outcomes were found to be consistent across individualism-preferred and collectivism-preferred cultures (e.g., Kumar, Calvo, Avendano, Sivaramakrishnan, & Berkman, 2012). However, it should be noted that although both the fulfillment of perceived obligations and volunteerism involve helping others, the underlying motivations for these two helping behaviors are distinct. The act of volunteerism is driven by an intrinsic altruistic motivation to help or support others, whereas the act of meeting perceived obligations is extrinsically driven. Correspondingly, the health consequences for these two types of helping behaviors differ. Indeed, studies on individualism-preferred cultures show that providing care that is extrinsically driven by a sense of inescapable obligation (such as the duty to support one’s family) can be detrimental to the physical health of caregivers, but not if it is driven by positive feelings about family support (Kim et al., 2007; Sayegh & Knight, 2010). It is reasonable to assume that for people from individualism-preferred cultures, providing intrinsically motivated care would not constrain their personal autonomy and, therefore, would not conflict with their cultural mandates.
Close scrutiny of the goal disengagement scale used in the present research reveals relatively higher inter-rater correlations for items that imply avoidance of rumination (e.g., “I stop thinking about a goal that has become unattainable and let it go”; “When something I wanted did not work out, I try not to think about it too much”). This may suggest that our measure of GDT centers particularly around cognitive or thought-related mechanisms that covary with the ability to avoid ruminating about goal loss and allow the stress of shortcomings in goal pursuit to pass, which may relate to an intervention typically associated with “mindfulness” (Frewen, Evans, Maraj, Dozois, & Partridge, 2008). Although mindfulness—a form of attention-awareness wherein observations and thoughts are processed in non-judging, de-centered, and non-attached ways—is typically associated with zen philosophy which in turn tends to be associated with cultures such as Japan (Kato, 2005), the current investigation showed that GDT interestingly did not aid the Japanese respondents. That said, as goal disengagement allows individuals to cope with stressful obligations and commitment while retaining their autonomy and personal control, such a coping strategy may be especially adaptive in individualism-preferred cultures valuing autonomy and personal control but prove to be ineffective for collectivism-preferred cultures, especially in the context of social obligations where relational harmony is at stake. Future research can tease apart further nuances in the effects of GDT with due consideration of specific goal domains.
Limitations
The MIDUS and MIDJA biomarker projects offer an invaluable source of robust and objective data for the exploration of cross-cultural differences in health-related research. However, our study is not without its limitations. For instance, the complexity of two-way and three-way interactions may render the sample size of the current study suboptimal for the detection of such interactions. This could also be an unforeseen alternative explanation for why we failed to find any associations between perceived obligation and biological health risk among participants with low GDT across cultures. As such, future studies should probe these associations using larger sample sizes. Another limitation of the current study pertains to the low reliability of our scales for perceived obligation and GDT, which is likely due to the small number of items in each scale (see Supplementary Materials). Future studies should utilize scales with greater reliability or employ multiple measures to examine perceived obligation and GDT. Taken together, these methodological limitations suggest that the results of the current study should be interpreted with some degree of caution.
While a cross-sectional design serves the current study well given the complexity of the analyses, future studies can shed further light by incorporating longitudinal designs to examine cross-cultural health trajectories as a function of perceived obligation, which may fluctuate across time and situation. Studying health trajectories helps not only with illuminating the specific mechanisms that underlie the associations between perceived obligation and health, but also with understanding the onset age of perceived obligations as a protective or risk factor of physical heath decline. Moreover, future studies can extend the current investigation to adolescent populations as the types of obligations perceived by adolescents differ vastly from mid-life adults (e.g., Darling, Cumsille, & Martínez, 2008). Despite the limitations associated with using a cross-sectional design, the current study has addressed several prominent methodological issues by employing large cross-cultural samples with rigorous and objective biomarker indicators to elucidate the relations between perceived obligations and biological health risks.
Conclusion
In conclusion, the current study highlights the importance of examining how perceived obligations influence physical health from a cultural perspective while incorporating individual differences in goal disengagement. Furthermore, the current study provides evidence for the hypothesis that culturally distinct pathways to positive health exist (Kitayama et al., 2010), thus highlighting the need to understand the factors that underlie our wellbeing with greater nuance.
Supplementary Material
Acknowledgements
This research was supported by grants from the National Institute on Aging (P01-AG020166 & 5R37AG027343) to conduct MIDUS II and MIDJA. A preliminary version of this research was presented at the 24th Congress of the International Association for Cross-Cultural Psychology. The authors declare no conflicts of interest
References
- Adler NE, Epel ES, Castellazzo G, & Ickovics JR (2000). Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, white women. Health Psychology, 19(6), 586–592. [DOI] [PubMed] [Google Scholar]
- Ayalon L (2015). Intergenerational perspectives on autonomy following a transition to a continuing care retirement community. Research on Aging, 38(2), 127–149. [DOI] [PubMed] [Google Scholar]
- Boylan JM, Tsenkova VK, Miyamoto Y, & Ryff CD (2017). Psychological resources and glucoregulation in Japanese adults: Findings from MIDJA. Health Psychology, 36(5), 449–457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burr JA, Han SH, & Tavares JL (2015). Volunteering and cardiovascular disease risk: Does helping others get “under the skin?” The Gerontologist, 1–12. [DOI] [PubMed] [Google Scholar]
- Coe CL, Love GD, Karasawa M, Kawakami N, Kitayama S, Markus HR, … & Ryff CD (2011). Population differences in proinflammatory biology: Japanese have healthier profiles than Americans. Brain, Behavior, and Immunity, 25(3), 494–502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conway N, Guest D, & Trenberth L (2011). Testing the differential effects of changes in psychological contract breach and fulfilllment. Journal of Vocational Behavior, 79(1), 267–276. [Google Scholar]
- Curhan KB, Sims T, Markus HR, Kitayama S, Karasawa M, Kawakami N, … & Ryff CD (2014). Just how bad negative affect is for your health depends on culture. Psychological Science, 25(12), 2277–2280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darling N, Cumsille P, & Martínez ML (2008). Individual differences in adolescents’ beliefs about the legitimacy of parental authority and their own obligation to obey: A longitudinal investigation. Child Development, 79(4), 1103–1118. [DOI] [PubMed] [Google Scholar]
- De Jong JD, Clinton M, Rigotti T, & Bernhard-Oettel C (2015). Nonlinear associations between breached obligations and employee well-being. Journal of Managerial Psychology, 30(4), 374–389. [Google Scholar]
- Dempster AP, Laird NM, & Rubin DB (1977). Maximum likelihood from incomplete data via the EM algorithm. Journal of the Royal Statistical Society: Series B (Methodological), 39(1), 1–22. [Google Scholar]
- Frewen PA, Evans EM, Maraj N, Dozois DJA, & Partridge K (2008). Letting go: Mindfulness and negative automatic thinking. Cognitive Therapy and Research, 32(6), 758–774. [Google Scholar]
- Friedman HS, Kern ML, & Reynolds CA (2010). Personality and health, subjective well-being, and longevity. Journal of Personality, 78(1), 179–216. [DOI] [PubMed] [Google Scholar]
- Greenfield PM, Keller H, Fuligni A, & Maynard A (2003). Cultural pathways through universal development. Annual Review of Psychology, 54(1), 461–490. [DOI] [PubMed] [Google Scholar]
- Hardin EE, Robitschek C, Flores LY, Navarro RL, & Ashton MW (2014). The cultural lens approach to evaluating cultural validity of psychological theory. American Psychologist, 69(7), 656–668. [DOI] [PubMed] [Google Scholar]
- Hashimoto H, & Yamagishi T (2015). Preference-expectation reversal in the ratings of independent and interdependent individuals: A USA–Japan comparison. Asian Journal of Social Psychology, 18(2), 115–123. [Google Scholar]
- Hayes AF (2012). PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling. Retrieved from http://www.afhayes.com/public/process2012.pdf
- Hong Y. y. (2009). A dynamic constructivist approach to culture: Moving from describing culture to explaining culture. In Wyer RS, Chiu C.-y., & Hong Y.-y. (Eds.), Understanding culture: Theory, research, and application (pp. 3–23). New York, NY, US: Psychology Press. [Google Scholar]
- Johnson BT, & Acabchuk RL (2018). What are the keys to a longer, happier life? Answers from five decades of health psychology research. Social Science & Medicine, 196, 218–226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kannan VD, Brown TM, Kunitz SJ, & Chapman BP (2019). Political parties and mortality: The role of social status and personal responsibility. Social Science & Medicine, 223, 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kato H (2005). Zen and psychology. Japanese Psychological Research, 47(2), 125–136. [Google Scholar]
- Kim JH, Knight BG, & Longmire CVF (2007). The role of familism in stress and coping processes among African American and White dementia caregivers: effects on mental and physical health. Health Psychology, 26(5), 564. [DOI] [PubMed] [Google Scholar]
- Kitayama S, Karasawa M, Curhan KB, Ryff CD, & Markus HR (2010). Independence and interdependence predict health and wellbeing: Divergent patterns in the United States and Japan. Frontiers in Psychology, 163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kitayama S, Park J, Boylan JM, Miyamoto Y, Levine CS, Markus HR, … & Ryff CD (2015). Expression of Anger and Health in Two Cultures An Examination of Inflammation and Cardiovascular Risk. Psychological Science, 26(2), 211–220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumar S, Calvo R, Avendano M, Sivaramakrishnan K, & Berkman LF (2012). Social support, volunteering and health around the world: Cross-national evidence from 139 countries. Social Science & Medicine, 74(5), 696–706. [DOI] [PubMed] [Google Scholar]
- Losada A, Márquez-González M, Knight BG, Yanguas J, Sayegh P, & Romero-Moreno R (2010). Psychosocial factors and caregivers’ distress: Effects of familism and dysfunctional thoughts. Aging & Mental Health, 14(2), 193–202. [DOI] [PubMed] [Google Scholar]
- Love G, Seeman TE, Weinstein M, & Ryff CD (2010). Bioindicators in the MIDUS national study: Protocol, measures, sample, and comparative context. Journal of Aging and Health, 22(8), 1059–1080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markus HR, Ryff CD, Conner AL, Pudberry EK, & Barnett KL (2001). Themes and variations in American understandings of responsibility. In Rossi AS (Ed.), Caring and doing for others: Social responsibility in the domains of family, work, and community (pp. 349–399). Chicago, IL: University of Chicago Press. [Google Scholar]
- Marshall GN, Wortman CB, Vickers RR, Kusulas JW, & Hervig LK (1994). The five-factor model of personality as a framework for personality-health research. Journal of Personality and Social Psychology, 67(2), 278–286. [DOI] [PubMed] [Google Scholar]
- Matsumoto D, & Juang L (2013). Culture and Psychology (5th ed.) Wadsworth, Cengage. [Google Scholar]
- Mroczek DK, & Kolarz CM (1998). The effect of age on positive and negative affect: A developmental perspective on happiness. Journal of Personality and Social Psychology, 75(5), 1333–1349. [DOI] [PubMed] [Google Scholar]
- Nguyen CD, Strazdins L, Nicholson JM, & Cooklin AR (2018). Impact of missing data strategies in studies of parental employment and health: Missing items, missing waves, and missing mothers. Social Science & Medicine, 209, 160–168. [DOI] [PubMed] [Google Scholar]
- O’Connor MF, Bower JE, Cho HJ, Creswell JD, Dimitrov S, Hamby ME, … & Thomas KS (2009). To assess, to control, to exclude: effects of biobehavioral factors on circulating inflammatory markers. Brain, Behavior, and Immunity, 23(7), 887–897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okun MA, Yeung EW, & Brown S (2013). Volunteering by older adults and risk of mortality: A meta-analysis. Psychology and Aging, 28(2), 564–577. [DOI] [PubMed] [Google Scholar]
- Oyserman D, Coon HM, & Kemmelmeier M (2002). Rethinking individualism and collectivism: Evaluation of theoretical assumptions and meta-analyses. Psychological Bulletin, 128(1), 3–72. [PubMed] [Google Scholar]
- Park J, Kitayama S, Karasawa M, Curhan K, Markus HR, Kawakami N, … & Ryff CD (2013). Clarifying the links between social support and health: Culture, stress, and neuroticism matter. Journal of Health Psychology, 18(2), 226–235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peeters G (2002). From good and bad to can and must: Subjective necessity of acts associated with positively and negatively valued stimuli. European Journal of Social Psychology, 32(1), 125–136. [Google Scholar]
- Post SG (2005). Altruism, happiness, and health: It’s good to be good. International Journal of Behavioral Medicine, 12(2), 66–77. [DOI] [PubMed] [Google Scholar]
- Ross CE, & Mirowsky J (2013). The sense of personal control: Social structural causes and emotional consequences. In Aneshensel CS, Phelan JC & Bierman A (Eds.), Handbook of the Sociology of Mental Health (pp. 379–402). Netherlands: Springer. [Google Scholar]
- Rossi AS (2001). Caring and doing for others: Social responsibility in the domains of family, work, and community. Chicago, IL: University of Chicago Press. [Google Scholar]
- Rubin DB (1987). Multiple imputation for nonresponse in surveys. New York, NY: Wiley. [Google Scholar]
- Sayegh P, & Knight BG (2010). The effects of familism and cultural justification on the mental and physical health of family caregivers. Journals of Gerontology: Series B, 66(1), 3–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sidi Y, & Harel O (2018). The treatment of incomplete data: Reporting, analysis, reproducibility, and replicability. Social Science & Medicine, 209, 169–173. [DOI] [PubMed] [Google Scholar]
- Spielberger CD (1996). State-trait anger expression inventory: Professional manual. Odessa, FL: Psychological Assessment Resources. [Google Scholar]
- Tam K-P, & Lee S-L (2010) What Values Do Parents Want to Socialize in Their Children? The Role of Perceived Normative Values. Journal of Cross-Cultural Psychology, 21(2), 175–181 [Google Scholar]
- Tam K-P, & Chan H-W (2015). Parents as cultural middlemen: The role of perceived norms in value socialization by ethnic minority parents. Journal of Cross-Cultural Psychology, 46, 489–507. [Google Scholar]
- Taylor SE (1991). Asymmetrical effects of positive and negative events: The mobilization-minimization hypothesis. Psychological Bulletin, 110(1), 67–85. [DOI] [PubMed] [Google Scholar]
- Xu H (2019). Physical and mental health of Chinese grandparents caring for grandchildren and great-grandparents. Social Science & Medicine, 229, 106–116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wrosch C, Heckhausen J, & Lachman ME (2000). Primary and secondary control strategies for managing health and financial stress across adulthood. Psychology and Aging, 15(3), 387–399. [DOI] [PubMed] [Google Scholar]
- Wrosch C, Scheier MF, Miller GE, Schulz R, & Carver CS (2003). Adaptive self-regulation of unattainable goals: Goal disengagement, goal reengagement, and subjective well-being. Personality and Social Psychology Bulletin, 29(12), 1494–1508. [DOI] [PubMed] [Google Scholar]
- Zou X, Tam KP, Morris MW, Lee SL, Lau IY, & Chiu CY (2009). Culture as common sense: Perceived consensus versus personal beliefs as mechanisms of cultural influence. Journal of Personality and Social Psychology, 97(4), 579–597. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.