

Abstract
Appendix-associated hernias are extremely rare. They have been described sporadically in the literature, mostly as inguinal hernias. Appendix-associated incisional hernias are even more unusual. High clinical awareness is needed as complications can arise if misdiagnosis or delay occurs. We present an 80-year-old man with acute appendicitis in an incisional hernia. After successful surgery, the patient made a full recovery.
Keywords: Acute appendicitis, Incisional hernia, Hernia surgery
Case history
Our patient was an 80-year-old man with a past medical history of open cholecystectomy, prostatectomy and bilateral inguinal hernia repair. At the site of his Kocher incision, he had a 2×2cm incisional hernia diagnosed 35 years ago. As he was asymptomatic, he never sought medical attention.
He presented to the emergency room with a three-day history of upper abdominal pain, asthenia, nausea and vomiting. On clinical examination, he was febrile, tachycardic and dehydrated. He had a 3×2cm non-reducible painful mass around the Kocher incision, with pain on touch and tenderness.
Examination revealed mild leucocytosis without neutrophilia. Abdominal echography was inconclusive. Contrast-enhanced abdominal computed tomography (CT) revealed a 2×2cm abdominal wall defect over the previous Kocher incision. The hernia sac contained an inflamed appendix; its wall measured over 6mm and had slight fat enhancement (Figure 1). The diagnosis was acute appendicitis within an incarcerated incisional hernia.
Figure 1 .
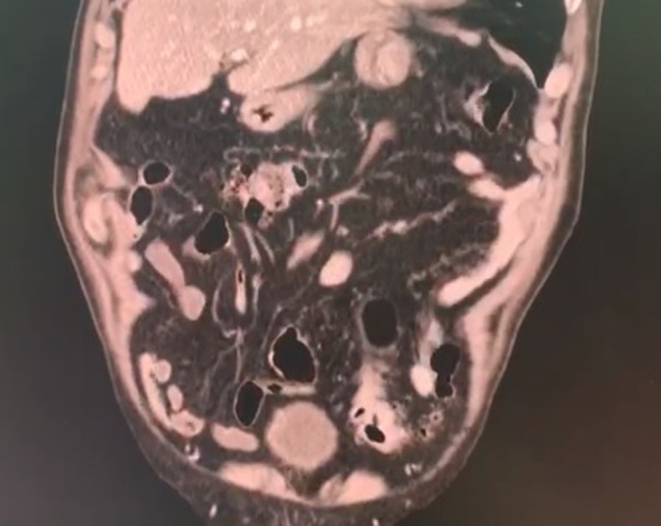
Computed tomography: the appendix is seen in the hernia sac
The patient had a surgical consultation, and surgery was planned. At surgery, a 2×2cm abdominal wall defect was identified over the previous incision. The hernia sac was opened, unveiling the caecum and appendix. On gross examination, the appendix measured 12cm in length and 0.7cm in diameter. The external surface of the appendix was pink and showed congestion (Figures 2 and 3).
Figure 2 .
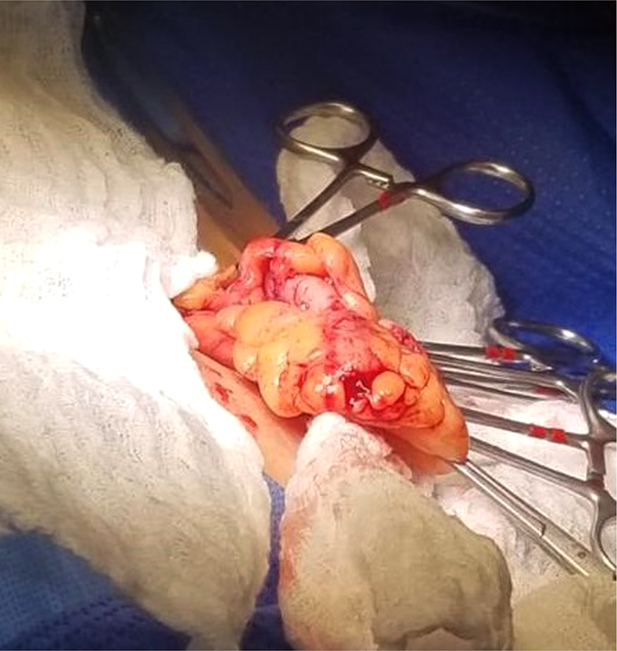
Appendix during surgery
Figure 3 .

Appendectomy
Appendectomy was completed, and the abdominal wall defect was sutured using a 1-0 non-absorbable suture (Prolene, Ethicon, Somerville, NJ, USA). A mesh was considered but ruled out due to the high risk of infection.
Pathology reported acute appendicitis.
The postoperative period was uneventful. A liquid diet was initiated on the first postoperative day and was followed by a full diet. The patient was discharged on his third postoperative day without complications. Six months later, the patient is doing well and has no hernia recurrence.
Discussion
The presence of the appendix within an anterior wall hernia, inflamed or not, was first reported by Claudius Amyand in 1735.1,2 This rare phenomenon (incidence 0.51%) is thought to be caused by atypical positions of the caecum and appendix, malrotation of the intestine or previous surgery.1,3 When the appendix is in an abdominal wall hernia, it is usually in the inguinal (Amyand hernia) or femoral (De Garengeot hernia) canal on the right side.1,3,4 It is extremely rare to encounter the appendix in an incisional hernia. This has been described in limited case reports, mostly in Pfannenstiel incisions, umbilical hernias, trocar entry sites, Spigelian hernias and upper midline laparotomies (Table 1).1,5
Table 1 .
Previous case reports from acute appendicitis within incisional hernias
| Ref. | Age / sex | Presentation | Hernia location | Preoperative diagnosis | Outcome | Perforated appendix | Mesh | Approach |
|---|---|---|---|---|---|---|---|---|
| 6 | 71 F | Lower abdominal pain and mass | Previous ileostomy | CT | Complete recovery | Yes | No | Open |
| 7 | N/A F | Abdominal pain | Port-site hernia | N/A | N/A | Yes | No | Open |
| 8 | 27 F | Abdominal pain | Pfannenstiel | CT | Complete recovery | No | No | Laparoscopic |
| 9 | 78 M | Abdominal pain | Midline | CT | Complete recovery | No | Biological | Open |
| 81 M | Abdominal pain | Port-site hernia | CT | Complete recovery | No | N/A | Open | |
| 10 | 48 F | Abdominal pain | Pfannenstiel | CT | Complete recovery | No | No | Laparoscopic |
| 11 | 57 M | Abdominal pain | Lumbotomy incision | CT | Complete recovery | No | Polypropylene | Open |
| 12 | 37 F | Upper abdominal pain | Port-site hernia | CT | Complete recovery | No | Polypropylene | Open |
| 13 | 62 F | Abdominal pain | Pfannenstiel | Abdominal x-ray | Complete recovery | Yes | No | Open |
| 14 | 51 F | Nausea, bloating, intermittent vomiting, fever, diarrhoea | Ventral hernia | CT | Complete recovery | Yes | No | Laparoscopic |
| 15 | 70 F | Lower abdominal pain, constipation | Incisional hernia over right iliac crest | CT | Complete recovery | No | No | Open |
In our patient, we detected the appendix in the previous Kocher incision, an event that has not been described in the literature. We speculate that his previous surgery may have created adhesions, leading to the unusual location of the appendix.
Unlike routine appendicitis, it is thought that extraluminal compression leads to acute inflammation; however, primary appendicitis can still occur.1,2 The clinical presentation of this rare pathology does not follow the course of acute appendicitis but rather shows the symptoms of an incarcerated hernia, which could lead to higher perforation rates.1,3 As symptoms may be atypical, high clinical suspicion is needed. Preoperative diagnosis based on clinical symptoms is difficult. CT can demonstrate the appendix within the hernia. Our patient had symptoms mimicking an incarcerated hernia, but CT aided in the diagnosis.4 Appendectomy and hernia repair using laparoscopic or open approaches form the treatment of choice.1, 4
Due to the late diagnosis and complications associated with appendiceal hernias, combined with the high risk of infection following a hernia repair when the appendix is acutely inflamed, repairing the defect with a mesh is still controversial. A large amount of newer literature advocates the use of prosthetic or biological mesh in clean-contaminated or contaminated ventral hernias because use dramatically decreases recurrence rates. Considering the rarity of incisional hernia appendicitis, however, and since most of our experience results from the management of Amyand hernias, these recommendations from other fields of study should be considered cautiously. The decision to use a mesh will depend on the patient and the intraoperative findings.1,16 In our case, the repair was deferred to avoid the risk of infection, as the hernia could be addressed at a later stage.
Conclusions
Incisional hernia appendicitis is an uncommon pathology that must be treated promptly. The risk of potential complications due to delayed perioperative diagnosis and treatment is high due to the low incidence and atypical clinical presentation. It is possible for the appendix to become incarcerated in any abdominal wall hernia, and surgeons should always be aware of these rare entities, since delay can potentially change the outcome.
References
- 1.Sugrue C, Hogan A, Robertson Iet al. Incisional hernia appendicitis: a report of two unique cases and literature review. Int J Surg Case Rep 2013; 4: 256–258. 10.1016/j.ijscr.2012.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tubbs SR. Amyand's hernia: a review. Med Sci Monit 2014; 20: 140–146. 10.12659/msm.889873 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Menenakos C, Tsilimparis N, Guenther N, Braumann C. Strangulated appendix within a trocar site incisional hernia following laparoscopic low anterior rectal resection: a case report. Acta Chir Belg 2009; 109: 411–413. 10.1080/00015458.2009.11680450 [DOI] [PubMed] [Google Scholar]
- 4.Dittmar Y, Scheuerlein H, Götz M, Settmacher U. Adherent appendix vermiformis within an incisional hernia after kidney transplantation mimicking acute appendicitis: report of a case. Hernia 2010; 16: 359–361. [DOI] [PubMed] [Google Scholar]
- 5.Lam A, Black J, Parnell B, West C. Appendicitis due to incarceration within a laparoscopic umbilical port-site hernia secondary to a degree of intestinal malrotation. Ann R Coll Surg Engl 2019; 101: e119–e121. 10.1308/rcsann.2019.0034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Becker D, Woodfield J. Complicated appendicitis within an incisional hernia. ANZ J Surg 2019; 89: E270–E271. 10.1111/ans.14339 [DOI] [PubMed] [Google Scholar]
- 7.Cerná M, Sulc R, Kacerovská D. [Incisional hernia following laparoscopy, complicated by perforated gangrenic appendicitis: a case review.] Rozhl Chir 2011; 90: 519–522. 10.1038/s43018-020-0074-y [DOI] [PubMed] [Google Scholar]
- 8.Galiñanes EL, Ramaswamy A. Appendicitis found in an incisional hernia. J Surg Case Rep 2012; 2012: 3. 10.1093/jscr/2012.8.3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sugrue C, Hogan A, Robertson Iet al. Incisional hernia appendicitis: a report of two unique cases and literature review. Int J Surg Case Rep 2013; 4: 256–258. 10.1016/j.ijscr.2012.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kler A, Hossain N, Singh S, Scarpinata R. Vermiform appendix within incisional hernia. BMJ Case Rep 2017; 2017: bcr2017221216. 10.1136/bcr-2017-221216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Al-Hadithy N, Erotocritou P, Portou MJ, Hamilton H. Appendicitis in an incisional hernia after radical nephrectomy: a case report. Ann R Coll Surg Engl 2010; 92: W23–W24. 10.1308/147870810x12699662981230 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lam A, Black J, Parnell B, West CT. Appendicitis due to incarceration within a laparoscopic umbilical port-site hernia secondary to a degree of intestinal malrotation. Ann R Coll Surg Engl 2019; 101: e119–e121. 10.1308/rcsann.2019.0034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Horgan PG, O'Donoghue J, Courtney D. Perforated appendicitis in an incisional hernia. Ir J Med Sci 1991; 160: 350–351. 10.1007/bf02957893 [DOI] [PubMed] [Google Scholar]
- 14.Kane ED, Bittner KR, Bennett Met al. A case report of unexpected pathology within an incarcerated ventral hernia. Int J Surg Case Rep 2017; 38: 61–65. 10.1016/j.ijscr.2017.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Singal R, Mittal A, Gupta Aet al. An incarcerated appendix: report of three cases and a review of the literature. Hernia 2012; 16: 91–97. 10.1038/s43018-020-0074-y [DOI] [PubMed] [Google Scholar]
- 16.Logan MT, Nottingham JM. Amyand's hernia: a case report of an incarcerated and perforated appendix within an inguinal hernia and review of the literature. Am Surg 2010; 67: 628–629. 10.1038/s43018-020-0074-y [DOI] [PubMed] [Google Scholar]