

Abstract
Retinoblastoma eyes with choroidal invasion may not have to be enucleated and may be successfully managed with OAC using Melphalan, Carboplatin and Topotecan without compromising patient survival.
Keywords: retinoblastoma, ophthalmic artery chemosurgery, intraarterial chemotherapy, choroidal invasion
Introduction
Choroidal invasion in retinoblastoma eyes is common and histopathological evidence is found in approximately a quarter of enucleated eyes1. It was previously thought eyes with choroidal invasion more often developed metastatic disease and therefore should be enucleated. In fact, some authors have recommended enucleation in eyes for the purpose of detecting choroidal invasion, and if found, recommending multiagent (adjuvant) systemic chemotherapy2. More recently many authors have questioned whether choroidal invasion (by itself) is really associated with a higher rate of metastases3 and whether the finding of choroidal invasion alone warrants adjuvant systemic chemotherapy3.
Because choroidal invasion was routinely managed by enucleation worldwide, there have been few attempts or reports on treating such eyes without enucleation. There were no discussions about the use of external beam irradiation for choroidal invasion in the literature.
In 2018 we were the first to report on the successful eye saving treatment of choroidal invasion in two patients managed with intraarterial chemotherapy4. Later that year two additional patients were reported from Switzerland5: One received intraarterial chemotherapy and did well, the second had clinical disappearance of tumor confirmed with imaging after receiving systemic multiagent chemotherapy, but died of complications from the systemic chemotherapy. We have now successfully treated 4 patients with OAC who developed “massive” choroidal invasion > 3mm in diameter and now report on longer follow-up of the first two and add two additional cases.
Methods and materials
This retrospective small series of 4 eyes was approved by the Institutional Review Board of Memorial Sloan Kettering Cancer Center. Informed consent was obtained. The study was Health Insurance Portability and Accountability Act (HIPAA) compliant. Research adhered to the tenets of the Declaration of Helsinki. Choroidal invasion was diagnosed clinically by amelanotic elevation of the choroid by ophthalmoscopy and confirmed with ultrasonography.
Results:
Case descriptions (summarized in supplemental Table 1):
Update on previously reported cases10:
Case 1: A 7-month-old infant was diagnosed with bilateral retinoblastoma. The right eye was classified as Reese Ellsworth (RE) Va and International Classification of Retinoblastoma/COG Version (ICRb) E and the left eye as RE Va, ICRb E. The right eye was primarily enucleated elsewhere. Thirty-two months prior, the left eye had received systemic chemotherapy (Vincristine, Carboplatin and Etoposide (VEC)) elsewhere and referred when the tumors regrew. The eye was treated with OAC three times (Melphalan 2.5mg and Carboplatin 30mg x 1, Melphalan 3mg and Carboplatin 40mg x 2) followed by laser and two intravitreal melphalan (30mcg) injections with control of all tumors. Three months following completion of initial treatment, choroidal invasion developed. After just one OAC session with Melphalan 4mg, Carboplatin 40mg and Topotecan 1mg complete resolution of the choroidal invasion occurred. One additional session of OAC was delivered (Topotecan 2mg, Carboplatin 40mg). Thirty-five months later the vision was 20/60. No metastases developed.
Case 2: A 7-month-old infant with familial retinoblastoma was diagnosed with bilateral disease. Both eyes were classified as RE IIIa, ICRb C. Twenty-one months after three sessions of OAC (Melphalan 3–4mg and Topotecan 0.5mg) and multiple lasers, choroidal invasion developed in the right eye (Figure 1). The choroidal invasion disappeared after one OAC session (Melphalan 5mg, Topotecan 2mg, Carboplatin 70mg). Two additional sessions of OAC were delivered (both Melphalan 5mg, Topotecan 2mg, Carboplatin 60mg. Sixty-six months later vision is 20/200 and the child is metastases free.
Figure 1:
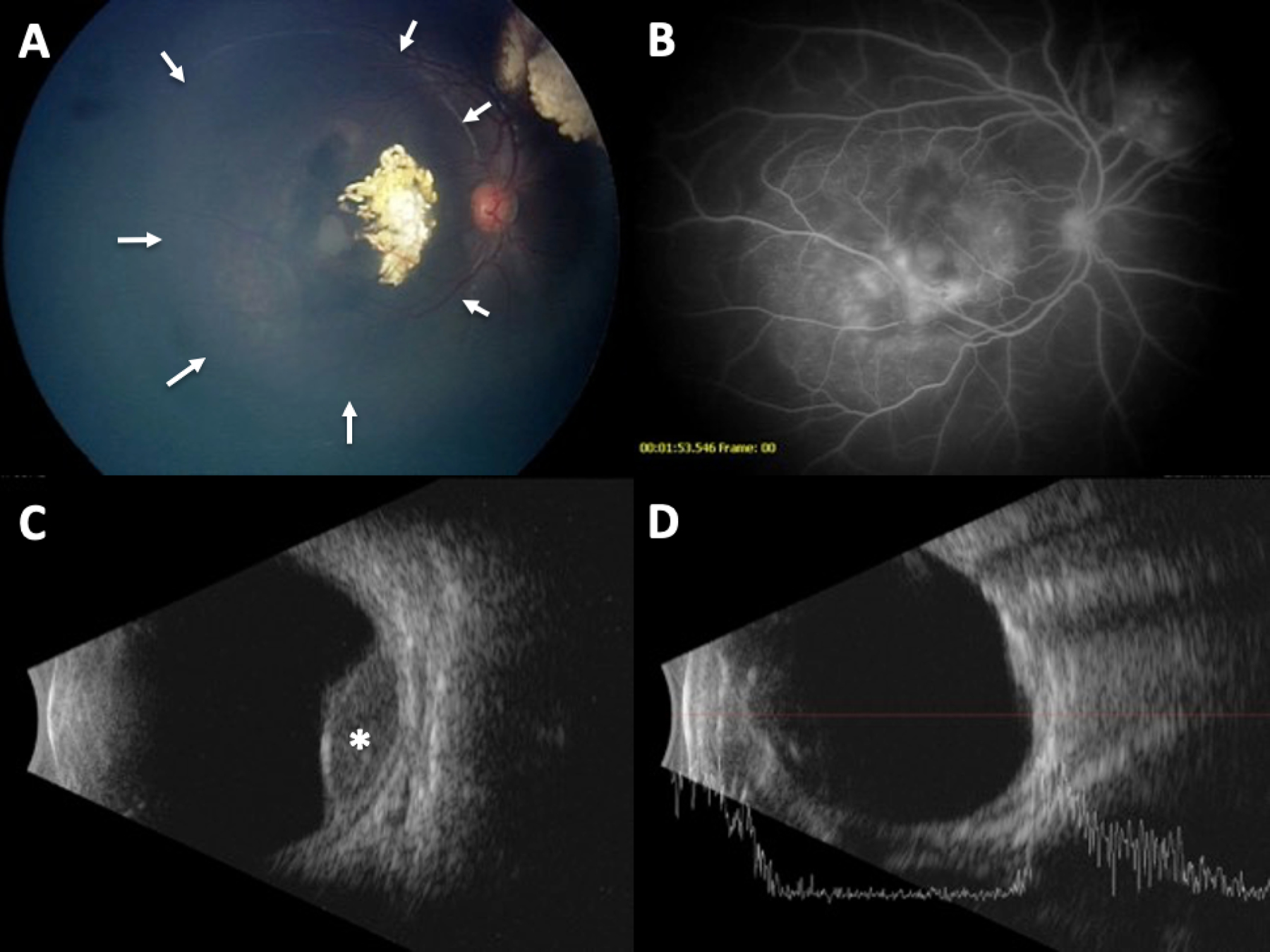
Representative images of case 2: At 25 months following completion of primary treatment with OAC, choroidal invasion was noted beneath the macula tumor of the right eye as shown in this RetCam image (arrows) (A). The choroidal invasion was delineated by hyperfluorescence on fluorescein angiography (B) and the mass appeared as a dome-shaped choroidal elevation on ultrasonography (asterisk) (C). After two cycles of OAC, the choroidal mass has regressed to a flat scar by ultrasonography (D).
New cases:
Case 3: A 23-month-old was diagnosed with bilateral retinoblastoma. The right eye was classified as RE Vb, ICRb D and the left RE IIa ICRb D. The left eye received OAC three times (Carboplatin 40mg, Topotecan 0.5mg) in addition to laser, cryotherapy and three intravitreal melphalan injections (30mcg x 2, 25mcg x 1) and 17 months following completion of initial treatment, choroidal invasion developed in the left eye. Within one treatment of OAC (Melphalan 5mg, Topotecan 1mg, Carboplatin 40mg) the choroidal invasion disappeared. Two additional sessions of OAC were delivered using the same drugs and dosages. Vision 18 months later was Finger Counting and there is no evidence of metastases.
Case 4: An 11-month-old was diagnosed with bilateral retinoblastoma. Twenty-four months prior, the right eye was classified as RE IIIb/ICRb C and the left with RE IVb, ICRb D and she was treated with 4 cycles of systemic chemotherapy (VEC) elsewhere. After bilateral recurrences we treated the child with OAC to both eyes (to the right eye: Carboplatin 30mg Topotecan 0.5mg x 1; Melphalan 3mg and Carboplatin 30mg x 2) and laser, cryotherapy and intravitreal injections melphalan 25mcg seven times and topotecan 20–30mcg twice, and 6 months following completion of the above treatment, she developed cilio-choroidal invasion in the right eye (supplemental Figure 2). The eye was treated with OAC (Melphalan 5mg, Carboplatin 30mg and Topotecan 0.5mg) and within a month had complete disappearance of the cilio-choroidal invasion. Two additional sessions of OAC were delivered (Melphalan 5mg, Topotecan 0.5mg, Carboplatin 30mg followed by Melphalan 5mg, Topotecan 0.5mg, Carboplatin 30mg). With 20-months follow-up there was no recurrence and vision was central, steady, maintained and the child is metastases free.
Discussion
We present four eyes of four children with bilateral retinoblastoma who had eye saving treatments (systemic chemotherapy, intrarterial chemotherapy and focal treatments with laser, cryotherapy and intravitreal injection) who developed choroidal invasion 3, 6, 17 and 21 months later. In all cases the choroidal invasion responded to one OAC session and all 4 eyes retained vision comparable to what they had before treatment. No child has developed metastases to date.
Choroidal invasion has been routinely treated by enucleation because of a perception that it is associated with a higher risk of developing metastases. Some centers recommend enucleating an eye for the purpose of detecting choroidal invasion and then aggressively treating that with multiagent systemic chemotherapy because of the belief that leaving in such an eye could be a threat to life. Some authors also feel that treating an eye with choroidal invasion, may downstage the tumor and pose a risk2. There is debate on the utility of adjuvant systemic chemotherapy for high-risk pathological features, such as choroidal invasion. This present small series demonstrates that children with choroidal invasion can successfully retain their eye and remain metastases-free without systemic chemotherapy at a median of 28 months follow up.
Ophthalmic artery chemotherapy (OAC) delivers concentrations to the eye that are approximately 100 times that of intravenous delivery6 7 but because the systemic dose is so low it rarely (<1%) requires transfusion of any blood products or causes fever/neutropenia of clinical significance6. Because the choroid receives a very high concentration of drug, we thought it reasonable to treat eyes with choroidal invasion with OAC, and based on these successes will continue to explore this option for eyes with choroidal invasion since there were no untoward ocular consequences nor any metastases.
Supplementary Material
Acknowledgements
Supported in part by grants from the Fund for Ophthalmic Knowledge, Inc. New York, N.Y. and Cancer Center Support Grant (P30 CA008748). The sponsor or funding organization had no role in the design or conduct of this research.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interests: None of the authors have any relevant financial disclosures or conflicts.
References
- 1.Chévez-Barrios P, Eagle RC, Krailo M, et al. Study of Unilateral Retinoblastoma With and Without Histopathologic High-Risk Features and the Role of Adjuvant Chemotherapy: A Children’s Oncology Group Study. J Clin Oncol 2019;37:2883–2891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Zhao J, Dimaras H, Massey C, et al. Pre-enucleation chemotherapy for eyes severely affected by retinoblastoma masks risk of tumor extension and increases death from metastasis. J Clin Oncol 2011;29:845–851. [DOI] [PubMed] [Google Scholar]
- 3.Bosaleh A, Sampor C, Solernou V, et al. Outcome of children with retinoblastoma and isolated choroidal invasion. Arch Ophthalmol 2012;130:724–729. [DOI] [PubMed] [Google Scholar]
- 4.Abramson DH, Francis JH, Gobin YP. Choroidal Invasion in Retinoblastoma Treated with Intrarterial Chemotherapy. Ophthalmology Retina 2018;2:9. [DOI] [PubMed] [Google Scholar]
- 5.Stathopoulos C, Gaillard M-C, Puccinelli F, et al. Successful conservative treatment of massive choroidal relapse in 2 retinoblastoma patients monitored by ultrasound biomicroscopy and/or spectral domain optic coherence tomography. Ophthalmic Genet 2018;39:242–246. [DOI] [PubMed] [Google Scholar]
- 6.Schaiquevich P, Fabius AW, Francis JH, et al. OCULAR PHARMACOLOGY OF CHEMOTHERAPY FOR RETINOBLASTOMA. Retina (Philadelphia, Pa) 2016. [DOI] [PubMed] [Google Scholar]
- 7.Abramson DH, Francis JH, Gobin YP. What’s New in Intra-Arterial Chemotherapy for Retinoblastoma? Int Ophthalmol Clin 2019;59:87–94. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.