

Abstract
Purpose of the review:
Along with the marked increase in the population of older adults with obesity is the need for effective strategies to treat aging- and obesity-related complications. This review highlights recent progress in obesity management in older adults.
Recent findings:
While calorie restriction (CR) is needed to significantly reduce fat mass, an exercise protocol is crucial to ameliorate functional outcomes. The addition of a resistance exercise protocol improves muscle protein synthesis response to anabolic stimuli, preventing the CR-induced reduction in muscle and bone mass. The addition of an aerobic exercise protocol improves cardiorespiratory fitness and cognitive function. However, the addition of both aerobic and resistance exercise protocols to CR provides the greatest improvement in myocellular quality, frailty, and cardiometabolic and cognitive outcomes, translating into the greatest improvement in quality of life. Such comprehensive lifestyle intervention also effectively improves glucometabolic control and age-relevant outcomes in older adults with type 2 diabetes. When combined with testosterone therapy, such lifestyle protocol preserves muscle and bone mass in older, hypogonadal men with obesity.
Summary:
We conclude that CR among older adults with obesity should be prescribed in combination with both aerobic and resistance exercise to maximize benefits on overall health.
Keywords: Aging, Sarcopenia, Frailty, Exercise, Diet
1. Introduction
The number of older adults (age ≥65 years) is steeply rising worldwide. In 2017, older adults accounted for 13% of the global population and are expected to reach the 20% by 2030 (1). As obesity prevalence is estimated to affect the 50% of older adults in the next few decades (2), effective approaches able to promote healthy aging while curbing the obesity pandemic are warranted. Studies conducted in older adults with functional impairments are in fact scarce (3). Calorie restriction (CR) strategies have been extensively investigated to promote weight loss. However, CR in older adults holds the potential risk of inducing muscle and bone loss, hence increasing the risk of frailty and disability (4, 5). Aging is associated with profound body composition changes—fat mass increases and redistributes in favor of visceral adipose depots while both muscle and bone mass decrease (4). Importantly, along with the reduction in muscle mass is the further reduction in muscle strength. Accordingly, sarcopenia is common among older adults with obesity (sarcopenic obesity) and is closely associated with frailty (4, 6, 7). The age-related changes in body composition not only increase the risk of frailty and disability, but also strongly contribute to the deterioration in cardiometabolic health (6, 8). In addition, both aging and obesity are associated with cognitive decline and increased risk of dementia (9). Successful protocols able to induce fat mass loss while preserving muscle and bone mass are hence pivotal to reduce the aging- and obesity-related cardiometabolic and cognitive deterioration and prevent frailty. In this article, we summarize the most recent evidence from the literature reporting the effect of CR (alone or in combination with different exercise protocols) on the health-related outcomes of older adults with obesity along with promising strategies to promote long-term weight loss maintenance.
2. Body composition and frailty
Besides resulting in fat mass reduction, weight loss interventions may lead to muscle and bone mass loss, a phenomenon particularly detrimental among older adults with obesity as it increases the risk of frailty and disability (4, 6). The combination of CR and exercise training is a well-established therapeutic approach among older adults with obesity as it induces fat mass loss while minimizing muscle and bone mass loss compared to CR or exercise alone (10). Importantly, such lifestyle intervention results in the greatest improvement in physical function and reduction of frailty, associated with enhancement of quality of life (10). Interestingly, the addition of testosterone therapy (anabolic stimulation) to the same lifestyle protocol in older males with obesity and hypogonadism, led to a better preservation of muscle mass and bone mineral density (BMD) compared to placebo, even though it did not result in further improvement in overall physical function (11•). These data are of relevance as low testosterone levels are extremely frequent among older men with obesity, which contribute to physical and cognitive decline in this population (12).
The CR protocol in these types of lifestyle intervention includes a balanced diet consisting of ~500–750 Kcal energy restriction per day with the following composition: ~30% of energy from fat, 50% from carbohydrate, and 20% from protein (or at least ~1.0 g/kg protein/day) supplemented with multivitamin and minerals (1500 mg Ca/day and 1000 IU vitamin D/day) to protect against deficiencies. When incorporated with behavioral strategies, this CR protocol usually results in ~10% weight loss over 6 months. On the other hand, the exercise protocol includes the following: i. resistance training: where muscles work against a weight or force (e.g., bench press, knee extensions), 1–3 sets of 8–12 repetitions performed at 60–80% of 1-repetition maximum for 2–3 days per week; ii. aerobic training: where heart pumps faster (e.g., running, cycling), 20–60 min/session performed at 60–75% of the maximum heart rate for 3–7 days per week; iii. balance training: exercises emphasizing static and dynamic postures (e.g., heel-to-toe walking, standing on one foot), 1–2 sets for 3–7 days per week (13).
Based on the Lifestyle Intervention Trial in Obese Elderly (LITOE) conducted on 160 frail, older adults with obesity, the same CR protocol combined with resistance and aerobic exercise training resulted in the greatest preservation of muscle and bone mass, and in the greatest improvement in muscle strength and physical function compared to CR plus aerobic or resistance training alone (14, 15). The same lifestyle intervention led to the greatest reduction in ectopic fat deposition in visceral depots and in skeletal muscle (16•), suggesting the greatest amelioration of muscle quality among the interventions tested. Accordingly, a substudy of the LITOE conducted on 47 subjects also reported the greatest improvement in muscle quality among the calorie restricted individuals performing both exercise types—greatest reduction in the expression of atrophy-related genes (LAMP2) and of inflammatory (TLR2, CD68) and mitochondrial stress (FIS1, PARL, OPA1) markers in the vastus lateralis, indicating an attenuated myocellular stress due to the intervention (17). On the other hand, CR plus aerobic exercise alone provoked the greatest increase in peak oxygen consumption (VO2peak), skeletal muscle mitochondrial function, and expression of modulators of mitochondrial fusion, fission and mitophagy (OPA1, MFF, DRP), but led to the least preservation of skeletal muscle mass (17). Although aerobic training was shown to prevent the age-related decline in mitochondrial respiratory capacity (18), it is possible that in the context of CR and frailty, the elevated activation of the oxidative network leads to an excessive catabolic stimulation and therefore muscle mass loss (17). The expression of the muscle regeneration regulator MEF2A was in fact reduced among calorie restricted individuals performing aerobic exercise, while it was preserved when a resistance exercise component was added to the protocol (17). A resistance exercise component (with or without aerobic exercise) was also necessary to improve muscle strength and preserve muscle mass in the same study population (14, 17). Accordingly, muscle protein synthesis (MPS) response to anabolic stimuli (mixed meal), typically impaired among older adults (19), improved only when a resistance exercise component was included in the intervention (17). The importance of resistance exercise during CR was also evidenced in the context of bone health—while aerobic exercise led to the greatest decrease in total hip and femoral neck BMD (~−2.5%) and to the greatest increase in circulating bone turnover markers (reflecting an excessive catabolic stimulation), these were relatively preserved when resistance training was included in the exercise protocol (15).
Overall, these results suggest the importance of performing both aerobic and resistance exercise in conjunction with CR among older adults with obesity to induce the greatest improvement in body composition and frailty outcomes. Furthermore, based on data from a recent metanalyses that included 1317 adults, the CR-induced improvement in physical function varies in a sex and race dependent manner (20), both variables that would be important to account for in future studies.
3. Cardiometabolic profile
Aging and obesity are associated with increased dyslipidemia, insulin resistance, and hypertension all of which strongly contribute to an individual’s cardiometabolic risk (8, 21). Insulin resistance and type 2 diabetes (T2D) can be effectively counteracted through lifestyle intervention—both CR-induced weight loss and exercise have been proven to ameliorate glucose control and are considered the first line of intervention to treat prediabetes and T2D (21, 22). However, most of the data have been based on studies in younger adults and evidence of their efficacy among older adults are lacking. Losing weight through lifestyle change is difficult and engagement in such activities is particularly challenging among older adults. Furthermore, what works in younger adults cannot be assumed to be effective among older adults with frailty, hence the adoption of such strategies to counteract T2D among older adults is still controversial (22). Our group recently conducted a randomized controlled trial on 100 older adults with T2D and chronic comorbidities to assess the efficacy of lifestyle intervention in improving glycemic control and age-relevant health outcomes (Lifestyle Intervention for Seniors with Diabetes; LISD) (23•). Participants were randomized to one-year intensive lifestyle intervention (ILI) (CR and exercise at a facility transitioned into community-fitness centers and homes) or healthy lifestyle (control group). The group randomized to ILI significantly lost weight (~10%) associated with improvements in HbA1c levels (~ −1%), VO2peak, gait, and overall physical function compared to controls (23•). Furthermore, the ILI group experienced a significant reduction in total and visceral fat mass and a moderate loss in total lean body mass (−1.2 kg) compared to controls. Despite the loss of lean body mass, muscle strength improved, indicating a positive effect of the ILI on muscle quality. The between-group differences in HbA1c were lost after adjusting data for changes in VO2peak, thus pointing to the critical link between the improvements in cardiovascular fitness and glucometabolic control. Furthermore, the between-group differences in HbA1c were also eliminated after adjusting data for changes in fat mass, pointing to the importance of improvement in body composition as a potential mediator of improvement in glucometabolic health (8). These findings are in line with the recent report from the LITOE that 10% CR-induced weight loss in combination with aerobic and resistance exercise reduced ectopic fat deposition (visceral and intermuscular fat), findings that correlated with improvement in cardiometabolic profile (i.e., insulin sensitivity index) (16•). Visceral and ectopic fat deposition are in fact associated with low-grade inflammation and insulin resistance in humans and animal models (8).
Obesity may accelerate the age-related increase in aortic stiffness which in turn is associated with cardiovascular disease, dementia, and kidney disease (24). In a study comparing the effect of aerobic exercise alone or in combination with high-intensity CR (~−600 Kcal from total energy expenditure) or moderate CR (~−250 Kcal from total energy expenditure), Brinkley and colleagues demonstrated that only the latter intervention resulted in improvement in measures of proximal aortic stiffness in older adults with obesity (25•). These data are of relevance as they demonstrate that moderate, but not high-intensity CR in combination with aerobic exercise induces improvements in aortic stiffness, hence may reduce cardiovascular risk. Therefore, aerobic exercise may be prescribed together with moderate CR in older adults with obesity to achieve improvement in aortic stiffness.
4. Cognitive function
Aging is associated with a reduction in cognitive function and increased risk of dementia (9). Based on a recent study conducted on 108 older adults with obesity, frailty was demonstrated to be the strongest predictor of cognitive function, followed by sex and truncal fat mass (26). Interventions able to improve frailty may hence not only lower the cardiometabolic and disability risks but also improve cognitive function. Biological age can predict mortality risk and associated differences in cognitive and physical function in older adults. In frail, older adults with obesity, CR and CR plus exercise (aerobic and resistance) improved biological age as reflected by improved scores in the Klemera-Doubal and Homeostatic Dysregulation algorithms while CR plus exercise improved biological age as reflected by improved scores in the Healthy Aging Index (27). These findings suggest that CR and CR plus exercise are effective methods of improving biological age, and that biological age may be a valuable method of assessing geroprotective interventions in older adults with obesity.
As the aging- and obesity-related decline in cognitive function are exacerbated by hypogonadism in older men (12), an intervention that concurrently targets all these conditions could significantly reduce the risk of cognitive impairment. In the Lifestyle Intervention and Testosterone Replacement in Obese Seniors (LITROS) trial, the combination of lifestyle therapy (CR plus aerobic and resistance exercise) plus testosterone resulted in greater improvement in cognitive function compared to lifestyle therapy plus placebo (28•). Based on multiple regression analyses, changes in VO2peak, strength, testosterone, and luteinizing hormone were independent predictors of the improvement in global cognition (28•). These findings suggest that in the high-risk population of older men with obesity and hypogonadism, testosterone replacement therapy may improve cognitive function with lifestyle behaviors controlled through lifestyle intervention therapy.
5. Weight Regain
The relapsing nature of obesity makes the identification of successful therapeutic approaches extremely challenging. Although several interventions work in the short term, their long-term effectiveness is difficult to achieve (29). Such phenomenon has been attributed to hormonal adaptations to the energy restricted-weight loss, of which the main features are elevated appetite, desire to eat, and reduced energy expenditure and satiety in response to food ingestion (30). Importantly, a recent study conducted on 80 older women with obesity demonstrated that resistance plus aerobic exercise without CR-induced weight loss resulted in a metabolic adaptation to the mild energy deficit induced by the intervention (31). In another study, Rejeski and colleagues assessed changes in ghrelin and GLP-1 (orexigenic and anorexigenic, respectively) in 177 older adults with obesity and cardiometabolic diseases randomly assigned to weight loss alone, or weight loss plus aerobic or resistance exercise to evaluate the hormonal adaptations to weight loss (32••). Following 6 months of intervention, all groups experienced a significant loss of weight which was accompanied by an increase in circulating ghrelin and a decrease in GLP-1 levels (32••). These hormonal changes were significantly related to the loss of weight at 6 months and accounted for 30.2% of its variance, even though they did not predict weight changes at 18 months (32••). These data suggest that these types of lifestyle intervention may be adequate to counter the physiological pressure responsible for weight regain exerted by ghrelin and GLP-1 hormonal changes in older adults.
Structured exercise provokes little change in the overall daily energy expenditure as people, especially older adults, tend to decrease activities of daily living as a compensatory strategy. Fanning and colleagues studied the effect of CR plus aerobic exercise (EX), or increased daily active time (AT), or both on short-term and long-term weight loss in 183 older adults with obesity (33••). Because of the COVID-19 pandemic, analyses were limited to 112 completers of 120 randomized in the first four waves. All groups lost ~10% of their weight over 6 months (intensive phase), while over the 12-month follow-up period, the CR + AT group regained less weight than the CR + EX group, even though differences with the CR+AT+EX group were not detected (33••). These data provide preliminary evidence that a CR intervention that includes educational sessions directed at increasing daily movement activities could help in minimizing weight regain.
6. Conclusions
This evidence emphasizes the importance of prescribing CR in combination with both resistance and aerobic exercise among older adults with obesity (14–17). CR is in fact necessary to achieve a significant reduction in fat mass content, while exercise is crucial to improve frailty outcomes and prevent the CR-induced reduction in muscle and bone mass. Specifically, resistance exercise is needed to improve the MPS response to anabolic stimuli and to prevent muscle and bone reduction, while aerobic exercise is critical to improve VO2peak, skeletal muscle mitochondrial function, cardiometabolic, and cognitive outcomes (Figure 1). Such comprehensive lifestyle intervention can thus be considered an effective strategy to mitigate the physical, metabolic, and cognitive complications associated with obesity and aging, with the overarching goal to maintain the older adult’s functional independence and quality of life (Figure 1). Importantly, increasing the amount of daily active time may be a useful strategy to help reduce weight regain after CR. Healthcare providers should therefore consider prescribing both exercise types during CR to offset sarcopenic obesity, a health care challenge affecting an increasing proportion of older adults.
Figure 1.
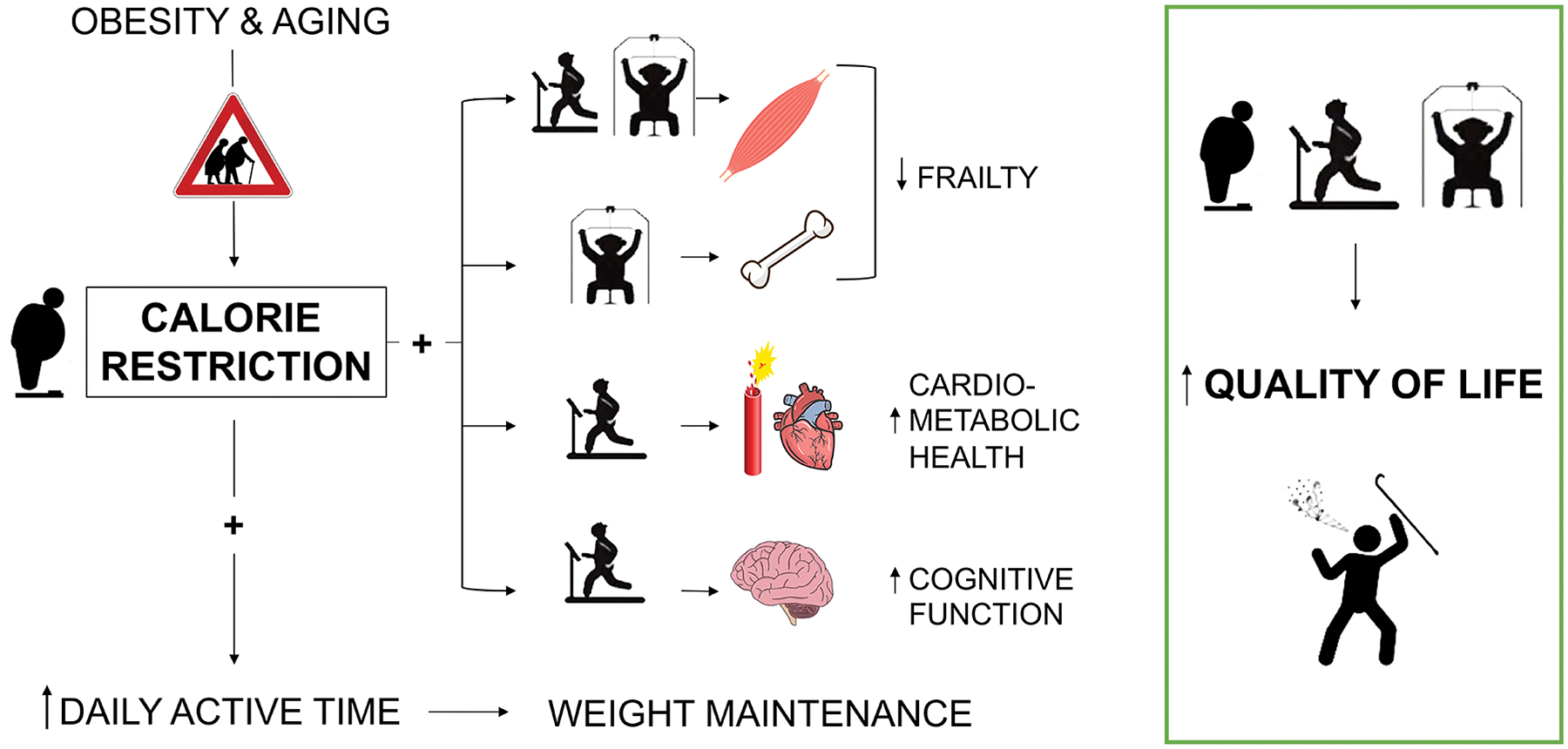
Obesity worsens the age-related decline in physical function and causes frailty in older adults. Calorie restriction in combination with aerobic and resistance exercise ameliorates frailty and improves quality of life in older adults with obesity. Specifically, resistance exercise prevents the bone and muscle mass loss induced by weight reduction, while aerobic exercise promotes improvement in cardiometabolic health and cognitive function. The combination of aerobic and resistance exercise improves myocellular quality more than either exercise type alone. An increase in the daily active time in combination with calorie restriction may be a strategy for promoting weight maintenance.
Key points.
Calorie restriction in combination with resistance and aerobic exercise improves outcomes of frailty and myocellular quality in older adults with obesity.
Resistance exercise attenuates the calorie restriction-induced reduction of muscle and bone mass and improves the muscle protein synthesis response to anabolic stimuli.
Calorie restriction plus aerobic exercise improves cardiovascular and cognitive function in older adults with obesity.
Calorie restriction should be prescribed among older adults with obesity and frailty only in conjunction with aerobic and resistance exercise.
Financial support and sponsorship:
This work was supported by the National Institutes of Health (R01-AG031176, RO1-DK109950) and the US Department of Veterans Affairs (101 CX00906 and CX002161). The contents do not represent the view of the United States Government or the US Department of Veterans Affairs.
Footnotes
Conflict of interest: Authors have nothing to disclose.
References
- 1.Nations U. World Population Prospects: The 2017 Revisions, Key Findings and Advance Tables. Working Paper No ESA/P/WP/248. 2017.
- 2.Flegal KM, Kruszon-Moran D, Carroll MD, et al. Trends in Obesity Among Adults in the United States, 2005 to 2014. JAMA. 2016;315(21):2284–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Galicia Ernst I, Torbahn G, Schwingshackl L, et al. Outcomes addressed in randomized controlled lifestyle intervention trials in community-dwelling older people with (sarcopenic) obesity-An evidence map. Obes Rev. 2022:e13497. [DOI] [PubMed] [Google Scholar]
- 4.Colleluori G, Villareal DT. Aging, obesity, sarcopenia and the effect of diet and exercise intervention. Exp Gerontol. 2021;155:111561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gielen E, Beckwee D, Delaere A, et al. Nutritional interventions to improve muscle mass, muscle strength, and physical performance in older people: an umbrella review of systematic reviews and meta-analyses. Nutr Rev. 2021;79(2):121–47. [DOI] [PubMed] [Google Scholar]
- 6.Donini LM, Busetto L, Bischoff SC, et al. Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO consensus statement. Clin Nutr. 2022. [DOI] [PubMed] [Google Scholar]
- 7.Morgan PT, Smeuninx B, Breen L. Exploring the Impact of Obesity on Skeletal Muscle Function in Older Age. Front Nutr. 2020;7:569904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Colleluori G, Perugini J, Giordano A, et al. From Obesity to Diabetes: The Role of the Adipose Organ. Handb Exp Pharmacol. 2022. [DOI] [PubMed] [Google Scholar]
- 9.Gonzales MM, Garbarino VR, Pollet E, et al. Biological aging processes underlying cognitive decline and neurodegenerative disease. J Clin Invest. 2022;132(10). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Villareal DT, Chode S, Parimi N, et al. Weight loss, exercise, or both and physical function in obese older adults. N Engl J Med. 2011;364(13):1218–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Barnouin Y, Armamento-Villareal R, Celli A, et al. Testosterone Replacement Therapy Added to Intensive Lifestyle Intervention in Older Men With Obesity and Hypogonadism. J Clin Endocrinol Metab. 2021;106(3):e1096–e110. [DOI] [PubMed] [Google Scholar]; • This randomized double-blind, placebo-controlled trial comparing the effect of 6 months lifestyle therapy (diet-induced weight loss and exercise) plus testosterone therapy or placebo in hypogonadal older adults with frailty. Testosterone therapy did not improve more outcomes of frailty compared to placebo, even though it caused a better preservation of muscle mass and hip bone mineral density.
- 12.Aceves-Martins M, Quinton R, Brazzelli M, et al. Identifying the outcomes important to men with hypogonadism: A qualitative evidence synthesis. Andrology. 2022;10(4):625–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Izquierdo M, Merchant RA, Morley JE, et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J Nutr Health Aging. 2021;25(7):824–53. [DOI] [PubMed] [Google Scholar]
- 14.Villareal DT, Aguirre L, Gurney AB, et al. Aerobic or Resistance Exercise, or Both, in Dieting Obese Older Adults. N Engl J Med. 2017;376(20):1943–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Armamento-Villareal R, Aguirre L, Waters DL, et al. Effect of Aerobic or Resistance Exercise, or Both, on Bone Mineral Density and Bone Metabolism in Obese Older Adults While Dieting: A Randomized Controlled Trial. J Bone Miner Res. 2020;35(3):430–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Waters DL, Aguirre L, Gurney B, et al. Effect of Aerobic or Resistance Exercise, or Both, on Intermuscular and Visceral Fat and Physical and Metabolic Function in Older Adults With Obesity While Dieting. J Gerontol A Biol Sci Med Sci. 2022;77(1):131–9. [DOI] [PMC free article] [PubMed] [Google Scholar]; •This randomized controlled trial is the first head-to-head comparison of different exercise types added to matched calorie restriction-induced weight loss investigating metabolic outcomes and ectopic fat deposition in older adults with obesity and frailty. The results showed that among the methods tested, weight loss and combined aerobic and resistance exercise was the most effective in improving ectopic fat deposition and insulin sensitivity.
- 17.Colleluori G, Aguirre L, Phadnis U, et al. Aerobic Plus Resistance Exercise in Obese Older Adults Improves Muscle Protein Synthesis and Preserves Myocellular Quality Despite Weight Loss. Cell Metab. 2019;30(2):261–73 e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cartee GD, Hepple RT, Bamman MM, et al. Exercise Promotes Healthy Aging of Skeletal Muscle. Cell Metab. 2016;23(6):1034–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Volpi E, Mittendorfer B, Rasmussen BB, et al. The response of muscle protein anabolism to combined hyperaminoacidemia and glucose-induced hyperinsulinemia is impaired in the elderly. J Clin Endocrinol Metab. 2000;85(12):4481–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Beavers KM, Neiberg RH, Kritchevsky SB, et al. Association of Sex or Race With the Effect of Weight Loss on Physical Function: A Secondary Analysis of 8 Randomized Clinical Trials. JAMA Netw Open. 2020;3(8):e2014631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.American Diabetes Association. Obesity Management for the Treatment of Type 2 Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S100–S10. [DOI] [PubMed] [Google Scholar]
- 22.American Diabetes Association Professional Practice C. Summary of Revisions: Standards of Medical Care in Diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S4–S7. [DOI] [PubMed] [Google Scholar]
- 23.Celli A, Barnouin Y, Jiang B, et al. Lifestyle Intervention Strategy to Treat Diabetes in Older Adults: A Randomized Controlled Trial. Diabetes Care. 2022;45(9):1943–52. [DOI] [PMC free article] [PubMed] [Google Scholar]; •This is the first randomized controlled trial investigating the effect of an intensive lifestyle therapy compared to a healthy lifestyle education on metabolic and physical function specifically in older adults with diabetes and comorbidities. The intensive lifestyle therapy was more effective in improving HbA1c, insulin sensitivity, body composition and outcomes of frailty. This evidence support the adoption of a lifestyle intervention strategy to improve metabolic and functional health of older adults with diabetes.
- 24.Vatner SF, Zhang J, Vyzas C, et al. Vascular Stiffness in Aging and Disease. Front Physiol. 2021;12:762437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Brinkley TE, Leng I, Bailey MJ, et al. Effects of Exercise and Weight Loss on Proximal Aortic Stiffness in Older Adults With Obesity. Circulation. 2021;144(9):684–93. [DOI] [PMC free article] [PubMed] [Google Scholar]; • Randomized controlled trial comparing the effect of aerobic exercise alone or in combination with high-intensity or with moderate calorie restriction on proximal aortic stiffness il older adults with obesity. The study shows that only aerobic exercise plus moderate calorie restriction resulted in improvements in measures of proximal aortic stiffens.
- 26.Heisey HD, Kunik ME, Qualls C, et al. Truncal Fat and Frailty Are Important Predictors of Cognitive Performance among Aging Adults with Obesity. J Nutr Health Aging. 2022;26(5):425–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ho E, Qualls C, Villareal DT. Effect of Diet, Exercise, or Both on Biological Age and Healthy Aging in Older Adults with Obesity: Secondary Analysis of a Randomized Controlled Trial. J Nutr Health Aging. 2022;26(6):552–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gregori G, Celli A, Barnouin Y, et al. Cognitive response to testosterone replacement added to intensive lifestyle intervention in older men with obesity and hypogonadism: prespecified secondary analyses of a randomized clinical trial. Am J Clin Nutr. 2021;114(5):1590–9. [DOI] [PMC free article] [PubMed] [Google Scholar]; •This randomized double-blind, placebo-controlled trial comparing the effect of 6 months lifestyle therapy (diet-induced weight loss and exercise) plus testosterone therapy or placebo in hypogonadal older adults with frailty. Lifestyle intervention in combination with testosterone therapy improved more cognitive function compared to placebo.
- 29.Muller TD, Bluher M, Tschop MH, et al. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov. 2022;21(3):201–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hall KD. Energy compensation and metabolic adaptation: “The Biggest Loser” study reinterpreted. Obesity (Silver Spring). 2022;30(1):11–3. [DOI] [PubMed] [Google Scholar]
- 31.Martins C, Gower B, Hunter GR. Metabolic adaptation after combined resistance and aerobic exercise training in older women. Obesity (Silver Spring). 2022;30(7):1453–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rejeski JJ, Fanning J, Nicklas BJ, et al. Six-month changes in ghrelin and glucagon-like peptide-1 with weight loss are unrelated to long-term weight regain in obese older adults. Int J Obes (Lond). 2021;45(4):888–94. [DOI] [PMC free article] [PubMed] [Google Scholar]; •• Randomized controlled trial investigating the effect of weight loss alone or in combination with aerobic and resistance exercise on the hormonal adaptation to weight loss in older adults with obesity and cardiometabolic diseases. Changes in circulating GLP-1 and ghrelin did not predict weight regain from 6 to 18 months.
- 33.Fanning J, Rejeski WJ, Leng I, et al. Intervening on exercise and daylong movement for weight loss maintenance in older adults: A randomized, clinical trial. Obesity (Silver Spring). 2022;30(1):85–95. [DOI] [PMC free article] [PubMed] [Google Scholar]; •• Randomized control trial investigating the effect of calorie restrcition plus aerobic exercise or increased daily active time or both on short-term and long-term weight loss in older adults with obesity. All interventions lead to a ~10% weight loss at 6 months, while calorie restriction and increased daily active time led to a lower weight regain at 12 months. Calorie restriction intervention should include educational session oriented at promoting the increase in active time to ensure long-term weight maintenance.