

Abstract
Objective
To investigate the association between oral health management (OHM) by dental hygienists and the occurrence of pneumonia, and determine the effectiveness of OHM in pneumonia prevention.
Background
In long‐term care facilities in Japan, the need for professional OHM is increasing with an increase in the number of severely debilitated residents.
Materials and methods
A 1‐year prospective multicentre cohort study was conducted using data from 504 residents (63 men; mean age: 87.4 ± 7.8 years) in Japanese long‐term care facilities. Basic information, medical history, willingness to engage in oral hygiene behaviour, need for OHM and oral conditions were investigated at baseline. In addition, information on the occurrence of pneumonia was collected using a follow‐up survey after one year. A Poisson regression analysis with robust standard errors was conducted, with pneumonia as the dependent variable, and factors associated with OHM and pneumonia occurrence as explanatory variables.
Results
Overall, 349 (69.2%) residents required OHM by dental hygienists during that year of follow‐up. Of those, 238 (68.2%) were provided with OHM, and 18 (7.5%) developed pneumonia. Among the 111 patients (31.8%) who were not provided with OHM, 21 (18.9%) developed pneumonia. The OHM group had lower pneumonia rates than the non‐OHM group (prevalence rate ratio: 0.374; 95% CI: 0.210‐0.665).
Conclusion
Oral health management by dental hygienists was associated with a lower incidence of pneumonia among residents of long‐term care facilities, underlining the importance of professional OHM for such individuals. It is recommended that OHM be practised routinely in long‐term care facilities.
Keywords: dental hygienists, long‐term care, oral health, pneumonia
1. INTRODUCTION
According to the 2018 Japanese government's Vital Statistics, 1 pneumonia and aspiration pneumonia are the third leading causes of death. The aspiration of oral bacteria with saliva or food is the predominant cause of pneumonia in older adult patients. 2 , 3 Yoneyama et al 4 , 5 showed the effectiveness of professional and mechanical oral cleaning by dentists or dental hygienists in the prevention of pneumonia when undertaken in addition to self‐oral cleaning by residents or by caregivers in special nursing homes in Japan. Subsequently, oral health management (OHM) by oral health professionals was included as a service in the long‐term care (LTC) insurance system of Japan, whereby dental hygienists provide dentist‐supervised oral health care for residents of LTC facilities. OHM means that the nurse selects the resident, and the dental hygienist provides oral hygiene (hereafter professional OHM) at least twice a month and instructs the nursing staff for those who have given consent. This service does not include dental visits for dental treatment.
Since the study by Yoneyama et al 4 , 5 was conducted approximately 20 years ago, the necessity for oral healthcare (OHC) provision is more crucial than before because of the increased number of older residents in LTC facilities, high demand for nursing care, 6 greater number of older adult patients with dementia, 7 and most notably, more teeth present in older individuals 8 , 9 than was observed 20 years ago. However, there have been no large‐scale reports in Japan since the report by Yoneyama et al 4 , 5 in 2002. Therefore, there is limited available information on the current status of professional OHM and its effects on the incidence reduction in pneumonia in residents at LTC facilities.
Accordingly, we conducted a 1‐year longitudinal multicentre study in Japanese LTC facilities to test the hypothesis that professional OHM by dental hygienists is associated with a lower incidence of pneumonia among residents of Japanese LTC insurance facilities, in which the number of older adults with many teeth and severe health care needs has increased.
2. MATERIALS AND METHODS
Thirty members of the Special Committee of the Japanese Society of Gerodontology conducted a workshop to discuss the concept of the prospective cohort study and define the evaluation criteria for the contents of the survey. The facilities to be surveyed were LTC insurance facilities throughout Japan, which were visited by the Special Committee members of the Japanese Society of Gerodontology. The directors and staff of the LTC facilities were briefed about the study, and permission for study participation was obtained from the directors of 37 facilities situated throughout Japan. A baseline survey was conducted between October 2018 and February 2019. One year after the baseline survey, permission to conduct a follow‐up survey was obtained from the directors of 22 of the 37 facilities. Individuals receiving parenteral feeding and those who did not require professional OHM at the time of the baseline survey were excluded from this study.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Japanese Society of Gerodontology (approval numbers 2018‐1 and 2019‐3). Written informed consent for participation in the follow‐up survey was obtained from participants or their proxies.
2.1. Baseline surveys
2.1.1. Questionnaire administration
Data on age, sex, body mass index (BMI), medical history (pneumonia, including aspiration pneumonia, stroke, diabetes mellitus and respiratory disease (chronic obstructive pulmonary disease, asthma and other)), willingness to engage in oral hygiene behaviours and the provision of professional OHM by dental hygienists were obtained with the help of the facility staff using a structured questionnaire. Professional OHM by dental hygienists was indicated if the facility staff could not maintain optimal oral health of the residents. A facility nurse determined the need for dental hygienist‐delivered professional OHM for residents based on the oral hygiene management manual published by the Japanese Society of Gerodontology. Ultimately, professional OHM was provided by a dental hygienist if the individual or family consented to the procedure. Activities of Daily Living were assessed by a facility nurse using the Barthel Index (BI). 10 Cognitive impairment was assessed by a trained specialist using the Clinical Dementia Rating (CDR) scale. 11
2.1.2. Assessment of oral conditions
The number of dentists and dental hygienists who visited each facility to conduct assessments varied according to the size of the facility. In total, 50 dentists and dental hygienist conducted assessments, ranging from three to ten per facility. They were trained in the evaluation criteria and had no prior knowledge of the participants’ existing oral health status. During the survey, at least one researcher with survey experience always participated, to confirm that the standards were consistent. The dentists and dental hygienists who conducted the actual survey were not informed about the availability of oral health care for the residents. Only mouth mirrors and headlights were used to assess the oral conditions. The number of teeth present was defined as the number of erupted teeth in the oral cavity, and those who had no teeth present were defined as edentulous. Residents who used a denture during meals were defined as prosthesis users.
The Oral Health Assessment Tool (OHAT) is a convenient oral screening tool for nurses and nursing staff to assess oral problems in people with disabilities and those in need of care. 12 This study used the Japanese version of the OHAT (OHAT‐J), which has been evaluated for reliability and validity. 13 The OHAT‐J was administered by a dentist. In addition, the Tongue Coating Index (TCI), which assesses oral health status by the degree of attachment of the tongue coat based on a visual inspection, 14 was used. Oral function was assessed using oral diadochokinesis, modified water swallow test and repetitive saliva swallowing test.
2.2. Follow‐up questionnaire
Information on pertinent events during the observation period was obtained from the staff of each facility. These events included the incidence of pneumonia, hospitalisations (and causes), discharge from the facility and death.
2.3. Statistical analysis
Descriptive characteristics of the study participants (Table 1) were compared according to their need for professional OHM. Based on the necessity for professional OHM as determined by the nurse, and consent provision by the participants or their families, participants requiring professional OHM were stratified into two groups (those not requiring oral hygiene management and those requiring oral hygiene management). Professional OHM was provided by a dental hygienist. Intergroup comparisons of the participant characteristics were conducted. Student's t test was used to assess differences in normally distributed continuous data, while the Mann‐Whitney U test was used for non‐normally distributed continuous data. Cross tabulations and chi‐squared tests were used for categorical variables.
TABLE 1.
Characteristics of study participants according to the requirement for oral health management
| Variables | Overall (N = 504) | No requirements for oral hygiene management(N = 155) | With requirements for oral hygiene management(N = 349) | P‐value | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD/N (%) | Median, [Q1, Q3] | Mean ± SD/N (%) | Median, [Q1, Q3] | Mean ± SD/N (%) | Median, [Q1, Q3] | ||
| Age, years | 87.4 ± 7.8 | 88.0 [83.0, 93.0] | 86.4 ± 7.6 | 87.0 [82.0, 92.0] | 87.8 ± 7.9 | 88.0 [83.0, 93.5] | .059 |
| Sex (female) | 441 (81.5) | 124 (80.0) | 287 (82.2) | .537 | |||
| Barthel Index | 31.7 ± 26.0 | 30.0 [5.0, 50.0] | 39.1 ± 27.7 | 40.0 [10.0, 60.0] | 28.4 ± 24.6 | 25.0 [5.0, 45.0] | <.001 |
| Body mass index | 20.5 ± 3.6 | 20.1 [17.8, 22.7] | 21.1 ± 4.1 | 20.9 [17.7, 23.6] | 20.2 ± 3.4 | 19.9 [17.9, 22.3] | .009 |
| Clinical dementia rating | |||||||
| 0, 0.5 | 49 (9.9) | 20 (12.9) | 29 (8.5) | .190 | |||
| 1 | 89 (17.9) | 33 (21.3) | 56 (16.4) | ||||
| 2 | 131 (26.4) | 37 (23.9) | 94 (27.6) | ||||
| 3 | 227 (45.8) | 65 (41.9) | 162 (47.5) | ||||
| Onset of pneumonia/1 year, N (%) | 61 (12.1) | 22 (14.2) | 39 (11.2) | .375 | |||
| Oral conditions | |||||||
| Willingness for oral hygiene, N (%) | 267 (53.2) | 96 (62.3) | 171 (49.0) | .007 | |||
| Oral Health Assessment Tool‐J Score | 2.9 ± 2.2 | 2.0 [1.0, 4.0] | 3.1 ± 2.0 | 3.0 [1.0, 4.0] | 2.8 ± 2.3 | 2.0 [1.0, 4.0] | .04 |
| Tongue Coating Index | 20.9 ± 22.6 | 11.1 [0.0, 33.3] | 21.1 ± 22.6 | 16.7 [0.0, 33.3] | 20.8 ± 22.6 | 11.1 [0.0, 33.3] | .8 |
| Number of teeth present | 9.9 ± 9.4 | 7.5 [0.0, 18.0] | 11.0 ± 9.5 | 9.0 [0.0, 20.0] | 9.4 ± 8.9 | 7.0 [0.0, 17.0] | .136 |
| Edentulous, N (%) | 171 (34.2) | 45 (29.4) | 126 (36.3) | .152 | |||
| Prosthesis use, N (%) | 265 (52.6) | 84 (54.2) | 181 (51.9) | .699 | |||
| Medical history | |||||||
| Stroke, N (%) | 190 (37.8) | 55 (35.5) | 135 (38.7) | .561 | |||
| Diabetes mellitus, N (%) | 82 (16.3) | 23 (14.8) | 59 (16.9) | .694 | |||
| Respiratory disease a , N (%) | 75 (14.9) | 19 (12.4) | 56 (16.0) | .342 | |||
P < .05 was considered statistically significant. Q1, first quartile; Q3, third quartile; SD, standard deviation.
Respiratory disease: chronic obstructive pulmonary disease, asthma, other (without pneumonia)
To investigate the factors associated with pneumonia incidence among study participants, the characteristics of the study groups were compared based on whether they had had pneumonia during the follow‐up period. A multivariable Poisson regression analysis with robust standard errors was used to estimate the relative risk (RR) of having pneumonia during that period. The main exposure variable was professional OHM provision. Models were adjusted for variables reported to be associated with pneumonia, including age, sex, BI, BMI, CDR, stroke, diabetes and respiratory disease. To examine the possibility of multicollinearity, correlations between each factor were checked. As we collected data from multiple institutions, we conducted a likelihood ratio test comparing the multilevel model with a single‐level model containing the same predictors. As logistic regression might have overestimated the risk of association in a high incidence of outcomes, 15 a Poisson regression model with robust standard errors was used. 16 Statistical analyses used Stata version 16.1 (StataCorp, College Station) and SPSS Statistics version 26 (IBM), with the significance level set at P < .05.
3. RESULTS
Of 889 residents in 37 facilities surveyed at baseline, 525 from 22 facilities (59.1%) participated in this follow‐up study (Figure 1). Twenty‐one residents who required parenteral feeding and 155 who did not require OHM were excluded from the analysis dataset. The final analysis dataset included data from 349 individuals (82.2% women, mean age: 87.8 ± 7.9 years) who required professional OHM. Eighteen (7.5%) participants of the 238 (68.2%) who were provided professional OHM developed pneumonia, and of the 111 participants who were not provided with professional OHM, 21 (18.9%) developed pneumonia. In addition, of the 155 participants who did not require professional OHM, 22 (14.2%) developed pneumonia.
FIGURE 1.
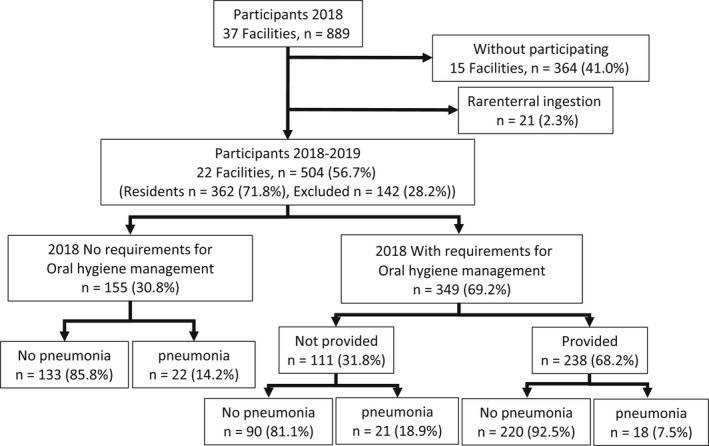
Flow chart of study participants. A baseline survey of 889 residents of long‐term care insurance facilities was conducted. For follow‐up, 525 (59.0%) residents gave consent to participate. Of these, 21 (2.3%) participants receiving parenteral feeding at the time of the baseline survey were excluded. The remaining 504 (56.7%) participants were divided into groups based on their need for oral health management (OHM) by a dental hygienist. Of the 349 (69.2%) residents who needed OHM by a dental hygienist, 238 (68.2%) were provided the service, and 111(31.8%) were not provided the service. Among the 238 residents who were provided OHM by a dental hygienist, 18 (7.5%) residents had pneumonia, and 220 (92.5%) residents did not during that year. Among the 111 residents who did not receive OHM by a dental hygienist, 21 (18.9%) residents had pneumonia, and 90 (81.1%) residents did not during that year
Table 1 lists the baseline characteristics of the study participants. The group that required professional OHM had a significantly lower BI score, BMI, proportion of participants willing to engage in oral hygiene care and OHAT‐J scores than the participants in the group that did not require professional OHM.
Table 2 shows that 111 (31.8%) of the 349 residents were considered by the nurses to require OHM, but were not provided with professional OHM because they could not give consent. The participants who received professional OHM had significantly lower rates of pneumonia and a lower TCI over the 1‐year follow‐up period than those who did not receive professional OHM.
TABLE 2.
Intragroup comparison by the requirement of oral health management according to the provision of oral health management
| Variables | With requirements for oral hygiene management (N = 349) | P‐value | |||
|---|---|---|---|---|---|
| Not provided (N = 111) | Provided (N = 238) | ||||
| Mean ± SD/N (%) | Median, [Q1, Q3] | Mean ± SD/N (%) | Median [Q1, Q3] | ||
| Age, years | 88.7 ± 7.5 | 89.0 [85.0, 94.0] | 87.4 ± 8.0 | 88.0 [82.0, 93.0] | .135 |
| Sex (female), N (%) | 92 (82.9) | 195 (81.9) | .881 | ||
| Barthel Index | 29.4 ± 28.1 | 20.0 [5.0, 50.0] | 28.0 ± 22.9 | 25.0 [5.0, 45.0] | .927 |
| Body mass index | 20.4 ± 3.1 | 20.2 [18.1, 22.4] | 20.2 ± 3.5 | 19.8 [17.8, 22.3] | .628 |
| Clinical dementia rating | 2.2 ± 0.8 | 2.0 [2.0, 3.0] | 2.1 ± 0.9 | 2.0 [1.0, 3.0] | .537 |
| 0, 0.5 | 4 (3.9) | 25 (10.5) | |||
| 1 | 20 (19.4) | 36 (15.1) | .207 | ||
| 2 | 29 (28.2) | 65 (27.3) | |||
| 3 | 50 (48.5) | 112 (47.1) | |||
| Onset of pneumonia/1 year, N (%) | 21 (18.9) | 18 (7.6) | .003 | ||
| Oral conditions | |||||
| Willingness for oral hygiene, N (%) | 59 (53.2) | 112 (47.1) | .303 | ||
| Oral Health Assessment Tool‐J Score | 2.8 ± 2.2 | 2.0 [1.0, 4.0] | 2.8 ± 2.4 | 2.0 [1.0, 4.0] | .547 |
| Tongue Coating Index | 27 ± 25.4 | 22.2 [0.0, 44.4] | 17.9 ± 20.6 | 11.1 [0.0, 27.8] | .002 |
| Number of teeth present | 7.6 ± 9.0 | 3.0 [0.0, 14.5] | 7.9 ± 8.9 | 5.0 [0.0, 14.5] | .791 |
| Edentulous, N (%) | 39 (35.5) | 87 (36.7) | .905 | ||
| Prosthesis use, N (%) | 57 (51.4) | 124 (52.1) | .909 | ||
| Medical history | |||||
| Stroke, N (%) | 39 (35.1) | 96 (40.3) | .409 | ||
| Diabetes mellitus, N (%) | 14 (12.6) | 45 (18.9) | .168 | ||
| Respiratory disease a , N (%) | 17 (15.3) | 39 (16.4) | .876 | ||
Q1, first quartile; Q3, third quartile; SD, standard deviation.
Respiratory disease: chronic obstructive pulmonary disease, asthma, other (without pneumonia).
Table 3 shows that among the 349 participants who required professional OHM, 39 (11.2%) had pneumonia during the follow‐up period. Moreover, the participants who had pneumonia had a significantly lower BI, were less likely to receive professional OHM and had a higher TCI than the residents who did not have pneumonia.
TABLE 3.
Intragroup comparison by the requirement for oral health management according to the occurrence of pneumonia
| Variable | With requirements for oral hygiene management (N = 349) | ||||
|---|---|---|---|---|---|
| Non‐pneumonia (N = 310) | Pneumonia (N = 39) | P‐value | |||
| Mean ± SD/N (%) | Median, [Q1, Q3] | Mean ± SD/N (%) | Median [Q1, Q3] | ||
| Age, years | 87.8 ± 8.1 | 88.0 [83.0, 93.3] | 88.1 ± 6.5 | 87.0 [84.0, 94.0] | .801 |
| Sex (female), N (%) | 258 (83.2) | 29 (74.4) | .184 | ||
| Barthel Index | 29.3 ± 24.6 | 50.0 [25.0, 45.0] | 21.5 ± 23.9 | 10.0 [0.0, 40.0] | 0.035 |
| Body mass index | 20.3 ± 3.4 | 19.9 [18.0, 22.3] | 19.7 ± 2.9 | 19.5 [17.2, 21.6] | .346 |
| Clinical dementia rating | 2.2 ± 0.9 | 2.0 [1.0, 3.0] | 2.3 ± 0.9 | 3.0 [1.8, 3.0] | .304 |
| 0, 0.5 | 26 (8.6) | 3 (7.9) | .513 | ||
| 1 | 50 (16.5) | 6 (15.8) | |||
| 2 | 87 (28.7) | 7 (18.4) | |||
| 3 | 140 (46.2) | 22 (57.9) | |||
| Oral conditions | |||||
| Oral hygiene management, N (%) | 220 (71.0) | 18 (46.2) | .003 | ||
| Willingness for oral hygiene, N (%) | 149 (48.1) | 22 (56.4) | .671 | ||
| Oral Health Assessment Tool‐J Score | 2.8 ± 2.3 | 2.0 [1.0, 4.0] | 2.7 ± 2.3 | 2.0 [1.0, 4.0] | .547 |
| Tongue Coating Index | 20.1±22.5 | 11.1 [0.0, 33.3] | 26.4±22.3 | 22.2 [5.6, 50.0] | .002 |
| Number of teeth present | 8.7 ± 9.1 | 6.0 [0.0, 17.0] | 9.8 ± 9.3 | 7.0 [0.0, 17.5] | .297 |
| Edentulous, N (%) | 117 (38.0) | 9 (23.1) | .078 | ||
| Prosthesis use, N (%) | 165 (53.2) | 16 (41.0) | .671 | ||
| Medical history | |||||
| Stroke, N (%) | 122 (39.4) | 13 (33.3) | .492 | ||
| Diabetes mellitus, N (%) | 56 (18.1) | 3 (7.7) | .117 | ||
| Respiratory disease a , N (%) | 51 (16.5) | 5 (12.8) | .651 | ||
P < .05 was considered statistically significant. Q1, first quartile; Q3, third quartile; SD, standard deviation.
Respiratory disease: chronic obstructive pulmonary disease, asthma, other (without pneumonia)
Table 4 shows the outcome of the Poisson regression analysis used to assess the association between pneumonia incidence and professional OHM. The likelihood ratio test results comparing the multilevel model against a single‐level model that contained the same predictors were not significant (P = .18); therefore, we used the single‐level model. Provision of professional OHM resulted in significantly lower RR for pneumonia incidence (0.37, 95% CI: 0.21‐0.67). In addition, the number of teeth present was associated with pneumonia incidence (RR: 1.05, 95% CI: 1.01‐1.08). There was no correlation of r ≥ 0.6 between the factors.
TABLE 4.
Effect of oral hygiene management on incident pneumonia in Poisson regression analysis with robust standard errors
| RR | 95% CI | P‐value | |
|---|---|---|---|
| Age | 1.012 | 0.972 ‐ 1.053 | .569 |
| Sex (0: male, 1: female) | 0.674 | 0.358 ‐ 1.270 | .223 |
| Barthel Index | 0.988 | 0.973 ‐ 1.003 | .120 |
| Body mass index | 0.955 | 0.861‐ 1.059 | .383 |
| Clinical dementia rating | |||
| 0, 0.5 | Reference | ||
| 1 | 0.704 | 0.206‐2.401 | .575 |
| 2 | 0.516 | 0.137‐1.942 | .328 |
| 3 | 0.604 | 0.183‐1.988 | .406 |
| Diabetes mellitus (0: no, 1: yes) | 0.451 | 0.148‐1.370 | .160 |
| Number of teeth present | 1.045 | 1.012‐1.079 | .007 |
| Oral hygiene management (0: no, 1: yes) | 0.374 | 0.210‐0.665 | .001 |
Abbreviations: CI, confidence interval; RR, relative risk.
4. DISCUSSION
This study investigated the general and oral conditions, and provision of professional OHM, among residents of LTC facilities in Japan to examine the association between professional OHM and the incidence of pneumonia, and investigate the effectiveness of professional OHM provided by dental hygienists in preventing pneumonia. The incidence of pneumonia was significantly lower in residents who had received professional OHM than in those who had not.
Based on the effectiveness and current status of oral care, 17 , 18 , 19 , 20 the Japanese LTC insurance system accepted dental professional OHM as a nursing care service in 2009. Subsequently, the content of this nursing care service was revised in 2018 to provide direct professional OHM at least twice a month to residents of LTC facilities and provide support for daily oral care, such as specific technical advice and guidance to the nursing staff. Thus, under the professional OHM service outlined by the Japanese LTC insurance system, dental hygienists need to perform direct professional OHM and promote the provision of professional OHM by LTC facility staff. However, this is the first study to evaluate the implementation and efficacy of these guidelines.
An interventional study by Yoneyama et al 4 , 5 verified the efficacy of oral care in preventing pneumonia. Since then, nurses and caregivers have widely provided oral care to patients in LTC facilities. As it is ethically challenging to conduct new interventional studies on oral care practices in such settings, this research was conducted as an observational study.
In a similar study conducted 20 years ago, the participants had fewer teeth present than the participants in our study, and they were younger and performed more ADLs. 3 , 4 , 21 However, the participants in our study were similar to Japanese LTC residents in the last 10 years, in terms of their ADLs, incidence of dementia, number of teeth present and incidence of pneumonia. 22 , 23 , 24 The nursing care requirements of individuals in LTC facilities in Japan are increasing, the implementation of oral care is more difficult, and there is a higher risk of pneumonia. In contrast with previous studies with LTC facilities in Japan, 25 the incidence of pneumonia was lower in this study. Thus, considering residents' current status, the care provided for pneumonia prevention appears to be improving. However, expected changes in oral health, caused by factors such as an increase in the number of teeth and the number of people unwilling to receive or perform their oral hygiene due to the greater number of people with severe dementia, indicate that the provision of professional OHM must be increased among LTC residents. As indicated by the findings of our study, it is necessary to identify individuals who require professional OHM so as to intervene appropriately to prevent pneumonia from occurring in LTC facilities. Efforts should be made to ensure measures to prevent dental caries and periodontal diseases, and promote professional OHM, for such individuals are taken.
Study participants who required professional OHM were older, had higher professional OHM intervention rates, and lower OHAT‐J and TCI scores than those who did not require professional OHM. In addition, just over two‐thirds of the residents who required professional OHM had already undergone professional OHM by a dental hygienist, which is likely to have resulted in their lower OHAT and TCI scores. Participants who required professional OHM also had a lower BI, BMI and willingness to receive or perform their oral hygiene than the group that did not require professional OHM. Thus, the need for professional OHM by dental hygienists was assessed by nurses, suggesting that this assessment was generally accurate. We also wanted to examine the association between OHAT (which is often used by non‐dental professionals in the assessment of the oral cavity) and pneumonia, as well as to identify oral risk factors for pneumonia. However, no association was found between OHAT and pneumonia incidence; therefore, screening for pneumonia risk needs further investigation.
There was no difference in the general characteristics (BI, BMI, CDR, etc) of the participants who did or did not receive professional OHM. However, the incidence of pneumonia among patients who received professional OHM was significantly lower, as was the TCI, used to evaluate oral hygiene status. An association between bacterial counts on the tongue and pneumonia has been reported previously, 26 and one of our previous studies found that oral care reduces the bacterial count on the tongue. 27 In this study, we observed that participants who received professional OHM potentially had lower oral bacterial counts (indicated by a lower TCI), which may have resulted in the reduced incidence of pneumonia. Furthermore, we hypothesise that the development of the tongue coat is associated with a reduction in oral function, 28 and that the approach to oral function is an important factor in oral health. Professional OHM includes not only oral care aimed at removing oral deposits with an emphasis on oral hygiene but also oral care with an emphasis on functional aspects. Therefore, the provision of professional OHM by dental hygienists may have resulted in enhanced oral function and a reduction in the amount of attachment of the tongue coat.
The Japanese nationwide provision rate of professional OHM by nursing care services (8.92% in October 2018) 29 differs greatly from the provision rate identified among the 504 participants in this study (47.2%). This may be because the participating facilities were members of the Japanese Society of Gerodontology. To reduce the impact of this bias, we sought the participation of as many residents as possible and achieved a larger sample size than in previous studies. Furthermore, although the participants were comparable to residents of a typical LTC insurance facility, the results of this study should be interpreted with caution.
Unlike other smaller studies, this study collected data (including oral examination data) from more than 500 of older adult LTC residents from 22 LTC facilities across 14 regions in Japan. In multicentre studies, differences in institutional policies and staff awareness can be a source of bias. However, the results of this study may have been less affected by this bias, as the findings of likelihood ratio tests comparing single‐level models, which included the same predictors as multilevel models, were not significant.
It should be noted that the results do not include data from all residents of the 22 LTC facilities. Residents who did not consent to participate or were at high risk for aspiration pneumonia were excluded. Residents who required parenteral feeding were also excluded on the basis that the need for professional OHM for this group is primarily to manage their oral hygiene rather than maintain and improve oral function, and in turn, ability to consume food orally. The main objective of professional OHM for residents receiving parenteral feeding was to manage oral hygiene. However, one of the main objectives of professional OHM for oral consumers is to maintain and improve oral function in order to maintain oral intake. In other words, because of the different purposes of OHM, we excluded residents receiving parenteral feeding from our analyses. Although the relationship between denture wearing during sleep and pneumonia has been reported previously, 30 dentures are generally removed at bedtime in LTC insurance facilities in Japan. As there were no participants who wore dentures in this study, we could not examine the relationship between denture wearing at night and the incidence of pneumonia. Furthermore, the need for professional OHM was determined by the nurse at each facility. This assessment may be influenced by facility environments and staff professional OHM competencies. It is possible that the criteria for determining the need for professional OHM were not consistently applied across all facilities. In the future, we recommend standardisation of the assessment criteria for persons requiring professional OHM. Moreover, the services provided for residents professional OHM are highly individualised, provided according to the conditions of the resident and at the discretion of the dental hygienist who provides the service. To further inform the provision of OHM in LTC facilities, studies with medication data, dental visits, other healthcare and nursing care services related to pneumonia prevention, and the details of services such as the type, time, and frequency of care, are needed.
5. CONCLUSION
Professional OHM for Japanese‐insured LTC residents was associated with a lower incidence of pneumonia. The findings of this study suggest that the provision of professional OHM may help reduce the incidence of pneumonia.
CONFLICT OF INTEREST
The authors declare no conflicts of interest associated with this manuscript.
AUTHOR CONTRIBUTIONS
Yasuyuki Iwasa, Yuki Ohara, Masanori Iwasaki, Kayoko Ito, Junko Nakajima, Takashi Tohara, Mayumi Sakamoto, Masataka Itoda, Ken Inohara, Yoshie Ozaki, Rikimaru Sasaki, Yasuhiro Nishi, Midori Tsuneishi, Junichi Furuya, Yutaka Watanabe, Yoshihiko Watanabe, Yuji Sato and Mitsuyoshi Yoshida were involved in study design and data interpretation. Yasuyuki Iwasa, Yuki Ohara, Masanori Iwasaki, Kayoko Ito, Junko Nakajima, Takae Matsushita and Yutaka Watanabe were involved in data collection and data analysis. All authors critically revised the report, commented on drafts of the manuscript and approved the final report.
ACKNOWLEDGEMENTS
This project was funded by the Japanese Ministry of Health, Labor and Welfare (Geriatric Health Promotion Project). However, the sponsors were not involved in study design, collection, analysis and interpretation of data, writing of the report or in the decision to submit the article for publication.
APPENDIX 1. Characteristics of study participants and comparison between those who required oral hygiene management and other groups
| Variables | Other (N = 540) | With requirements for Oral hygiene management (N = 349) | P‐value | ||
|---|---|---|---|---|---|
| Mean ± SD/N (%) | Median, [Q1, Q3] | Mean ± SD/N (%) | Median, [Q1, Q3] | ||
| Age, years | 86.3 ± 7.8 | 87.0, [82.0, 92.0] | 87.8 ± 7.9 | 88.0, [83.0, 93.5] | .003 |
| Sex (female) | 124 (80.0) | 287 (82.2) | .074 | ||
| Barthel Index | 31.1 ± 27.1 | 30.0, [5.0, 50.0] | 28.4 ± 24.6 | 25.0, [5.0, 45.0] | .336 |
| Body mass index | 20.5 ± 3.7 | 20.3, [17.6, 22.7] | 20.2 ± 3.4 | 19.9, [17.9, 22.3] | .373 |
| Clinical dementia rating | |||||
| 0, 0.5 | 50 (9.4) | 29 (8.5) | .426 | ||
| 1 | 98 (18.4) | 56 (16.4) | |||
| 2 | 130 (24.4) | 94 (27.6) | |||
| 3 | 255 (48.8) | 162 (47.5) | |||
| Oral conditions | |||||
| Oral hygiene management, N (%) | 91 (16.9) | 238 (68.2) | <.001 | ||
| Willingness for oral hygiene, N (%) | 255 (47.3) | 171 (49.0) | .623 | ||
| Oral Health Assessment Tool‐J Score | 3.3 ± 2.3 | 3.0, [2.0, 5.0] | 2.8 ± 2.3 | 2.0, [1.0, 4.0] | <.001 |
| Tongue Coating Index | 25.0 ± 24.3 | 16.7, [0.0, 38.9] | 20.8 ± 22.6 | 11.1, [0.0, 33.3] | .010 |
| Number of teeth present | 10.1 ± 9.4 | 8.0, [0.0, 18.0] | 9.4±8.9 | 7.0, [0.0, 17.0] | .349 |
| Edentulous, N (%) | 176 (33.2) | 126 (36.3) | .344 | ||
| Prosthesis use, N (%) | 257 (48.5) | 181 (51.9) | .252 | ||
| Medical history | |||||
| Stroke, N (%) | 198 (36.9) | 135 (38.7) | .587 | ||
| Diabetes mellitus, N (%) | 94 (17.5) | 59 (16.9) | .818 | ||
| Respiratory disease a , N (%) | 69 (12.9) | 56 (16.0) | .182 | ||
P < .05 was considered statistically significant. Q1, first quartile; Q3, third quartile; SD, standard deviation
Respiratory disease: chronic obstructive pulmonary disease, asthma, other (without pneumonia)
Hama K, Iwasa Y, Ohara Y, et al. Pneumonia incidence and oral health management by dental hygienists in long‐term care facilities: A 1‐year prospective multicentre cohort study. Gerodontology. 2022;39:374–383. 10.1111/ger.12604
DATA AVAILABILITY STATEMENT
Data are available on reasonable request to the corresponding author.
REFERENCES
- 1. Ministry of Health Vital statistics of Japan. 2018. https://www.mhlw.go.jp/english/database/db-hw/dl/81-1a2en.pdf. Accessed May 17, 2020
- 2. Sumi Y, Miura H, Michiwaki Y, Nagaosa S, Nagaya M. Colonization of dental plaque by respiratory pathogens in dependent elderly. Arch Gerontol Geriat. 2007;44(2):119‐124. [DOI] [PubMed] [Google Scholar]
- 3. Official Statistics Japan . Vital statistics of Japan. 2018. https://www.e‐stat.go.jp/stat‐search/files?page=1&layout=datalist&toukei=00450011&tstat=000001028897&cycle=7&year=20180&month=0&tclass1=000001053058&tclass2=000001053061&tclass3=000001053065&stat_infid=000031883939&result_back=1&cycle_facet=tclass1%3Atclass2%3Atclass3%3Acycle. Accessed May 17, 2020
- 4. Yoneyama T, Yoshida M, Ohrui T, et al. Oral care reduces pneumonia in older patients in nursing homes. J Am Geriatr Soc. 2002;50(3):430‐433. [DOI] [PubMed] [Google Scholar]
- 5. Yoneyama T, Yoshida M, Matsui T, Sasaki H. Oral care and pneumonia. Lancet. 1999;354(9177):515. [DOI] [PubMed] [Google Scholar]
- 6. Ministry of Health . Long‐term care insurance system of Japan. 2016. https://www.mhlw.go.jp/english/polich/care‐welfare/care‐welfare‐elderly/dl/ltcisj_e.pdf. Accessed April 11, 2020
- 7. Cabinet Office . Annual report on the ageing society 2017 (Summary). https://www8.cao.go.jp/kourei/english/annualreport/2017/pdf/c1‐2‐1.pdf. Accessed April 11, 2020
- 8. Zaitsu T, Saito T, Kawaguchi Y. The oral healthcare system in Japan. Healthcare. 2018;6(3):79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Ministry of Health, Labour and Welfare of Japan . Annual health, labour and welfare report 2017. 2017. https://www.mhlw.go.jp/english/wp/wp‐hw11/dl/02e.pdf. Accessed May 17, 2020
- 10. Mahoney FI, Barthel DW. Functional evaluation: the barthel index. Md State Med J. 1965;14:61‐65. [PubMed] [Google Scholar]
- 11. Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412‐2414. [DOI] [PubMed] [Google Scholar]
- 12. Chalmers JM, King PL, Spencer AJ, Wright FA, Carter KD. The oral health assessment tool—validity and reliability. Aust Dent J. 2005;50(3):191‐199. [DOI] [PubMed] [Google Scholar]
- 13. Matsuo K, Nakagawa K. Reliability and validity of the Japanese Version of the Oral Health Assessment Tool (OHAT‐J). J Japan Soc Disabil Oral Health. 2016;37:1‐7. (in Japanese). [Google Scholar]
- 14. Shimizu T, Ueda T, Sakurai K. New method for evaluation of tongue‐coating status. J Oral Rehabil. 2007;34(6):442‐447. [DOI] [PubMed] [Google Scholar]
- 15. Zhang J, Yu KF. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA. 1998;280(19):1690‐1691. [DOI] [PubMed] [Google Scholar]
- 16. Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159(7):702‐706. [DOI] [PubMed] [Google Scholar]
- 17. Sasaki H, Sekizawa K, Yanai M, Arai H, Yamaya M, Ohrui T. New strategies for aspiration pneumonia. Intern Med. 1997;36(12):851‐855. [DOI] [PubMed] [Google Scholar]
- 18. Adachi M, Ishihara K, Abe S, Okuda K, Ishikawa T. Effect of professional oral health care on the elderly living in nursing homes. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(2):191‐195. [DOI] [PubMed] [Google Scholar]
- 19. Hanagata T, Tamura F, Kikutani T, et al. Efficacy of management of oral health care on the nursing home. Japan J Gerodontol. 2009;23:424‐434. (in Japanese). [Google Scholar]
- 20. Abe S, Ishihara K, Okuda K. Prevalence of potential respiratory pathogens in the mouths of elderly patients and effects of professional oral care. Arch Gerontol Geriatr. 2001;32(1):45‐55. [DOI] [PubMed] [Google Scholar]
- 21. Arai Y, Washio M, Kudo K. Factors associated with admission to a geriatric hospital in semisuburban southern Japan. Psychiatry Clin Neurosci. 2000;54(2):213‐216. [DOI] [PubMed] [Google Scholar]
- 22. Nakazawa A, Nakamura K, Kitamura K, Yoshizawa Y. Association between activities of daily living and mortality among institutionalized elderly adults in Japan. J Epidemiol. 2012;22(6):501‐507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Kageyama S, Takeshita T, Furuta M, et al. Relationships of variations in the tongue microbiota and pneumonia mortality in nursing home residents. J Gerontol A Biol Sci Med Sci. 2018;73(8):1097‐1102. [DOI] [PubMed] [Google Scholar]
- 24. Tamakoshi A, Yatsuya H, Lin Y, et al. BMI and all‐cause mortality among Japanese older adults: Findings from the Japan Collaborative Cohort Study. Obesity. 2010;18(2):362‐369. [DOI] [PubMed] [Google Scholar]
- 25. Nakagawa T, Sekizawa K, Nakajoh K, Tanji H, Arai H, Sasaki H. Silent cerebral infarction: a potential risk for pneumonia in the elderly. J Intern Med. 2000;247(2):255‐259. [DOI] [PubMed] [Google Scholar]
- 26. Abe S, Ishihara K, Adachi M, Okuda K. Oral hygiene evaluation for effective oral care in preventing pneumonia in dentate elderly. Arch Gerontol Geriatr. 2006;43(1):53‐64. [DOI] [PubMed] [Google Scholar]
- 27. Kishi M, Takahashi M, Kishi K, et al. Relationship between clinical indicators and the total amount of bacteria in the tongue coat assessed by real‐time PCR in oral care evaluation. J Dent Health. 2006;56:665‐672. [Google Scholar]
- 28. Kikutani T, Tamura F, Nishiwaki K, et al. The degree of tongue‐coating reflects lingual motor function in the elderly. Gerodontology. 2009;26(4):291‐296. [DOI] [PubMed] [Google Scholar]
- 29. Official Statistics Japan . Nursing care benefit statistics. 2018. https://www.e‐stat.go.jp/statsearch/files?page=1&layout=datalist&toukei=00450049&tstat=000001123535&cycle=1&year=20180&month=24101210&tclass1=000001123536&tclass2=000001123537. Accessed May 9, 2020
- 30. Iinuma T, Arai Y, Abe Y, et al. Denture wearing during sleep doubles the risk of pneumonia in the very elderly. J Dent Res. 2015;94(3):28‐36. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data are available on reasonable request to the corresponding author.