

Abstract
Purpose:
To evaluate the efficacy and safety of hybrid 26-gauge needle drainage in scleral buckling for rhegmatogenous retinal detachment (RRD).
Methods:
In this retrospective study, we included patients who underwent scleral buckling surgery along with subretinal fluid (SRF) drainage using the ‘Hybrid 26G needle drainage technique’. Pre-operative assessment included the best corrected visual acuity (BCVA), lens status, and extent of retinal detachment. Intra-operative surgical details such as the height of retinal detachment, number of attempts required to drain the fluid, amount of fluid drained, adequacy of break buckle relationship, and any intra-operative or post-operative complications were noted. Post-operatively, the final visual outcome and retina status were assessed at 3 months of follow-up.
Results:
A total of 10 eyes with primary RRD and proliferative vitreoretinopathy C1 or less were included. Pre-operatively, the mean BCVA was 2.43 ± 1.01 logMAR units, which improved significantly to 0.679 ± 0.45 logMAR units (p value < 0.05) at 3 months of follow-up. Regarding the extent of RRD, five eyes (50%) had a total detachment, two eyes (20%) had a sub-total detachment, and three eyes (30%) had an inferior detachment. Four eyes had shallow detachment, four had a moderate detachment, and two eyes had bullous detachment. Complete drainage of SRF (>75%) was achieved in five patients, and a partial but adequate drainage (50–75%) was achieved in the rest of the five patients. In none of the patients, inadequate or dry tap was encountered. No intra-operative complications were encountered. The retina was attached in eight out of ten eyes at 1 week and at a 1-month follow-up period. Two patients required pars plana vitrectomy for persistent SRF. The retina was attached in all the patients at 3 months of follow-up.
Conclusion:
The ‘Hybrid needle drainage’ technique is a safe and effective technique for SRF drainage in scleral buckling surgery.
Keywords: External needle drainage, hybrid technique, rhegmatogenous retinal detachment, scleral buckling
External drainage of the subretinal fluid (SRF) is very crucial and considered the most dangerous step in buckling surgery.[1] External drainage has a learning curve as it can be associated with dreaded complications such as choroidal hemorrhage, subretinal bleed, vitreous and retinal incarceration, and iatrogenic retinal break formations.[1,2,3] Various surgical techniques have been described for external drainage, that is, the two-step scleral cut-down technique, various needle drainage techniques, and laser drainage.[2,4,5,6,7] Each of these techniques needs skills and can be associated with various complications. These techniques are difficult to perform initially by beginners. In this index study, we present the results of a new technique, that is, the Hybrid 26G needle drainage technique, for SRF drainage.
Methods
In a retrospective study conducted at a tertiary eye care center, we included all patients with rhegmatogenous retinal detachment (RRD) who underwent scleral buckling surgery with the “Hybrid 26G needle drainage technique”. Ethical approval was obtained from the institutional review board (NK/7379/Study/632), and the study was conducted as per the declaration of Helsinki.
Pre-operative assessment included the best corrected visual acuity (BCVA), lens status, extent of retinal detachment, and presence of any proliferative vitreoretinopathy (PVR). Intra-operative surgical details such as the height of retinal detachment, site of drainage, number of attempts required to the drain the fluid, amount of fluid drained, adequacy of break buckle relationship, and any intra-operative or post-operative complications were noted [Table 1]. Post-operative assessment included BCVA and the retinal status at 1 week, 1 month, and 3 months of follow-up.
Table 1.
Extent of RRD and intra-operative details of scleral buckling surgery
| Patient | RRD | Height | Drainage site | Attempts made | Grading of SRF drainage |
|---|---|---|---|---|---|
| 1 | Inferior | Shallow | Inferotemporal | 2 | 1 |
| 2 | Total | Moderate | Inferotemporal | 1 | 2 |
| 3 | Total | Bullous | Inferotemporal | 1 | 1 |
| 4 | Total | Shallow | Inferotemporal | 1 | 2 |
| 5 | Sub-total | Moderate | Superonasal | 1 | 2 |
| 6 | Inferior | Moderate | Inferotemporal | 1 | 1 |
| 7 | Inferior | Shallow | Inferonasal | 1 | 1 |
| 8 | Total | Bullous | Inferotemporal | 2 | 2 |
| 9 | Total | Moderate | Inferior | 1 | 2 |
| 10 | Sub-total | Shallow | Temporal | 1 | 1 |
Surgical technique: Standard surgical steps of scleral buckling were performed. After the exact localization of breaks, cryopexy was performed. This was followed by passing scleral sutures for 277 tire and 240 band. After both the tire and the band were passed underneath the sutures, the drainage site was localized preferably close to the horizontal recti muscles near the equator and in the bed of the buckle. Drainage was performed in the quadrant where the height of detachment was maximum.
A 26-gauge half-inch needle was then attached to a 2 ml syringe with the plunger removed. A 26-gauge needle was then placed at the drainage site such that the bevel of the needle was facing away from the scleral surface. This was followed by linear movement of the tip of the needle on the sclera to cut down the sclera under high magnification [Fig. 1a and b]. Scleral cut-down is usually slightly more than the diameter of the bevel of the needle. The cut-down is performed until the choroid starts to appear. One can clearly see scleral fibers separating while performing the cut-down, and the underlying brown choroid tissue starts to appear. It is at this point one should gently enter into subretinal space using the needle tip in a perpendicular direction [Fig. 1c]. A single puncture with the needle tip creates a sufficient opening and allows passive extrusion of SRF. This was followed by the application of external pressure on the sclera using a cotton bud posterior to the drainage site [Fig. 1d]. Video 1 describes the surgical steps involved in hybrid needle drainage. Drainage was stopped as soon as RPE pigments started to come out or sufficient hypotony was created, and no more fluid came out. Drainage was followed by performing indirect ophthalmoscopy and assessing the amount of residual SRF [Table 1].
Figure 1.
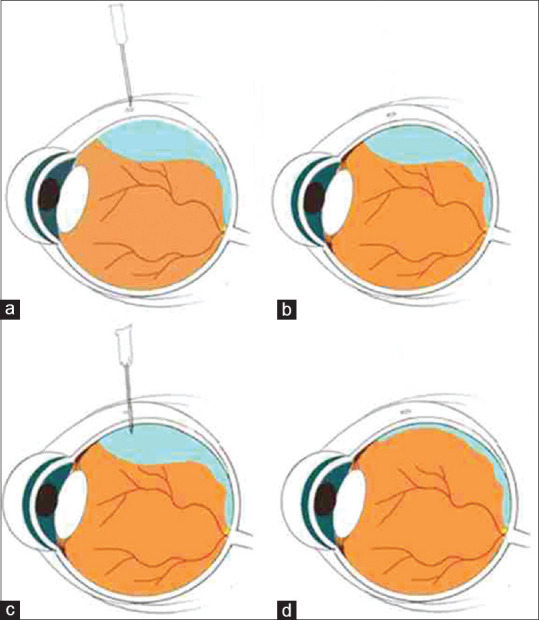
(a) Linear movement with the tip of a 26-gauge needle and bevel facing away from the scleral surface. (b) Scleral cut-down using the tip of a 26-gauge needle. (c) Perpendicular entry into subretinal space using the tip of the needle. (d) External compression with a cotton bud to drain the SRF
Adequacy of drainage was assessed by indirect ophthalmoscopy and graded as described by Aylward et al.[2] Grade 1 was defined as complete drainage of SRF, grade 2 as partial but adequate drainage (allowing an adequate break buckle relationship), grade 3 as partial but inadequate drainage, and grade 4 as dry tap.
The procedure was repeated, preferably at another site, if the surgeon felt that residual SRF was too much to avoid apposition of the break to the choroid.
Once the drainage was completed, buckle and band sutures were tied. Post-operatively, the patients were started on the following eye drops: moxifloxacin 0.5% four times a day, betamethasone 1% six times a day, and homatropine 2% four times a day.
The patients were followed up at 1 week, 1 month, and 3 months, respectively. BCVA and the retinal status were assessed at the respective follow-up visits.
Categorical variables were measured as percentages, and continuous variables were measured as mean. Paired t test (SPSS software 2003) was applied to compare final visual acuity with the initial presenting visual acuity. A P value <0.05 was considered statistically significant.
Results
A total of nine patients (ten eyes) were included in this retrospective study. The mean age of the patients was 26.44 ± 6.28 years, with a male to female ratio of 3.5:1. All eyes were phakic and had a clear lens. The mean BCVA at baseline was 2.43 ± 1.01 logMAR units. Regarding the extent of RRD, five eyes (50%) had a total detachment, two eyes (20%) had a sub-total detachment, and three eyes (30%) had an inferior detachment. All eyes had PVR grade C1 or less. Nine eyes had a macula off RRD, whereas one eye had a macula on RRD. The height of detachment was assessed intra-operatively. Shallow detachment was seen in four eyes (40%), moderate detachment was seen in another four (40%), and bullous detachment was noted in two eyes (20%).
After drainage using ‘Hybrid needle drainage’, an adequate break buckle relationship was obtained in all ten patients with no intra-operative complications. We did not encounter scleral gaping and the need for suturing in any of our patients at the drainage site. In eight out of ten eyes, adequate drainage could be achieved with a single attempt. The retina was attached at 1 week and 1 month follow-up in eight patients. Two patients (Patient 2 and 9) had a persistent fluid despite adequate drainage and subsequently underwent pars plana vitrectomy.
The final mean BCVA improved significantly to 0.679 ± 0.45 logMAR units (p value < 0.05) at 3 months of follow-up. The retina was attached in all ten eyes at 3 months of follow-up.
Discussion
This case series highlights safety and efficacy of a newly described hybrid 26G needle drainage technique in scleral buckling surgery.
Our technique is a hybrid of techniques described by Schepens[7] and Azad et al.[4] It involves a scleral cut using the tip of a 26-gauge needle instead of a scleral blade as described by Schepens.[7]
This is followed by using the tip of the same needle to enter into the subretinal space through the choroid as described by Azad et al.[4] Contrary to a direct perpendicular entry by a 26-gauge needle through the sclera as described by Azad et al.,[4] we prefer to make a perpendicular entry after the scleral cut-down. This allows for a very controlled entry into the subretinal space and avoids a sudden jerk which is felt while directly entering through the sclera. The technique described by Azad et al.[4] is associated with poor control and depth of puncture. Sudden jerk is usually felt as soon as there is a loss of resistance as one pierces through the sclera. A sudden jerk can cause choroidal hemorrhage and more than required penetration of the needle tip, resulting in iatrogenic retinal break formation in cases of shallow retinal detachments.
The traditional cut-down technique of drainage has the risk of incomplete drainage, retinal and vitreous incarceration, bleeding from choroidal vessels, and sudden hypotony.[8] Trans-scleral needle drainage using a 26-gauge ½ inch needle is a safer alternative with negligible risk of hemorrhage and incarceration owing to smaller sclera choroidal opening.
Another technique, that is, the external needle drainage technique, was initially described by Charles.[9] in 1985 using a 25-gauge, 5/8-in needle. After an oblique entry through the sclera into the subretinal space, indirect ophthalmoscopy was used to assess the correct placement of the needle tip and the needle is withdrawn as soon as sufficient fluid is drained. This technique, although effective in reducing retinal incarceration and retinal injuries, is associated with a steep learning curve. Also, oblique passage through the choroid increases the chances of choroidal hemorrhage as compared to perpendicular passage.
Kitchens et al.[6] have described the ‘Guarded needle approach’ to avoid over-penetration of the needle while draining the SRF. The technique involves the placement of a buckle sleeve over the shaft of the needle. This prevents over-penetration of the needle and associated complications. Our technique also aims to prevent over-penetration by creating a mini scleral cut-down and avoiding scleral resistance and jerk associated with needle drainage. The guarded needle approach involves exposing 4 mm of the needle tip anterior to the buckle sleeve. We believe that exposing 4 mm of the needle tip can still be associated with over-penetration and risk of iatrogenic damage in the case of shallow detachments. Apart from this, the guarded needle drainage technique requires use of a buckle sleeve, which further adds to the cost of treatment.
Another modification of external needle drainage involves bending the tip of the 26-gauge needle by 2 mm (as in anterior capsulotomy) without bending the shaft.[10] The sclera is punctured in such a way that the tip is perpendicular to the sclera and the shaft is tangential to the sclera which acts as a guard, thus preventing entry beyond 2 mm.
All the above-described techniques aim to avoid over-penetration of the needle to prevent inadvertent damage to the retina. The chances of such complications increase in cases where detachment is shallow.
We in this technique aim to avoid this sudden jerk associated with trans-scleral needle drainage. A mini scleral cut-down created using the tip of the needle allows easy passage of the needle through the choroid and controlled drainage. The surgeon need not wait for the fluid to enter into the hub of the needle, as described by Azad et al.[4] Waiting for the fluid to come into the hub can be associated with iatrogenic retinal injury in the case of shallow detachments.
Laser choroidotomy involves scleral cut-down and choroidotomy using an endolaser probe.[5] This causes coagulation of choroidal vessels and prevents any retinal injury. This technique is particularly useful in cases of shallow detachment but requires additional instrumentation which might not be available at peripheral centers. Contrary to this, our technique also effectively drained the fluid in all the cases of shallow retinal detachment and does not require any special instrumentation.
Our technique has an advantage over the previously described needle drainage techniques in the sense that it is more controlled and thus can even be performed in cases of shallow retinal detachments. Second, as the point of entry through the choroid is so small, diathermy of the choroid before entering into the subretinal space is not required. Third, this small opening in the choroid also avoids the risk of retinal or vitreous incarceration. Last, perpendicular entry using the needle tip causes fewer chances of choroidal and subretinal hemorrhage as the passage through the choroid is decreased compared to oblique 25-gauge needle entry as was originally described by Steve Charles.[9]
This technique can also be performed in high myopic eyes and thin scleras. The cut-down is performed in multiple strokes using a needle tip and not as a single linear cut as with a blade. This makes it more controlled and can easily cut down even thin scleras.
Our study has few limitations. First, this is a retrospective study with a limited sample size. Prospective comparative studies with a large sample size are warranted. Second, because of a small sclerotomy, the drainage may be difficult in cases of old RRDs with viscous SRF.
Conclusion
To conclude, the hybrid 26-gauge needle drainage technique is much easier to perform, does not require much learning curve, and can be easily performed by the beginners. This technique is much more controlled and can even be performed in shallow retinal detachments without any risk of iatrogenic retinal break formation. Compared to the traditional drainage technique, the hybrid needle drainage technique is much safer and not associated with inadvertent complications such as iatrogenic retinal injury, retinal or vitreous incarceration, hypotony, choroidal detachment, or choroidal hemorrhage.[3,8,11]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video avaliable on: www.ijo.in
References
- 1.Johnston GP, Okun E, Boniuk I, Arribas NP. Drainage of subretinal fluid: Why, when, where and how. Mod Probl Ophthalmol. 1975;15:197–206. [PubMed] [Google Scholar]
- 2.Aylward GW, Orr G, Schwartz SD, Leaver PK. Prospective, randomised, controlled trial comparing suture needle drainage and argon laser drainage of subretinal fluid. Br J Ophthalmol. 1995;79:724–7. doi: 10.1136/bjo.79.8.724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wilkinson CP, Bradford RH. Complications of draining subretinal fluid. Retina. 1984;4:1–4. doi: 10.1097/00006982-198400410-00001. [DOI] [PubMed] [Google Scholar]
- 4.Azad R, Kumar A, Sharma YR, Rajpal Modified needle drainage. A safe and efficient technique of subretinal fluid drainage in scleral buckling procedure. Indian J Ophthalmol. 2004;52:211–4. [PubMed] [Google Scholar]
- 5.Bovino JA, Marcus DF, Nelsen PT. Argon laser choroidotomy for drainage of subretinal fluid. Arch Ophthalmol. 1985;103:443–4. doi: 10.1001/archopht.1985.01050030139041. [DOI] [PubMed] [Google Scholar]
- 6.Kitchens JW. Modified external needle drainage of subretinal fluid in the management of rhegmatogenous retinal detachment using a “guarded needle” approach. Arch Ophthalmol. 2011;129:949–51. doi: 10.1001/archophthalmol.2011.165. [DOI] [PubMed] [Google Scholar]
- 7.Schepens CL. Philadelphia: W. B. Saunders & Co; 1983. Retinal Detachment and all Allied Diseases; pp. 409–16. [Google Scholar]
- 8.Burton RL, Cairns JD, Campbell WG, Heriot WJ, Heinze JB. Needle drainage of subretinal fluid. A randomized clinical trial. Retina. 1993;13:13–6. doi: 10.1097/00006982-199313010-00004. [DOI] [PubMed] [Google Scholar]
- 9.Charles ST. Controlled drainage of subretinal and choroidal fluid. Retina. 1985;5:233–4. doi: 10.1097/00006982-198500540-00009. [DOI] [PubMed] [Google Scholar]
- 10.Agarwal MK. Modified needle drainage. A safe and efficient technique of subretinal fluid drainage in scleral buckling procedure. Indian J Ophthalmol. 2004;52:342–3. author reply 343. [PubMed] [Google Scholar]
- 11.Hilton GF. The drainage of subretinal fluid: A randomized controlled clinical trial. Trans Am Ophthalmol Soc. 1981;79:517–40. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.