

Abstract
Background
Research indicates that food parcels provided by food banks are nutritionally poor. Food insecurity and the use of food banks are both rising, with detrimental effects on the dietary intake and health of users. This mixed‐method systematic review aims to investigate the current nutritional adequacy of pre‐packaged food parcels and whether using food banks reduces the food insecurity and improves the dietary intake of their users.
Methods
A mixed‐method systematic literature review, restricted to articles published from 2015, was conducted using eight electronic databases, four grey literature databases and eight relevant websites. Quantitative findings, investigating the nutritional quality of food parcels and/or their impact on dietary intake or food insecurity, were presented narratively. Qualitative findings reporting the views of food bank users regarding food from food banks underwent thematic synthesis. These independent syntheses were integrated using configurative analysis and presented narratively.
Results
Of 2189 articles, 11 quantitative and 10 qualitative were included. Food parcels were inconsistent at meeting nutritional requirements and often failed to meet individual needs, including cultural and health preferences. Using food banks improved food security and dietary quality of users, allowing otherwise unachievable access to food. However, food insecurity remained, and is explained by limited food variety, quality and choice. The mixed‐method findings support interventions to ensure consistent, adequate nutrition at food banks, including catering for individual needs.
Conclusions
Food banks are a lifeline for those severely food insecure. However when used alone, food banks struggle to eliminate the heightened food insecurity of their users. Efforts to improve the nutritional quality of food parcels could improve the experiences and diet‐related outcomes of those requiring food banks.
Keywords: food assistance, food parcel, food security, food bank, nutrition
Key points
The nutritional quality of food parcels is inconsistent, and is often poor compared with national nutritional recommendations. This can be explained by the limited quantity and variety of food options as well as a lack of nutritional guidelines at food banks.
Food banks struggle to meet individual health, social, and cultural dietary needs in socially acceptable ways. Positive outcomes from diabetes‐specific food parcels highlight the advantages of tailoring parcels to meet individual needs and preferences.
Food banks are a lifeline, which improve dietary intake and food security in times of crisis. However, as a sole intervention, food banks do not eliminate the heightened food insecurity and poor diets of food bank users.
INTRODUCTION
Food insecurity is a state which is defined as the limited or uncertain access to nutritionally adequate, safe foods, in a socially acceptable way. 1 Food insecurity can be mild, moderate or severe, ranging from worrying about accessing food to experiencing days without eating. 2 Economic need drives food insecurity, thus incidence is highest among households at the bottom of the income distribution table. 2 , 3 , 4 Food insecurity has been rising over the past decade across high‐income countries. 5 In Canada, the USA, and the UK, 10.5%, 12.7%, and 14% of households experience food insecurity, respectively. 6 , 7 , 8 Such countries have experienced unprecedented levels of food insecurity during the COVID‐19 pandemic, owing to reduced food access and economic crises. 9 , 10 , 11 , 12 This trend is predicted to continue; thus the world is not on track to meet the UN Sustainable Development Goal of diminishing hunger by 2030. 13 , 14
Social‐security policies, including welfare benefits, intend to ensure basic standards of living are met, but they are inadequate to eradicate food insecurity. 15 , 16 , 17 Therefore, charity‐run food services such as soup kitchens, community‐based meal provision, and food banks have been increasingly used, with the aim of minimising food insecurity. 18 , 19 Food banks have been established in the USA and Canada for decades and they are now common across high‐income countries, including the UK, Australia and Germany. 20 , 21 , 22 , 23 Food banks are either warehouses collecting and distributing food to charities or smaller charitable organisations serving clients directly. 20 , 24 The latter will be the focus of this review, and these typically operate by providing households with prepackaged food parcels without charge. 19 , 21 Measures of key performance indices for food banks are nonmonetary (i.e. efficiency and effectiveness) as they are nonprofit organisations. Food bank efficiency is defined as the total allocated amount (in terms of weight) of food items distributed by a food bank. However, the effectiveness of a food bank is defined by how well the nutritional needs of users are met by the service provided by that food bank. 25
Food bank use is greatest among unemployed, lone‐parent and single‐person households, and those suffering ill‐health. 2 , 26 Individuals using food banks are predominantly severely food insecure, hence they represent a small proportion of food insecure populations. 2 , 27 , 28 For example, 3% of the Canadian population is severely food insecure, a figure rising to 66% among food bank users. 28 In the UK, 14% of households experience food insecurity, yet only 2.5% use food banks. 2 , 6 Similarly, among a sample of low‐income families in Canada, only 23% of those suffering food insecurity used a food bank. 4 These figures are unsurprising as food banks are not the only intervention for food insecurity; in addition, referrals are often not received and stigma discourages use. 4 , 29 , 30
Corresponding with rising food insecurity, food bank use has been increasing. 2 , 31 In the UK, USA, and Canada, this is driven by recession, austerity and welfare reforms, particularly benefit sanctions and delays. 2 , 12 , 14 , 30 COVID‐19 saw an exacerbated demand for food banks, including an increase of 33% in the UK from 2020 to 2021, resulting in 2 537 198 parcels being distributed. 32 This is significantly greater than typical annual rises, with 37% of use attributed to COVID‐19. 2 Europe, Canada, the USA, and Australia also report unforeseen demand from consequences related to the COVID‐19 pandemic. 33 , 34 , 35 , 36
A high‐quality diet can be defined as aligning with national dietary recommendations, including the UK ‘Eatwell Guide’ and the ‘MyPlate’ in the USA. 37 , 38 Food insecurity is associated with poor dietary intake, including low fruit and vegetable (FV) and micronutrient consumption, 39 , 40 as well as undernutrition and obesity. 41 , 42 The latter relationship is supported by reliance on inexpensive, nutrient‐poor, energy‐dense food. 41 Rising food costs, increasing price gaps between healthy and unhealthy foods, and reduced access to nutrient‐dense food in deprived areas further hinders dietary quality. 43 , 44 , 45 , 46 Individuals who use food banks have inadequate energy, FV, dairy, and meat intake compared with national recommendations. 47 , 48 , 49 In addition, their dietary quality is worse than the general population. 50 This is unsurprising, as for example, the poorest UK decile require 74% of their disposable income to follow the ‘Eatwell Guide’ dietary recommendations. 51 Moreover, in the USA, food‐insecure food bank users have a poorer knowledge of nutrition, which negatively influences dietary choices compared with those that of the food secure. 47
Food insecurity influences health‐inequalities, with heart disease, diabetes, anaemia, and poor mental health more prevalent among the food insecure. 52 , 53 , 54 , 55 , 56 This is reflected in food bank users: in the UK, 83% suffer ill‐health, and in the USA, rates of obesity, diabetes, and heart disease are greater than in the general populations. 2 , 55 Food insecurity, ill‐health and food bank use is cyclical, with poor nutrition influencing chronic disease and ill‐health driving use. 29 This is exacerbated when donated food is unsuitable for some health conditions and healthcare professionals struggle to support patients with food insecurity. 56 , 57 Economic disparities and an overwhelmed healthcare system due to the COVID‐19 pandemic means ill‐health is projected to worsen for those with food insecurity. 58
Food provided by food banks can provide over half of their clients’ total dietary intake. 59 Previous systematic reviews investigating the nutritional quality of food bank parcels found variance across studies. 48 , 60 However, parcels are often insufficient in dairy, meat, FV, and micronutrients (e.g. calcium, iron, and vitamins A and C). 48 , 60 These reviews were published in 2016 and are limited to the USA, Australia, and Canada. 60 Since 2016, studies in Europe have investigated the nutritional quality of food bank parcels. 61 , 62 Qualitative research similarly suggests that food banks inadequately meet dietary needs, with food that is of poor quality, disliked, and culturally inappropriate. 4 , 23 , 63 , 64 , 65 Despite food banks being considered an emergency source of food, their chronic and multiple use is reported, suggesting their contribution to dietary intake is long‐term. 15 , 66 , 67 Annually, 43–50% of UK food bank users receive multiple parcels and in Canada, 65% of parcels are supplied to repeat clients. 2 , 31 , 68
Despite the rising use of food banks, qualitative research indicates that they are inadequate to address food insecurity. 16 , 48 In addition, quantitative studies investigating whether food banks reduce food insecurity have conflicting results. 30 , 47 , 69 Considering dietary intake, improvements in energy and nutrient intake are seen following food bank use, yet overall dietary quality may remain poor. 59 , 70 There is recognised need for further research investigating the efficacy of food banks, including a synthesis of these studies. 15 This systematic review aims to provide an update on the nutritional quality of food parcels and their effectiveness at improving food security, building on reviews published in 2016. 48 , 60 This review is limited to high‐income countries and the objectives were to (a) investigate the nutritional quality of food parcels compared with adult nutritional requirements and (b) investigate the effectiveness of food banks at improving the food security and dietary intake of food bank users.
METHODOLOGY
This systematic review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines. 71 , 72 The Joanna Briggs Institute (JBI) methodology for mixed‐method systematic reviews was followed 73 and the review protocol was registered a priori with PROSPERO (CRD42021269065).
Eligibility criteria
The terms food ‘banks’, ‘pantries’, and ‘shelves’ describe charitable food parcel provision. In this review, the term ‘food bank’ refers to charitable organisations providing prepackaged food parcels directly to eligible clients without charge.
The eligibility criteria is outlined in Table S1. Quantitative and qualitative studies available in English were considered. A mixed‐method approach allows greater insight, with personal perspective and experience investigated in the context of objective findings. 74 To update the previous systemic reviews, articles included were published from 2015 onwards. 48 , 60
The population of interest was adults receiving prepackaged food parcels from food banks in high‐income countries as defined by the World Bank. 75 While food banks are present globally, operational characteristics in low‐income countries often differ. 76 Therefore, with limited similarities, studies from low‐income countries were excluded. Articles solely investigating food parcel provision to children were also excluded, as different nutritional requirements from those of adults would make comparison between studies difficult. 77
Quantitative studies either, (a) measured the nutritional quality of food parcels provided by food banks, compared to national dietary recommendations, and/or (b) evaluated the impact or association of food banks on the food security and/or dietary intake of food bank users. Qualitative studies investigated both research objectives, exploring the views/perceptions of users regarding food bank food. With differences in aims and operations, interventions providing only preprepared meals, such as soup kitchens, subsidiary programmes, or client‐choice food banks were excluded. 15 , 18 , 78 Articles were excluded if food parcel items were listed without indication of quantity, as this does not allow nutritional assessment. If food security or dietary intake were measured, yet not related to food bank use, articles were excluded as this does not explore their effectiveness. Unlike Simmet et al., excluding interventions <6 months, no temporal restrictions were placed on intervention studies. 60 Although precluding long‐term outcomes, temporal restrictions could exclude beneficial approaches for improving food banks.
Search
On 15 June 2021, systematic title and abstract literature searches were conducted by reviewer 1 (L.O.) to simultaneously retrieve qualitative and quantitative studies. Eight databases were used: ASSIA (ProQuest), CINAHL (EBSCOhost), Cochrane Central Register of Controlled Trials (Cochrane Library), EMBASE (Ovid), MEDLINE (EBSCOhost), PubMed, PsycINFO (EBSCOhost), Scopus. A scoping search identified relevant grey literature. 79 With public health research abundant in grey literature, and to prevent omission of appropriate data, grey literature databases and relevant websites were searched on 17 June 202180 (Table 1).
Table 1.
The grey literature sources searched for grey literature to include in the review
| Grey literature databases | Organisational websites |
|---|---|
|
OpenGrey (System for Information on Grey Literature in Europe) The Grey Literature Report Health Management Information centre (HMIC) (Ovid) Social Care Online (SCO) |
The Trussell Trust The Food Foundation The Independent Food Aid Network (IFAN)Feeding America European Food Bank Federation Food Banks Canada Food Bank Australia The Global Food Banking Network |
There was initially a limited search of MEDLINE, including analysis of free‐text keywords in titles/abstracts and medical subject headings (MesH). The search strategy was adapted to include the identified keywords and MesH. The following free‐text keywords were used in the search strategies: ‘food bank’, ‘food bank’, ‘food pantry’, ‘food shelves’, ‘food parcel’, ‘diet’, ‘nutrition’, ‘food security’, ‘food insecurity’. MEDLINE, PubMed, CINAHL, and Cochrane searches used the subject heading ‘food assistance’. Searches were filtered to English articles published from 2015 onwards. Tables S2 and S3 document the search strategies.
Study selection
Stage 1: All search results were exported to ‘EndNote20’, and duplicates were removed. Two reviewers (L.O., C.P.) independently screened the results by title and abstract, and articles were excluded if they did not meet the inclusion criteria.
Stage 2: Full texts included in Stage 1 were reviewed for inclusion by reviewer 1 (L.O.) and 20% were independently assessed by reviewer 2 (C.P.). Full texts that did not meet the inclusion criteria were excluded (Figure 1).
Figure 1.
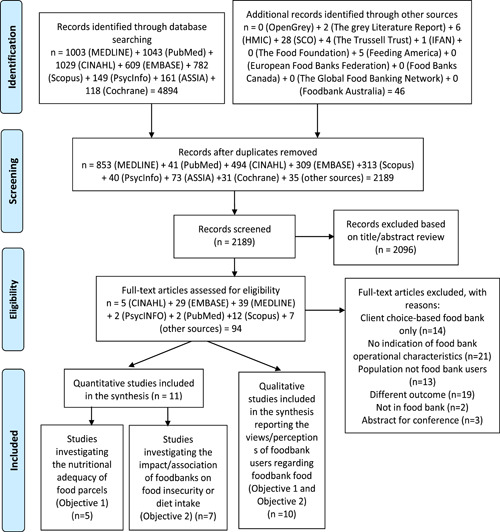
Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flow chart outlining the study selection process for inclusion in the mixed‐method systematic review 71
The reference lists of full texts meeting the eligibility criteria were searched by reviewer 1 (L.O.). Any uncertainties during study selection were resolved through consensus between the reviewers.
Data extraction
A standardised data extraction form was used to ensure that the data extracted from the included studies was consistent. The following information was gathered: study characteristics (authors, year, location, study design, sample size), population characteristics, methodology, outcomes, and key findings. By comparison with the eligibility criteria, studies were organised into quantitative and qualitative, and data was arranged in Microsoft Excel spreadsheets (Tables 2, 3, 4).
Table 2.
The characteristics and findings of the five quantitative studies that were included in the systematic review and investigated the nutritional adequacy of food parcels provided by food banks (objective 1)
| Study characteristics | Population | Methodology | Outcomes | Key findings | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Citation | Location | Study design | Sample size | Aim/intervention | Data collection and analysis | Food parcel | Diet | Other | ||
| Fallaize et al. (2020) 61 | England, Oxfordshire Food banks (prepackaged) | Cross‐sectional | Food banks: n = 10 Food parcels: n = 11 | NA | To investigate the nutritional adequacy of single‐adult food parcels | Food bank manager questionnaire. Researchers collect contents and input into dietplan7 Controlled for recommended days of parcel use (4–9), mean nutritive values compared with UK adult DRVs t‐test | Nutrients and energy: E, F, Sf, Uf, P, C, S, Fi, Sa, Na, K, Ca, Mg, Po, Fe, Cu, Zn, Se, I, Va, Vd, Th, Ni, Vb6, Fo, Vb12, Vc | NA | Days food parcels could provide sufficient energy Independent foodbanks compared to Trussell Trust foodbanks | Nutrients and energy: mean weighted F met DRV and E, P, C, S, Fi and Sa significantly exceeded DRVs (p < 0.05); providing 138%, 220%, 170%, 277%, 238%, and 180% DRVs, respectively. Carbohydrates provided greatest percentage of energy per parcel (62.2%) significantly exceeding DRV (50%, p < 0.001). All micronutrients significantly exceeded DRVS (p < 0.05), other than selenium meeting DRV, and Vd and Va, meeting 25% and 27% of DRVs, respectively Ideal days: food parcels provided adequate energy beyond recommended days, ranging 4–9 days Independent vs. Trussell Trust: no differences in nutritional quality, other than mean Vd and Cu, where significantly less of these nutrients was provided in Trussell Trust parcels (p < 0.05) |
| Hughes and Prayogo (2018) 79 | England, London Food banks (prepackaged) | Cross‐sectional | Food banks: n = 5 Food parcels: n = 71 | NA | Nutritional analysis of single‐adult food parcels | Photographs of food parcel contents, data inputted into dietplan7 Controlled for recommended days of parcel use (3), mean nutritive values compared with UK adult RNIs | Nutrients and energy: E, P, C, F, S, Sf, tf, Sa, Na, K, Ca, Mg, Fe, Cu, Zn, Se, I, Va, Vc, Ve, Th, Ri, Ni, Vb6, Vb12, Fo | NA | Ideal number of days food parcels could provide sufficient energy and nutrients Impact of removing items on sugar content | Nutrients and energy: Parcels exceeded 100% of RNIs for E, P, C, S, Sa, minerals, trace elements and all vitamins, other than Vd and Ve, which were below 100% of RNIs. Fat was also below nutritional recommendations Ideal days: parcels could provide sufficient P for 6 days and E for 5 days; however, nutrients (Fe, Vc, Vd, Ve, and Fo) would be below recommendations Removing items: removing sugar, jam and preserves, biscuits, or apple juice, reduced S by over 10% |
| Long et al. (2019) 81 | USA, Northwest Arkansas Food pantries (prepackaged) | Pre–post | Food banks: n = 3 Food parcels: n = 123 (pre), n = 172 (post) Food bank users: n = 123 (pre), n = 172 (post) | Age (years): ≥18 Female: pre (99, 80.4%), post (109, 63.4%) | Evaluate an intervention aiming to improve the nutritional quality of food parcels Intervention: food donation lists and informing donors, educational material for food bank users, discussing healthy foods | Foodbank user surveys; audit of food parcel items at baseline and 1 year Mean nutritive values of parcels per‐household and per person Parcels controlled for maximum 2000 kcals of food and compared with US adult DRVs χ 2; t‐test | Nutrients and energy: E, P, Na, C, Fi, S, F, Sf, Tf, Ch Food groups: Fresh fruit and vegetable servings | NA | NA | Nutrients and energy: from pre‐ to post‐intervention, no nutrients changed per person. Mean E per household significantly increased (20,256.38 [SD 16,301.03] vs. 25,108.46 [SD 19,099.66], p = 0.009), but no significant change per person Up to 2000 kcals, mean food parcels exceeded P, C, Na, and Fi DRVs and were below F, Sf and Ch DRVs (both pre‐ and post‐intervention) Food groups: from pre‐ to post‐intervention, mean fruit and vegetable servings per person significantly increased (0.22 [SD 1.38] vs. 3.33 [SD 7.69], p < 0.001). Pre‐intervention, fruit and vegetable servings were 99% apples; however, post‐intervention, servings included strawberries (29.0%), tomatoes (13.6%), onions (13.5%), apples (10.6%), and others (33.2%) |
| Neter et al. (2016) 62 | Netherlands Food banks (prepackaged) | Cross‐sectional | Food banks: n = 11 Food parcels: n = 96 | NA | To assess the nutritional quality of food bank parcels | Standard scoring form – food items coded using Dutch food composition table code using measures, weights and Codes guide Controlled for recommended days of parcel use (2.5) and the intended number of users. Mean nutritive values compared with Dutch healthy diet nutritional guidelines and Dutch food composition table of food groups | Nutrients and energy: E, C, P, F, Uf, Fi Food groups: fruit, vegetable, fish. Dutch food composition food groups | NA | Ideal number of days that food parcels could provide sufficient energy, nutrients, fish, fruit, and vegetables for one adult | Nutrients and energy: mean E, P, and Sf exceeded nutritional guidelines and C met nutritional guidelines Food groups: mean fruit and fish were below, whereas vegetable content exceeded guidelines. Food (percentage of parcels including): bread and vegetables (100); pastry and cookies (96); nuts, seeds and snacks (95); sugar, candy, sweet filling, sweet sauces (90); milk, milk products (82); fats, oils and savoury sauces (78); fruits (76); meat, meat products and poultry (75); grains, flour, rice (69); potatoes (69); combined dish (55); cheese (52); soup (34); fish (27); soya and vegetarian (25); eggs (21); savoury fillings (17); legumes (8) Median amount (g) and IQR in parcels: bread (256 [156–398]); milk (358 [91–724]); meat (124 [6–228]); bread (256 [156–398]); vegetables (247 [168–455]); potatoes (143 [0–245]); fish (0 [0–22]); soya and vegetarian (0 [0–1]); eggs, legumes (0) Ideal days: Nutrient (days could last): E (4.4–6.2); P (6.4–11.3); C (3.1–7.8), Fi (3.1–1.4); F (3.7–10.5); fish (1.7); fruit (1.2), vegetables (3.7) |
| Philip et al. (2018) 82 | Israel Food pantries (prepackaged) | Cross‐sectional | Food banks: n = 16 Food parcels: n = 90 Food bank users: n = 105 | Mean age (SD): 52.1 (14.5) Female: 81 (77.1%) | To assess the nutritional quality of food parcels and the association between food parcel quality and their users dietary quality and food security | Telephone survey with food bank users; staff‐reported food parcel items Based on weekly parcel provision and controlled for household size, age and gender. Mean nutritive values compared to weekly USA RDAs and energy and portions recommended by the National Nutrition Security CouncilUnivariate analysis; χ 2 test; t‐test; one‐way ANOVA | Nutrients and energy: E, P, Fi, Ca, Fe, Mg, Va, Ve, Vd, Vc, Th, Ri, Ni, pa, vb6, Fo, and Vb12 Nutritional quality: HPS; NDS Food groups: fruit and vegetable portions | FFQ for HPS and NDS | Percentage of parcels meeting weekly household RDAs | Food parcel nutrition (objective 1): nutrients and energy: mean parcels provided 29.6% E, 54.9% P, 49.9% Fi recommendations; 1.1%, 11.1%, 11.1% of parcels met household E, P, Fi requirements, respectively. Mean parcels exceeded Va, Ri, Fo, and Vb12 recommendations, but were insufficient in Ca, Fe, Ve, Vd, Th, Ni, Pa, and Vb6. No parcels met weekly household Vd and Ca requirements Nutritional quality: Mean parcel HPS and NDS were 20 (SD 20.3) and 0.3 (SD 0.3), respectively. Mean parcels provided 36.4% of recommended total portions and 14.4% of parcels met household portion guidelines Food groups: Mean parcels provided 87% of recommended fruit and vegetable portions, with 25% of parcels meeting fruit and vegetable portions Food bank effectiveness (objective 2): dietary quality: food parcel nutritional quality (HPS) positively correlated with diet quality (NDS), both before and after adjusting for gender, marital status and country of birth (Standardized: β = 0.22, p = 0.03. Overall model: R 2 = 0.18, F = 4.65, p < 0.01) |
Note: Dutch food composition groups: bread, non‐alcoholic beverages, vegetables, pastry and cookies, nuts, seeds and snacks, sugar, candy, sweet filling and sweet sauces, fruits, meat and poultry, grains, flour and rice, potatoes, cheese, combined dish, cheese, soup, fish, soya and vegetarian products, eggs, savoury filling, legumes. 61 HPS: adherence to “Basic Healthy Food Basket Guidelines” established by the Government of Israel's National Nutritional Security Council and Ministry of Health. These guidelines define adequate portion sizes for each of five healthy food groups (whole grains, fruits, vegetables, protein‐rich foods, fats and oils) and the recommended daily portions according to RR age and sex. HPS is a food‐based score. Division of total healthy portions by total energy is meant to account for unhealthy foods in the diet so the HPS score increases as healthy portions in the diet increases but decreases with increasing total energy intake. The higher the score the higher the quality of food or diet. 82 NDS: degree to which the diet achieves the RDA for macronutrients and micronutrients, divided by the overall energy density of the food. A score of 1 indicates a food or diet that provides 100% of the RDA at the required energy intake; a score <1 indicates some degree of deficiency, and a score higher than 1 indicates possible excess. 82 Nutrient and energy outcomes key: E (energy), P (protein), C (carbohydrate), F (fat), Sf (saturated fat), Uf (unsaturated fat), Tf (trans fat), Ch (cholesterol), Fi (fibre), S (sugar), Sa (salt), K (potassium), Na (sodium) Ca (calcium), Fe (iron), Mg (magnesium), Po (phosphorus), I (iodine), Zn (zinc), Cu (copper), Se (selenium), Va (vitamin A), Ve (vitamin E), Vd (vitamin D), Vc (vitamin C), Vk (vitamin K), Th (Thiamine), Ri (Riboflavin), Ni (niacin), Ma (manganese), pa (pantothenic acid), vb6 (vitamin B6), Fo (folate), Vb12 (vitamin B12), FV (fruit and vegetables).
Abbreviations: DRV, dietary reference value; HPS, healthy portions score; IQR, interquartile range; NA, not applicable for the study or this systematic review; NDS, nutrient density score; RDA, recommended daily allowance; RNI, reference nutrient intake; SD, standard deviation.
Table 3.
The characteristics and findings of the seven quantitative studies that were included in the systematic review which investigated the impact or association of food banks on the food insecurity or diet intake of food bank users (objective 2)
| Study characteristics | Population | Methodology | Outcomes | Key findings | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Citation | Location | Study design | Sample size | Aims/intervention | Data collection and analysis | Food parcel | Food security | Diet | Other | ||
| Cheyne et al. (2020) 83 | USA, Oakland, California Food pantries (prepackaged) | Pre–post | Food banks: n = 12 Food bank users: n = 192 | Mean age (SD): 48.5 (12.7) years Female: 174 (90.6%) Condition: food bank user with prediabetes | To assess effectiveness of food bank‐based intervention at improving food insecurity, diet intake and diabetes risk Intervention: monthly food parcels, text‐based health promotion education; engagement messages | Participants completed survey at baseline and at 6 months χ 2test; t‐test; Fisher exact tests | NA | USDA 6‐item | Food groups: FRESH foods survey | Physical activity, general health, BMI, engagement in the intervention | Food security: after 6 months, percentage of participants reporting food insecurity decreased from 68.8% to 62.5% (Pearson χ 2 = 72.6, p < 0.001). Food groups: from pre–post, frequency of consumption of fruits and vegetables, whole grains, green salad, potatoes, nonfried vegetables, and cooked beans significantly increased, whereas consumption of sweetened drinks, fried potatoes, candy/chocolate, cookies and cakes significantly decreased (p ≤ 0.05). Other: minutes of physical activity per week increased 95.6–145.1 (paired t‐test = 4.05, p < 0.001). Percentage reporting health status as poor or fair declined 73.9–60.1% (Fisher exact = 39.19, p < 0.001). Mean BMI (32.4 kg/m2) did not change |
| Ferrer et al. (2019) 84 | USA Food bank (prepackaged) | RCT | Food banks: n = 1 Food bank users: n = 58 (29 control, 29 intervention) | Age (mean): 34–72 (54) years Female: 36 (62%) Condition: HbA1c >9% and food insecure | To assess whether a food bank–primary care collaboration improves food security and diabetes control Intervention: 2× weekly provision of fresh and canned food parcels; nutrition education conducted by a dietitian; health worker visits | Outcome measurement at baseline and at 6 months Kernel density plots | NA | NA | Dietary quality: STC‐Diet | HbA1c, BMI | Dietary quality: mean STC‐Diet increased by 2.47 points (21‐point scale) in intervention (95% CI = 1.42–3.52; Cohen's d = 1.10, p < 0.001). No significant difference in the STC‐Diet in the controls. Other: mean baseline BMI and HbA1c were 32 kg/m2 and 11%, respectively. Both decreased more in the intervention group, but differences were only significant for the outcome HbA1c, which decreased −3.09% (95% CI = −4.04 to −2.13; Cohen's d = −0.516, p = 0.012) |
| Liu et al. (2019) 85 | USA,Indiana Food pantries (pre‐packaged and client choice) | Cross‐sectional | Food banks: n = 27 Food bank users: n = 270 | Mean age (SEM): 45.7 (0.9) years Female: 149 (67%) | To determine the associations between food bank use and food security status with BMI, diet quality and chronic disease | Food bank user survey, interviewer assisted 24‐h diet recallχ 2 test; least‐squares means; logistic regression | NA | USDA 18‐item | Dietary quality: ASA24‐2014 for HEI‐2010 total and component scores | Frequency food bank use (> once a month; < once a month), BMI, self‐reported chronic disease; BMI; chronic disease | Dietary quality: visiting food banks > once a month showed significantly greater HEI‐2010 total (44.1 [SD 3.9] vs. 38.9 [SD 3.7], p = 0.03), and greater protein component score (4.7 [SD 0.4] vs. 4.3 [SD 0.4], p = 0.05), compared with visiting foodbanks < once a month). Food security was not associated with HEI‐2010 |
| Mousa and Freeland‐Graves (2019) 59 | USA, Central Texas Food pantries (pre‐packaged) | Cross‐sectional | Food banks: n = 10 Food bank users: n = 112 | Mean age (SD): 50.91 (1.17) Female: 75 (67%) | To assess impact of 2× monthly food parcels on the total nutrient intake of foodbank users | Interview; FFQ to measure past months nutrient and food intake Daily nutrient intake of base diet, food parcel and total diet estimated. Percentage of nutrients and food groups in total diet and from food parcels. Compared with USA adult DRIs and ‘Choose MyPlate’ t‐tests | NA | NA | Nutrients and energy: E, C, P, F, Sf, Uf, Tf, Ch, Fi, S, Va, Vd, Ve, Vk, Vc, Th, Ri, Ni, Vb6, Fo, Vb12, Ca, Po, Mg, Fe, Zn, Cu, Ma, Se, Na, and K Food groups: ‘choose MyPlate’ | Weight and monthly value ($) of food parcel items (per person and household) | Nutrients and energy: base diets were below DRIs for C, Fi, F and all vitamins and minerals, except Vb12 and Na, which exceeded DRIs. After food parcels, total daily diet exceeded DRIs of E, P, F, Ch, Th, Ri, Ni, Vb6, Fo, Po Vb12, Zn, Cu, Ma, Se, and Na. After food parcels, significant increases in: E, C, P, F, Ch, Fi, S, Va, Vk, Vc, Ni, Fo, Vb12, Ca, Po, Mg, Fe, Zn Se Na, and K (p < 0.05) Food parcels provided >40% of DRI for: macronutrients, E, Fi, Vc, Ri, Vb6, Vb12, Fe, Zn, Na, Po, Cu, and Se Food groups: food parcels provided >50% of whole grains, fruit, vegetable, dairy, protein, and meat portions, contributing significantly to total diet (p ≤ 0.05). Total diets lacked whole grains and dairy |
| Neter et al. (2020) 86 | Netherlands Food banks (prepackaged) | RCT | Food banks: n = 3 Food bank users: n = 163 (56 control, 28 − snacks, 25 + FV, 54 − snacks + FV) | Mean age (SD): 45.1 (10.8) years Female: 111 (68.1%) | To assess if improving the diet quality of food parcels positively impacts diet intake Intervention: crossover RCT of 10 possible sequences. Weekly provision of food parcels (control parcel,a −snacks, +FV, −snacks +FV) in two consecutive 4‐week periods | Baseline socio‐demographic questionnaire and 24‐h diet recall using USDA MPM at baseline, 4 weeks (T1)and 8 weeks (T2) Multi‐level linear regression analysis | NA | NA | Nutrients and energy: E, P, F, Sf, S, Fi, Vc, Na, and KFood groups: fruit and vegetables; grains, flour, rice; nuts, seeds, and snacks; pastry and cookies; pulses; sugar, candy, sweet filling, and sweet sauces | NA | Nutrients and energy: In +FV and −snacks + FV, mean daily C, S, fi were significantly higher, whereas F was significantly lower, compared with controls (p < 0.05). In −snacks + FV, mean daily Vc and K were significantly higher compared with controls and −snacks (p < 0.05). Food groups: mean daily intake of fruit was significantly greater in + FV and −snacks + FV interventions compared with controls. Intake of vegetables was significantly higher in −snacks + FV compared with controls Intake of pulses was significantly higher in −snacks than controls and −snacks + FV (p < 0.05) |
| Philip et al. (2018) 82 | Israel Food pantries (prepackaged) | Cross‐sectional | Food banks: n = 16 Food parcels: n = 90 Food bank users: n = 105 | Mean age (SD): 52.1 (14.5) years Female: 81 (77.1%) | To assess the nutritional quality of food parcels and the association between food parcel quality and their users’ dietary quality | Telephone survey with food bank users; staff‐reported food parcel items Based on weekly parcel provision and controlled for household size, age and gender. Compared with USA RDAs Univariate analysis; χ 2 test; t‐test; one‐way ANOVA | Nutrients: E, P, Fi, Ca, Fe, Mg, Va, Ve, Vd, Vc, Th, Ri, Ni, pa, vb6, Fo, and Vb12. Nutritional quality: HPS; NDS Food groups: fruits and vegetables | NA | Dietary quality: FFQ to devise HPS; NDS | Percentage of parcels meeting weekly household dietary requirements | Food parcel nutrition (objective 1): nutrients and energy: mean parcels provided 29.6% E, 54.9% P, and 49.9% Fi recommendations. 1.1%, 11.1%, 11.1% of parcels met household E, P, and Fi requirements, respectively. Mean parcels exceeded Va, Ri, Fo, and Vb12 recommendations, but were insufficient in Ca, Fe, Ve, Vd, Th, Ni, Pa, and Vb6. No parcels met weekly household Vd and Ca requirements Nutritional quality: mean parcel HPS and NDS were 20 (SD 20.3) and 0.3 (SD 0.3), respectively. Mean parcels provided 36.4% of recommended total portions and 14.4% of parcels met household portion guidelines Food groups: mean parcels provided 87% of recommended fruit and vegetable portions, with 25% of parcels meeting fruit and vegetable portions Food bank effectiveness (objective 2): dietary quality: food parcel nutritional quality (HPS) positively correlated with diet quality (NDS), both before and after adjusting for gender, marital status, and country of birth (Standardized: β = 0.22, p = 0.03. Overall model R 2 = 0.18, F = 4.65, p < 0.01) |
| Seligman et al. (2018) 87 | USA Food pantries (pre‐packaged) | RCT | Food banks: n = 27 Food bank users: n = 568 (285 intervention, 285 control) | Mean age (±SD): 55 (±11.4) years Female: 384 (68.3%) Condition: food bank user with HbA1c ≥7.5% | To investigate the effectiveness of a foodbank‐based diabetes intervention Intervention: diabetes self‐management education; 2× monthly food parcels Randomised into intervention or waitlist control | Participant survey and HbA1c at baseline and 6 months χ 2test; t‐test; Wilcoxon rank sums test | NA | USDA 6‐item | Food groups: fruit, vegetable, and sugar intake (California health interview survey) | Food instability; HbA1c; self‐management; satisfaction | Food insecurity: at baseline, 75.5% of participants were food insecure. Intervention participants had significant improvements in food security compared with controls (60% vs. 69.4%, RR = 0.85, 95% CI = 0.73, 0.98, p = 0.03) Food groups: intervention participants had significant increase in fruit and vegetable servings compared with controls (4.2 vs. 3.9, RD = 0.34; 95% CI = 0.34, 0.34, p = 0.04). No significant differences in sugar intake Other: food instability significantly decreased in interventions, compared with controls (54.9% vs. 70.2%, RD = 0.34; 95% CI = 0.34, 0.34, p = 0.01). No other outcomes differed; 80% preferred the food parcel compared with usual food offered |
Note: Choose MyPlate: developed by USDA to determine serving size equivalents for food groups (vegetables, fruits, refined and whole grains, milk and dairy products, beans and meat, and empty calories (solid fats, added sugars and alcohol). 59 HEI‐2010: higher scores indicate better diet quality. HEI‐2010 total score is the sum of 12 component scores. 85 HPS: adherence to “Basic Healthy Food Basket Guidelines” established by the Government of Israel's National Nutritional Security Council and Ministry of Health. These guidelines define adequate portion sizes for each of five healthy food groups (whole grains, fruits, vegetables, protein‐rich foods, fats and oils) and the recommended daily portions according to RR age and sex. HPS is a food‐based score. Division of total healthy portions by total energy is meant to account for unhealthy foods in the diet so HPS score increases as healthy portions in the diet increases but decreases with increasing total energy intake. The higher the score the higher the quality of food or diet. 82 NDS: degree to which the diet achieves the RDA for macronutrients and micronutrients, divided by the overall energy density of the food. A score of 1 indicates a food or diet that provides 100% of the RDA at the required energy intake; a score <1 indicates some degree of deficiency, and a score higher than 1 indicates possible excess. 82 Nutrient and energy outcomes key: E (energy), P (protein), C (carbohydrate), F (fat), Sf (saturated fat), Uf (unsaturated fat), Tf (trans fat), Ch (cholesterol), Fi (fibre), S (sugar), Sa (salt), K (potassium), Na (sodium) Ca (calcium), Fe (iron), Mg (magnesium), Po (phosphorus), I (iodine), Zn (zinc), Cu (copper), Se (selenium), Va (vitamin A), Ve (vitamin E), Vd (vitamin D), Vc (vitamin C), Vk (vitamin K), Th (Thiamine), Ri (Riboflavin), Ni (niacin), Ma (manganese), pa (pantothenic acid), vb6 (vitamin B6), Fo (folate), Vb12 (vitamin B12), FV (fruit and vegetables). STC‐Diet: 7‐item diet assessment for intake of: fruit/vegetables, fast food, chicken/fish/beans, chips/crackers, soda, sweets, and butter. Items are scored 1–3 and a higher score indicates better diet quality.. 84 USDA MPM: developed for collecting interviewer‐administered 24‐h recalls and includes multiple passes through the 24‐h of the previous day, during which respondents receive cues to help them remember and describe foods and drinks they consumed. Interviewers also asked participants whether the recall day was a normal day regarding dietary intake (yes/no) and a portion size photo booklet assisted in portion‐size estimation of foods and drink consumed. 86 USDA 6‐item: questions are about the food eaten in your household in the last 12 months. 83
Abbreviations: ASA24‐2014, automated self‐administered 24‐h recall version 2014 85 ; BMI, body mass index; CI, confidence interval; DRI, dietary reference intake; HEI‐2010, Healthy Eating Index‐2010; HPS, healthy portions score; NA, not applicable for the study or this systematic review; NDS, nutrient density score; RD, risk difference; RDA, recommended daily allowance; RCT, randomised controlled trial; RR, relative risk; SEM, standard error of the mean; SD, standard deviation; STC‐Diet, starting the conversion‐Diet; USDA MPM, USDA five‐step multiple‐pass method (MPM); USDA 6‐item, the United States Department of agriculture 6‐item questionnaire for food security.
Control parcel (standard food bank specific food parcel with additional non‐food items [e.g. personal care products, blanket]). −Snacks (standard food bank specific food parcel in which unhealthy snacks [e.g. chocolate, cookies, potato chips]) were replaced by staple foods (e.g. pasta, rice), with additional non‐food items (e.g. personal care products, blanket), +FV (standard food bank specific food parcel plus recommended daily amount of fruit [2] and vegetables [200 g] for all household members for 7 days), −snacks + FV (standard food bank specific food parcel in which unhealthy snacks [e.g. chocolate, cookies, potato chips]) were replaced by staple foods (e.g. pasta, rice) plus the recommended daily amount of fruit (2) and vegetables (200 g) for all household members for 7 days. 86
Table 4.
Characteristics of the 10 qualitative studies included in the mixed‐method systematic review
| Study characteristics | Population | Methodology | |||
|---|---|---|---|---|---|
| Citation | Location (country, area, foodbank) | Sample size | Aim/phenomena of interest | Method of data collection | |
| Douglas et al. (2020) 57 | Scotland Food bank (pre‐packaged) and food pantry (client choice) |
Foodbank: n = 1 Foodbank users: n = 20 |
Age range (mean): 23–83 (53) years Female: 9 (45%): 6 food bank, 3 food pantry Inclusion: physical or mental health condition/s |
What challenges face food insecure people affected by a long‐term health condition as far as their self‐care/management practices are concerned; what issues they encountered in disclosing and discussing the experience of managing their health condition with a third party such as a health care professional; and what sort of support they would wish from a health care professional | Semi‐structured interviews |
| Douglas et al. (2015) 63 | Scotland Food bank (pre‐packaged) |
Foodbank: n = 1 Foodbank users: n = 7 |
Age range: 25–50 years Female: 2 (28.6%) |
Factors that caused individuals to seek food aid from the food bank; strategies food bank clients use to try to reduce or mitigate household food insecurity; what they thought of the food they received from the food bank; and how they were incorporating it in their diets | Participant observation and semi‐structured interviews |
| Enns et al. (2020) 88 | Canada, Ottawa Food banks (pre‐packaged and client choice) |
Food banks: n = 11 (8 prepackaged; 3 client choice) Food bank users: n = 29 |
Age range (mean): 21–67 (45) years Female: 13 (44.8%) |
To explore experiences of food insecurity and accessing food banks over time and investigate the perceived impact of food banks on the participants’ lives | Semi‐structured interviews at baseline and 6 months |
| Garthwaite et al. (2015) 64 | England, Stockton‐on‐Tees Food bank (prepackaged) |
Food bank: n = 1 Food bank users: n = 42 |
Age range: 18–60 years Female: 20 (47.6%) |
To examine the relationship between ill health and food insecurity among food bank users in the UK | Participant observation and semi‐structured interviews |
| Greenthal et al. (2019) 89 | USA Food pantry (prepackaged) |
Foodbank: n = 1 Foodbank users: n = 30 |
Age category (n): <50 (7), 50–66 (16), >65 (7) years Female: 20 (67%) Inclusion: hospital patients used food pantry at least once |
To identify strengths and opportunities for improvement in programme functioning and common aspects of patients’ experiences at a hospital‐based food bank | Semi‐structured interviews |
| Hardcastle and Caraher (2021) 90 | Australia, Perth Food bank (pre‐packaged) |
Foodbank: n = 1 Foodbank users: n = 33 |
Mean age (SD): 44.12 (13.74) Female: 25 (76%) |
To investigate the perceptions of food received by users attending a food bank, and, to better understand household food choices | Semi‐structured interviews |
| Lee et al. (2020) 91 | Canada, Food bank (prepackaged) |
Food bank: n = 1 Foodbank users: n = 9 |
Age range: ≥18 years Female: 4 (44.4%) Inclusion: students used university food bank at least once in past year |
To summarise the experience of food insecurity among students attending a Canadian university food bank who were caring for children | Semi‐structured interviews |
| McKay et al. (2018) 92 | Australia, Melbourne Food bank (prepackaged) |
Foodbank: n = 1 Foodbank users: n = 70 |
Age category (n): <30 (29), 31–40 (24), 41–50 (11), ≥50 (6) years Female: 18 (25.7%) Inclusion: asylum seekers used a food bank at least twice in past year, but no longer |
To explore the experiences of asylum seekers who were entitled to use a foodbank but who had ceased attending the service, to understand why they were not using the charity, and to investigate their food‐related experiences | Telephone interviews closed and open‐ended questions |
| Neter et al. (2020) 65 | Netherlands Food banks (prepackaged) |
Foodbank: n = 7 Food bank users: n = 44 |
Age range: 20–64 years Female: 22 (50%) |
To gain insight in Dutch foodbank recipients’ perception on the content of the food parcels, their dietary intake and how the parcels contribute to their overall dietary intake | Semi‐structured focus groups of 2–6 people |
| Remley et al. (2019) 93 | USA Food pantries (prepackaged) |
Foodbank: not reported. Foodbank users: n = 612 |
Age category (%): 18–34 (18.8%), 35–54 (37%), ≥55 (44.2%) years Female: 435 (71.1%) |
To determine whether clients self‐reporting chronic health conditions in their households have unique perceptions about food banks and their ability to meet needs | Survey of closed and open‐ended questions |
Assessment of methodological quality
The methodological quality of the included studies was assessed using standardised critical appraisal tools from JBI, which were specific for the study design of each article. 81 – 83 The scores are based upon the possibility of risk of bias in the methodology, conduct, and analysis. ‘Yes’ represents a score of 1. The following maximum scores show the highest quality: RCT, 13; quasi‐experimental, 9; cross‐sectional, 9; and qualitative, 10. Uncertainties were agreed through discussion between reviewers. Methodological quality is reported, but this did not influence inclusion.
Quantitative data synthesis
The outcomes extracted from quantitative studies were, (i) the nutritional quality of food parcels: overall quality, food groups, energy and nutrients; and (ii) the effect and/or association of food bank use on the food security or dietary intake of food bank users. Heterogeneity of study designs, methodology and outcomes precluded meta‐analysis; therefore, common outcomes were narratively synthesised.
Qualitative data synthesis
Qualitative data underwent meta‐synthesis, involving generating themes that captured the views from food bank users regarding whether food banks meet their nutritional needs. Analysis followed steps adapted from thematic synthesis: (1) line‐by‐line coding; (2) developing descriptive themes; (3) generating analytical themes. 97
Mixed‐method data synthesis
A convergent segregated approach was followed for mixed‐method data synthesis. 73 This included integration of quantitative and qualitative data, linking complementary findings using configurative analysis. Mixed‐method synthesis was presented narratively and relevant outcomes, limitations, and recommendations were discussed.
RESULTS
Figure 1 details the study selection process. After removing duplicates, a total of 2189 records were identified. Following title and abstract screening, the full texts of 93 articles were reviewed for inclusion. No additional studies were identified through reference searching. Twenty‐one studies met the inclusion criteria, including 11 quantitative studies, 59 , 61 , 62 , 79 , 81 , 82 , 83 , 84 , 85 , 86 , 87 and 10 qualitative studies. 57 , 63 , 64 , 65 , 88 , 89 , 90 , 91 , 92 , 93
Quantitative study characteristics
Of 11 quantitative studies published from 2016 to 2020, three were randomised‐controlled trials (RCTs) 84 , 86 , 87 ; two were pre–post studies, 81 , 83 and six were cross‐sectional studies 59 , 61 , 62 , 79 , 82 , 85 . Six studies were conducted in the USA, 59 , 84 , 85 , 87 , 89 , 91 two in England, 61 , 79 two in the Netherlands, 62 , 86 and one in Israel 82 (Tables 2, 3).
Five studies investigated the nutritional adequacy of 563 food parcels, from 45 food banks (Table 2). All five studies compared mean nutritive values with national guidelines, controlled by household size, and four controlled analysis by intended days of parcel use, ranging 2–9 days. 61 , 62 , 82 One pre–post study, evaluating an intervention to improve parcel quality, analysed up to 2000 kcals from parcels. 81 Outcomes varied: all five reported energy and macronutrients; four reported micronutrients 61 , 79 , 81 , 82 ; three reported food groups 62 , 81 , 82 ; and one reported nutritional quality. 82 Three studies calculated the days parcels provided sufficient energy or nutrients, 61 , 62 , 79 andone study also assessed the percentage of parcels meeting household requirements 82 (Table 2).
Seven studies explored the effect of food banks on food insecurity or diet (Table 3). All seven studies investigated the impact or association of food banks on the diets of 1513 users across 96 food banks (Table 3). One study also included client‐choice food banks in addition to pre‐packaged parcels. 85 Dietary outcomes varied: four studies reported food groups; 59 , 83 , 86 , 87 two reported energy and nutrients; 59 , 86 and two assessed dietary quality. 84 , 85 Three studies evaluated the impact of 6‐month food bank based diabetes interventions, including monthly or twice monthly food parcel provision, on food bank users with diabetes or prediabetes. 83 , 84 , 87 One study evaluated an 8‐week intervention focused on improving the nutritional quality of food parcels. 86 Two studies investigated the impact of food banks on the food security of 760 food bank users across 39 food banks 83 , 87 (Table 3). One of these studies was a pre–post design 83 and the other study was a RCT. 87 Both studies were food bank‐based diabetes interventions. 83 , 87
Qualitative study characteristics
Of 10 qualitative studies published from 2015 to 2021, three were conducted in the UK 57 , 63 , 64 ; two in the USA, 89 , 93 two in Canada 88 , 91 ; two in Australia 90 , 92 ; and one the Netherlands. 65 The sample size ranged from 7 to 612, totalling 896 participants (63.4% female) (Table 4). One study recruited participants suffering health conditions, 57 another focused on Australian asylum seekers, 92 one explored a hospital‐based food bank, 89 and two studies included client‐choice food banks in addition to prepackaged parcels. 57 , 88
Five studies investigated users’ perceptions regarding food bank food. 63 , 65 , 90 , 92 , 93 The remaining five studies investigated food bank users experiences, which included views on the food provided. 57 , 64 , 88 , 89 , 91 Methodologies varied: one study administered a survey, 93 one used focus groups, 65 one used telephone interviews, 98 and seven used semistructured interviews, 57 , 63 , 64 , 88 , 89 , 90 , 91 of which two included participant observation 63 , 64 (Table 4).
Methodological quality
Results from the methodological quality assessment of the quantitative and qualitative studies included are presented below.
Quantitative studies
All three RCTs scored 7/13 using the JBI Critical Appraisal Checklist for RCTs (Table 5). The nature of the interventions meant blinding was challenging. Two studies did not describe losses at follow up or measure food bank use in controls 84 , 87 and one did not detail randomisation 86 (Table S4). Both quasi‐experimental studies scored 4/9 using the JBI Critical Appraisal Checklist for Quasi‐Experimental Studies (Table 5). Quality was limited by self‐reported outcomes, not considering additional exposures, and the precluded pre–post designs controls 81 , 83 (Table S4).
Table 5.
Critical appraisal results for the 10 quantitative studies included
| JBI Critical Appraisal Checklist for Randomised Controlled Trials | ||||||
|---|---|---|---|---|---|---|
| Citation | Ferrer et al. (2019) 84 | Neter et al. (2020) 86 | Seligman et al. (2018) 87 | |||
| Overall score | 7 | 7 | 7 | |||
| JBI Critical Appraisal Checklist for Quasi‐Experimental Studies (nonrandomised experimental studies) | ||||||
| Citation | Cheyne et al. (2020) 83 | Long et al. (2019) 81 | ||||
| Overall score | 4 | 4 | ||||
| JBI Critical Appraisal Checklist for Analytical Cross‐Sectional Studies | ||||||
| Citation | Philip et al. (2018) 82 | Fallaize et al. (2020) 61 | Hughes and Prayogo (2018) 79 | Liu et al. (2019) 85 | Mousa and Freeland‐Graves (2018) 59 | Neter et al. (2016) 62 |
| Overall score | 6 | 7 | 4 | 8 | 4 | 7 |
Scores of the six cross‐sectional studies ranged from 4 to 8 using the JBI Critical Appraisal Checklist for Analytical Cross‐Sectional Studies (Table 5). Five studies used standardised methods to assess outcomes, excluding Hughes and Prayogo's study where the inclusion criteria and methodology lacked detail 79 (Table S4). One study did not identify and consider confounders. 59 Another study was limited by self‐reported exposure. 82
Qualitative studies
The 10 qualitative studies were deemed as good quality, with congruity between the methodology, analysis, and interpretation. Scores ranged from 7 to 10 the JBI Critical Appraisal Checklist for Qualitative Research (Table 6). All studies used thematic analysis, reporting verbatim quotes. The lower scores were explained by the philosophical premises being unstated and researcher influence being unaddressed 89 , 92 (Table S4).
Table 6.
Critical appraisal results for the 10 included qualitative studies
| JBI Critical Appraisal Checklist for Qualitative Research | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Citation | Le et al. (2020) 58 | Douglas et al. (2015) 63 | Enns et al. (2020) 88 | Garthwaite et al. (2015) 64 | Greenthal et al. (2019) 89 | Hardcastle and Caraher (2021) 90 | Lee et al. (2018) 91 | McKay et al. (2018) 92 | Neter et al. (2020) 65 | Remley et al. (2019) 93 |
| Overall score | 10 | 10 | 8 | 10 | 7 | 10 | 8 | 7 | 10 | 8 |
Note: Higher scores demonstrate higher quality, with a maximum score of 10.81
Abbreviation: JBI, Joanna Briggs Institute.
Quantitative findings
Below is a narrative summary of the data from the 11 quantitative studies that were included. The findings are presented based on common outcomes for each objective of this systematic review.
Nutritional quality of food parcels
The quantitative findings of the first objective of this review, to investigate the nutritional quality of food parcels compared with adult nutritional requirements, are presented below.
Nutritional quality
The one study investigating the overall nutritional quality of food parcels reported a mean Nutrient Density Score of 0.3 (SD 0.3). A score below 1 indicates a relative deficiency in macronutrients and micronutrients. 82
Food groups
Three studies assessed FV content 62 , 81 , 82 (Table 2). One study found that a mean number parcels provided 87% of recommended FV portions, with 25% of parcels meeting requirements. 82 In the pre–post study, mean FV servings per person were 3.33 (SD 7.690), increasing significantly from 0.22 (SD 1.38, p < 0.001). 81 Preintervention, 99.9% of FV servings were apples; postintervention, parcels also included strawberries, tomatoes, onions, and other FV. 81 These were considered separately by Neter et al. (2016), who found mean weighted fruit was below (97 g [SD: 1441 g]), whereas vegetables exceeded (295 g [SD: 2700 g]) guidelines. Moreover, FVs were adequate for 1.2 and 3.7 days, respectively. 62
Neter et al. (2016) investigated other foods, including mean weight of fish, which was below guidelines (23 g [SD: 640 g]), and lasted 1.7 days. 62 The most prevalent foods were bread, vegetables, pastries, and cookies, whereas vegetarian products, eggs, and legumes were least prevalent (Table 2).
Energy
Of five studies reporting energy, requirements were exceeded in four. 61 , 62 , 79 , 81 In contrast, Philip et al. (2018) found that a mean of parcels met 29.6% of recommendations, with 1.1% meeting requirements. 82 Considering ideal days of use, energy was sufficient beyond recommended, ranging from 4–9 (recommended 3–5), 61 4.4–6.2 (recommended 2.5), 62 and 4–5 (recommended 3). 79 The pre–post study saw no changes in mean energy per person (p = 0.44). 81
Nutrients
Four of the studies reporting macronutrient content found protein and carbohydrates met or exceeded recommendations 61 , 62 , 79 , 81 ; however, one study found that parcels were below requirements. 82 When calculating ideal days of parcel use, protein was sufficient for 6–11.3 days, although other nutrient deficiencies were present 62 , 79 (Table 2). One study revealed that carbohydrates contributed the greatest proportion energy in the parcels (62.2% [SD: 5]), which is significantly greater than recommended (50%, p < 0.001). 61 In the two studies reporting sugar content, recommendations were exceeded. 61 , 79 Fat content varied across studies (Table 2).
Of the four studies reporting mean micronutrient content, parcels generally exceeded or met recommendations, 61 , 79 , 81 , 82 however this included salt and sodium exceeding requirements in the three studies reporting these. 61 , 79 , 81 In contrast, vitamin D was insufficient in the three studies assessing this, 61 , 79 , 82 and insufficiencies, including vitamin E, vitamin A, calcium, and iron, were found across other studies (Table 2). Philip et al. (2018) found that no parcels met calcium or vitamin D requirements. 82 Nutrient content did not change in the pre–post study design. 81
Effectiveness of food banks on food insecurity
The quantitative findings of the second objective of this review, to investigate the effectiveness of food banks at improving the food insecurity and dietary intake of food bank users, are presented below.
Food insecurity
Studies investigating the impact of food banks on insecurity found improvements at 6 months. 83 , 87 In the pre–post study, food insecurity significantly decreased from 68.8 to 62.5% (Pearson χ 2 = 72.6, p < 0.001). 83 In the RCT, 74.5% of participants were food insecure at baseline, with food insecurity significantly decreased in interventions, compared with controls (60% vs. 69.4%, 0.85 [0.73, 0.98] [RR (95% CIs)], p = 0.03). 87
Dietary intake
The included articles that investigated the effectiveness of food banks at improving dietary intake of food bank users are presented as findings from the cross‐sectional and intervention studies.
Cross‐sectional studies
Food parcel quality and dietary quality were positively correlated (standardised β = 0.22, p = 0.03) 82 ; also, visiting food banks over once‐per‐month was associated with significantly higher dietary quality scores, compared with visiting under once‐per‐month (4.1 [SD: 3.8] vs. 38.9 [SD: 3.7], p = 0.03). 85 Mousa and Freeland‐Graves (2019) found over 40% of nutrient and food group intake was attributed to food parcels, allowing insufficiencies to meet recommendations. 59 However, intake exceeded energy and fat yet lacked whole grains and dairy. 59
Intervention studies
Improving the nutritional quality of food parcels by adding FV and removing nutrient‐poor snacks significantly improved FV, vitamin C, and potassium intake. 86 Food bank based diabetes interventions also improved dietary intake. 83 , 84 , 87 Servings of FV significantly increased in interventions compared with controls (4.2 vs. 3.9, 0.34 [0.34–0.34] [RD (95% CIs)], p = 0.04). 87 Cheyne et al. (2020) similarly found FV consumption increased significantly postintervention (2.83 vs. 3.20, p < 0.001). 83 Assessing dietary quality, a significant improvement was seen in interventions (1.42–2.52 [95% CI] Cohen's d = 1.10, p < 0.001) compared with no change in controls. 84
Qualitative synthesis
The qualitative findings were coded into 12 descriptive themes (Figure 2). Table S5 provides details of the descriptive themes with illustrations. Five analytical themes, including recommendations, were then inferred based on the two objectives of this review (Table 7).
Figure 2.
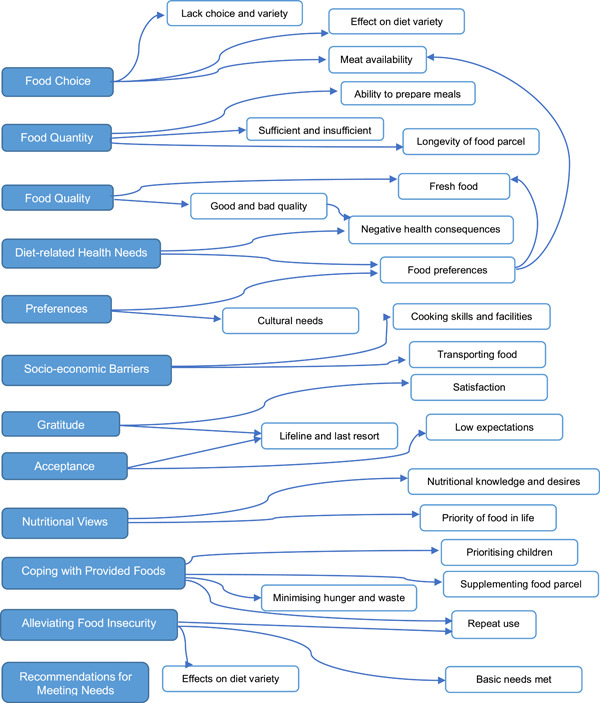
The 12 descriptive themes (blue) and codes derived by line‐by‐line coding of the 10 qualitative studies included in the systematic review. The themes and codes are reflective of the views of food bank clients regarding whether food banks meet their nutritional needs
Table 7.
The five analytical themes that were inferred from the 12 descriptive themes, including practice recommendations and illustrations
| Analytical themes | |
|---|---|
| 1 | Limited food options, particularly fresh foods and meat; and inadequate quantity to make meals and for families, limits food parcels ability to meet their users’ nutritional requirements. Increasing food variety is recommended |
| ‘Not a lot of meat options, lacking in fresh produce and dairy’ (Remley et al., 2019) | |
| ‘The problem is the food isn't worth it. We aren't interested in those foods. Food offered is not enough quantity or type of food they we interested in, for example canned food are not appropriate’ (Mckay et al., 2018) | |
| ‘We have to live from the parcel with five people, that is impossible. It is very meagre’; ‘Not all ingredients are always there for a complete meal’ (Neter et al., 2020) | |
| ‘There have been times when the fridge and cupboards were pretty bare despite going to the food bank’ (Lee et al., 2020) | |
| 2 | Food bank users recognise healthy eating; however, it is not prioritised, thus gratitude for food, regardless of its nutritional value, is apparent. Implementing consistent nutritional guidelines at food banks is advised |
| ‘I know enough about that, what I should be eating but you can't always manage to do it’ (Garthwaite et al., 2015) | |
| ‘The choices available are what they are and I must accept and choose what is available’; ‘You don't get a ton of choices, but hunger makes any choice great’ (Remley et al., 2019) | |
| ‘Well, in this crisis, I think that you just have to accept what you eat…you can't change anything’ (Neter et al., 2020) | |
| 3 | Prepackaged food parcels prevent the food from meeting health, cultural and social dietary needs. Therefore, providing choice for individual preferences is essential for mitigating food insecurity |
| ‘I found some foods that I didn't really use because I am Hindu and we didn't eat beef and sometimes like canned food or the noodles or whatever they have beef flavours…’ (Lee et al., 2020) | |
| ‘Since I became diabetic I can't eat 90% of the stuff they have there so it's not been that much help to me. The stuff they give out, I can't have’ (Enns et al., 2020) | |
| ‘At the beginning we received sweet food, salty food. But I had to ask for a letter for them, about this item. No salted food, no sweet food’ (Greenthal et al., 2019) | |
| ‘Well they give ya a lot of rice and they give ya a lot of vegetables… but if you're homeless like me it is not necessarily easy to cook those types of food’ (Douglas et al., 2015) | |
| ‘They said how to cook it but I still ain't know how to do that and I said nope, I ain't doin’ it’ (Greenthal et al., 2019) | |
| 4 | Food banks are a lifeline; however, reports of out‐of‐date food and food bank users still acquiring socially‐unacceptable strategies to reduce hunger (e.g. prioritising children, skipping meals), indicates absence of food security. Ensuring safe food, of sufficient quantity, is crucial |
| ‘So coming [to the food bank] by the end of the month is a key part of general surviving’ (Enns et al., 2020) | |
| ‘It is there when we need it. At least we are not starving to death’ (Remley et al., 2019) | |
| ‘Sometimes, the food, it's nearly expired which is scary’ (MacKay et al., 2018) | |
| ‘I eat the least so I can spare food for the rest of my family’ (Greenthal et al., 2018) | |
| ‘I feed my children first. If they are finished, I collect their leftovers in a Tupperware’ (Neter et al., 2020) | |
| 5 | Food parcels can increase dietary quantity and/or quality. However, foodbanks are insufficient for alleviating hunger, particularly for repeat and multiple‐person household users |
| ‘The content of the food parcel influences my dietary intake for 100%, because I completely rely on the food parcel’ (Neter et al., 2020) | |
| ‘Times… when you just see yourself right on ”E” [referring to ‘empty’] or close to ”E”, you come in here twice a month and it lifts you right back up to where you need to be’ (Greenthal et al., 2019) | |
| ‘It still isn't enough what [the food bank] gives you but you know I've got to make it last’ (Enns et al., 2020) | |
| ‘If I am lucky less than two days… the amount that teenage boys eat, you can probably imagine’ (Hardcastle and Caraher, 2021) | |
Mixed‐method synthesis
Based on the two objectives of this review, integrating the quantitative and qualitative findings explored whether they supported or contradicted each other. Furthermore, recommendations for practice and policy were devised (Table 8).
Table 8.
A summary of the integrated mixed‐method synthesis of the independent quantitative and qualitative study findings
| Synthesised qualitative findings | Textual description of quantitative findings | Mixed‐method synthesis with recommendations |
|---|---|---|
|
Whether food parcels meet national nutritional requirements for nutrients and food groups is inconsistent. However, food parcels do typically exceed energy, carbohydrate, sugar, and salt recommendations, yet are often insufficient in fruit, vegetables and various micronutrients, including vitamin D, calcium and iron. An intervention aiming to improve food parcel nutrition increased fruit and vegetable variety | Nutritionally inadequate food parcels can be explained by the charitable nature of food banks, often limiting the variety and quantity of food options. Improving the nutritional quality of food parcels should focus on increasing food variety, such as increasing meat, fruit and vegetable content, along with implementing nutritional guidelines, to allow consistency |
|
Participation in food bank based diabetes interventions, including prepackaged parcels significantly improved the food insecurity status and dietary quality of food bank users with diabetes. However, the incidence of food insecurity was still greater than in the general populations | Food banks struggle to meet individual dietary needs and in socially acceptable ways, thus allowing food security is limited. Positive outcomes from diabetes‐specific food parcels, and health‐related dietary needs often unmet by food banks, supports benefit of tailoring food parcels to meet individual preferences |
|
Despite food parcels contributing significantly to users diets and improving the nutritional quality of parcels having been shown to positively influence diet intake, overall dietary quality often remains insufficient | As a sole intervention, food banks do not eliminate the heightened food insecurity and poor diets of food bank users. Continuing effort to reduce diet‐related inequalities of food bank users is required, particularly among repeat and multiple‐person household users |
Whether parcels were nutritionally adequate varied across and within the quantitative and qualitative studies (Table 2; Figure 2). Cases of nutritional insufficiency were explained by qualitative reports of limited food quantity and variety. 63 , 88 , 90 , 91 The findings that sugar and salt exceeded requirements and FV were often insufficient, 62 , 63 , 79 , 81 were similarly reported qualitatively. 89 , 93 An absence of meat was reported in seven qualitative studies, 63 , 64 , 65 , 90 , 91 , 92 , 93 yet the one quantitative study investigating this outcome found 75% of parcels contained meat. 62 Despite energy exceeding requirements (Table 2), parcels were inadequate for meals and large families. 64 , 90 , 93 Any discrepancies between the findings are explained by the comparison with national guidelines in quantitative studies, whereas the qualitative studies reported the opinions and experiences of food bank users.
Intervention studies showed food banks reduce food insecurity in individuals. 83 , 87 Nevertheless, an inability to eliminate food insecurity was evident. 83 These findings were supported qualitatively as food banks allowed otherwise unachievable access to food. 63 , 90 , 93 However, cultural, social, and health‐related dietary needs were often unmet, which is explained by a limited choice of food. 57 , 65 , 90 , 91 In addition, expired food was common, yet food security requires being able to acquire safe food. 64 , 65 , 88 , 92
Aligning with qualitative findings that food banks are a lifeline for basic dietary needs, 88 quantitative studies revealed that the use of food banks use associated with improved dietary quality (Table 4). The positive dietary outcomes from diabetes‐specific interventions and after improving the nutritional quality of food parcels were unsurprising. 84 , 87 , 93 This is because traditional food parcels were often inadequate at meeting personal preferences. 63 , 88 , 89 , 93 Despite using food parcels, dietary quality often remained inadequate. 59 , 82 This was demonstrated qualitatively, as when using food banks, strategies to minimise hunger were still acquired 57 , 89 , 91 (Table 7).
The mixed‐method integration indicates benefit in improving the nutritional quality of food parcels, including implementing guidelines for consistency, increasing food variety, and tailoring food parcels to individual needs (Table 8).
DISCUSSION
This review has indicated that food parcels provided by food banks can reduce food insecurity and improve the dietary intake of their users by enabling access to food. However, food banks alone are limited in solving food insecurity and wider diet‐related inequalities. This review updates the evidence regarding the nutritional adequacy of food parcels and the mixed‐method findings support implementing policy to improve the nutritional quality of food parcels for them to meet individual dietary needs.
The first objective was to investigate whether food parcels adequately meet the nutritional requirements of food bank users. Aligning with findings from previous systematic reviews, our findings suggested that the nutritional content of food parcel varied across and within studies. In addition, nutritional inadequacies, which were the same as previous reviews, included iron, calcium, and FV. 48 , 60 Heterogeneity between the study designs, methodology, and outcomes similarly precluded meta‐analysis; thus, the results were presented narratively, and generalisation of findings is limited. This systematic review provides an expanded synthesis to previous reviews by including studies conducted in Europe and a study analysing overall nutritional quality. 61 , 62 , 79 , 82 In addition, the qualitative studies explored whether food parcels met personal dietary needs and, similar to previous research, the findings suggested nutritional insufficiencies. 23
The second objective was to investigate whether food banks improve the food security and dietary intake of food bank users, as there was previously no quantitative synthesis assessing this. 19 Although the findings indicated that using food parcels can improve food security and dietary quality, the prevalence of food insecurity remained higher than in general populations. 83 , 87 Moreover, the qualitative findings align with previous research in that the charitable food supply limits the variety, quantity, and choice of food at food banks, indicating that food insecurity persisted. 48 It is understood that the charitable nature of food banks is a key barrier to providing adequate nutrition. 98 This includes reliance on donations, insufficient food storage, a lack of nutritional guidance, and minimal links to fresh food distributors, which all hinder food quality. 98 , 99
Parcels consistently exceeded energy requirements, 61 , 62 , 79 , 81 contradicting qualitative reports of there being an insufficient quantity of food, particularly for families. 65 , 90 Based on energy content, food parcels lasted beyond recommended number of days, yet nutrients available in these were inadequate. 62 , 79 This, in addition to sugar and salt exceeding recommendations, indicates that food parcels provide energy‐dense and nutrient‐poor food. This is concerning as nutritionally poor diets and risk of obesity are greater among food bank users, and multiple‐child families are over‐represented at food banks. 2 , 50 Given that purchasing additional food is often unaffordable, exacerbated by rising food prices, acquiring food for health is challenging for those relying on food banks. 43 Inadequate vitamin D was reported in three studies. 61 , 79 , 82 Vitamin D insufficiency is common in the general population; thus, vitamin D supplementation is recommended over winter months. 100 Whether food bank users follow this guidance is unknown. Minimal provision of meat was consistent across the qualitative studies. 63 , 64 , 65 , 90 , 91 , 92 , 93 In addition to not meeting personal preferences, this is worrying as food bank users’ diets are known to lack meat and the prevalence of anaemia, most commonly caused by haem–iron deficiency, is greater when food insecure. 49 , 54 , 101
This systematic review expands on previous reviews by showing that food bank based diabetes interventions positively influenced diet intake and food insecurity. However, findings from these studies are not generalisable to all food bank users and despite improving, health‐related outcomes (for example HbA1c levels), did not always reach significance. 83 , 84 , 87 The multiple‐component interventions make distinguishing the effect of the food parcels challenging, however the diabetes‐specific parcels were preferred by participants. 87 Inclusion of diabetes‐specific studies in this review was relevant, with food parcels often inadequate for health‐related dietary needs, including diabetes. 88 The incidence of diabetes is also higher among food bank users. 55 To minimise the cyclical effects of food insecurity, poor diet and ill‐health, tailoring food parcels to health‐related dietary needs is indicated.
Findings from this systematic review demonstrate a benefit in improving the nutritional quality of food parcels. For example, Long et al.‘s pre–post study, 81 which included implementing food donation lists at food banks, showed significant increases in FV servings and food variety. Moreover, higher quality food parcels positively influenced diet intake. 82 , 86 The qualitative studies also revealed that food bank users were appreciative when parcels included fresh produce. 63 , 90 , 93 Supporting these findings from this review, a ‘no soda, no candy’ donation policy was successfully introduced in food banks in New York, which minimised the provision of these nutrient‐poor items. 102 Collaboration of food banks with fresh‐food distributors also allows provision of otherwise unaffordable items to food bank users. 60 , 98 Therefore, the current evidence supports interventions aiming to improve the variety and quality of food at food banks, particularly FV.
To enable food security, personal dietary needs, which were consistently unmet qualitatively, can be argued as important to meeting national nutritional guidelines. 103 Despite acceptance and powerlessness towards inclusion of prepackaged parcels, food bank users desired more choice to meet their preferences. 57 , 93 Although out of the scope of this review, client‐choice food banks are becoming increasingly popular and are shown to improve self‐efficacy, which is associated with reduced food insecurity. 78 Reflecting findings from previous research, 23 food parcels were also culturally inappropriate. 90 , 91 Food banks commonly recommend items to include in each food parcel. 104 Findings from this review support updating these recommendations and incorporating cultural needs.
The nature of food banks means that surplus or outdated food may be offered. 105 In this review, provision of expired food was frequently reported in qualitative studies. 64 , 65 , 88 , 92 Encouraging food bank clients to use resources, such as the ‘FoodKeeper App’, which is a phone application to educate around food quality and storage, may be beneficial. 106 The FoodKeeper App has shown to increase willingness to eat outdated foods that are still safe to consume. 107 Nevertheless, consuming outdated foods could be deemed unsafe and socially unacceptable (stigma attached), preventing food security. 2 Food provided was also often unsuitable for the cooking facilities and skills of food banks users. 63 Previous research suggests that food bank users with poor cooking facilities and nutrition knowledge use food parcel food suboptimally, limiting dietary quality. 47 , 48 , 99 Therefore, these findings support benefits of food bank‐based cooking and nutrition education interventions, which have been shown to improve the dietary quality, nutrition knowledge, cooking skills and food insecurity of food bank users. 108
Strengths and limitations
This systematic review provided a needed update to the evidence base regarding the nutritional quality of food bank parcels, but also expanded this by including additional countries, investigating the effectiveness of food banks, and exploring personal views regarding food bank food. Aspects of food insecurity can be subjective, hence the mixed‐method approach, combining quantitative data assessing the nutritional quality and effectiveness of food parcels, with the views of food bank users, was of great value, particularly for guiding public health recommendations. 73 , 74 The objectives, eligibility criteria, search strategy, and analysis were clearly stated and unlike previous reviews, 60 there were no time constraints on intervention studies. This was to ensure that all relevant evidence was captured. Including articles published from 2015 onwards ensured that there was no gap in the evidence between this review and the two previous reviews it was updating. 48 , 60 Research in public health, including food banks and food insecurity, is abundant in grey literature. 80 Therefore, searching for eligible studies in grey literature databases and relevant organisational websites prevented omission of relevant data.
We acknowledge a number of limitations. The focus on prepackaged food parcels meant that 12 articles were excluded from this review becaause the operational characteristics of the food banks were unstated. This included a cross‐sectional study, which found food donations provided by food banks significantly improve the diet quality and reduce the probability of food insecurity of adult food bank clients in the USA. 47 This potentially limited the inclusion of relevant evidence, with only two studies investigating the impact of food banks on food insecurity. 83 , 87 In addition, different dietary recommendations between high‐income countries means that international comparisons of nutritional quality are challenging. 62 , 77
The included studies which investigated the nutritional quality of food parcels assumed how long the food parcels lasted. However, the discrepancy between the nutritional content and the ideal length of use suggests inaccurate comparisons with nutritional guidelines. 61 , 62 , 79 This could explain the study conflictingly reporting inadequate energy, protein and carbohydrate. 82 Of the four intervention studies investigating the effectiveness of food banks, three studies were restricted to diabetes and the USA, limiting translation to general populations and other countries. 83 , 84 , 87 Moreover, the intervention studies being 8 weeks and 6 months long prevented investigation of lasting outcomes, limiting relevance for long‐term food bank users. 66 Only three RCTs, all moderate in methodological quality, explored the effectiveness of food banks, limiting the validity of the findings. 84 , 86 , 87
Recommendations for policy and practice
This systematic review revealed that food parcels significantly contribute to dietary intake and are repeatedly used by individuals. 59 , 89 This supports the evidence concerning chronic food bank use. 66 In addition to nutritionally poor food parcels, these findings emphasise the importance of encouraging societal action to reduce inequalities to facilitate national and international goals of eradicating food insecurity and the need for food banks. 13 , 14 , 109 Food banks do not solve the wider causes of food insecurity and there is an argument that they take this responsibility away from governments. 110 However, without policies to ensure sufficient income for adequate standards of living, combined with the economic crises related to COVID‐19, the incidence of poverty, food insecurity and food bank use are predicted to continue rising. 14 , 58 , 111
Although nutritional guidance at food banks is currently nonmandatory and limited by availability of donations, food banks that do follow nutritional recommendations are shown to have greater food variety. 112 Volunteers also support introducing nutritional guidance at food banks. 113 With food parcels variable at meeting nutritional guidelines and individual needs, this review supports implementing food bank‐based nutritional guidelines, allowing a sufficient and consistent quality of food. The findings also encourage interventions to improve the variety of food at food banks, in particular by increasing fresh produce and health condition‐specific parcels. In practice, guidelines and interventions should consider individual needs and preferences to promote food security and minimise diet‐related inequalities as well as try to reduce stigma attached to food bank use. 52 As established in some food banks, collaboration with dietitians and qualified nutritionists could ensure parcels are nutritionally adequate. 99
Recommendations for research
Further RCTs investigating the impact of food banks on food insecurity among general populations, rather than diabetes‐specific, and in countries beyond the USA, will strengthen the evidence base. Only one quantitative study investigated the adequacy of food groups beyond FV, thus additional research exploring this outcome would support increased incorporation into parcels. Food bank use is prevalent and rising among children, hence investigating and reviewing the nutritional adequacy of food parcels for children is required. Cultural preferences and social‐security programmes are country specific, which prevents generalisation of findings; 15 therefore, synthesis by country could strengthen the policy recommendations.
CONCLUSIONS
This comprehensive systematic review has updated evidence on the nutritional adequacy of food parcels provided by food banks and the effectiveness of food banks in terms of reducing food insecurity. The evidence highlights that food banks are a lifeline, particularly for those who are severely food insecure. However, it reinforces evidence that pre‐prepared food parcels struggle to meet the nutritional needs of their users. With inadequate social‐security driving food insecurity and food bank use, approaches to reduce the broader inequalities that these populations suffer is crucial. The mixed‐method findings support implementing policy to ensure adequate nutrition at food banks, including increasing food variety, choice and safety. Additionally, interventions that improve the suitability of food for individual needs and maintain the dignity of the user are supported. Therefore, these efforts could improve the experiences, food insecurity and health of those requiring food banks.
PEER REVIEW
The lead author affirms that this manuscript is an honest, accurate and transparent account of the study being reported. The reporting of this work is compliant with PRISMA guidelines. The lead author affirms that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been explained. This study is registered with PROSPERO (registration number CRD42021269065).
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
ETHICS STATEMENT
This review used only published sources of data. Ethical review by a Research Ethics Committee was not required.
AUTHOR CONTRIBUTIONS
Lucy Oldroyd, Fatemeh Eskandari and Amelia A. Lake contributed to developing the PROSPERO protocol. Lucy Oldroyd was the first reviewer and Charlotte Pratt was the second reviewer. Lucy Oldroyd conducted data analysis and led the writing of the manuscript. Amelia A. Lake and Fatemeh Eskandari provided supervision and support throughout the research project. All authors have commented on drafts of the manuscript.
Supporting information
Supporting information.
ACKNOWLEDGEMENT
This research was supported by Teesside University School of Health and Life Sciences.
Biographies
Lucy Oldroyd is a Registered Dietitian working in the NHS. She recently graduated from Teesside University, where she conducted this piece of work as part of her MSc Dietetics Course.
Fatemeh Eskandari is a nutritionist with a master's degree in Obesity and Weight Management. She is currently a PhD researcher in Nutrition and Public Health at Teesside University. Her current research interests include food insecurity, obesogenic food environments, health inequalities, Social Network Analysis, fluorides, and public health.
Charlotte Pratt is a Registered Dietitian working within the NHS. Contributions to this work were conducted as part of her MSc Dietetics Studies at Teesside University.
Amelia A. Lake, Professor, is a dietitian, a public health nutritionist and Associate Director of Fuse, The Centre for Translational Research in Public Health. Shaping public health policy, her transdisciplinary collaborations examine how the environment interacts with, and shapes behaviours around food, the broader food system, and our wider food environments.
Oldroyd L, Eskandari F, Pratt C, Lake AA. The nutritional quality of food parcels provided by food banks and the effectiveness of food banks at reducing food insecurity in developed countries: a mixed‐method systematic review. J Hum Nutr Diet. 2022;35:1202–1229. 10.1111/jhn.12994
REFERENCES
- 1. Anderson SA. Core indicators of nutritional state for difficult‐to‐sample populations. J Nutr. 1990;120:1559–1600. [DOI] [PubMed] [Google Scholar]
- 2. Bramley G, Treanor M, Sosenko F, Littlewood M. State of hunger: building the evidence on poverty, destitution, and food insecurity in the UK. The Trussell Trust. https://www.trusselltrust.org/wp-content/uploads/sites/2/2021/05/State-of-Hunger-2021-Report-Final.pdf (2021). Accessed June 2021.
- 3. O'Connell R, Owen C, Padley M, Simon A, Brannen J. Which types of family are at risk of food poverty in the UK? A relative deprivation approach. Soc Policy Soc. 2019;18:1–18. [Google Scholar]
- 4. Loopstra R, Tarasuk V. The relationship between food banks and household food insecurity among low‐income Toronto families. Can Public Policy. 2012;38:497–514. [Google Scholar]
- 5. Pool U, Dooris M. Prevalence of food security in the UK measured by the Food Insecurity Experience Scale. J Public Health (Oxf). 2021;120:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Vaughan M. National Statistics Family Resources Survey: financial year 2019 to 2020. Department for Work & Pensions. https://www.gov.uk/government/statistics/family-resources-survey-financial-year-2019-to-2020/family-resources-survey-financial-year-2019-to-2020 (2021). Accessed June 2021.
- 7. Coleman‐Jensen A, Rabbit MP, Gregory CA, Singh A. Household food security in the United States in 2019. U.S. Department of Agriculture, Economic Research Service. https://ageconsearch.umn.edu/record/305691/ (2020). Accessed June 2021.
- 8. Tarasuk V, Mitchel A. Household food insecurity in Canada 2017‐2018. Toronto: Research to identify policy options to reduce food insecurity (PROOF). https://proof.utoronto.ca (2020). Accessed June 2021.
- 9. Loopstra R. Vulnerability to food insecurity since the COVID‐19 lockdown. London: The Food Foundation. https://foodfoundation.org.uk/publication/vulnerability-to-food-insecurity-since-the-covid-19-lockdown/ (2020). Accessed June 2021.
- 10. Kent K, Murray S, Penrose B, Auckland S, Visentin D, Godrich S, et al. Prevalence and socio‐demographic predictors of food insecurity in Australia during the COVID‐19 pandemic. Nutrients. 2020;12:2682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Niles MT, Bertmann F, Belarmino EH, Wentworth T, Biehl E, Neff R. The early food insecurity impacts of COVID‐19. Nutrients. 2020;12:2096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Lauren BN, Silver ER, Faye AS, Rogers AM, Woo‐Baidal JA, Ozanne EM, et al. Predictors of households at risk for food insecurity in the United States during the COVID‐19 pandemic. Public Health Nutr. 2021;24:1–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Food and Agriculture Organization of the United Nations (FAO) . State of food security and nutrition in the world, 2020. Transforming food systems for affordable healthy diets. Rome: FAO. www.fao.org/3/ca9692en/CA9692EN.pdf (2020). Accessed June 2021.
- 14. Jenkins RH, Aliabadi S, Vamos EP, Taylor‐Robinson D, Wickham S, Millett C, et al. The relationship between austerity and food insecurity in the UK: a systematic review. EClinicalMedicine. 2021;33:100781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Loopstra R. Interventions to address household food insecurity in high‐income countries. Proc Nutr Soc. 2018;77:270–81. [DOI] [PubMed] [Google Scholar]
- 16. Berner M, Ozer T, Paynter S. A portrait of hunger, the social safety net, and the working poor. Policy Stud J. 2008;36:403–20. [Google Scholar]
- 17. Keith‐Jennings B, Llobrera J, Dean S. Links of the supplemental nutrition assistance program with food insecurity, poverty, and health: evidence and potential. Am J Public Health. 2019;109:1636–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Iacovou M, Pattieson DC, Truby H, Palermo C. Social health and nutrition impacts of community kitchens: a systematic review. Public Health Nutr. 2013;16:535–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Loopstra R. Rising food bank use in the UK: sign of a new public health emergency? Nutr Bull. 2018;43:53–60. [Google Scholar]
- 20. Riches G. Food banks and food security: welfare reform, human rights and social policy. Lessons from Canada? Soc Policy Adm. 2002;36:648–63. [Google Scholar]
- 21. Loopstra R, Lalor D. Financial insecurity, food insecurity, and disability: the profile of people receiving emergency food assistance from The Trussell Trust Food bank Network in Britain. Salisbury: The Trussell Trust. https://www.trusselltrust.org/wp-content/uploads/sites/2/2017/06/OU_Report_final_01_08_online.pdf (2017). Accessed June 2021.
- 22. Depa J, Gyngell F, Müller A, Eleraky L, Hilzendegen C, Stroebele‐Benschop N. Prevalence of food insecurity among food bank users in Germany and its association with population characteristics. Prev Med Rep. 2018;9:96–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Middleton G, Mehta K, McNaughton D, Booth S. The experiences and perceptions of food banks amongst users in high‐income countries: an international scoping review. Appetite. 2018;120:698–708. [DOI] [PubMed] [Google Scholar]
- 24. Parker MA, Mook L, Kao CY, Murdock A. Accountability and relationship‐definition among food banks partnerships. Voluntas. 2020;31:923–37. [Google Scholar]
- 25. Alkaabneh F, Diabat A, Gao H. A unified framework for efficient, effective, and fair resource allocation by food banks using an approximate dynamic programming approach. Omega. 2021;100:102300. [Google Scholar]
- 26. Food Banks Canada . HungerCount 2019. Mississauga: Food Banks Canada. https://hungercount.foodbankscanada.ca/ (2019). Accessed June 2021.
- 27. Loopstra R, Tarasuk V. Food bank usage is a poor indicator of food insecurity: insights from Canada. Soc Policy Soc. 2015;14:443–55. [Google Scholar]
- 28. Holmes E, Fowokan A, Seto D, Lear SA, Black JL. Examining food insecurity among food bank members in Greater Vancouver. J Hunger Environ Nutr. 2019;14:141–54. [Google Scholar]
- 29. Garthwaite K. Stigma, shame and ‘people like us’: an ethnographic study of foodbank use in the UK. J Poverty Soc Justice. 2016;24:277–89. [Google Scholar]
- 30. Holmes E, Black JL, Heckelman A, Lear SA, Seto D, Fowokan A, et al. “Nothing is going to change three months from now”: a mixed methods characterization of food bank use in Greater Vancouver. Soc Sci Med. 2018;200:129–36. [DOI] [PubMed] [Google Scholar]
- 31. Black J, Seto D. Examining patterns of food bank use over twenty‐five years in Vancouver, Canada. Int J Nonprofit Volunt Sect Mark. 2018;31:853–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. The Trussell Trust . Latest stats. https://www.trusselltrust.org/news-and-blog/latest-stats/ (2021). Accessed June 2021.
- 33. European Food Banks Federation (FEBA) . European Food Banks in a post COVID‐19 Europe, Belgium: European Food Banks Federation. https://www.eurofoodbank.org/ (2020). Accessed June 2021.
- 34. King A, Stewart C. Hunger report 2020: the impact of COVID‐19 on food bank use in Ontario. Toronto: Feed Ontario. https://feedontario.ca/research/hunger-report-2020/ (2020). Accessed June 2021.
- 35. Morello P. The food bank response to COVID, by the numbers. Feeding America. https://www.feedingamerica.org/hunger-blog/food-bank-response-covid-numbers (2021). Accessed June 2021.
- 36. Foodbank . Foodbank hunger report 2020: food insecurity in the time of COVID‐19. North Ryde: Foodbank Australia. https://www.foodbank.org.au/foodinsecurity/?state=au (2020). Accessed June 2021.
- 37. Public Health England . Government dietary recommendations. London: Public Health England. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/618167/government_dietary_recommendations.pdf (2016). Accessed December 2021.
- 38. The United States Department of Agriculture and The United States Department of Health and Human Services . Dietary guidelines for Americans 2020–2025. https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (2020). Accessed December 2021.
- 39. Hanson K, Connor L. Food insecurity and dietary quality in US adults and children: a systematic review. Am J Clin Nutr. 2014;100:684–92. [DOI] [PubMed] [Google Scholar]
- 40. Yau A, White M, Hammond D, White C, Adams J. Socio‐demographic characteristics, diet and health among food insecure UK adults: cross‐sectional analysis of the International Food Policy Study. Public Health Nutr. 2020;23:2602–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Kowaleski‐Jones L, Wen M, Fan J. Unpacking the paradox: testing for mechanisms in the food insecurity and BMI association. J Hunger Environ Nutr. 2019;14:683–97. [Google Scholar]
- 42. Moradi S, Mirzababaei A, Mohammadi H, Moosavian SP, Arab A, Jannat B, et al. Food insecurity and the risk of undernutrition complications among children and adolescents: a systematic review and meta‐analysis. Nutrition. 2019;62:52–60. [DOI] [PubMed] [Google Scholar]
- 43. Gregory C, Coleman‐Jensen A. High food prices increase food insecurity in the United States? Appl Econ Perspect Policy. 2013;35:679–707. [Google Scholar]
- 44. Reeves A, Loopstra R, Stuckler D. The growing disconnect between food prices and wages in Europe: cross‐national analysis of food deprivation and welfare regimes in twenty‐one EU countries, 2004–2012. Public Health Nutr. 2017;20:1414–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Jones NR, Conklin AI, Suhrcke M, Monsivais P. The growing price gap between more and less healthy foods: analysis of a novel longitudinal UK dataset. PLoS One. 2014;9:e109343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Williamson S, McGregor‐Shenton M, Brumble B, Wright B, Pettinger C. Deprivation and healthy food access, cost and availability: a cross‐sectional study. J Hum Nutr Diet. 2017;30:791–99. [DOI] [PubMed] [Google Scholar]
- 47. Mousa T, Freeland‐Graves J. Food security of food recipients of a food pantry and soup kitchen. Public Health Nutr. 2019;22:1451–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Bazerghi C, McKay F, Dunn M. The role of food banks in addressing food insecurity: a systematic review. J Community Health. 2016;41:732–40. [DOI] [PubMed] [Google Scholar]
- 49. Simmet A, Depa J, Tinnemann P, Stroebele‐Benschop N. The dietary quality of food pantry users: a systematic review of existing literature. J Acad Nutr Diet. 2016;117:563–76. [DOI] [PubMed] [Google Scholar]
- 50. Neter JE, Dijkstra SC, Dekkers A, Ocké MC, Visser M, Brouwer IA. Dutch food bank recipients have poorer dietary intakes than the general and low‐socioeconomic status Dutch adult population. Eur J Nutr. 2018;57:2747–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. The Food Foundation . The broken plate: ten vital signs revealing the health of our food system, its impact on our lives and the remedies we must pursue. The Food Foundation. https://foodfoundation.org.uk/wp-content/uploads/2019/02/The-Broken-Plate.pdf (2021). Accessed July 2021.
- 52. Marmot M, Allen J, Boyce T, Goldblatt P, Morrison J. Health equity in England: the marmot review 10 years on. London: Institute of Health Equity. https://www.health.org.uk/publications/reports/the-marmot-review-10-years-on (2020). Accessed July 2021.
- 53. Abdurahman AA, Chaka EE, Nedjat S, Dorosty AR, Majdzadeh R. The association of household food insecurity with the risk of type 2 diabetes mellitus in adults: a systematic review and meta‐analysis. Eur J Nutr. 2019;58:1341–50. [DOI] [PubMed] [Google Scholar]
- 54. Moradi S, Arghavani H, Issah A, Mohammadi H, Mirzaei K. Food insecurity and anaemia risk: a systematic review and meta‐analysis. Public Health Nutr. 2018;21:3067–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Eicher‐Miller H. A review of the food security, diet and health outcomes of food pantry clients and the potential for their improvement through food pantry interventions in the United States. Physiol Behav. 2020;220:112871. [DOI] [PubMed] [Google Scholar]
- 56. Douglas F, Machray K, Entwistle V. Health professionals' experiences and perspectives on food insecurity and long‐term conditions: a qualitative investigation. Health Soc Care Community. 2020;28:404–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Douglas F, MacIver E, Yuill C. A qualitative investigation of lived experiences of long‐term health condition management with people who are food insecure. BMC Public Health. 2020;20:1309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Leddy AM, Weiser SD, Palar K, Seligman H. A conceptual model for understanding the rapid COVID‐19–related increase in food insecurity and its impact on health and healthcare. Am J Clin Nutr. 2020;112:1162–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Mousa T, Freeland‐Graves J. Impact of food pantry donations on diet of a low‐income population. Int J Food Sci Nutr. 2019;70:78–87. [DOI] [PubMed] [Google Scholar]
- 60. Simmet A, Depa J, Tinnemann P, Stroebele‐Benschop N. The nutritional quality of food provided from food pantries: a systematic review of existing literature. J Acad Nutr Diet. 2016;117:577–88. [DOI] [PubMed] [Google Scholar]
- 61. Fallaize R, Newlove J, White A, Lovegrove JA. Nutritional adequacy and content of food bank parcels in Oxfordshire, UK: a comparative analysis of independent and organisational provision. J Hum Nutr Diet. 2020;33:477–86. [DOI] [PubMed] [Google Scholar]
- 62. Neter JE, Dijkstra SC, Visser M, Brouwer IA. Dutch food bank parcels do not meet nutritional guidelines for a healthy diet. B J Nutr. 2016;116:526–33. [DOI] [PubMed] [Google Scholar]
- 63. Douglas F, Sapko J, Kiezebrink K, Kyle J. Resourcefulness, desperation, shame, gratitude and powerlessness: common themes emerging from a study of food bank use in Northeast Scotland. AIMS Public Health. 2015;2:297–317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Garthwaite K, Collins P, Bambra C. Food for thought: an ethnographic study of negotiating ill health and food insecurity in a UK foodbank. Soc Sci Med. 2015;132:38–44. [DOI] [PubMed] [Google Scholar]
- 65. Neter JE, Dijkstra SC, Nicolaou M, Visser M, Brouwer IA. The role of food parcel use on dietary intake: perception of Dutch food bank recipients ‐ a focus group study. Public Health Nutr. 2020;23:1647–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Garratt E. Please sir, I want some more: an exploration of repeat foodbank use. BMC Public Health. 2017;17:828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Kicinski L Characteristics of short and long‐term food pantry users. Mich Sociol Rev. 2012;26:58–74. [Google Scholar]
- 68. Prayogo E, Chater A, Chapman S, Barker M, Rahmawati N, Waterfall T, et al. Who uses foodbanks and why? Exploring the impact of financial strain and adverse life events on food insecurity. J Public Health. 2017;40:676–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Roncarolo F, Bisset S, Potvin L. Short‐term effects of traditional and alternative community interventions to address food insecurity. PLoS One. 2016;11:e0150250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Wright BN, Bailey RL, Craig BA, Mattes RD, McCormack L, Stluka S, et al. Daily dietary intake patterns improve after visiting a food pantry among food‐insecure rural midwestern adults. Nutrients. 2018;10:583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–89. [DOI] [PubMed] [Google Scholar]
- 73. Lizarondo L, Stern C, Carrier J, Godfrey C, Rieger K, Salmond S, et al. Chapter 8: Mixed methods systematic reviews. In: Aromataris E, Munn Z, editors. JBI manual for evidence synthesis; 2020. https://synthesismanual.jbi.global [DOI] [PubMed]
- 74. National Institutes of Health (NIH) . Best practices for mixed methods research in the health sciences. Bethesda: National Institutes of Health; 2018.
- 75. The World Bank . High income. The World Bank Group. https://data.worldbank.org/income-level/high-income (2021). Accessed June 2021.
- 76. Watuleke J. The role of food banks in food security in Uganda: the case of the hunger project food bank, Mabel Epicentre. Current African Issues; 2015.
- 77. Scientific Advisory Committee on Nutrition (SACN) . Dietary reference values for energy. London: TSO; 2011. https://www.gov.uk/government/publications/sacn-dietary-reference-values-for-energy
- 78. Martin KS, Colantonio AG, Picho K, Boyle KE. Self‐efficacy is associated with increased food security in novel food pantry program. SSM Popul Health. 2016;2:62–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Hughes D, Prayogo E. A nutritional analysis of the trussell trust emergency food parcel. London: The Trussell Trust; 2018. https://www.trusselltrust.org/wp-content/uploads/sites/2/2018/06/Food_Parcel_Report_April_2018.pdf [Google Scholar]
- 80. Adams J, Hillier‐Brown FC, Moore HJ, Lake AA, Araujo‐Soares V, White M, et al. Searching and synthesising ‘grey literature’ and ‘grey information’ in public health: critical reflections on three case studies. Syst Rev. 2016;5:164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Long CR, Rowland B, McElfish PA. Intervention to improve access to fresh fruits and vegetables among arkansas food pantry clients. Prev Chronic Dis. 2019;16:E09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Efrati Philip D, Baransi G, Shahar DR, Troen AM. Food‐aid quality correlates positively with diet quality of food pantry users in the leket israel food bank collaborative. Front Nutr. 2018;5:123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Cheyne K, Smith M, Felter EM, Orozco M, Steiner EA, Park Y, et al. Food bank‐based diabetes prevention intervention to address food security, dietary intake, and physical activity in a food‐insecure cohort at high risk for diabetes . Pre Chronic Dis. 2020;17:1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Ferrer RL, Neira LM, De Leon Garcia GL, Cuellar K, Rodriguez J. Primary care and food bank collaboration to address food insecurity: a pilot randomized trial. Nutr Metab Insights. 2019;12:1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Liu Y, Zhang Y, Remley DT, Eicher‐Miller HA. Frequency of food pantry use is associated with diet quality among indiana food pantry clients. J Acad Nutr Diet. 2019;119:1703–12. [DOI] [PubMed] [Google Scholar]
- 86. Neter JE, Dijkstra SC, Twisk JWR, Visser M, Brouwer IA. Improving the dietary quality of food parcels leads to improved dietary intake in Dutch food bank recipients—effects of a randomized controlled trial. Eur J Nutr. 2020;59:3491–501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Seligman HK, Smith M, Rosenmoss S, Marshall MB, Waxman E. Comprehensive diabetes self‐management support from food banks: a randomized controlled trial. Am J Public Health. 2018;108:1227–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Enns A, Rizvi A, Quinn S, Kristjansson E. Experiences of food bank access and food insecurity in Ottawa, Canada. J Hunger Environ Nutr. 2020;15(4):456–72. [Google Scholar]
- 89. Greenthal E, Jia J, Poblacion A, James T. Patient experiences and provider perspectives on a hospital‐based food pantry: a mixed methods evaluation study. Public Health Nutr. 2019;22:3261–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Hardcastle S, Caraher M. The role of foodbanks in the context of food insecurity: experiences and eating behaviours amongst users. Appetite. 2021;163:105208. [DOI] [PubMed] [Google Scholar]
- 91. Lee S, Ball GD, Farmer A, Willows ND. Exploring the experience of food insecurity among university students caring for children: a qualitative descriptive study. J Hunger Environ Nutr. 2020;15:360–71. [Google Scholar]
- 92. McKay FH, Bugden M, Dunn M, Bazerghi C. Experiences of food access for asylum seekers who have ceased using a food bank in Melbourne, Australia. Br Food J. 2018;120:1708–21. [Google Scholar]
- 93. Remley D, Franzen‐Castle L, McCormack L, Eicher‐Miller HA. Chronic health condition influences on client perceptions of limited or non‐choice food pantries in low‐income, rural communities. Am J Health Behav. 2019;43:105–18. [DOI] [PubMed] [Google Scholar]
- 94. Lockwood C, Munn Z, Porritt K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta‐aggregation. Int J Evid Based Healthc. 2015;13:179–87. [DOI] [PubMed] [Google Scholar]
- 95. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. JBI manual for evidence synthesis; 2020. https://synthesismanual.jbi.global
- 96. Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L. Chapter 3: Systematic reviews of effectiveness. In: E Aromataris, Z Munn, editors. JBI manual for evidence synthesis; 2020. https://synthesismanual.jbi.global
- 97. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Loopstra R, Goodwin S, Goldberg B, Lambie‐Mumford L, May J, Williams A. A survey of food banks operating independently of The Trussell Trust food bank network. Independent Food Aid Network. https://www.foodaidnetwork.org.uk/independent-food-bank-survey (2019). Accessed June 2021.
- 99. Thompson C, Smith D, Cummins S. Understanding the health and wellbeing challenges of the food banking system: a qualitative study of food bank users, providers and referrers in London. Soc Sci Med. 2018;211:95–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Scientific Advisory Committee on Nutrition (SACN) . Vitamin D and health. https://www.gov.uk/government/groups/scientific-advisory-committee-on-nutrition (2016). Accessed July 2021.
- 101. DeLoughery T. Iron deficiency anemia. Med Clin. 2017;101:319–32. [DOI] [PubMed] [Google Scholar]
- 102. Handforth B, Hennink M, Schwartz M. A qualitative study of nutrition‐based initiatives at selected food banks in the feeding America network. J Acad Nutr Diet. 2013;113:411–5. [DOI] [PubMed] [Google Scholar]
- 103. Fuller E, Bankiewicz U, Davies B, Mandalia D, Stocker B. The food & you survey wave 5 combined report for England, Wales and Northern Ireland. London: Food Standards Agency. https://www.food.gov.uk/sites/default/files/media/document/food-and-you-wave-5-combined-report.pdf (2019). Accessed June 2021.
- 104. The Trussell Trust . What's in a food parcel. https://www.trusselltrust.org/get-help/emergency-food/food-parcel/ (2021). Accessed July 2021.
- 105. Tarasuk V, Eakin J. Charitable food assistance as symbolic gesture: an ethnographic study of food banks in Ontario. Soc Sci Med. 2003;56:1505–15. [DOI] [PubMed] [Google Scholar]
- 106. The United States Department of Health and Human Services . FoodKeeper App. https://www.foodsafety.gov/keep-food-safe/foodkeeper-app (2019). Accessed December 2021.
- 107. Gong Z, Su LYF, Zhang JS, Chen T, Wang YC. Understanding the association between date labels and consumer‐level food waste. Food Qual Pref. 2022;96:104373. [Google Scholar]
- 108. An R, Wang J, Liu J, Shen J, Loehmer E, McCaffrey J. A systematic review of food pantry‐based interventions in the USA. Public Health Nurt. 2019;22:1704–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Marmot M, Allen J, Goldblatt P, Herd E, Morrison J Build back fairer: the COVID‐19 marmot review. The pandemic, socioeconomic and health inequalities in England. London: Institute of Health Equity. https://www.health.org.uk/publications/build-back-fairer-the-covid-19-marmot-review (2020). Accessed July 2021.
- 110. Tarasuk V, Dachner N, Hamelin AM, Ostry A, Williams P, Bosckei E, et al. A survey of food bank operations in five Canadian cities. BMC Public Health. 2014;14:1234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Power M, Doherty B, Pybus K, Pickett K. How COVID‐19 has exposed inequalities in the UK food system: the case of UK food and poverty. Emerald Open Research. 2020;2:11. [Google Scholar]
- 112. Long CR, Narcisse MR, Rowland B, Faitak B, Caspi CE, Gittelsohn J, et al. Written nutrition guidelines, client choice distribution, and adequate refrigerator storage are positively associated with increased offerings of Feeding America's Detailed Foods To Encourage (F2E) in a large sample of Arkansas food pantries. J Acad Nutr Diet. 2020;120:792–803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Cooksey‐Stowers K, Read M, Wolff M, Martin KS, McCabe M, Schwartz M. Food pantry staff attitudes about using a nutrition rating system to guide client choice. J Hunger Environ Nutr. 2019;14:35–49. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.