

Abstract
Introduction
Since July 2021, a worldwide shortage of verteporfin (Visudyne®) occurred: an essential medicine required for photodynamic therapy (PDT). PDT with verteporfin has a broad range of indications in ophthalmology, including chronic central serous chorioretinopathy, polypoidal choroidal vasculopathy and choroidal haemangioma. For these disorders, PDT is either the first‐choice treatment or regarded as a major treatment option.
Materials and methods
A questionnaire was sent to key opinion leaders in the field of medical retina throughout the world, to assess the role of PDT in their country and the effects of the shortage of verteporfin. In addition, information on the application of alternative treatments during shortage of verteporfin was obtained, to further assess the impact of the shortage.
Results
Our questionnaire indicated that the shortage of verteporfin had a major impact on ophthalmic care worldwide and was regarded to be a serious problem by most of our respondents. However, even though there is ample evidence to support the use of PDT in several chorioretinal diseases, we found notable differences in its use in normal patient care throughout the world. Various alternative management strategies were noted during the verteporfin shortage, including lowering the dose of verteporfin per patient, the use of alternative treatment strategies and the use of a centralized system for allocating the remaining ampoules of verteporfin in some countries.
Conclusion
The shortage of verteporfin has had a large effect on the care of ophthalmic patients across the world and may have resulted in significant and irreversible vision loss. Mitigation strategies should be developed in consultation with all stakeholders to avoid future medication shortages of verteporfin and other unique ophthalmic medications. These strategies may include mandatory stock keeping, compulsory licensing to an alternative manufacturer or incentivizing the development of competition, for example through novel public‐private partnerships.
Keywords: age‐related macular degeneration, central serous chorioretinopathy, choroidal haemangioma, photodynamic therapy, polypoidal choroidal vasculopathy, verteporfin
Introduction
In 2021, there was a worldwide shortage of verteporfin (Visudyne®, Cheplapharm Arzneimittel GmbH, Greifswald, Germany). Verteporfin is a photosensitizing, pharmacological agent used to perform ocular photodynamic therapy (PDT) in patients with choroidal neovascularization (CNV), central serous chorioretinopathy (CSC), polypoidal choroidal vasculopathy (PCV) and several other chorioretinal diseases.
The constrained supply of verteporfin was caused by a manufacturing problem in a factory situated in the United States, which is apparently the single producer of verteporfin worldwide. Recent reports suggest that the medication will not be available until the first quarter of 2022 (Cheplapharm Arzneimittel GmbH 2021; European Medicines Agency 2021b).
This article highlights the history of the use of PDT in ophthalmology and in other medical fields, provides the current evidence of its efficacy for ophthalmic indications and describes the impact of its decreased availability on ophthalmic patient care in different regions in the world. In addition, we describe the results of a questionnaire among international experts in the field of ophthalmic use of PDT on the variability of PDT use worldwide for common treatment indications. Moreover, we suggest possible solutions, which may prevent similar problems in the future.
History of Photodynamic Therapy
PDT is the activation of a photosensitive drug using laser treatment, which creates free oxygen radicals that induce a local cytotoxic reaction (Kwiatkowski et al. 2018). The discovery of this effect was attributed to Von Tappeiner et al. (1903) in the beginning of the 20th century. These researchers were working with fluorescent dyes, when subsequent illumination proved to have destructive effects on the studied microorganisms, called paramecia. However, already in the 16th century this ‘photodynamic’ reaction was observed in patients suffering from porphyria (Hurst 1982), a group of diseases that result from a deficiency of one of the enzymes involved in the haem synthesis pathway. In these patients, accumulation of the metabolites of intermediates in this pathway, known as porphyrins, can cause damage to organs or skin tissue, especially when exposed to sunlight (Batlle 1993). Various photosensitizers that are used today are derived from porphyrins, including the benzoporphyrin derivative verteporfin (Santosa & Limantara 2008). Following Von Tappeiner's discovery, Figge et al. (1948) recognized the tendency of some photosensitizers to accumulate in neoplastic tissues in 1948. This affinity of photosensitizers for tumour cells and the tumour stroma was utilized to explore PDT in different malignancies. A photosensitizer was injected either intraperitoneally or intravenously, and the tumour was subsequently illuminated with a light source to activate the photosensitizer locally and destroy the cancer (Diamond et al. 1972). However, the use of PDT in oncology did not become a part of the standard of care until the 1970s. Currently, oncological indications for PDT are mainly cutaneous malignancies, but PDT also serves a purpose in several other types of cancer, facilitating tumour resolution while sparing the function of normal tissues (Dolmans et al. 2003; Nyst et al. 2009; Allison et al. 2010; Ozog et al. 2016).
The early photosensitizers had to be illuminated for several hours to achieve the desired effect. In addition, the half‐life of these photosensitizers was so long that patients were required to protect themselves from sunlight for several weeks after injection of the photosensitizer to prevent skin damage. The discovery of various new photosensitizers over the years, including agents with shorter half‐lives and shorter time of required illumination, has allowed PDT to be used for a variety of new purposes, including retinal diseases (Allison et al. 2010). Verteporfin is one of these photosensitizers.
Photodynamic Therapy in Ophthalmology
Nearly a century after the discovery of the basic concept of PDT, PDT was introduced in ophthalmology in 2000, after the TAP Study reported PDT with verteporfin to be effective for slowing vision loss in certain forms of subfoveal choroidal neovascularization (CNV) due to age‐related macular degeneration (AMD) (TAP study group 1999). This study demonstrated PDT's utility could extend beyond treating malignant tissues to targeting other fast‐growing vascular cell structures as found in the new blood vessels in AMD. For several years, PDT was the standard of care in the management of AMD. However, PDT has been found to be inferior to intravitreal injections of anti‐vascular endothelial growth factor (VEGF) in the ANCHOR study (Brown et al. 2009). Thus, although verteporfin is registered for the treatment of CNV caused by either AMD or pathologic myopia (European Medicines Agency 2020), in current practice, indications for PDT with verteporfin in ophthalmology have shifted to PCV, a particular subtype of AMD, and to off‐label use for conditions such as CSC and various types of ocular haemangioma (van Dijk et al. 2020; Raizada & Naik 2021). PDT is also sometimes used in choroidal melanomas (Quhill et al. 2021) and retinal angiomatous proliferations (Saito et al. 2012), but these conditions are rare and will therefore not be discussed in this article.
A standard treatment with PDT requires a 10‐minute intravenous infusion of verteporfin with a dosage of 6 mg/m2 body surface, diluted in 30 ml of infusion fluid. At 15 minutes after the start of the infusion, verteporfin is activated with a diode laser that uses 689 nm wavelength light. At the recommended light intensity of 600 mW/cm2, the spot of interest is illuminated for 83 seconds to achieve the required light dosage of 50 J/cm2 (European Medicines Agency 2020).
Photodynamic therapy in central serous chorioretinopathy
CSC is a disease originating in the choroid, in which specific choroidal abnormalities (thickening (‘pachychoroid’), venous congestion and leakage) are associated with serous subretinal fluid (SRF) accumulation, generally occurring in the macula. If the fluid does not resolve, subsequent damage to the retinal pigment epithelium (RPE) may occur (Cheung et al. 2019; van Rijssen et al. 2019b; van Dijk & Boon 2021; Spaide et al. 2022). This macular SRF can cause blurred vision, loss of contrast sensitivity, metamorphopsia and micropsia. Male gender, type‐A personalities, psychiatric disorders, steroid exposure and sleep disturbances are risk factors, and first, symptoms usually occur in patients aged between 30 and 50 years old. In the case of persistent (>3 months) SRF, when relapses occur, and when the patient has other signs of chronicity on multimodal imaging, such as more diffuse atrophic RPE alterations (DARA), treatment is often advised (Mohabati et al. 2018; van Rijssen et al. 2019b).
Various forms of treatment have been used for CSC, including focal thermal laser, micropulse laser treatment, oral eplerenone, intravitreal injections with anti‐VEGF agents and PDT. For PDT, several studies have shown that altering the standard parameters for PDT treatment may give results similar to those achieved when standard settings are used (van Rijssen et al. 2019b; van Dijk et al. 2020). For example, the administered dosage of verteporfin in PDT can be reduced to 3 mg/m2 (referred to as ‘half‐dose PDT’), or alternatively, the laser settings can be altered to emit light at a dosage of 25 J/cm2 (referred to as ‘half‐fluence PDT’). The available studies suggest that these reduced settings have a similar treatment effect, while reducing the risk of side effects (van Rijssen et al. 2019b).
In the European PLACE trial, the first large prospective treatment trial for chronic CSC, Van Dijk et al. showed that half‐dose PDT is superior to high‐density subthreshold micropulse laser treatment in chronic CSC patients, both in terms of functional and anatomical outcome measures (van Dijk et al. 2018). In the PLACE trial, complete resolution of SRF occurred in 67.2% of PDT‐treated patients at 7 to 8 months after treatment, as compared to only 28.8% of micropulse laser‐treated patients (van Dijk et al. 2018). Additionally, a significantly larger increase in retinal sensitivity on microperimetry was seen in the PDT‐treated eyes. Furthermore, a significantly higher proportion of PDT‐treated chronic CSC patients in the PLACE trial had an improvement in functional parameters in comparison with the micropulse laser‐treated group. This was also the case after crossover treatment to half‐dose PDT after unsuccessful micropulse laser, but not vice versa, as shown in the REPLACE trial (van Rijssen et al. 2020). This superior treatment effect of half‐dose PDT was seen regardless of the presence of focal or more extensive leakage on fluorescein angiography (van Rijssen et al. 2019a). Recently, van Rijssen et al. (2021) have shown in another large prospective treatment trial from the Netherlands, the SPECTRA trial, that half‐dose PDT is also superior to the oral mineralocorticoid receptor (MR) antagonist eplerenone for the treatment of chronic CSC. The SPECTRA study used similar outcome measures as the PLACE trial and showed a complete resolution of SRF in 87% of PDT‐treated patients, as compared to only 17% of eplerenone‐treated patients. In addition, a significantly higher increase in retinal sensitivity on microperimetry was seen in the PDT‐treated group. Similarly, low rates of SRF resolution with eplerenone treatment were found in the VICI trial, in which eplerenone treatment was compared with placebo in chronic CSC patients (Lotery et al. 2020). These and other (retrospective) publications support a prominent role of PDT with reduced settings in the treatment of chronic CSC, for which no alternative treatment is presently available (van Rijssen et al. 2019b).
Photodynamic therapy in polypoidal choroidal vasculopathy
PCV is a disease manifestation in which CNV is associated with sub‐RPE aneurysmal vascular dilations (Dansingani et al. 2018; Chaikitmongkol et al. 2020; Cheung et al. 2021). The origin of the name is not entirely clear, but may come from the resemblance of these ‘polyps’ to either intestinal polyps or animals called freshwater and saltwater polyps. PCV may cause haemorrhages and leakage of SRF and lipoproteins, and, consequently, loss of visual acuity. They may be present in patients with neovascular AMD, but they can also present in other diseases associated with CNV including CSC. In Asian populations, between 22.3 and 61.6% of patients diagnosed with neovascular AMD have evidence of PCV, as compared to between 8 and 13% of White patients of European descent (Wong et al. 2016). As a result of this higher prevalence in Asian patients, most of the available data on clinical characteristics and treatment in PCV come from Asian populations. The pathophysiology and its possible correlation with AMD remain a subject of discussion. A recently proposed classification of subtypes of PCV may resolve the discussion by suggesting different aetiologies in different PCV cases (Van Dijk et al. 2021). Van Dijk et al. (2021) suggested differentiating the following subtypes of PCV: (1) PCV within the context of AMD, characterized by the presence of at least 5 macular drusen; (2) PCV without the presence of drusen, but with a non‐polypoidal CNV or a branching vascular network, defined as a network of intertwining choroidal vessels supplying the polyp with blood; (3) Idiopathic PCV without the presence of drusen, a branching vascular network or a non‐polypoidal CNV. PCV is not easily recognized due to its resemblance to a type 1 CNV in ‘classic’ neovascular AMD. However, it is important to establish this diagnosis, as PCV patients often do not respond as well to monotherapy with anti‐VEGF as ‘classic’ AMD patients. Indocyanine green angiography (ICGA) is considered the gold standard for diagnosing PCV, but this imaging technique is not available to every ophthalmologist. Therefore, recent studies have focused on developing diagnostic criteria based on other imaging modalities, including the appearance of a sharp‐peaked RPE detachment with a hyperreflective ring under it on optical coherence tomography or a red‐orange nodule on colour fundus photography (Cheung et al. 2021). When the diagnosis is confirmed using multimodal imaging (including ICGA), PDT with or without intravitreal anti‐VEGF injections may be considered, based on several clinical treatment trials. In the EVEREST trial, conducted by Koh et al., it was shown that combination therapy of anti‐VEGF and full‐dose PDT was superior to anti‐VEGF monotherapy, with regard to polyp closure rate (77.8% versus 28.6%) at 6 months after treatment (Koh et al. 2012). The follow‐up study, EVEREST II, described the longer‐term follow‐up: at 24 months after treatment, combination therapy of PDT and anti‐VEGF compared with anti‐VEGF monotherapy showed a greater gain in best‐corrected visual acuity (9.6 versus 5.5 letters) and a better polyp closure rate (56.6% versus 26.7%) (Lim et al. 2020). Additionally, the EVEREST II cohort showed that fewer anti‐VEGF injections were required when combination therapy was performed (median of 6 versus 12 after 24 months). However, another study has shown anti‐VEGF monotherapy to yield a good response in 85% of (predominantly Asian) patients (Lee et al. 2018). Generally, full‐dose PDT is used in PCV, but half‐dose PDT may be equally effective (Wong et al. 2018). In summary, PDT may be considered in patients with PCV, especially when the response to anti‐VEGF alone is inadequate.
Photodynamic therapy in choroidal haemangioma
Choroidal haemangiomas are benign vascular tumours that occur in the posterior pole of the eye. Two forms exist, which are diffuse choroidal haemangioma and circumscribed choroidal haemangioma. The diffuse form predominantly occurs in patients with Sturge–Weber syndrome who usually have a port‐wine stain on the same side of the face and a diffuse thickening of the choroid. It is present from birth and may manifest at a young age.
Circumscribed choroidal haemangiomas are usually diagnosed at an older age and are characterized by a more localized tumour. In both forms, the leakage of these tumours can cause intra‐ and subretinal fluid and may eventually lead to an exudative retinal detachment, resulting in a severe reduction in visual acuity (Schmidt‐Erfurth et al. 2002). Treatment with conventional laser generally leads to resolution of SRF and a temporary improvement in visual acuity, but long‐term results show the visual acuity to deteriorate further in the majority of cases (Anand et al. 1989). Although no large studies have been conducted on the efficacy of PDT in these tumours, the available evidence suggests a good response to treatment with PDT (Boixadera et al. 2009; Sachdeva et al. 2010). A review of the literature has also deemed PDT to be the preferred treatment (Tsipursky et al. 2011). Various treatment protocols exist for PDT in ocular haemangiomas, for example using a bolus of verteporfin, or an increased fluence of 100 J/m2, compared with a standard fluence of 50 J/m2. In all cases, a full dose of 6 mg/m2 verteporfin is used. Various forms of radiotherapy, including low‐dose (20 Gy) external beam radiotherapy are also used in large choroidal haemangioma, with good effect. However, radiotherapy may induce side effects to ocular and surrounding tissues (Karimi et al. 2015).
Thus, we have described a range of ocular diseases that respond well to PDT with verteporfin. For some diseases, this is in fact the only effective treatment option.
Current Situation and Management in the Netherlands
At a national population of about 17.5 million people, approximately 700 Dutch patients are treated yearly with PDT (Nederlands Oogheelkundig Gezelschap 2021). This consists of 80–85% of chronic CSC patients, 10–15% of PCV patients and 5% of other indications, including choroidal haemangioma. In the second half of 2021, supplies of verteporfin were so restricted that only 10–15% of cases where PDT was indicated could be treated with the remaining stock that was available in the Netherlands. This unwanted situation was covered by several major national news media. The Dutch Ophthalmological Society and Medical Retina Working Group therefore established a national committee, consisting of retina specialists commonly performing PDT treatment from all PDT expertise centres within the country, to allocate the remaining supply of verteporfin based on a prioritization scheme (Nederlands Oogheelkundig Gezelschap 2021; Werkgroep Medische Retina van het Nederlands Oogheelkundig Gezelschap 2021). This was done to ensure that PDT was available to patients that were most at risk of a further deterioration of visual function and irreversible changes without PDT. The committee came together once every 4 weeks to evaluate the history and multimodal imaging of cases nominated by their treating ophthalmologists throughout the country.
Several criteria were set to prioritize cases (Werkgroep Medische Retina van het Nederlands Oogheelkundig Gezelschap 2021). For example, children with choroidal haemangioma and (functionally) monocular patients were prioritized (see full list of criteria in Table 1). Inevitably, this resulted in 85–90% of cases in whom a suboptimal treatment had to be given or treatment had to be deferred until verteporfin was available again.
Table 1.
Prioritization criteria in the allocation of remaining ampoules of verteporfin in the Netherlands
| Patients with 1 functional eye, or a maximum visual acuity of 20/40 Snellen equivalent in the other eye, and… |
| Choroidal haemangioma with subretinal fluid in the macula |
| Central serous chorioretinopathy with optical coherence tomography documented persistent subfoveal fluid, where the leakage point is not treatable with focal laser |
| Polypoidal choroidal vasculopathy with foveal intraretinal or subretinal fluid or foveal hard exudates, deteriorating despite 4‐weekly treatment with intravitreal anti‐vascular endothelial growth factor (VEGF) injections and despite switching to aflibercept. Not treatable with focal laser |
| Non‐inflammatory choroidal neovascularization with subfoveal intraretinal or subretinal fluid with a height of >200 μm or foveal hard exudates, deteriorating despite 4‐weekly treatment with intravitreal anti‐VEGF injections and despite switching to aflibercept. Not treatable with focal laser |
| Children under the age of 18 with a choroidal haemangioma with subretinal fluid in the macula |
anti‐VEGF = anti‐vascular endothelial growth factor.
Although there are no exact numbers to back this up, it can be assumed that there are many patients whose visual function was impacted due to this shortage and that some may have suffered irreversible damage to their vision. In addition, when the supply of verteporfin is restored, PDT treatments will likely have to be performed at a higher volume than previously, because of postponement of treatments in the previous period. Altogether, this shortage of verteporfin poses a serious problem. Drug shortages are not a rare occurrence, as 1492 drug shortages were reported for instance in the Netherlands alone in 2019 (Koninklijke Nederlandse Maatschappij ter Bevordering der Pharmacie 2020). In this report, a drug shortage was defined as a national unavailability, which was expected to last for 14 days or more.
Current Situation and Management in the Rest of the World
The shortage of verteporfin affects patients and the ophthalmic community worldwide. However, the impact on patients may not be the same in every country. Despite current evidence of the efficacy of verteporfin‐assisted PDT in the aforementioned diseases, guidelines on treating these diseases may differ per country, or even per region within a country, or be absent altogether (Mehta et al. 2017). Whereas PDT is the standard of care for patients with chronic CSC in the Netherlands, it might not even be available or used for this indication in other parts of the world. We took the opportunity of this severe situation to assess the ‘normal’ standard of care across the world when it comes to treating several retinal diseases, as well as to evaluate the effect of the unavailability of verteporfin. We contacted several key opinion leaders in the medical retina field throughout Europe, Asia and the United States who were known to the initiators of this article and asked them to complete a questionnaire to comment on the following themes: what is the role of PDT in ophthalmology in your country in the normal situation and how has the current shortage affected your patient care? (See Appendix S1 for the full list of questions).
Results of the International Questionnaire on the Role of PDT and Effect of Current Verteporfin Shortage
The questionnaire was sent to 18 retina experts who practice in the United Kingdom, France, Germany, Israel, Switzerland, Spain, Italy, Denmark, Sweden, the Netherlands, Singapore, Japan and the United States. We received 15 answers from retinal specialists from 12 different countries (response rate 83%). All the questionnaires were performed between December 2021 and January 2022.
There were notable differences between countries in the use of PDT in the normal situation (See Table 2). For chronic CSC, the treatment of choice for most countries was PDT. For Italy, it was reported that PDT was given in approximately 50% of cases, while the rest would be treated with conventional laser treatment, MR antagonists, nutritional supplements or acetazolamide tablets. For the United States, it was reported that 25–50% of chronic CSC cases receive PDT, while a larger proportion receive MR antagonists. For Japan, it was reported that conventional laser treatment was performed if dye leakage was observed on fluorescein angiography. For PCV, both anti‐VEGF and anti‐VEGF + PDT were chosen by most specialists as treatment of choice. In about half of the countries only 0–20% of PCV patients were treated with additional PDT, whereas in the other half of countries, roughly 20–50% of cases were treated with PDT. For choroidal haemangioma, the consensus was that 80–100% of cases received PDT. For ‘classic’ neovascular AMD, additional PDT was only applied when patients responded poorly to anti‐VEGF monotherapy (generally 1% of cases).
Table 2.
Use of photodynamic therapy in the normal situation per country
| What is the primary treatment in your country in the normal situation? | ||||||||
|---|---|---|---|---|---|---|---|---|
| What percentage of patients do you estimate is treated with PDT in your country in the normal situation? | ||||||||
| Chronic CSC | PCV | Choroidal haemangioma | Neovascular AMD | |||||
| Country | Primary treatment | % treated with PDT | Primary treatment | % treated with PDT | Primary treatment | % treated with PDT | Primary treatment | % treated with PDT |
| Denmark | PDT | 100% | Anti‐VEGF or Anti‐VEGF + PDT | 30% | PDT | 100% | Anti‐VEGF | <1% |
| France | PDT | 75% | Anti‐VEGF | 5% | PDT | 80% | Anti‐VEGF | 1% |
| Germany | PDT | 80% | Anti‐VEGF | 5% | PDT | 90% | Anti‐VEGF | <5% |
| Israel | PDT | 90% | Anti‐VEGF or Anti‐VEGF + PDT | 5–10% | PDT | 90–100% | Anti‐VEGF | 0% |
| Italy | PDT | 50% | Anti‐VEGF + PDT | 20% | PDT | 80% | Anti‐VEGF | 1% |
| The Netherlands | PDT | 90% | Anti‐VEGF + PDT | 50% | PDT | 95% | Anti‐VEGF | 1% |
| Sweden | PDT | 75–100% | Anti‐VEGF | 20–30% | PDT | 80% | Anti‐VEGF | 0% |
| Switzerland | PDT | 100% | Anti‐VEGF or Anti‐VEGF + PDT | 35–40% | PDT | 100% | Anti‐VEGF | 2% |
| United Kingdom | PDT | 80% | Anti‐VEGF + PDT | 50% | PDT | 70% | Anti‐VEGF | 5% |
| United States | MR antagonist (1st) or PDT (2nd) | 25–50% | Anti‐VEGF or PDT | 5–20% | PDT | 50–80% | Anti‐VEGF | 0–10% |
| Japan | PDT or conventional laser treatment | 20% | Anti‐VEGF or Anti‐VEGF + PDT | 5% | Conventional laser treatment or PDT | 15% | Anti‐VEGF or Anti‐VEGF + PDT | 2% |
| Singapore | PDT or conventional laser treatment | 90% | Anti‐VEGF or Anti‐VEGF + PDT | 30% | PDT | 70% | Anti‐VEGF | <5% |
AMD = age‐related macular degeneration; anti‐VEGF = anti‐vascular endothelial growth factor; CSC = central serous chorioretinopathy; MR = mineralocorticoid receptor; PCV = polypoidal choroidal vasculopathy; PDT = photodynamic therapy.
In most countries, it was reported that no more supply of verteporfin was available at the time when the questionnaire was completed. Respondents from France, the Netherlands and Singapore mentioned that they still had a limited supply/stock of verteporfin. The number of patients treated in the normal situation and during the shortage is shown per respondent in Table 3. Surprisingly, our respondent in Japan and two out of three respondents from the United States declared that they have had no major problems in their supply of verteporfin. A possible explanation may be that remaining batches of verteporfin had already been released in the United States and Japan around the time of the production problems. However, our respondents from the United States have also informed us that PDT is performed much less frequently in the United States, and therefore, a shortage will not occur as swiftly as in other countries. Upon further inquiry, one of our respondents has stated that retinal specialists in the United States are aware of the evidence supporting the role of PDT in retinal disease, but that its use is limited due to insurance coverage and lack of FDA label. Most ophthalmologists no longer own the laser device that is required for performing this treatment and buying new machines is challenging, as well as repairing existing machines. Thus, referral to another centre is the first hurdle to overcome. Moreover, the need for insurance verification and often additional out‐of‐pocket expenses for the patient are barriers to use. For Japan, we have no information that may explain why their supplies of verteporfin were not interrupted.
Table 3.
Absolute number of patients treated with photodynamic therapy per year in the clinic of the respondent, both in the normal situation and during the verteporfin shortage
| What is the approximate number of patients treated with PDT in your centre per year? | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Chronic CSC | PCV | Choroidal haemangioma | Neovascular AMD | ||||||
| Country and respondent | Is PDT still available? | Normal situation | Shortage situation | Normal situation | Shortage situation | Normal situation | Shortage situation | Normal situation | Shortage situation |
| Denmark | No | Unknown | 0 | Unknown | 0 | Unknown | 0 | 2 | 0 |
| France | Yes, but limited | 10 | 2 | 5 | 0 | 3 | 1 | 5 | 0 |
| Germany | No | 40 | 0 | 5 | 0 | 8 | 0 | 0 | 0 |
| Israel – Respondent #1 | No | 27 | 0 | 2 | 0 | 6 | 0 | 0 | 0 |
| Israel – Respondent #2 | No | 50–60 | 8 | Unknown | 0 | 3–5 | 1 | 0 | 0 |
| Italy | No | 200 | 0 | 100 | 0 | 20 | 0 | 0 | |
| The Netherlands | Yes, but limited | 150 | 35 | 60 | 6 | 5 | 5 | 5 | 0 |
| Sweden | No | 35 | 0 | 15 | 0 | 4–5 | 0 | 0 | |
| Switzerland | No | 70 | 10 | 80 | 0 | 15 | 2 | 5 | 0 |
| The United Kingdom | No | 40 | 0 | 10 | 0 | 1 | 0 | 0 | 0 |
| The United States – Respondent #1 | Yes, as usual | 18 | N/A | <5 | N/A | 1–2 | N/A | 0 | N/A |
| The United States – Respondent #2 | Yes, but limited | Unknown | 5 | Unknown | 20 | Unknown | 25 | Unknown | 0 |
| The United States – Respondent #3 | Yes, as usual | 48 | N/A | 48 | N/A | 10–20 | N/A | < 2 | N/A |
| Japan | Yes, as usual | 20 | N/A | 2 | N/A | 0–1 | N/A | 0–1 | N/A |
| Singapore | Yes, but limited | 16 | 1–2 | 45 | 10 | <7 | 1–2 | <7 | 0 |
AMD = age‐related macular degeneration; CSC = central serous chorioretinopathy; N/A = not applicable; PCV = polypoidal choroidal vasculopathy; PDT = photodynamic therapy.
In contrast to the Netherlands, the distribution of remaining ampoules of verteporfin was not centrally organized in most countries. In France, a similar system with preset criteria was chosen, although ophthalmologists only had to declare that their patient met these criteria, instead of having to present multimodal imaging to confirm this statement (Société Française d'Ophtalmologie 2021). In the United Kingdom, all remaining ampoules of verteporfin were sent to the four national ophthalmological oncology centres (Royal College of Ophthalmologists 2021). Thus, they prioritized treating ocular tumours with PDT.
There were some differences in the management of different retinal diseases in the absence of verteporfin (See Table 4). For chronic CSC, most respondents chose a watchful waiting approach, with the use of focal laser in select cases. Some reported using anti‐VEGF in cases with a CNV, and some respondents said they were using MR antagonists. For PCV, all respondents said they used intravitreal anti‐VEGF injections, with two specialists using focal laser if indicated. For choroidal haemangioma, most respondents chose a watchful waiting approach while awaiting PDT, and some respondents mentioned argon laser, brachytherapy and intravitreal anti‐VEGF therapy as their current strategy.
Table 4.
Managing strategies per respondent in the absence of photodynamic therapy
| How are you managing these diseases in the absence of PDT? | ||||
|---|---|---|---|---|
| Country and respondent | Chronic CSC | PCV | Choroidal haemangioma | Neovascular AMD |
| Denmark | Watchful waiting. In case of CNV: anti‐VEGF. A few cases: focal laser | Anti‐VEGF | Watchful waiting | Anti‐VEGF |
| France | Watchful waiting, focal laser | Anti‐VEGF | Anti‐VEGF | Anti‐VEGF |
| Germany | Anti‐VEGF therapy, focal laser | Anti‐VEGF | Anti‐VEGF | Anti‐VEGF |
| Israel – Respondent #1 | Watchful waiting. A few cases: focal laser. Considering to perform HSML | Anti‐VEGF | Watchful waiting, brachytherapy | Anti‐VEGF |
| Israel – Respondent #2 | Focal laser if possible. MR antagonists in selected cases | Anti‐VEGF | Watchful waiting | Anti‐VEGF |
| Italy | HSML, MR antagonist. In case of CNV: anti‐VEGF | Anti‐VEGF | Mixed strategies | Anti‐VEGF |
| The Netherlands | Watchful waiting. Focal laser if possible | Anti‐VEGF, focal laser | PDT | Anti‐VEGF |
| Sweden | HSML, focal laser | Anti‐VEGF | Focal laser for two extrafoveal tumours. Two cases awaiting PDT, for whom anti‐VEGF and oral propranolol are being discussed | Anti‐VEGF |
| Switzerland | In case of extrafoveal leakage: focal laser. Watchful waiting and reduction in risk factors, HSML. In case of CNV or FIPED: anti‐VEGF | Anti‐VEGF, and if not enough: combined anti‐VEGF + focal laser if extrafoveal aneurysm | Watchful waiting, while awaiting PDT | Anti‐VEGF |
| The United Kingdom | Watchful waiting | Anti‐VEGF | PDT, by referring to an oncology centre | Anti‐VEGF |
| The United States – Respondent #1 | N/A | N/A | N/A | N/A |
| The United States – Respondent #2 | Anti‐VEGF | Anti‐VEGF | Anti‐VEGF | Anti‐VEGF |
| The United States – Respondent #3 | N/A | N/A | N/A | N/A |
| Japan | N/A | N/A | N/A | N/A |
| Singapore | Focal laser if possible | Anti‐VEGF | Unknown | Anti‐VEGF |
AMD = age‐related macular degeneration; anti‐VEGF = anti‐vascular endothelial growth factor; CNV = choroidal neovascularization; CSC = central serous chorioretinopathy; FIPED = flat irregular pigment epithelial detachment; HSML = high‐density subthreshold micropulse laser; MR = mineralocorticoid receptor; N/A = not applicable; PCV = polypoidal choroidal vasculopathy; PDT = photodynamic therapy.
In Fig. 1, the average percentage of patients treated with PDT is depicted for the different indications, both in the normal situation and during the period of shortage. A significant reduction in number of patients that were treated can be noted for cases with chronic CSC, PCV and choroidal haemangioma.
Fig. 1.
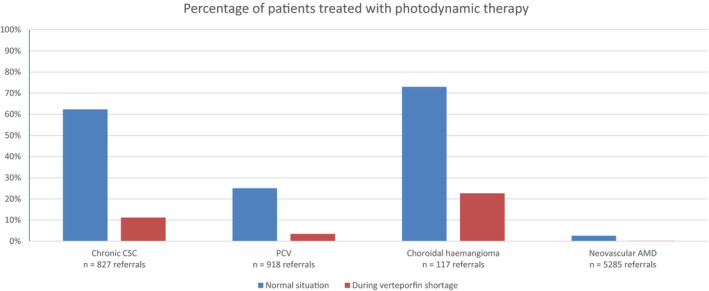
Percentage of patients treated with photodynamic therapy per disease, both in the normal situation and during the verteporfin shortage. These values were calculated by dividing the number of PDT‐treated patients by the number of referred patients per clinic and averaging these percentages. The absolute number of referrals is noted below the bars. AMD = age‐related macular degeneration; CSC = central serous chorioretinopathy; PCV = polypoidal choroidal vasculopathy; PDT = photodynamic therapy. [Colour figure can be viewed at wileyonlinelibrary.com]
Fifty per cent of respondents indicated that they more often considered using half‐dose PDT since the shortage, in cases where they would normally have used a full dose. None declared that they were considering using a different photosensitizer than verteporfin, mainly due to lack of evidence of its safety and efficacy.
Eleven out of 12 of our respondents agreed that the absence of verteporfin is a very serious situation with grave consequences for the patients who require PDT, and 9 out of 12 completely agreed with this statement (based on a 5‐point scale). Several respondents think that measures should be taken at the national or international level (e.g. the level of the European Union) to prevent the occurrence of future shortages. One measure that was mentioned several times was that emergency stocks of essential medications should be kept.
Why is There a Lack of Verteporfin?
Verteporfin is manufactured by a single manufacturer: Alcami Carolinas Corporation (Charleston, South Carolina, United States). It is produced for Bausch Health US, LLC (Bridgewater, New Jersey, United States), and for Cheplapharm Arzneimittel GmbH (Greifswald, Germany) in the European Union (Cheplapharm Arzneimittel GmbH 2020). The marketing authorization holder (MAH) in Europe, Cheplapharm Arzneimittel GmbH, has informed the national competent authorities (who have, in turn, notified the national organizations representing ophthalmologists) that there are ‘technical defects in the filling machine’ in the United States that is responsible for the production of Visudyne® (Cheplapharm Arzneimittel GmbH 2021). The production was transferred to a new line with equivalent machines within the same building. In July 2021, however, Cheplapharm Arzneimittel GmbH reported that the ‘validation processes were delayed due to unforeseeable technical malfunctions’, resulting in an estimated delay in supply until early 2022 (Cheplapharm Arzneimittel GmbH 2021).
Possible Solutions in Times of Shortage
There are several management options during such a longer period of shortage.
The first solution that should be considered is to look for alternative medicines for (subgroups of) patients. In the situation described here, other photosensitizers or alternative approaches or medicines could be considered. Several photosensitizers, such as PhotoPoint (Miravant Medical Technologies, Inc., Santa Barbara, Florida, United States), have been developed for PDT but discontinued due to inadequate efficacy, suboptimal properties or an unfavourable safety profile (Ciulla et al. 2005; Ziemssen & Heimann 2012). Indocyanine green (ICG), commonly used in retinal angiography, could also be used as a photosensitizer. Studies have described the antimicrobial effect of PDT with ICG, both in vitro (Wong et al. 2019) and in vivo in patients with periodontitis (Niazi et al. 2020). Other studies have shown its efficacy in the treatment of cutaneous diseases, such as Kaposi sarcoma (Abels et al. 1998). However, the use of ICG as a photosensitizer seems not to have been described in ophthalmology yet. Currently, only verteporfin seems to have a favourable profile and a new suitable photosensitizer will likely take years of research and development before gaining regulatory approval.
Alternative treatment options could be used. In chronic CSC, alternatives such as micropulse laser (van Dijk et al. 2018) and oral eplerenone (van Rijssen et al. 2021) have been studied, but various randomized controlled trials indicate that PDT with verteporfin has better outcomes. The use of eplerenone has been shown not to yield superior outcomes when compared to placebo in one randomized study (Lotery et al. 2020). In patients with chronic CSC, ophthalmologists should watch for the presence of an additional type 1 CNV (a flat irregular pigment epithelial detachment with mid‐reflective sub‐RPE material), as this could be treated with anti‐VEGF agents, such as aflibercept, bevacizumab, brolucizumab or ranibizumab. For PCV, intravitreal anti‐VEGF monotherapy is a good alternative treatment, although a significant proportion of patients might not fully respond to anti‐VEGF monotherapy (Lim et al. 2020). For choroidal haemangioma, various forms of radiation therapy have been reported to be effective, but can often only be performed in specialized centres and bring a risk of several ocular side effects, such as cataract, subretinal fibrosis, radiation retinopathy and optic neuropathy (Karimi et al. 2015). Besides this, intravitreal anti‐VEGF therapy could be initiated to reduce SRF, but this still requires further studies.
Another option in case of a medicine shortage at a local level is to ask a pharmacist to compound the medication in a pharmacy for an individual patient (Directive/83/EC 2001). However, for verteporfin, this option was deemed impossible due to complexity, as stated by the Dutch Ministry of Health, Wellbeing and Sports (Broekers‐Knol 2021). In addition, no pharmaceutical grade raw material from an alternative supplier was available.
On an international level, medicine shortages need to be reported to regulatory authorities, who may respond with specific requests to a market authorization holder (MAH) (European Medicines Agency 2021a). The MAH is a company that is allowed to market a specific medicinal product. In principle, the MAH is responsible for aligning demand with supply and preparing an appropriate response. However, it is questionable whether they understand the impact of a given shortage on patients. Managing stock is therefore something that should ideally be directed by, or at least aligned with healthcare professionals in collaboration with patient societies. In the past, shortages of enzyme replacement therapies have resulted in international programmes for prioritization of patients, for example in Gaucher disease (Hollak et al. 2010). Similarly, for verteporfin, committees were installed, albeit on a national level, to set criteria to prioritize patients. Such initiatives were undertaken in the Netherlands (Werkgroep Medische Retina van het Nederlands Oogheelkundig Gezelschap 2021), France (Société Française d'Ophtalmologie 2021), the United Kingdom (Royal College of Ophthalmologists 2021) and Canada (Canadian Ophthalmological Society 2021). In general, patients with ocular cancers were prioritized, followed by (functional) monocular patients with other retinal diseases. In some countries, retina specialists had to present multimodal imaging to confirm that their patient met these criteria.
An additional approach, which should also be orchestrated by healthcare professionals, is to maximize the number of treatable patients by reducing the dosage. As previously described in this article, half‐dose PDT has been proven to be equally effective in CSC and in PCV when compared to full‐dose PDT. A further reduction to one‐third‐dose PDT was studied in CSC but appeared to be inferior compared with half‐dose PDT (van Rijssen et al. 2019b). This could allow more patients to be treated with each ampoule.
Possible Preventive Measures for Future Shortages
Drug shortages are not a rare occurrence. In 2019, 1492 drug shortages were reported in the Netherlands (Koninklijke Nederlandse Maatschappij ter Bevordering der Pharmacie 2020). Currently, MAHs are expected to develop shortage prevention and response plans (European Medicines Agency 2021a, b). For life‐saving and unique products, incorporating qualified back‐ups and sufficient stock might be essential (International Society for Pharmaceutical Engineering 2014). Several European Member States have quantified this sufficient stock, for example at 2.5 months in the Netherlands (Koninklijke Nederlandse Maatschappij ter Bevordering der Pharmacie 2021; Tweede Kamer der Staten‐Generaal 2021). This stock, however, would not have been enough in the current case, as a halt of supplies has occurred for over 6 months. In addition to this, MAHs may inform competitors to scale up production (International Society for Pharmaceutical Engineering 2014). However, competition may be limited by patent protection and other regulatory exclusivities (Tomas & Peng 2017). When the treatment is still under patent protection, compulsory licensing may be an option if the raw material can be obtained from another manufacturer. Compulsory licensing enables governments to grant the right to use a patent without the consent of the patent holder (t Hoen et al. 2017). When patent protection has expired, competition by generic manufacturers may not arise for small patient populations since manufacturers may not sufficiently recoup their investments (Beall et al. 2020). In the case of verteporfin, for example, the introduction of intravitreal anti‐VEGF therapy as a superior treatment for neovascular AMD has drastically decreased the population that requires PDT. This problem may be overcome by novel publicly funded public–private partnerships that develop a treatment for a cost‐based price. However, due to its complexity, it was not possible to set up a new short‐term verteporfin production facility (Broekers‐Knol 2021). Implementation of any of these measures may require investments and could result in higher prices.
Conclusions
The shortage of verteporfin due to production problems at the sole manufacturing plant has had a great impact on ophthalmological care and patient outcomes throughout the world. PDT has a prominent role in several chorioretinal diseases, mostly on an off‐label basis, for which fully equivalent alternative treatments are not available. Hence, this shortage of verteporfin for a prolonged period may have resulted in significant and irreversible vision loss worldwide. Steps should be taken to avoid future shortages.
Supporting information
Appendix S1. The questionnaire on the verteporfin shortage that was sent to key opinion leaders in medical retina from around the world.
None.
NR and CEMH are members of the platform ‘Medicijn voor de Maatschappij’, an academic initiative that aims to support sustainable access to medicines for rare diseases, funded by the Nationale Postcode Loterij.
CMGC: Bayer, Novartis, Roche; IC: Genentech; CME: Bayer, Novartis, Roche; KBF: Bayer, Genentech, Novartis, Regeneron, Roche; FGH: Bayer, Genentech, Novartis, Roche; PKK: Bausch + Lomb, Bayer, Novartis, Regeneron; GQ: Bausch + Lomb, Bayer, Novartis, Roche; RT: Bayer, Genentech, Novartis, Roche; CCW: Bausch + Lomb; ROS: Bayer, Novartis. MJS, EHCvD, NR, CEMH, SA, AJL, KOM, YS, DZ, RMHD and CJFB report no relevant conflicts of interest.
References
- Abels C, Karrer S, Bäumler W, Goetz AE, Landthaler M & Szeimies RM (1998): Indocyanine green and laser light for the treatment of AIDS‐associated cutaneous Kaposi's sarcoma. Br J Cancer 77: 1021–1024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allison RR, Bagnato VS & Sibata CH (2010): Future of oncologic photodynamic therapy. Future Oncol 6: 929–940. [DOI] [PubMed] [Google Scholar]
- Anand R, Augsburger JJ & Shields JA (1989): Circumscribed choroidal hemangiomas. Arch Ophthalmol 107: 1338–1342. [DOI] [PubMed] [Google Scholar]
- Batlle AM (1993): Porphyrins, porphyrias, cancer and photodynamic therapy‐‐a model for carcinogenesis. J Photochem Photobiol B 20: 5–22. [DOI] [PubMed] [Google Scholar]
- Beall RF, Quinn AE, Kesselheim AS, Tessema FA & Sarpatwari A (2020): Generic competition for drugs treating rare diseases. J Law Med Ethics 48: 789–795. [DOI] [PubMed] [Google Scholar]
- Boixadera A, García‐Arumí J, Martínez‐Castillo V et al. (2009): Prospective clinical trial evaluating the efficacy of photodynamic therapy for symptomatic circumscribed choroidal hemangioma. Ophthalmology 116: 100–105.e101. [DOI] [PubMed] [Google Scholar]
- Broekers‐Knol A (2021): Kamerbrief over melding medicijntekort Visudyne. Available at: https://www.rijksoverheid.nl/documenten/kamerstukken/2021/07/29/kamerbrief‐over‐melding‐medicijntekort‐visudyne (Accessed on 6 January 2022).
- Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP & Ianchulev T (2009): Ranibizumab versus verteporfin photodynamic therapy for neovascular age‐related macular degeneration: two‐year results of the ANCHOR study. Ophthalmology 116: 57–65.e55. [DOI] [PubMed] [Google Scholar]
- Canadian Ophthalmological Society (2021): Guidelines for Supply Triage During Visudyne (Verteporfin) Shortage. Available at: https://www.cosprc.ca/guidelines‐for‐supply‐triage‐during‐visudyne‐verteporfin‐shortage (Accessed on 27 January 2022).
- Chaikitmongkol V, Cheung CMG, Koizumi H, Govindahar V, Chhablani J & Lai TYY (2020): Latest developments in polypoidal choroidal vasculopathy: Epidemiology, etiology, diagnosis, and treatment. Asia Pac J Ophthalmol (Phila) 9: 260–268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheplapharm Arzneimittel GmbH (2020): VISUDYNE® (verteporfin for injection). Available at: http://www.hpra.ie/docs/default‐source/Shortages‐Docs/visudyne_september‐2020.pdf?sfvrsn=2 (Accessed on 21 December 2021).
- Cheplapharm Arzneimittel GmbH (2021): Statement concerning the prolonged shortage of Visudyne®. Available at: http://www.hpra.ie/docs/default‐source/Shortages‐Docs/visudyne‐current‐shortage_update‐(1).pdf?sfvrsn=2 (Accessed on 21 December 2021).
- Cheung CMG, Lai TYY, Teo K et al. (2021): Polypoidal choroidal vasculopathy: consensus nomenclature and non‐indocyanine green angiograph diagnostic criteria from the Asia‐Pacific ocular imaging society PCV workgroup. Ophthalmology 128: 443–452. [DOI] [PubMed] [Google Scholar]
- Cheung CMG, Lee WK, Koizumi H, Dansingani K, Lai TYY & Freund KB (2019): Pachychoroid disease. Eye (Lond) 33: 14–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ciulla TA, Criswell MH, Snyder WJ & Small W (2005): Photodynamic therapy with PhotoPoint photosensitiser MV6401, indium chloride methyl pyropheophorbide, achieves selective closure of rat corneal neovascularisation and rabbit choriocapillaris. Br J Ophthalmol 89: 113–119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dansingani KK, Gal‐Or O, Sadda SR, Yannuzzi LA & Freund KB (2018): Understanding aneurysmal type 1 neovascularization (polypoidal choroidal vasculopathy): a lesson in the taxonomy of 'expanded spectra' ‐ a review. Clin Experiment Ophthalmol 46: 189–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diamond I, Granelli SG, McDonagh AF, Nielsen S, Wilson CB & Jaenicke R (1972): Photodynamic therapy of malignant tumours. Lancet 2: 1175–1177. [DOI] [PubMed] [Google Scholar]
- Directive 2001/83/EC (2001): Directive 2001/83/EC Of the European Parliament and of the council of 6 November 2001 on the community code relating to medicinal products for human use. Official Journal L311: 67 art 3.1. [Google Scholar]
- Dolmans DE, Fukumura D & Jain RK (2003): Photodynamic therapy for cancer. Nat Rev Cancer 3: 380–387. [DOI] [PubMed] [Google Scholar]
- European Medicines Agency (2020): Summary of product characteristics. Available at: https://www.ema.europa.eu/en/documents/product‐information/visudyne‐epar‐product‐information_en.pdf (Accessed on 24 December 2021).
- European Medicines Agency (2021a): Guidance on detection and notification of shortages of medicinal products for Marketing Authorisation Holders (MAHs) in the Union (EEA). Available at: https://www.ema.europa.eu/en/documents/regulatory‐procedural‐guideline/guidance‐detection‐notification‐shortages‐medicinal‐products‐marketing‐authorisation‐holders‐mahs_en.pdf (Accessed on 28 January 2022).
- European Medicines Agency (2021b): Shortage of Visudyne (verteporfin). Available at: https://www.ema.europa.eu/en/documents/shortage/shortage‐visudyne‐verteporfin‐supply‐shortage_en.pdf (Accessed on 8 January 2022).
- Figge FH, Weiland GS & Manganiello LO (1948): Cancer detection and therapy; affinity of neoplastic, embryonic, and traumatized tissues for porphyrins and metalloporphyrins. Proc Soc Exp Biol Med 68: 640. [DOI] [PubMed] [Google Scholar]
- Hollak CE, vom Dahl S, Aerts JM et al. (2010): Force majeure: therapeutic measures in response to restricted supply of imiglucerase (Cerezyme) for patients with Gaucher disease. Blood Cells Mol Dis 44: 41–47. [DOI] [PubMed] [Google Scholar]
- Hurst LC (1982): Porphyria revisited. Med Hist 26: 179–182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- International Society for Pharmaceutical Engineering (2014): ISPE drug shortages prevention plan: a holistic view from root cause to prevention. Available at: https://ispe.org/sites/default/files/initiatives/drug‐shortages/drug‐shortages‐prevention‐plan.pdf (Accessed on 7 January 2022).
- Karimi S, Nourinia R & Mashayekhi A (2015): Circumscribed choroidal hemangioma. J Ophthalmic Vis Res 10: 320–328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koh A, Lee WK, Chen LJ et al. (2012): EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina 32: 1453–1464. [DOI] [PubMed] [Google Scholar]
- Koninklijke Nederlandse Maatschappij ter Bevordering der Pharmacie (2020): KNMP Achtergrondinformatie: Geneesmiddelentekorten. Available at: https://www.knmp.nl/downloads/knmp‐achtergrondinformatie‐geneesmiddelentekorten.pdf (Accessed on 13 January 2022).
- Koninklijke Nederlandse Maatschappij ter Bevordering der Pharmacie (2021): Staatssecretaris Blokhuis: ijzeren voorraad geneesmiddelen van tweeënhalve maand. Available at: https://www.knmp.nl/actueel/nieuws/nieuws‐2021/staatssecretaris‐blokhuis‐ijzeren‐voorraad‐geneesmiddelen‐van‐tweeenhalve‐maand (Accessed 25 November 2021).
- Kwiatkowski S, Knap B, Przystupski D et al. (2018): Photodynamic therapy – Mechanisms, photosensitizers and combinations. Biomed Pharmacother 106: 1098–1107. [DOI] [PubMed] [Google Scholar]
- Lee WK, Iida T, Ogura Y et al. (2018): Efficacy and safety of intravitreal aflibercept for polypoidal choroidal vasculopathy in the PLANET study: a randomized clinical trial. JAMA Ophthalmol 136: 786–793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lim TH, Lai TYY, Takahashi K et al. (2020): Comparison of ranibizumab with or without verteporfin photodynamic therapy for polypoidal choroidal vasculopathy: the EVEREST II randomized clinical trial. JAMA Ophthalmol 138: 935–942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lotery A, Sivaprasad S, O'Connell A et al. (2020): Eplerenone for chronic central serous chorioretinopathy in patients with active, previously untreated disease for more than 4 months (VICI): a randomised, double‐blind, placebo‐controlled trial. Lancet 395: 294–303. [DOI] [PubMed] [Google Scholar]
- Mehta PH, Meyerle C, Sivaprasad S, Boon C & Chhablani J (2017): Preferred practice pattern in central serous chorioretinopathy. Br J Ophthalmol 101: 587–590. [DOI] [PubMed] [Google Scholar]
- Mohabati D, van Dijk EH, van Rijssen TJ et al. (2018): Clinical spectrum of severe chronic central serous chorioretinopathy and outcome of photodynamic therapy. Clin Ophthalmol 12: 2167–2176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nederlands Oogheelkundig Gezelschap (2021): Ernstig tekort aan Visudyne. Available at: https://www.oogheelkunde.org/nieuws/ernstig‐tekort‐aan‐visudyne (Accessed on 22 October 2021).
- Niazi FH, Noushad M, Tanvir SB, Ali S, Al‐Khalifa KS, Qamar Z & Al‐Sheikh R (2020): Antimicrobial efficacy of indocyanine green‐mediated photodynamic therapy compared with Salvadora persica gel application in the treatment of moderate and deep pockets in periodontitis. Photodiagnosis Photodyn Ther 29: 101665. [DOI] [PubMed] [Google Scholar]
- Nyst HJ, Tan IB, Stewart FA & Balm AJ (2009): Is photodynamic therapy a good alternative to surgery and radiotherapy in the treatment of head and neck cancer? Photodiagnosis Photodyn Ther 6: 3–11. [DOI] [PubMed] [Google Scholar]
- Ozog DM, Rkein AM, Fabi SG, Gold MH, Goldman MP, Lowe NJ, Martin GM & Munavalli GS (2016): Photodynamic therapy: a clinical consensus guide. Dermatol Surg 42: 804–827. [DOI] [PubMed] [Google Scholar]
- Quhill H, Gosling D, Sears K & Rundle P (2021): Primary photodynamic therapy for small amelanotic choroidal melanomas: consecutive case series of 69 patients with at least 24‐month follow‐up. Br J Ophthalmol 105: 794–799. [DOI] [PubMed] [Google Scholar]
- Raizada K & Naik M (2021): Photodynamic therapy for the eye StatPearls. Treasure Island, FL: StatPearls Publishing. [PubMed] [Google Scholar]
- Royal College of Ophthalmologists (2021): Medicine Supply Notification: Visudyne® (verteporfin) 15mg powder for solution for infusion. Available at: https://www.rcophth.ac.uk/wp‐content/uploads/2021/07/MSN_2021_027‐Visudyne‐Verteporfin‐15mg‐powder‐for‐solution‐for‐infusion.pdf (Accessed on 22 October 2021).
- Sachdeva R, Dadgostar H, Kaiser PK, Sears JE & Singh AD (2010): Verteporfin photodynamic therapy of six eyes with retinal capillary haemangioma. Acta Ophthalmol 88: e334–e340. [DOI] [PubMed] [Google Scholar]
- Saito M, Iida T & Kano M (2012): Combined intravitreal ranibizumab and photodynamic therapy for retinal angiomatous proliferation. Am J Ophthalmol 153: 504–514.e501. [DOI] [PubMed] [Google Scholar]
- Santosa V & Limantara L (2008): Photodynamic therapy: new fight in medicine world. Indo J Chem 8: 279–291. [Google Scholar]
- Schmidt‐Erfurth UM, Michels S, Kusserow C, Jurklies B & Augustin AJ (2002): Photodynamic therapy for symptomatic choroidal hemangioma: visual and anatomic results. Ophthalmology 109: 2284–2294. [DOI] [PubMed] [Google Scholar]
- Société Française d'Ophtalmologie (2021): Rationalisation de l'utilisation des flacons de Visudyne® en contexte de pénurie mondiale. Available at: https://www.sfo‐online.fr/actualites/rationalisation‐de‐lutilisation‐des‐flacons‐de‐visudyner‐en‐contexte‐de‐penurie‐mondiale (Accessed on 22 October 2021).
- Spaide RF, Gemmy Cheung CM, Matsumoto H et al. (2022): Venous overload choroidopathy: a hypothetical framework for central serous chorioretinopathy and allied disorders. Prog Retin Eye Res 86: 100973. [DOI] [PubMed] [Google Scholar]
- t Hoen EFM, Boulet P & Baker BK (2017): Data exclusivity exceptions and compulsory licensing to promote generic medicines in the European Union: a proposal for greater coherence in European pharmaceutical legislation. J Pharm Policy Pract 10: 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- TAP study group (1999): Photodynamic therapy of subfoveal choroidal neovascularization in age‐related macular degeneration with verteporfin: one‐year results of 2 randomized clinical trials‐‐TAP report. Treatment of age‐related macular degeneration with photodynamic therapy (TAP) study group. Arch Ophthalmol 117: 1329–1345. [PubMed] [Google Scholar]
- Tomas MC & Peng B (2017): A cheat sheet to navigate the complex maze of pharmaceutical exclusivities in Europe. Pharm Pat Anal 6: 161–170. [DOI] [PubMed] [Google Scholar]
- Tsipursky MS, Golchet PR & Jampol LM (2011): Photodynamic therapy of choroidal hemangioma in sturge‐weber syndrome, with a review of treatments for diffuse and circumscribed choroidal hemangiomas. Surv Ophthalmol 56: 68–85. [DOI] [PubMed] [Google Scholar]
- Tweede Kamer der Staten‐Generaal (2021): Kamerstukken II. 29 477: 1‐16.
- van Dijk EHC & Boon CJF (2021): Serous business: delineating the broad spectrum of diseases with subretinal fluid in the macula. Prog Retin Eye Res 84: 100955. [DOI] [PubMed] [Google Scholar]
- van Dijk EHC, Fauser S, Breukink MB et al. (2018): Half‐dose photodynamic therapy versus high‐density subthreshold micropulse laser treatment in patients with chronic central serous chorioretinopathy: the PLACE trial. Ophthalmology 125: 1547–1555. [DOI] [PubMed] [Google Scholar]
- Van Dijk EHC, Mohabati D, Veselinovic S, Chung WH, Dijkman G & Boon CJF (2021): The spectrum of polypoidal choroidal vasculopathy in Caucasians: clinical characteristics and proposal of a classification. Graefes Arch Clin Exp Ophthalmol 259: 351–361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Dijk EHC, van Rijssen TJ, Subhi Y & Boon CJF (2020): Photodynamic therapy for Chorioretinal diseases: a practical approach. Ophthalmol Ther 9: 329–342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Rijssen TJ, van Dijk EHC, Scholz P et al. (2019a): Focal and diffuse chronic central serous chorioretinopathy treated with half‐dose photodynamic therapy or subthreshold micropulse laser: PLACE trial report no. 3. Am J Ophthalmol 205: 1–10. [DOI] [PubMed] [Google Scholar]
- van Rijssen TJ, van Dijk EHC, Scholz P et al. (2020): Crossover to photodynamic therapy or micropulse laser after failure of primary treatment of chronic central serous chorioretinopathy: the REPLACE trial. Am J Ophthalmol 216: 80–89. [DOI] [PubMed] [Google Scholar]
- van Rijssen TJ, van Dijk EHC, Tsonaka R et al. (2021): Half‐dose photodynamic therapy versus eplerenone in chronic central serous chorioretinopathy (SPECTRA): a randomized controlled trial. Am J Ophthalmol 233: 101–110. [DOI] [PubMed] [Google Scholar]
- van Rijssen TJ, van Dijk EHC, Yzer S et al. (2019b): Central serous chorioretinopathy: towards an evidence‐based treatment guideline. Prog Retin Eye Res 73: 100770. [DOI] [PubMed] [Google Scholar]
- von Tappeiner HJA (1903): therapeutische Versuche mit fluoreszierenden Stoffen (therapeutic experiments with fluorescent substances). Munch Med Wochenschr 50: 2042–2044. [Google Scholar]
- Werkgroep Medische Retina van het Nederlands Oogheelkundig Gezelschap (2021): Triage van patiënten voor fotodynamische therapie ten tijde van schaarste van Visudyne. Available at: https://www.oogheelkunde.org/files/nieuws/2021.07.29%20Prioriteringsschema%20PDT%20definitief_0.pdf (Accessed on 22 October 2021).
- Wong CW, Yanagi Y, Lee W‐K, Ogura Y, Yeo I, Wong TY & Cheung CMG (2016): Age‐related macular degeneration and polypoidal choroidal vasculopathy in Asians. Prog Retin Eye Res 53: 107–139. [DOI] [PubMed] [Google Scholar]
- Wong IY, Shi X, Gangwani R, Iu LP, Fung N, Li Q, Ng ALK & Li X (2018): One‐year results of half‐ versus standard‐dose photodynamic therapy combined with ranibizumab for polypoidal choroidal vasculopathy. Retina 38: 725–730. [DOI] [PubMed] [Google Scholar]
- Wong T‐W, Liao S‐Z, Ko W‐C, Wu C‐J, Wu SB, Chuang Y‐C & Huang IH (2019): Indocyanine green‐mediated photodynamic therapy reduces methicillin‐resistant Staphylococcus aureus drug resistance. J Clin Med 8: 411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ziemssen F & Heimann H (2012): Evaluation of verteporfin pharmakokinetics – Redefining the need of photosensitizers in ophthalmology. Expert Opin Drug Metab Toxicol 8: 1023–1041. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. The questionnaire on the verteporfin shortage that was sent to key opinion leaders in medical retina from around the world.