

Abstract
Background
Mesh is frequently utilized intraoperatively for the repair of groin hernias. However, patients may request non‐mesh hernia repairs owing to adverse events reported in other mesh procedures. To inform surgical safety, this study aimed to compare postoperative complications between mesh and non‐mesh groin hernia repairs and identify other operative and patient‐related risk factors associated with poor postoperative outcomes.
Methods
Ovid MEDLINE and grey literature were searched to 9 June 2021 for studies comparing mesh to non‐mesh techniques for primary groin hernia repair. Outcomes of interest were postoperative complications, recurrence of hernia, pain and risk factors associated with poorer surgical outcomes. Methodological quality was appraised using the AMSTAR 2 tool.
Results
The systematic search returned 4268 results, which included seven systematic reviews and five registry analyses. Mesh repair techniques resulted in lower hernia recurrence rates, with no difference in chronic pain, seroma, haematoma or wound infection, compared to non‐mesh techniques. Risk factors associated with increased risk of hernia recurrence were increased body mass index (BMI), positive smoking status and direct hernia. These were independent of surgical technique. Patients under 40 years of age were at increased risk of postoperative pain.
Conclusions
Surgical repair of primary groin hernias using mesh achieves lower recurrence rates, with no difference in safety outcomes, compared with non‐mesh repairs. Additional risk factors associated with increased recurrence include increased BMI, history of smoking and hernia subtype.
Keywords: hernia, mesh, rapid review, recurrence, safety, surgery
To inform surgical safety, we performed a rapid review comparing postoperative complications between mesh and non‐mesh groin hernia repairs and identify other operative and patient‐related risk factors associated with poor postoperative outcomes. We found that surgical repair of primary groin hernia utilizing mesh results in lower recurrence rates with no difference in safety outcomes, compared to non‐mesh repairs. Other factors associated with increased incidence of recurrence include increased BMI and smoking history.

Introduction
Hernias are protrusions of organs, or part of organs, through the cavity which lines it. 1 They are generally stratified by anatomical location, with inguinal and femoral hernias (collectively known as groin hernias) the most common type of hernia. Groin hernias are frequently encountered with or without symptoms in clinical practice with an estimated lifetime risk of 27% in men and 3% in women, and can be symptomatic or asymptomatic. 1 Surgical repair is indicated for symptomatic hernias, with inguinal hernia repair being one of the most frequently performed operations globally. 2 Repair can be achieved by suturing the defect closed, or by implanting surgical mesh to reinforce the weakened or damaged tissue. 1
The successful use of mesh products in hernia repair prompted the introduction of similar products for urogynaecological procedures. 3 Urogynaecological mesh was used to reinforce weakened vaginal walls in pelvic organ prolapse and support the urethra or bladder in stress urinary incontinence. However, amid safety concerns – specifically ongoing pain, infection, bleeding and urinary problems 4 – international regulatory agencies cancelled approval of these devices and medical societies no longer recommend their use. 5 , 6 , 7 An exception is the use of midurethral sling for the treatment of stress urinary incontinence, which is still considered safe and effective. 8 , 9
Surgeons have noted public confusion regarding the use of mesh products intraoperatively. 10 Patients are requesting non‐mesh hernia repairs 10 despite increased hernia recurrence when mesh is not used. 1 , 2 Owing to public misinformation and failure of clarification of terminology, surgeons have noted that patients are confusing adverse events associated with mesh used for urogynaecological procedures with mesh used for hernia repair. 10 , 11 Approximately half of surgical hernia repair patients may have felt that the use of mesh increases the risk of complications or would have no benefit compared to a non‐mesh repair. 11 Clarifying the safety of mesh is important. However, focusing solely on mesh as the key safety concern may omit discussion of other factors that could potentially affect the postoperative outcomes. Thus, there is a need to both evaluate the safety of mesh and identify other risk factors associated with hernia repair to better inform patients and providers. Accordingly, this study aimed to compare outcomes after hernia repair with mesh versus without mesh and identify operative and patient‐related factors associated with poor outcomes.
Methods
This study comprised a rapid review that was broadly congruent with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta‐Analyses) statement standards. 12
Search strategy
A systematic search of Ovid MEDLINE was performed from database inception to 9 June 2021. The full search strategy is outlined in Appendix A in Data S1. A research librarian designed the search strategy, which included text and medical subject heading terms relating to hernia, mesh repair, non‐mesh repair, safety and adverse events. Study design was limited to systematic reviews, meta‐analyses and registry analyses to identify high‐level evidence with the longest length of follow‐up. Searches were not limited by language to avoid publication bias; however, study selection was limited to English articles. No date limits were applied. In addition to the systematic search, the following hernia registry websites were searched for relevant publications: Swedish Groin Hernia Registry, Danish Hernia Database, Herniamed, Evereg, Club Hernie and the Abdominal Core Health Quality Collaborative.
Study selection was performed in duplicate by two authors, who independently reviewed records by title and abstract, and then by full text. Articles were imported into Rayyan 13 (Qatar Computing Research Institute, Ar‐Rayyan, Qatar) with differences settled via consensus. Data were extracted by one author and reviewed by another author. Extracted data included author, year, study design, patient demographics, surgical technique, follow‐up duration and outcomes of interest.
Study selection
The PICO (Population, Intervention, Comparator and Outcome) framework guided the search strategy and study selection. Table 1 outlines the PICO criteria used for study selection.
Table 1.
PICO criteria for study selection
| Population | Patients undergoing surgical repair of an inguinal or femoral hernia |
|---|---|
| Intervention | Hernioplasty using mesh (open or laparoscopic) |
| Comparator | Herniorrhaphy without mesh (open or laparoscopic) |
| Outcomes |
Pain Recurrence Seroma Haematoma Wound infection Other adverse events (testicular atrophy, urinary retention, neurovascular or visceral injury) Length of stay Risk factors |
| Study designs | Systematic reviews, meta‐analyses, registry analyses |
Sliding, hiatal, incisional, umbilical and bilateral hernias were excluded. Similarly, strangulated hernias and hernias necessitating emergency surgery were excluded. Postoperative pain is often delineated into acute and chronic, and in this study only chronic pain was included, defined as pain lasting over 1 month post‐surgery. Systematic reviews were excluded if more than 50% of included studies were not from WHO mortality stratum A countries. 14 Where reviews had more than 50% overlap of included studies, the review with the largest number of studies was included to avoid overlapping data. Where registry studies sourced data from the same database with matching inclusion criteria and dates, the study with the largest number of patients was included. Registry studies with more than 1000 included patients were considered.
Data analysis
The direction of effect for odds ratios was standardized to mesh versus non‐mesh to allow comparison between studies. This was achieved by taking the reciprocal of reported odds ratios for included studies reporting non‐mesh versus mesh.
Methodological quality
Methodological quality was appraised using AMSTAR 2 (A MeaSurement Tool to Assess systematic Reviews 2 15 ) for systematic reviews, and the Institute of Health Economics (IHE) quality appraisal checklist for case series studies and cohort studies for registry studies. 16 Quality was assessed by two authors independently and disagreements were settled via consensus.
Results
The systematic and database search returned 4268 results, from which 7 systematic reviews and 5 registry analyses comparing mesh techniques to non‐mesh techniques were included. The PRISMA flow diagram 17 is shown in Figure 1.
Fig. 1.
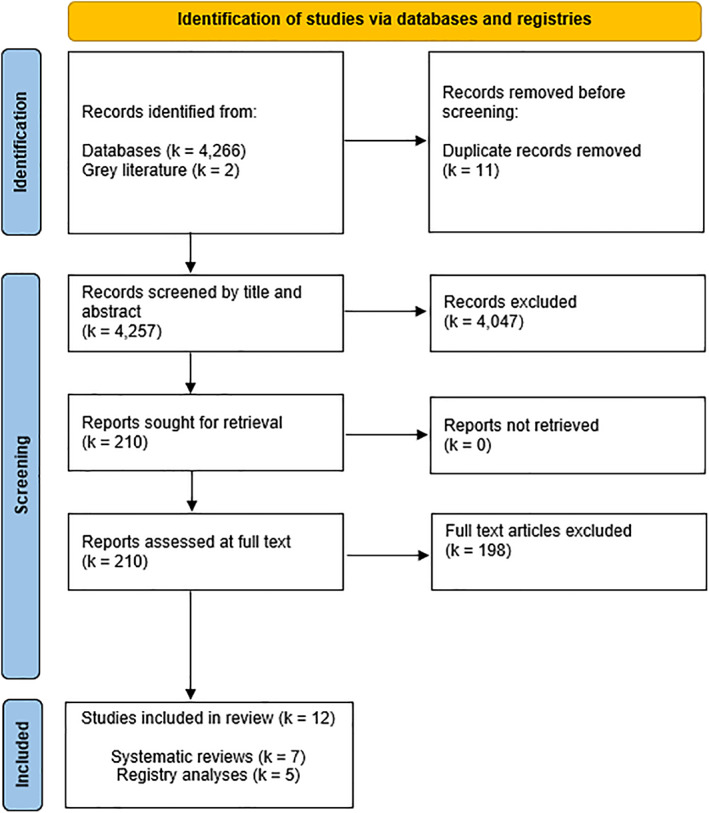
PRISMA flow diagram showing study selection.
Study characteristics
The characteristics of the included systematic reviews and registry analyses are summarized in Appendix B and Appendix C in Data S1. The meta‐analyses included randomized controlled trials and observational studies. Patient numbers in the systematic reviews ranged from 3044 18 to 714 167, 19 and in registry analyses ranged from 2612 20 to 117 898. 21 Mesh repair techniques were predominantly Lichtenstein, totally extraperitoneal (TEP) and transabdominal preperitoneal (TAPP). Less frequently used mesh repair techniques included Prolene Hernia System, Stoppa and Trabucco. The Shouldice technique was the most performed non‐mesh technique, in addition to Bassini, Modified darn, Desarda, Marcy, Moloney and McVay. Trials within the reviews were conducted in North America, Europe, Asia and Australia. Baseline characteristics were similar among mesh and non‐mesh groups. Patient age ranged from 18 to 90 years (mean 49 years) and 97% were male. Most patients were undergoing repair of a unilateral primary hernia, of which inguinal hernias were the most common. Femoral hernias were included in seven studies; however, they constituted ~1% of the total included population (the remainder were inguinal hernias). The mean duration of follow‐up was 35 months, ranging from 3 to 180 months (15 years).
Chronic pain was reported in six systematic reviews and two registry analyses, with follow‐up ranging from 2 months to 10 years. Pain was generally measured via questionnaires, as dichotomous (present or absent) or continuous (0 to 10) variables. Hernia recurrence was reported in five systematic reviews and two registry analyses, with a minimum follow‐up of 1 month postoperatively up to 5 years. Regarding other complications, seroma, haematoma and wound infections were each reported in four reviews. Secondary reported outcomes were infrequently reported; these included testicular atrophy (k = 3), urinary retention (k = 2), length of hospital stay (k = 2) and neurovascular or visceral injury (k = 1). Risk factors associated with increased adverse outcomes were reported in two systematic reviews and three registry analyses.
Quality of included studies
Results of the quality assessment are presented in Appendix D and Appendix E in Data S1 . All seven systematic reviews were deemed high‐quality following appraisal with AMSTAR 2. All systematic reviews used a comprehensive literature search strategy, specified the PICO, had a satisfactory method of assessing risk of bias and declared conflicts of interest. Most studies performed study selection in duplicate (k = 6), established the protocol method prior to conducting the review (k = 6), and performed data extraction in duplicate (k = 5). Few studies declared the sources of funding of the included studies (k = 3).
No methodological issues were discovered in quality assessment of the registry analyses. The objective was clearly stated, and all were multicentre, prospective studies. Inclusion and exclusion criteria were clearly defined. Competing interests and sources of support were reported in four of the five studies.
Outcomes
Results of the systematic reviews and registry analyses reporting on postoperative complications following groin hernia repair are provided in Appendix F and Appendix G in Data S1. Table 2 summarizes the reported outcomes.
Table 2.
Summary of results of postoperative complications following groin repair
| Outcome | Meta‐analysis (range of effects) mesh versus non‐mesh | Registry analyses (range) mesh versus non‐mesh |
|---|---|---|
| Pain |
OR 0.36 (95% CI 0.29 to 0.46) 22 OR 1.15 (95% CI 0.62 to 2.12) 23 |
OR 0.78 (95% CI 0.63 to 0.97) 21 |
| Recurrence |
OR 0.26 (95% CI 0.25 to 0.28) 23 RR 0.46 (95% CI 0.26 to 0.80) 1 |
HR 0.25 (95% CI 0.16 to 0.40) 24 |
| Seroma |
OR 1.04 (95% CI 0.37 to 2.94) 23 RR 1.63 (95% CI 1.03 to 2.59) 1 |
NR |
| Haematoma |
OR 0.86 (95% CI 0.58 to 1.28) 18 OR 1.56 (95% CI 0.16 to 15.52) 23 |
OR 1.05 (95% CI 0.95 to 1.17) 21 |
| Wound infection |
OR 1.24 (95% CI 0.84 to 1.84) 25 OR 1.35 (95% CI 0.38 to 4.82) 23 |
OR 0.87 (95% CI 0.74 to 1.02) 21 |
Abbreviations: CI, confidence interval; HR, hazard ratio; NR, no result; OR, odds ratio; RR, risk ratio.
Pain
Six systematic reviews provided evidence on pain, of which four had meta‐analyses performed 22 , 23 , 25 , 26 and two were narrative syntheses. 1 , 18 The number of patients in the meta‐analyses ranged from 387 26 to 4366. 22 Three meta‐analyses found no significant difference in pain between mesh repair and non‐mesh repair groups. 23 , 25 , 26 Effect sizes ranged from OR 0.93 (95% CI 0.53 to 1.65; P = 0.83) 25 to OR 1.15 (95% CI 0.62 to 2.12; P = 0.57). 23 In one meta‐analysis, mesh repair was less likely to result in chronic pain (>12 months) compared to non‐mesh repair (OR 0.36; 95% CI 0.29 to 0.46; P <0.00001). 22
The two narrative systematic reviews were in favour of mesh or noted that there were no significant differences in reported pain between mesh and non‐mesh groups. 1 , 18 Analysis of 104 108 patients in the Swedish Hernia Registry found that patients who had a mesh repair were significantly less likely to have pain compared to those who had a non‐mesh repair (OR 0.78; 95% CI 0.63 to 0.97; P < 0.005). 21 Another database analysis of 2612 patients did not find any difference in reported pain between mesh and non‐mesh techniques. 20
Recurrence
Hernia recurrence was evaluated in five meta‐analyses. 1 , 18 , 22 , 23 , 25 The number of patients in the meta‐analyses ranged from 1565 23 to 8221. 22 Four meta‐analyses concluded that mesh repair significantly decreased hernia recurrence rates compared to non‐mesh repair. The effect sizes were OR 0.26 (95% CI 0.25 to 0.28; P <0.0001) 23 and RR 0.46 (95% CI 0.26 to 0.80; P = 0.006). 1 One meta‐analysis found no significant difference in recurrence rates between open mesh repairs and open non‐mesh repairs (risk difference (RD) 0.00; 95% CI −0.01 to 0.01; P = 0.93). 18 Recurrence was evaluated in two registry analyses. Both found that patients who had a mesh repair had a significantly lower risk of hernia recurrence than did those who had a non‐mesh repair. 24 , 27 Risk of reoperation for recurrence decreased over time following mesh repairs, from hazard ratio (HR) 0.45 (95% CI 0.39 to 0.51; P <0.001) after 0 to 30 months, to HR 0.25 (95% CI 0.16 to 0.40; P <0.001) after 60 to 96 months (5–8 years) following surgery. 24
Seroma
Seroma was evaluated in four meta‐analyses. The number of patients in the meta‐analyses ranged from 1700 to 2640. 1 , 18 , 23 , 25 Three meta‐analyses found no difference in rates of seroma between mesh groups and non‐mesh groups. 18 , 23 , 25 Effect size ranged from OR 1.04 (95% CI 0.37 to 2.94) 23 to OR 1.52 (95% CI 0.92 to 2.52; P = 0.10). 25 One meta‐analysis concluded that mesh repair significantly increased the rate of seroma compared to non‐mesh repair (RR 1.63; 95% CI 1.03 to 2.59; P = 0.04). 1 No registry analyses reported this outcome.
Haematoma
Haematoma was evaluated in four meta‐analyses, with patient numbers ranging from 562 to 3773. 1 , 18 , 23 , 25 All four meta‐analyses reported no significant difference in the rate of haematoma between the mesh and non‐mesh repair groups. Effect sizes ranged from OR 1.56 (95% CI 0.16 to 15.52; P = 0.35) 23 to OR 0.86 (95% CI 0.58 to 1.28; P = 0.59). 18 Haematoma was evaluated in one registry analysis of 104 108 patients in the Swedish Hernia Registry. 21 The study found no difference in the rate of haematoma between mesh and non‐mesh groups (OR 1.05; 95% CI 0.95 to 1.17; P = NR [not reported]). 21
Wound infection
Wound infection was evaluated in four meta‐analyses, with patient numbers ranging from 1938 to 4540. 1 , 18 , 23 , 25 All four meta‐analyses reported no significant difference in the rates of wound infection between the mesh or non‐mesh repair groups. Effect sizes ranged from OR 1.24 (95% CI 0.84 to 1.84; P = 0.28) 25 to OR 1.35 (95% CI 0.38 to 4.82; P = 0.39). 23 Wound infection was evaluated in two registry analyses, both of which found no significant difference in the rate of wound infection between mesh and non‐mesh groups (OR 0.87; 95% CI 0.74 to 1.02; P = NR 21 ; and 3.0% Lichtenstein versus 3.3% Shouldice and 2.7% Marcy; P >0.05). 20
Secondary outcomes
Other reported outcomes were testicular atrophy or injury, urinary retention, length of hospital stay and neurovascular or visceral injury. Testicular atrophy or injury following hernia repair was evaluated in three meta‐analyses. 1 , 18 , 23 All meta‐analyses reported no significant difference in the rate of testicular atrophy or injury between mesh and non‐mesh groups. Effect sizes were RD −0.00 (95% CI −0.01 to 0.00; P = 0.58) 18 and RR 1.06 (95% CI 0.63 to 1.76; P = 0.83). 1 Urinary retention was evaluated in two meta‐analyses. One meta‐analysis concluded that the rate of urinary retention was significantly less following mesh repair compared with non‐mesh repair (RR 0.53; 95% CI 0.38 to 0.73; P = 0.0001). 1 The other meta‐analysis reported no significant difference between the groups (OR 0.69; 95% CI 0.48 to 0.98; P = 0.33). 18 Urinary retention was evaluated in one registry analysis, which concluded that the rate of urinary retention was significantly less following mesh repair than it was after non‐mesh repair (0.31; 95% CI 0.21 to 0.47; P < 0.005). 21 Length of stay was evaluated in 2 meta‐analyses, which found no difference between mesh and non‐mesh groups (mean difference [MD] = −0.09; 95% CI −0.44 to 0.26; P = 0.62 18 ; weighted MD = 0.38; 95% CI −0.41 to 1.18; P = 0.34 23 ). Neurovascular or visceral injury was evaluated in one meta‐analysis, which concluded that the rate of injury was less following mesh repair than it was following non‐mesh repair (RR 0.61; 95% CI 0.49 to 0.76; P <0.001). 1
Risk factors
A summary of the results (systematic review, k = 1; registry analyses, k = 3) reporting on risk factors for postoperative complications, hernia recurrence or pain following groin hernia repair is provided in Table 3.
Table 3.
Summary of results of systematic reviews and registry analyses reporting on risk factors of complications
| Risk factor | Summary of findings |
|---|---|
| Patient factors | |
| BMI | Increased BMI (25–30 kg/m2) increases risk of postoperative complications and recurrence 19 , 28 |
| Age |
Younger age (<40 years) increases risk of pain 20 Older age (>65 years) increases risk of postoperative complications 21 but not recurrence 19 |
| Smoking status | Smoking increases risk of recurrence 19 |
| Gender | Female gender increases risk of recurrence 19 |
| Operative factors | |
| Length of operation | Longer operation (>50 min) increases risk of overall postoperative complications 21 |
| Surgeon experience† | Experienced surgeons (>26 groin hernia operations per year) decreases risk of overall postoperative complications 21 |
| Acute operation‡ | Acute operation increases risk of overall postoperative complications, 21 but not recurrence 19 |
| Anaesthesia | Local anaesthesia decreases risk of postoperative complications‡, 21 |
| Hernia characteristics | |
| Hernia subtype | Primary direct hernias result in increased risk of recurrence 19 |
| Hernia defect size | Hernia size did not influence risk of recurrence 19 |
Abbreviation: BMI, body mass index.
All complications which came to the knowledge of the unit within 30 days after operation.
Operated on within 24 h of admission, with signs of strangulated or incarcerated hernia.
One narrative systematic review 19 and one registry analysis 28 reported on the effect of body mass index (BMI) on the risk of postoperative complications following groin hernia repair. The narrative systematic review included six studies and concluded that increasing BMI (>25 kg/m2) was a risk factor for hernia recurrence. 19 The registry study included 49 094 groin hernia operations and found that increased BMI (>25 kg/m2) increased the risk of postoperative complications (HR 1.10; 95% CI 1.03 to 1.18; P = 0.005) and the risk of reoperation for recurrence (HR 1.19; 95% CI 1.00 to 1.40; P = 0.05) when compared with patients with a BMI of 20 to 25 kg/m2. 28 The analyses combined patients undergoing both mesh and non‐mesh repairs; findings were independent of surgical technique. Further, when patients with increased BMI underwent either suture or Lichtenstein mesh repair, patients with suture repair were at increased risk of recurrence (HR 1.68; 95% CI 1.14 to 2.48; P = 0.00). 28 Two registry analyses 20 , 21 and one meta‐analysis 19 reported on age as a risk factor for postoperative complications following groin hernia repair. Age was not a risk factor for hernia recurrence in a meta‐analysis of 78 967 patients (RR 0.99; 95% CI 0.84 to 1.17; P = 0.9). 19 Patients over 65 years of age were at increased risk of overall postoperative complications compared to patients under 65 years (OR 1.26; 95% CI 1.21 to 1.31; P <0.005). 21 Patients under 40 years of age were at increased risk of postoperative pain compared with patients over 40 years (26.8% vs. 19.7%; P = 0.001), regardless of surgical technique. 20 One meta‐analysis reported on the effects of smoking status on hernia recurrence. 19 Smoking was a significant and independent risk factor for recurrence following inguinal repair in the meta‐analysis of 773 patients (OR 2.53; 95% CI 1.43 to 4.47; P = 0.001). 19 These findings were independent of mesh or non‐mesh techniques. One meta‐analysis reported on the effect of sex on hernia recurrence. 19 Female sex was a significant risk factor for recurrence after hernia repair in a meta‐analysis of 284 898 patients (RR 1.38; 95% CI 1.28 to 1.48; P <0.001).
A registry analysis found that patients whose operations were longer than 50 min duration were at significantly increased risk of postoperative complications compared with those whose operations were less than 50 min (OR 1.27; 95% CI 1.22 to 1.33; P <0.005). 21 An additional registry analysis found that surgeon experience impacted the risk of postoperative complications. 21 Surgeons who performed greater than 26 groin hernia operations per year had a lower risk of postoperative complications compared to surgeons who performed 6 to 25 groin hernia operations per year (OR 0.93; 95% CI 0.88 to 0.98; P <0.005). This effect was even greater with surgeons who performed more than 50 groin hernia operations per year (OR 0.82; 95% CI 0.78 to 0.86; P < 0.005). A meta‐analysis and a registry analysis reported on the effect of acute operations on the risk of complications. The meta‐analysis found that acute operations did not affect the risk of recurrence compared to elective operations (RR 1.28; 95% CI 0.97 to 1.70; P = 0.08). 19 However, the registry analysis found that patients undergoing an acute operation were at increased risk of overall postoperative complications (OR 1.58; 95% CI 1.47 to 1.71; P <0.005). 21 A registry analysis found both regional anaesthesia (OR 1.53; 95% CI 1.43 to 1.63; P <0.005) and general anaesthesia (OR 1.30; 95% CI 1.23 to 1.37; P <0.005) resulted in an increased risk of postoperative complications when compared with local anaesthesia. 21 One meta‐analysis reported on inguinal hernia subtype as a risk factor for recurrence. 19 The meta‐analysis found that operating on a primary direct inguinal hernia was a significant risk factor for recurrence compared to a primary indirect hernia repair (RR 1.91; 95% CI 1.62 to 2.26; P <0.001). One meta‐analysis reported on hernia defect size and found that hernia defects larger than 3 cm did not increase the risk of hernia recurrence when compared with hernia defects smaller than 3 cm (RR 1.09; 95% CI 0.92 to 1.30; P = 0.33). 19
Discussion
This review evaluated the safety and effectiveness of groin hernia repair using mesh compared with non‐mesh repair and evaluated patient and operative risk factors associated with complications and recurrence. Evidence from both systematic reviews and registry analyses demonstrated that groin hernia repair using mesh is safe and effective, inferred by lower recurrence rates and similar postoperative complication rates compared to non‐mesh techniques. Results were consistent with multiple international guidelines, which advise that patients older than 30 years of age with a symptomatic groin hernia should undergo a repair with mesh. 2 , 25 , 29
Chronic pain is a significant and common postoperative complication following hernia repair. 26 This study found that pain rates were either similar or lower in patients with mesh repair compared to patients with non‐mesh repairs. Postoperative pain is likely to be influenced by multiple variables, and factors other than the presence of mesh need to be considered when assessing the risk of postoperative pain following groin hernia repair. The results show that age is a risk factor for chronic pain, with younger patients (<40 years) reporting increased pain levels compared to older patients, regardless of the repair technique. 19 , 20 , 21 Similar results were found in studies that solely investigated mesh techniques, indicating that the presence of mesh may not be the cause of pain following groin hernia repair. 30 , 31 Other influencing factors not captured by the present study include preoperative pain, surgical technique (open or laparoscopic), surgery for recurrence and nerve injury. 32
Hernia recurrence was significantly lower following mesh repair in four included meta‐analyses. The systematic review that reported no difference in recurrence had the shortest follow‐up duration. 18 Given that the incidence of recurrence increases over time, 33 this review may have had insufficient follow‐up to accurately detect true recurrence rates. However, longer‐term studies have highlighted that mesh does not simply delay hernia recurrence but improves the biomechanical strength of the surrounding tissue. 34 Given that hernia recurrence is consistently lower following mesh repair, risk factors for recurrence in addition to the choice of surgical technique need to be considered. Patients with increased BMI had increased rates of recurrence regardless of repair type. 28 Notably, in overweight patients non‐mesh repairs resulted in a 68% increase in reoperation for recurrence compared to mesh repairs. 28 Positive smoking status was also significantly and independently associated with increased rates of recurrence, 19 reinforcing the substantial literature on the link between smoking and postoperative complications. 35 , 36 Hernia subtype significantly affects recurrence, with direct hernia repair resulting in an increased risk of recurrence compared to repair of indirect hernias. The reason for this is unclear, but possible reasons include insufficient mesh overlap or pathophysiological aspects of the respective defects. 37 The operative‐related risk factors identified in this study (surgeon experience, anaesthesia type, operation length) are not unique to hernia repairs and may not reflect risk factors specific to mesh surgeries.
This review underscores the patient and operative factors – separate from the presence of mesh – that need to be considered when evaluating the safety profile of hernia repairs. Focusing solely on mesh as the proxy for postoperative complications unduly simplifies the problem. 9 Postoperative adverse events following hernia repair, including seroma, haematoma and wound infections, occur at a similar rate in mesh and non‐mesh repairs. 1 , 18 , 23 Surgeons can be confident when counselling patients on hernia repair techniques that mesh for hernia repair is a safe and effective choice, resulting in lower recurrence rates with similar frequencies of pain and adverse events, compared to non‐mesh techniques. Further this study's findings show that outcomes after mesh repair of groin hernias are not comparable to adverse events reported in transvaginal mesh cases. Complications caused by transvaginal mesh arise from mechanical incompatibility between the mesh and the host tissue, incomplete understanding of the underlying disease processes and the failure of surveillance and regulatory approval processes. 38 It is important to highlight that midurethral sling mesh repair is still recommended for cases of routine stress urinary incontinence.
Monitoring of healthcare quality by clinical quality registries is essential for improved patient outcomes. Multiple hernia registries worldwide actively monitor surgical quality of hernia repair. 39 , 40 For effective monitoring, clinical quality registries must aim to capture data on all operations in the specialty and include patient‐related risk factors such as BMI, smoking status and comorbidities, as well as operative details such as length of operation and anaesthesia type. 39 , 40 Monitoring of these indices is essential for informative surveillance for improved patient care. Clinical quality registries offer significant returns on investment owing to their contribution to improved patient outcomes and processes of care. 41 There is currently no Australian and Aotearoa New Zealand‐specific hernia registry collecting all long‐term patient data following hernia repair. The ANZ Hernia society is in the process of launching a pilot study for an Australian and New Zealand clinical quality registry with a learning healthcare system for all abdominal wall hernias with anticipated national rollout in 2023. This clinical quality registry will collect patient, operative and mesh related data from all hernia operations, regardless of technique. Such a registry is critical to support postoperative surveillance and long‐term patient outcomes reporting following all hernia repairs.
The therapeutic regulatory bodies of Australia (Therapeutic Goods Administration) and Aotearoa New Zealand (Medsafe) collect data on adverse events associated with medical devices, but the process is reactive and reflects only a subset of hernia operations. From December 2021, surgical mesh devices in Australia will be reclassified from Class IIb (medium risk) to Class III (high‐risk), to align with the European Union framework. 42 While this increase in classification level results in more stringent pre‐testing and mandatory long‐term follow‐up, only hernia repairs utilizing mesh will be captured. This change in regulatory processes will capture neither patient‐related risk factors nor non‐mesh hernia repairs, which contribute significantly to postoperative adverse events including hernia recurrence and pain.
This review has multiple limitations. Limiting the search to a single database may bias results and relevant articles may have been omitted. While this study's results were consistent with existing guidelines, applicability is limited to lower‐risk hernias. It is unclear whether mesh has a similar safety profile for hernias in regions other than the groin, or differing patient groups (e.g. complex cases, recurrent hernia, female patients or patients with existing comorbidities), however this was outside the scope of the present study. Included studies were predominantly conducted in high‐income countries, thus while reflecting a bias within the literature, the relevance of these findings to countries with less available resources is unclear.
Conclusion
Surgical repair of primary groin hernia utilizing mesh results in lower recurrence rates with no difference in safety outcomes, compared with non‐mesh repairs. Factors other than mesh that are associated with increased incidence of recurrence include increased BMI and smoking history. There is an urgent need to establish an Australia and Aotearoa New Zealand‐specific hernia registry to provide long‐term postoperative surveillance data and facilitate effective reporting of adverse events for all hernia operations. Surgeons can be confident when counselling patients on groin hernia repair techniques that the intraoperative utilization of mesh is a safe and effective choice.
Conflict of interest
None declared.
Author contributions
Sarah M. Smith: Conceptualization; data curation; formal analysis; investigation; writing – original draft; writing – review and editing. Adeel Khoja: Conceptualization; data curation; formal analysis; investigation; writing – review and editing. Jonathan Henry W. Jacobsen: Conceptualization; data curation; formal analysis; investigation; writing – original draft; writing – review and editing. Joshua G. Kovoor: Conceptualization; data curation; formal analysis; investigation; writing – review and editing. David R. Tivey: Conceptualization; investigation; supervision; writing – review and editing. Wendy J. Babidge: Conceptualization; investigation; supervision; writing – review and editing. Harsha S. Chandraratna: Conceptualization; formal analysis; investigation; supervision; writing – review and editing. David R. Fletcher: Conceptualization; investigation; supervision; writing – review and editing. Chris Hensman: Conceptualization; investigation; supervision; writing – review and editing. Alex Karatassas: Conceptualization; investigation; supervision; writing – review and editing. Ken Loi: Conceptualization; investigation; supervision; writing – review and editing. Karen McKertich: Conceptualization; investigation; supervision; writing – review and editing. Jessica M. A. Yin: Conceptualization; investigation; supervision; writing – review and editing. Guy J. Maddern: Conceptualization; investigation; supervision; writing – review and editing.
Supporting information
Data S1:Supporting Information
Acknowledgements
The authors thank Kaitryn Campbell, Dr. Kristin Weidenbach. Open access publishing facilitated by The University of Adelaide, as part of the Wiley ‐ The University of Adelaide agreement via the Council of Australian University Librarians.
S. M. Smith MPH, BLM; A. A. Khoja MBBS, MSc; Jonathan Henry W. Jacobsen BSc, BHlthSci (Hons) (Hons), PhD; Joshua G. Kovoor MBBS, BHlthMedSci (Hons); David R. Tivey Bsc (Hons), PhD; Wendy J. Babidge BApp Sci (Hons), PhD, Grad Dip Business; Harsha S. Chandraratna MBBS, FRACS; David R. Fletcher MBBS, MD, FRACS, GAICD; Chris Hensman MBBS, MS, FRACS; Alex Karatassas MBBS, MS, FRACS; K. W. Loi BSc (Med), MBBS, FRACS; K. M. F. McKertich MBBS, FRACS; Jessica M. A. Yin MBBS, FRACS; Guy J. Maddern MBBS, MS, PhD, MD, FRACS, FAHMS.
References
- 1. Lockhart K, Dunn D, Teo S et al. Mesh versus non‐mesh for inguinal and femoral hernia repair. Cochrane Database Syst. Rev. 2018; 9: CD011517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. HerniaSurge G. International guidelines for groin hernia management. Hernia 2018; 22: 1–165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Maher C, Feiner B, Baessler K et al. Transvaginal mesh or grafts compared with native tissue repair for vaginal prolapse. Cochrane Database Syst. Rev. 2016; 2: CD012079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Shah HN, Badlani GH. Mesh complications in female pelvic floor reconstructive surgery and their management: a systematic review. Indian J Urol 2012; 28: 129–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Australian Government Department of Health TGA . Therapeutic goods administration. TGA actions after review into urogynaecological surgical mesh implants. [Cited 2 Sep 2020.] Available from URL: https://www.tga.gov.au/hubs/transvaginal-mesh 2020).
- 6. U.S Food and Drug Administration . Urogynecologic Surgical Mesh Implants. [Cited 7 Jun 2021.] Available from URL: https://www.fda.gov/medical-devices/implants-and-prosthetics/urogynecologic-surgical-mesh-implants 2019.
- 7. Medsafe . Surgical Mesh – Safety Information. [Cited 5 Jun 2021.] Available from URL: https://medsafe.govt.nz/devices/Surgical%20Mesh/Landing.asp 2019.
- 8. Ford AA, Rogerson L, Cody JD et al. Mid‐urethral sling operations for stress urinary incontinence in women. Cochrane Database Syst. Rev. 2015; 7: CD006375. [DOI] [PubMed] [Google Scholar]
- 9. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists . Position statement on midurethral slings. [Cited 25 Aug 2021.] Available from URL: https://ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG‐MEDIA/Women%27s%20Health/Statement%20and%20guidelines/Clinical‐Obstetrics/MUS‐ (C‐Gyn‐32)‐Re‐write‐July‐2020_1.pdf?ext.=.pdf 2020.
- 10. Kelly S. Mesh abdominal wall hernia surgery is safe and effective—the harm New Zealand media has done. N. Z. Med. J. 2017; 130: 54–7. [PubMed] [Google Scholar]
- 11. Elhage SA, Thielen ON, Otero J et al. Perceptions and understanding about mesh and hernia surgery: what do patients really think? Surgery 2021; 169: 1400–6. [DOI] [PubMed] [Google Scholar]
- 12. Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta‐analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009; 339: b2700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan‐A web and mobile app for systematic reviews. Syst. Rev. 2016; 5: 210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. World Health Organization . List of Member States by WHO Region and Mortality Stratum. [Cited 7 Jun 2021.] Available from URL: https://www.who.int/choice/demography/mortality_strata/en/ 2021.
- 15. Shea BJ, Reeves BC, Wells G et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non‐randomised studies of healthcare interventions, or both. BMJ 2017; 358: j4008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Guo B, Moga C, Harstall C, Schopflocher D. A principal component analysis is conducted for a case series quality appraisal checklist. J. Clin. Epidemiol. 2016; 69: 199–207.e192. [DOI] [PubMed] [Google Scholar]
- 17. Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Finch DA, Misra VA, Hajibandeh S. Open darn repair vs open mesh repair of inguinal hernia: a systematic review and meta‐analysis of randomised and non‐randomised studies. Hernia 2019; 23: 523–39. [DOI] [PubMed] [Google Scholar]
- 19. Burcharth J, Pommergaard H‐C, Bisgaard T, Rosenberg J. Patient‐related risk factors for recurrence after inguinal hernia repair: a systematic review and meta‐analysis of observational studies. Surg. Innov. 2015; 22: 303–17. [DOI] [PubMed] [Google Scholar]
- 20. Bay‐Nielsen M, Nilsson E, Nordin P et al. Chronic pain after open mesh and sutured repair of indirect inguinal hernia in young males. BJS 2004; 91: 1372–6. [DOI] [PubMed] [Google Scholar]
- 21. Lundström K‐J, Sandblom G, Smedberg S, Nordin P. Risk factors for complications in groin hernia surgery: a national register study. Ann. Surg. 2012; 255: 784–8. [DOI] [PubMed] [Google Scholar]
- 22. E. U. Hernia Trialists Collaboration . Repair of groin hernia with synthetic mesh: meta‐analysis of randomized controlled trials. Ann. Surg. 2002; 235: 322–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Amato B, Moja L, Panico S et al. Shouldice technique versus other open techniques for inguinal hernia repair. Cochrane Database Syst. Rev. 2012; 2012: CD001543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Bisgaard T, Bay‐Nielsen M, Christensen IJ, Kehlet H. Risk of recurrence 5 years or more after primary Lichtenstein mesh and sutured inguinal hernia repair. Br. J. Surg. 2007; 94: 1038–40. [DOI] [PubMed] [Google Scholar]
- 25. Simons MP, Aufenacker T, Bay‐Nielsen M et al. European hernia society guidelines on the treatment of inguinal hernia in adult patients. Hernia 2009; 13: 343–403 Editorial Practice Guideline. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Oberg S, Andresen K, Klausen TW et al. Chronic pain after mesh versus nonmesh repair of inguinal hernias: a systematic review and a network meta‐analysis of randomized controlled trials. Surgery 2018; 163: 1151–9. [DOI] [PubMed] [Google Scholar]
- 27. Bisgaard T, Bay‐Nielsen M, Kehlet H. Groin hernia repair in young males: mesh or sutured repair? Hernia 2010; 14: 467–9. [DOI] [PubMed] [Google Scholar]
- 28. Rosemar A, Angerås U, Rosengren A, Nordin P. Effect of body mass index on groin hernia surgery. Ann. Surg. 2010; 252: 397–401. [DOI] [PubMed] [Google Scholar]
- 29. Rosenberg J, Bisgaard T, Kehlet H et al. Danish hernia database recommendations for the management of inguinal and femoral hernia in adults. Dan. Med. Bull. 2011; 58: C4243. [PubMed] [Google Scholar]
- 30. Forester B, Attaar M, Chirayil S et al. Predictors of chronic pain after laparoscopic inguinal hernia repair. Surgery 2021; 169: 586–94. [DOI] [PubMed] [Google Scholar]
- 31. Melkemichel M, Bringman S, Nilsson H et al. Patient‐reported chronic pain after open inguinal hernia repair with lightweight or heavyweight mesh: a prospective, patient‐reported outcomes study. Br. J. Surg. 2020; 107: 1659–66. [DOI] [PubMed] [Google Scholar]
- 32. Langeveld HR, Klitsie P, Smedinga H et al. Prognostic value of age for chronic postoperative inguinal pain. Hernia 2015; 19: 549–55. [DOI] [PubMed] [Google Scholar]
- 33. Köckerling F, Koch A, Lorenz R, Schug‐Pass C, Stechemesser B, Reinpold W. How long do we need to follow‐up our hernia patients to find the real recurrence rate? Front Surg 2015; 2: 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Brown CN, Finch JG. Which mesh for hernia repair? Ann. R. Coll. Surg. Engl. 2010; 92: 272–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Yoong S, Tursan d'Espaignet E, Wiggers J et al. WHO Tobacco Knowledge Summaries: Tobacco and Postsurgical Outcomes. Geneva: World Health Organization, 2020. [Google Scholar]
- 36. Grønkjær M, Eliasen M, Skov‐Ettrup LS et al. Preoperative smoking status and postoperative complications: a systematic review and meta‐analysis. Ann. Surg. 2014; 259: 52–71. [DOI] [PubMed] [Google Scholar]
- 37. Burcharth J, Andresen K, Pommergaard HC, Bisgaard T, Rosenberg J. Recurrence patterns of direct and indirect inguinal hernias in a nationwide population in Denmark. Surgery 2014; 155: 173–7. [DOI] [PubMed] [Google Scholar]
- 38. Mangir N, Betül Aldemir D, Chapple CR et al. Landmarks in vaginal mesh development: polypropylene mesh for treatment of SUI and POP. Nat. Rev. Urol. 2019; 16: 675–89. [DOI] [PubMed] [Google Scholar]
- 39. Friis‐Andersen H, Bisgaard T. The Danish inguinal hernia database. Clin. Epidemiol. 2016; 8: 521–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Kyle‐Leinhase I, Köckerling F, Jørgensen LN et al. Comparison of hernia registries: the CORE project. Hernia 2018; 22: 561–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Lee P, Chin K, Liew D et al. Economic evaluation of clinical quality registries: a systematic review. BMJ Open 2019; 9: e030984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Therapeutic Goods Administration . Reclassification of surgical mesh devices. [Cited 25 May 2021.] Available from URL: https://www.tga.gov.au/publication/reclassification-surgical-mesh-devices 2020.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1:Supporting Information