

Abstract
Uremic pruritus (UP) is common in the late stages of chronic kidney disease. Currently, there is a lack of effective treatment for UP. Limited evidence exists on the therapeutic effect of omega-3 fatty acid (O3FA). The aim of this study was to evaluate the efficacy of O3FA supplements in UP patients. We evaluated the efficacy of O3FA supplements in patients with UP through a systematic review and a meta-analysis of randomized control trials retrieved from PubMed, Embase, Cochrane Library, CINAHL, and ClinicalTrials.gov databases. The included studies were summarized and assessed for the risk of bias, and pruritus assessment results were analyzed. To compared with a controlled group, five articles including 164 participants published between 2012 and 2019 using different pruritus scales reported that patients taking O3FA supplement exhibited no significant decrease in the pruritus score (standardized mean difference [SMD] =1.34, 95% confidence interval [CI] = −2.70–0.01, P = 0.05), but three articles using same pruritus scale significant decrease Duo pruritus score (SMD = −0.85, 95% CI = −1.39 to −0.30, P < 0.05). O3FA supplement could be an appealing complementary therapy for UP patients. More rigorously designed studies are needed before recommending the O3FA supplement.
KEYWORDS: Chronic kidney disease, Dialysis, Meta-analysis, Omega-3 fatty acid, Uremic pruritus
INTRODUCTION
Uremic pruritus (UP) is also known as chronic kidney disease (CKD)-associated pruritus, which is commonly seen in patients with advanced or end-stage renal disease (ESRD), affecting more than 40% of patients on dialysis including hemodialysis (HD) and peritoneal dialysis (PD) [1,2,3]. Although the pruritus may be localized, around 50% of the patients diagnosed with UP suffer from generalized pruritus. The itching in patients with UP often exacerbates at night and affects the quality of sleep, resulting in fatigue, anxiety, and depression for the patients[4]. There are various pathogenesis proposed to be related to UP, such as xerosis, neuropathy, mast cell overactivity, the release of substance P, inflammation, or immunological impairment. Since the primary cause of pruritus is still not understood, increasingly different treatment plans are described for pruritus control. Considering the prolonged course and the difficulty to treat pruritus in UP, the advantage and disadvantages of each treatment should be evaluated carefully.
Standard therapies for UP, such as antihistamine, gabapentin, and nalfurafine, may be associated with adverse effects of dizziness and drowsiness [5,6,7]. Some natural or pharmaceutical topical therapies, such as baby oil, avena sativa[8], and capsaicin cream[9], which are mostly used as adjuvant therapy to systemic treatment, may cause burning sensation or irritation for some patients[10]. Besides, most of them have no or little benefit in inhibiting the release of pro-inflammatory cytokines such as serum C-reactive protein and interleukin 6[11,12]. Furthermore, one study has found an increased risk of skin malignancies with topical tacrolimus treatment[13]. Patients with UP may also seek treatment in Chinese medicine, but currently, acupuncture therapy has shown insufficient evidence[14], and the methodological quality of Chinese herbal bath therapy (CHBT) has been reported to be poor[15] [Table 1].
Table 1.
The antipruritic effects and adverse effects of therapeutic methods for uremic pruritus
| Intervention/medication | Study design | Result | ADR |
|---|---|---|---|
| Systemic treatments | |||
| Hydroxyzine [16] | Controlled trial | PSS↘ 33% | Dizziness and drowsiness |
| Gabapentin [7] | Meta-analysis | Pruritus↘ (RR=0.18) | Dizziness and drowsiness |
| Nalfurafine [17] | Meta-analysis | VAS↘ (MD=9.5) | Insomnia, drowsiness and constipation |
| Topical treatments | |||
| Capsaicin [9] | Controlled trial | Pruritus↘ (86% improved) | Burning sensation and erythema |
| Avena Sativa [8] | RCT | VAS↘ (5.21±1.69➔4.10±2.34) | N/A |
| CAM treatments | |||
| Acupressure [6] | Meta-analysis | Insufficient evidence | N/A |
| CHBT [15] | Meta-analysis | VAS↘ (MD=−2.38) | N/A |
↘ : Improved, CAM: Complementary alternative medicine, CHBT: Chinese herbal bath therapy, N/A: Not applicable, RCT: Randomized controlled trial, RR: Risk ratio, PSS: Pruritus severity score, VAS: Visual Analog Scale, MD: Mean differences, ADR: Adverse drug reaction
The omega-3 fatty acid (O3FA), represents a group of polyunsaturated fatty acids among which three are involved in human physiology, namely α-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). O3FA can be obtained mainly from aquagenic organisms or vegetable oil. The major O3FA from marine sources are EPA and DHA, while ALA is abundant in some seeds and nuts and also in some vegetable oils[18]. O3FA is the critical component of cell membranes and plays a vital role in eicosanoid biosynthesis, cell signaling cascades, and gene expression. Besides, eicosanoids derived from O3FA show clinical benefits on cardiovascular disease, diabetes, cancer[19,20], nephropathies[21], and certain skin disease[22] because of their anti-inflammatory effects. Oral supplementation of O3FA has shown the benefit of relieving pruritus in atopic eczema (AD) patients[23]. The xerotic pruritus of healthy people and patients with either ESRD or diabetes have also shown improvement after using a topical ointment containing O3FA[24]. One review has mentioned the potential benefits of O3FA on CKD-associated pruritus[25], and several studies have reported the improvement in dialysis-associated UP after the patients took omega-3, omega-6, and omega-9 supplementation[26,27].
Although some studies have shown that O3FA supplement is an easily accessible nutrition diet with low cost and fewer adverse effects and may benefit patients in dialysis to improve their UP[25,28], there is still limited evidence of O3FA efficacy in UP treatment. Therefore, in this study, we conducted a systematic literature review and meta-analysis of currently published randomized control trials (RCTs) to evaluate the actual efficacy of O3FA in the management of UP.
LITERATURE SEARCH
We searched the articles published in the PubMed, EMBASE, CINAHL, and Cochrane databases up to May 2020. The MeSH and Emtree search headings, which were used are omega-3, pruritus, uremic, CKD, dialysis, and their synonyms. To expand the search, we used the “related articles” option in PubMed and reviewed all the retrieved articles and citations. Furthermore, other studies were identified via searching the references of papers manually and getting in touch with known experts in the field. Finally, we also inspected the unpublished studies in ClinicalTrials.gov registry (http://clinicaltrials.gov/). There are no language restrictions in our search. The full search strategy for each database was put in [Supplementary Table 1]. This article was registered on the online PROSPERO of the National Institute for Health Research (CRD 42020198471).
Supplementary Table 1.
Search strategy
| PubMed | ||||
|---|---|---|---|---|
| Search | Query | Items found | Time | Condition |
| #6 | Search (((((uremic OR Uremia OR Uremias OR Atypical Hemolytic?Uremic?Syndrome))) AND ((Pruritus OR Pruritis OR itch* OR xerosis OR skin problems OR skin disorders OR Skin Diseases))) AND ((Fatty Acids, Omega-3 OR omega-3 fatty acids OR fish oil OR omega 3 OR fatty acids OR Fatty Acid OR n-3 fatty acids OR α-linolenic acid OR polyunsaturated fatty acids OR docosahexaenoic acid OR eicosapentaenoic acid))) AND ((chronic kidney disease OR kidney injury OR kidney failure OR Kidney Failure, Chronic OR end-stage renal disease OR end stage renal disease OR dialysis OR hemodialysis OR peritoneal dialysis)) | 26 | 02:09:35 | #1 AND #2 AND #3 AND #4 |
| #5 | Search ((((uremic OR Uremia OR Uremias OR Atypical Hemolytic?Uremic?Syndrome))) AND ((Pruritus OR Pruritis OR itch* OR xerosis OR skin problems OR skin disorders OR Skin Diseases))) AND ((Fatty Acids, Omega-3 OR omega-3 fatty acids OR fish oil OR omega 3 OR fatty acids OR Fatty Acid OR n-3 fatty acids OR α-linolenic acid OR polyunsaturated fatty acids OR docosahexaenoic acid OR eicosapentaenoic acid)) | 34 | 02:09:18 | #1 AND #2 AND #3 |
| #4 | Search (chronic kidney disease OR kidney injury OR kidney failure OR Kidney Failure, Chronic OR end-stage renal disease OR End Stage Renal Disease OR dialysis OR hemodialysis OR peritoneal dialysis) | 417763 | 02:08:49 | |
| #3 | Search (Fatty Acids, Omega-3 OR omega-3 fatty acids OR fish oil OR omega 3 OR fatty acids OR Fatty Acid OR n-3 fatty acids OR α-linolenic acid OR polyunsaturated fatty acids OR docosahexaenoic acid OR eicosapentaenoic acid) | 559390 | 02:08:27 | |
| #2 | Search (Pruritus OR Pruritis OR itch* OR xerosis OR skin problems OR skin disorders OR skin diseases) | 1099786 | 02:08:10 | |
| #1 | Search (uremic OR uremia OR uremias OR atypical hemolytic?uremic?syndrome) | 37027 | 02:07:46 | |
MeSH term
| Cochrane library | ||
|---|---|---|
| ID | Search | Hits |
| #1 | Uremic OR uremia or uremias or atypical haemolytic uremic syndrome | 1880 |
| #2 | Pruritus OR Pruritis OR itch* OR xerosis OR skin problems OR skin disorders OR skin diseases | 27,639 |
| #3 | Fatty Acids, Omega-3 OR omega-3 fatty acids OR fish oil OR omega 3 OR fatty acids OR fatty acid OR n-3 fatty acids OR α-linolenic acid OR polyunsaturated fatty acids OR docosahexaenoic acid OR eicosapentaenoic acid | 25,336 |
| #4 | Chronic kidney disease OR kidney injury OR kidney failure or kidney failure, chronic OR end-stage renal disease OR end-stage renal disease OR dialysis OR hemodialysis OR peritoneal dialysis | 39,428 |
| #5 | #1 AND #2 AND #3 | 15 |
| #6 | #1 AND #2 AND #3 AND #4 | 14 |
| Embase | |||
|---|---|---|---|
| Number | Query | Results | Date |
| #5 | #1 AND #2 AND #3 AND #4 | 157 | April 22, 2020 |
| #4 | ‘chronic kidney disease’/exp OR ‘chronic kidney disease’ OR ‘kidney injury’/exp OR ‘kidney injury’ OR ‘kidney failure’/exp OR ‘kidney failure’ OR ‘chronic kidney failure’/exp OR ‘chronic kidney failure’ OR ‘end-stage renal disease’/exp OR ‘end-stage renal disease’ OR ‘end stage renal disease’/exp OR ‘end-stage renal disease’ OR ‘dialysis’/exp OR dialysis OR ‘hemodialysis’/exp OR hemodialysis OR ‘peritoneal dialysis’/exp OR ‘peritoneal dialysis’ | 618,764 | April 22, 2020 |
| #3 | ‘omega 3 fatty acid’/exp OR ‘omega 3 fatty acid’ OR ‘omega-3 fatty acids’ OR ‘fish oil’/exp OR ‘fish oil’ OR ‘omega 3’/exp OR ‘omega 3’ OR ‘fatty acids’/exp OR ‘fatty acids’ OR ‘fatty acid’/exp OR ‘fatty acid’ OR ‘n-3 fatty acids’ OR ‘α-linolenic acid’ OR ‘polyunsaturated fatty acids’ OR ‘docosahexaenoic acid’/exp OR ‘docosahexaenoic acid’ OR ‘eicosapentaenoic acid’/exp OR ‘eicosapentaenoic acid’ | 695,758 | April 22, 2020 |
| #2 | pruritus’/exp OR pruritus OR ‘pruritis’/exp OR pruritis OR itch* OR ‘xerosis’/exp OR xerosis OR ‘skin problems’ OR ‘skin disorders’ OR ‘skin diseases’/exp OR ‘skin diseases’ | 1,598,014 | April 22, 2020 |
| #1 | uremic OR ‘uremia’/exp OR uremia OR uremias OR “atypical haemolytic uremic syndrome” | 53,197 | April 22, 2020 |
|
CINAHL
| ||||
|---|---|---|---|---|
| # | Query | Limiters/expanders | Last Run Via | Results |
| S5 | S1 AND S2 AND S3 AND S4 | Expanders - Apply equivalent subjects | Interface - EBSCOhost Research Databases | 1 |
| Search modes - Find all my search terms | Search Screen - Advanced Search | |||
| Database - CINAHL | ||||
| S4 | Chronic kidney disease OR kidney injury OR kidney failure OR Kidney Failure, Chronic OR end-stage renal disease OR End-Stage Renal Disease OR dialysis OR hemodialysis OR peritoneal dialysis |
Expanders - Apply equivalent subjects | Interface - EBSCOhost Research Databases | 87,527 |
| Search modes - Find all my search terms | Search Screen - Advanced Search | |||
| Database - CINAHL | ||||
| S3 | Fatty Acids, Omega-3 OR omega-3 fatty acids OR fish oil OR omega 3 OR fatty acids OR Fatty Acid OR n-3 fatty acids OR α-linolenic acid OR polyunsaturated fatty acids OR docosahexaenoic acid OR eicosapentaenoic acid | Expanders - Apply equivalent subjects | Interface - EBSCOhost Research Databases | 37,610 |
| Search modes - Find all my search terms | Search Screen - Advanced Search | |||
| Database - CINAHL | ||||
| S2 | Pruritus OR Pruritis OR itch* OR xerosis OR skin problems OR skin disorders OR Skin Diseases |
Expanders - Apply equivalent subjects | Interface - EBSCOhost Research Databases | 51,987 |
| Search modes - Find all my search terms | Search Screen - Advanced Search | |||
| Database - CINAHL | ||||
| S1 | Uremic OR Uremia OR Uremias OR Atypical Hemolytic Uremic Syndrome | Expanders - Apply equivalent subjects | Interface - EBSCOhost Research Databases | 4020 |
| Search modes - Find all my search terms | Search Screen - Advanced Search | |||
| Database - CINAHL | ||||
|
ClinicalTrials.gov registry
| |
|---|---|
| Situation | Query |
| Condition or disease | Uremic OR Uremia OR Uremias OR atypical hemolytic uremic syndrome |
| Other terms | Pruritus OR Pruritis OR itch OR xerosis OR skin problems OR skin disorders OR Skin Diseases |
| Intervention/treatment | Fatty Acids, Omega-3 OR omega-3 fatty acids OR fish oil OR omega 3 OR fatty acids OR Fatty Acid OR n-3 fatty acids OR α-linolenic acid OR polyunsaturated fatty acids OR docosahexaenoic acid OR eicosapentaenoic acid |
| Search result: 1 | Treatment of uremic pruritus by olive-omega 3 ointment |
STUDY SELECTION
RCTs were selected to assess the efficacy of O3FA for UP patients. The inclusion criteria were as follows: The presence of UP, administration of O3FA, and quantified data available for pruritus severity. The studies of patients who did not have UP were excluded. We considered any pruritus assessment tools. When raw or missing data were needed, we contacted the author of the studies via E-mail. We chose the studies with a larger population when we encountered repeat studies published using overlapping data sets.
DATA EXTRACTION AND QUALITY ASSESSMENT
Two reviewers extracted the following information of each article independently: Publication information, study population, age, sample size, study design, inclusion and exclusion criteria, matching criteria, period of intervention, O3FA and placebo dosage, pruritus severity measurement tool, pruritus severity results before and after the treatments.
Two reviewers individually screened the eligibility of selected studies following the specified inclusion criteria. When discrepancy arose, it was determined by a third reviewer. The risk of bias of selected articles was assessed by the Cochrane Collaboration's tool[29].
DATA SYNTHESIS AND ANALYSIS
The outcomes of O3FA efficacy for UP were evaluated via the following parameters, namely, pruritus score, itching intensity score. The meta-analysis was performed using the Review Manager (5.4 version, Cochrane Collaboration, Copenhagen, Denmark) to estimate the standardized mean difference (SMD) with the random-effect model. We followed the PRISMA guidelines to perform the meta-analysis[30]. When RCT was designed as a two-period, two-treatment crossover, we retrieved the data of the first period to avoid the carryover effect[31]. Standard deviations (SD) were calculated from the given confidence interval (CI) limits or range values in case of need. Mean was estimated from the provided mean of differences as necessary. Due to the unavailability of SD value after treatment, we assumed it as a small value when only giving initial SD and SD of differences. We combined the mean and SD from each item in the pruritus assessment tool to get the overall mean and SD of the pruritus score if required. For continuous outcomes, we analyzed and obtained the mean and SD from the studies using the mean differences (MD) or SMD with 95% CI. The random-effect model was used to pool estimates of SD and SMD, considering the diversity of pruritus assessment tools and possible heterogeneity. We used the I2 test and Cochran Q statistic to assess the heterogeneity among the studies. We conducted a funnel analysis to evaluate reporting bias regarding the pruritus scores. The quality of evidence was examined by using the Guideline Development Tool established by the GRADE Working Group[32].
RESULTS
Study characteristics
We searched 468 articles from seven electronic databases following the search strategy. Thity-two duplicate studies were excluded. After screening the title and abstract, we excluded 410 articles because of the screening criteria. Full texts of 26 articles were reviewed, and 21 articles were excluded for the following reasons: Eight were review articles[4,5,6,16,25,33,34,35], two were non-RCTs[28,36], one was non-omega-3[37], two were non-UPs[38,39], seven were protocols [40,41,42,43,44,45,46], and one was conference abstract[47]. Finally, five RCTs were included in the meta-analysis[26,27,48,49,50] [Figure 1].
Figure 1.
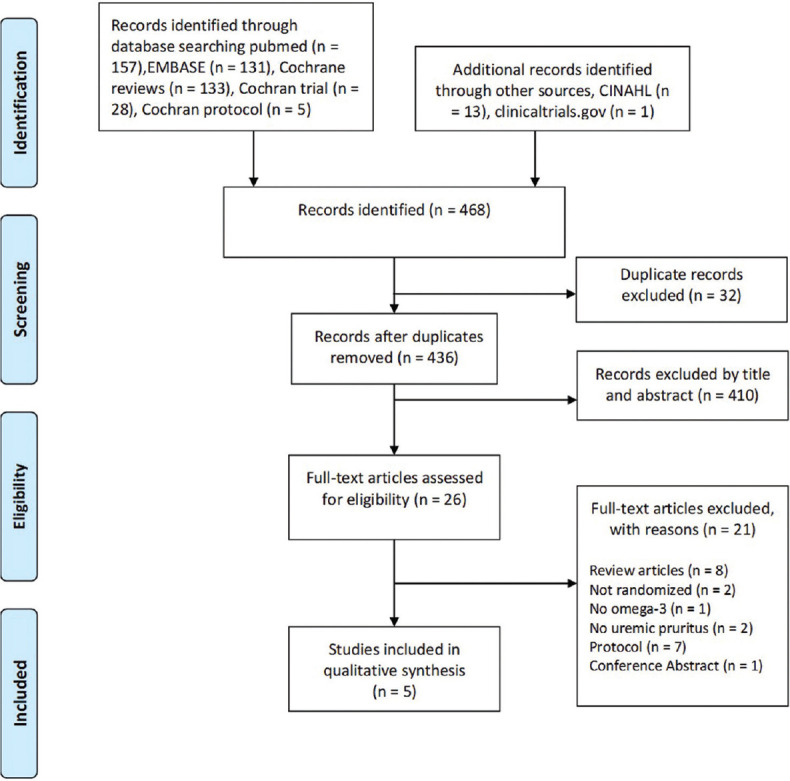
PRISMA-2009-Flow-Diagram-Omega-3
The primary characteristics of the five RCTs published from 1996 to 2019 are listed in Table 2. A total of 164 participants were enrolled with a sample size ranging from 16 to 64. All were RCTs reporting itching with UP. In the five eligible RCTs, four trials are UP in HD[26,27,48,50], while the other is UP in continuous ambulatory peritoneal dialysis[49]. Both groups were included in our meta-analysis because they met our selection criterion for the presence of UP. As for the pruritus assessment tool, three trials used duo pruritus score (DPS) systems[26,27,48], Lahiji et al. utilized the visual analog scale (VAS) score[49], and Shayanpour et al. measured pruritus via the 5-D itch scale (5-DIS) score[50]. VAS was applied to evaluate the itching intensity via a horizontal line marked from 0 to 10 (0 = no pruritus, 10 = the worst pruritus). Detailed pruritus score systems devised by Dr. Duo combined the score of itching intensity, distribution of itch, and sleep disturbance due to pruritus[51]. 5-DIS system assesses five dimensions as degree, duration, direction, disability, and distribution. The four dimensions were measured from 0 to 5 (0 = no, 5 = the most severe), while the distribution was assessed depending on the number of itchy places[52]. There are only two trials reported their dosage of the O3FA in fish oil capsule. The fish oil used in the RCT of Begum et al. and Ghanei et al. contains approximately 728 mg/g O3FA and 300 mg/g O3FA, respectively[27,48]. There are only two trials that reported the dosage of the EPA and DHA in their capsule. Each 1 g fish oil used in the RCT of Ghanei et al. and each 1 g O3FAl used in RCT Lahiji et al. contains 180 mg EPA and 120 mg DHA[48,49].
Table 2.
Characteristics of selected studies
| Study (year) | Study design | Inclusion criteria | Number of patients | Age (years) | Duration of dialysis | Efficacy of dialysis (Kt/V) | Dosage, route, and frequency (O3FA amount) | Duration | Severity assessment | Pruritus score (before→after), experimental control |
|---|---|---|---|---|---|---|---|---|---|---|
| Begum et al. 2004 [27] | RCT | HD | FO: 12 SO: 10 |
FO: 61.2±19.42 SO: 49.25±18.12 |
FO: 4.84±3.35 SO: 5.88±4.64 |
NA | FO, 6 g, oral, daily (4.36 g) | 16 weeks | DPS | FO: 16.7±11.4→8.9±9.2 SO: 17.6±8.8→13.1±5.6 |
| Ghanei et al. 2012 [48] | RCT Cross-over |
HD | O-P: 11 P-O: 11 |
O-P: 59.90±14.82 P-O: 53.09±13.08 |
O-P: 3.81±2.04 P-O: 5.09±4.88 |
O-P: 1.24±0.05 P-O: 1.41±0.27 |
FO, 1 g, oral, TID (0.9 g) | 20 days | DPS | O-P: 20.3±5.28→6.4±5.13 P-O: 17.0±6.84→14.4±5.73 |
| Lahiji et al. 2018 [49] | RCT Cross-over |
CAPD | O-P: 20 P-O: 20 |
O-P: 62.1±11.6 P-O: 61.9±10.8 |
NA | NA | O3FA, 3 g, oral, daily | 4 weeks | VAS | O-P1: 6.4±1.5→3.38±1.5 P-O1: 4.2±2.4→3.72±1.4 |
| Peck et al. 1996 [26] | RCT | HD | FO: 8 OO: 9 SO: 8 |
FO: 54.8±16.2 OO: 45.6±17.4 SO: 49.5±17.2 |
NA | NA | FO, 6 g, oral, daily | 8 weeks | DPS | FO: 8.79±4.65→4.95±4.02 OO: 6.63±2.82→3.62±2.13 SO: 8.18±4.49→8.06±4.85 |
| Shayanpour et al. 2019 [50] | RCT | HD | O: 32 P: 32 |
O: 51.91±6.586 P: 56.25±8.865 |
NA | NA | O3FA, 2 g, daily, oral | 3 weeks | 5-DIS | O: 12.97±1.71→6.66±1.24 P: 14.37±1.37→12.78±1.80 |
Data are presented as mean±SD. CAPD: Continuous ambulatory peritoneal dialysis, 5-DIS: 5-D Itch Scale, DPS: Duo Pruritus Score, FO: Fish oil, HD: Hemodialysis, NA: Not available, O: The omega-3 group, O3FA: Omega-3 fatty acid, OO: Olive oil, P: Placebo group, RCT: Randomized controlled trial, SO: Safflower oil, TID: Ter in die, VAS: Visual Analog Scale, SD: Standard deviation
The risk of bias assessment of the selected trials is shown in Figure 2. Double-blind and random allocation were applied in all included trials[26,27,48,49,50], but only one trial used blocking for concealed allocation sequences[50]. Another bias resulted from the absence of P value of baseline characteristics[48,50], and baseline imbalances in the VAS score[49]. The analysis of all trials was based on the intention-to-treat principle, and available outcome data[26,27,48,49,50]. Bias in the measurement of outcomes was low in all trials due to participant-reported outcomes and blinding[26,27,48,49,50].
Figure 2.
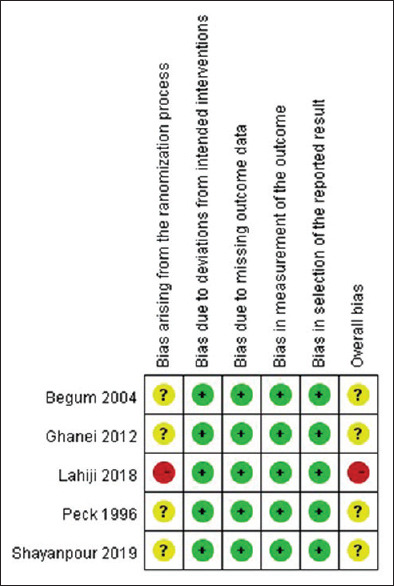
Risk of bias in different studies
A meta-analysis of the five trials showed that the pruritus score decreased not significantly after O3FA supplementation (SMD = 1.34, 95% CI = −2.70–0.01, P = 0.05). The random-effect model was performed since the pooled analysis of these five trials revealed heterogeneity (I2 = 92%, τ2 = 2.19, P < 0.00001) [Figure 3] statistically[26,27,48,49,50]. In addition, we carried out a subgroup analysis of DPS. The DPS significantly improved in the O3FA supplementation group (SMD = −0.85, 95% CI = −1.39 to − 0.30, P < 0.05). The fixed-effect model was performed since the pooled analysis of these three trials revealed low statistical heterogeneity (I2 = 3%, P = 0.36) [Figure 4][26 27 48]. Another subgroup analysis of pruritus score in HD patients was conducted. The pruritus score decreased not significantly after O3FA supplementation (SMD = 1.63, 95% CI = −3.25 to −0.02, P = 0.05). The random-effect model was performed since the pooled analysis of these four trials revealed heterogeneity (I2 = 92%, τ2 = 2.51, P = 0.05) [Figure 5] statistically[26,27,48,50]. Funnel plots of pruritus scores outcomes were asymmetric, suggesting publication bias existed [Figure 6].
Figure 3.

Forest plot for comparison of pruritus scores in uremic pruritus patients administered omega-3 fatty acids
Figure 4.

Forest Plot for comparison of Duo pruritus scores in uremic pruritus patients administered omega-3 fatty acids
Figure 5.

Forest plot for comparison of pruritus scores in HD patients with uremic pruritus administered omega-3 fatty acids
Figure 6.
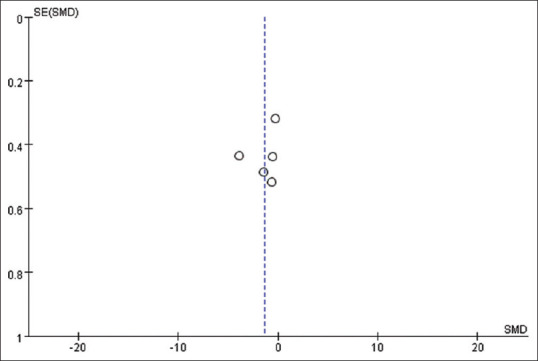
Funnel plot
Quality of evidence
The risk of bias of included RCTs was serious, the quality of evidence was very low to low, and the importance of outcomes was important for the O3FA supplement in UP patients [Table 3].
Table 3.
Grade profile summary of “omega-3 fatty acid for uremic pruritus” quality assessment
| Certainty assessment |
Number of patients |
Effect |
Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | O3FA | Control | Relative (95% CI) | Absolute (95% CI) | ||
| Pruritus scores | ||||||||||||
| 5 | Randomised trials | Serious | Serious | Not serious | Not serious | Publication bias strongly suspected | 83 | 81 | - | SMD 1.34 lower (2.7 lower-0.01 higher) | ⨁◯◯◯ (very low) | Important |
| Duo pruritus scores | ||||||||||||
| 3 | Randomised trials | Serious | Not serious | Not serious | Not serious | Publication bias strongly suspected | 31 | 29 | - | SMD 0.85 lower (1.39 lower-0.3 lower) | ⨁⨁◯◯ (low) | Important |
CI: Confidence interval, O3FA: Omega-3 fatty acid, SMD: Standardized mean difference
DISCUSSION
The review aims to systematically evaluate the efficacy of O3FA supplements for pruritus control in UP. The present meta-analysis of three RCTs included using a fixed-effects model illustrates that O3FA supplements significantly reduce the DPS in UP patients. The suggested dose of O3FA supplements was 0.9–4.36 g daily. Based on the result of Shayanpour et al. showed that UP patients who take O3FA 3 weeks have a significant improvement. It may be implicated 3 weeks is the minimum time needed to have effects on CKD patients by the O3FA supplement.
In our selected studies, the UP population contains both HD and PD groups, which is consistent with a previous study that UP appeared to be unaffected by the type of dialysis[53]. Ko et al. also reported that their prevalence of UP in these two groups was equal, but the pruritus severity of PD patients was lower than HD patients[54]. Besides, many treatments showed a similar antipruritic effect for both HD and PD patients, such as phototherapy, topical gamma-linolenic acid, gabapentin, and O3FA supplement[5,49,55].
The anti-inflammatory ability of O3FA has shown the clinical benefits of some skin disorders[22,56], such as psoriasis[57], and salicylate-induced urticarial rashes[58]. Kock et al. also performed an RCT recruiting 53 AD patients and showed that the group taking dietary DHA for 8 weeks had a significant improvement in symptoms which was evaluated by severity scoring of atopic dermatitis and decrease of peripheral immunoglobulin E level[23]. Kim et al. found topical chia seed oil, which is rich in O3FA improved the xerotic pruritus of healthy people and patients with ESRD or diabetes mellitus. Their epidermal permeability barrier function was also improved, which was assessed by skin capacitance and trans-epidermal water loss without adverse effect[24]. The benefits of antipruritic effect and increasing skin hydration with oral O3FA supplementation were also confirmed in the animal study, which was conducted with the rat model with dry skin induced by acetone[59]. EPA, an O3FA, by competing with arachidonic acid, can shift the synthesis pathway to promote the production of anti-inflammatory eicosanoids[18,25].
The previous clinical trials about O3FA supplementation in dialysis patients were suboptimal in study design, mostly because of the small sample sizes, uncontrolled groups, or the administered O3FA in the form of fish oil[18]. Our included studies were all conducted with capsule form with specific contents for O3FA supplementation. These studies showed that the O3FA supplement reduces the pruritus score and the severity of pruritus, though with low quality of evidence.
There are different types of measurements to assess the pruritus extent, including uni-dimensional, multi-dimensional, and other scales. However, there is still a lack of consensus to have a standard pruritus assessment tool[60]. Clinically, the common pruritus measurement tools for UP were numerical rating scale (NRS), VAS, DPS, and 5-DIS[51,52,61,62]. Our included studies used different tools for pruritus assessment, which may explain the high heterogeneity of our study. Therefore, to analyze the severity and therapeutic effects in different departments or studies, the transformation among these diverse pruritus measurements is required. Chang et al. proposed the categories for the transformation between 5-DIS and NRS according to itch severity in HD patients[61]. Lee et al. used the mapping model to successfully transform the pruritus assessment tool of VAS and EuroQol 5-dimension 3-level utility index[63]. Both of the transformation models could be taken for reference while conducting related studies in the future.
To our knowledge, there are few published meta-analyses about the antipruritic effect for UP, such as nalfurafine[17], gabapentin[7], acupressure[14], and CHBT[15]. This study is the first meta-analysis to evaluate the efficacy of O3FA supplements for pruritus control in CKD patients, and the result supported the benefits of oral O3FA and provided the reference dose of the supplement. However, this study also has limitations. First, the sample size of these articles is relatively small, so it can hardly give a crucial suggestion. Second, pruritus measurements in selected trials are all different and thus can barely assert a consistent result. Third, this meta-analysis only includes the UP patients with dialysis, whether our results are beneficial for UP patients of CKD remains unclear. Finally, the blinding procedure and publication bias of the chosen trials should be considered when explicating our results. Although having limitations, the DPS significantly improved in the O3FA supplementation group statistically. O3FA supplement showed the potential to improve the UP with easily accessible, low cost, and less adverse effects.
CONCLUSION
Our meta-analysis showed, with low-quality evidence, that O3FA supplementation significantly reduces pruritus in UP patients under the evaluation of the Duo pruritus scale. However, further trials with larger sample sizes and high-quality designs focused on the dosage of O3FA supplements for different methods of dialysis are recommended.
Financial support and sponsorship
This work was supported by grants from the Ministry of Science and Technology (MOST 108-2314-B-303-006-MY3), Taipei Tzu Chi Hospital (TCRD-TPE-MOST-109-08 and TCRD-TPE-110-03), Buddhist Tzu Chi Medical Foundation, Taiwan (TCMF-EP 109-01).
Conflicts of interest
Dr. Ko-Lin Kuo, an editorial board member at Tzu Chi Medical Journal, had no role in the peer review process of or decision to publish this article. The other authors declared no conflicts of interest in writing this paper.
Supplementary material available online
Acknowledgment
We thank all our colleagues at Mackay Memorial Hospital and Taipei Tzu Chi Hospital for helping with this study. We greatly appreciate technical support from the Core Laboratory of the Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation.
REFERENCES
- 1.Rayner HC, Larkina M, Wang M, Graham-Brown M, van der Veer SN, Ecder T, et al. International comparisons of prevalence, awareness, and treatment of pruritus in people on hemodialysis. Clin J Am Soc Nephrol. 2017;12:2000–7. doi: 10.2215/CJN.03280317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pisoni RL, Wikström B, Elder SJ, Akizawa T, Asano Y, Keen ML, et al. Pruritus in haemodialysis patients: International results from the dialysis outcomes and practice patterns study (DOPPS) Nephrol Dial Transplant. 2006;21:3495–505. doi: 10.1093/ndt/gfl461. [DOI] [PubMed] [Google Scholar]
- 3.Narita I, Iguchi S, Omori K, Gejyo F. Uremic pruritus in chronic hemodialysis patients. J Nephrol. 2008;21:161–5. [PubMed] [Google Scholar]
- 4.Mettang T, Kremer AE. Uremic pruritus. Kidney Int. 2015;87:685–91. doi: 10.1038/ki.2013.454. [DOI] [PubMed] [Google Scholar]
- 5.Malekmakan L, Tadayon T, Pakfetrat M, Mansourian A, Zareei N. Treatments of uremic pruritus: A systematic review. Dermatol Ther. 2018;31:e12683. doi: 10.1111/dth.12683. [DOI] [PubMed] [Google Scholar]
- 6.Simonsen E, Komenda P, Lerner B, Askin N, Bohm C, Shaw J, et al. Treatment of uremic pruritus: A systematic review. Am J Kidney Dis. 2017;70:638–55. doi: 10.1053/j.ajkd.2017.05.018. [DOI] [PubMed] [Google Scholar]
- 7.Eusebio-Alpapara KM, Castillo RL, Dofitas BL. Gabapentin for uremic pruritus: A systematic review of randomized controlled trials. Int J Dermatol. 2020;59:412–22. doi: 10.1111/ijd.14708. [DOI] [PubMed] [Google Scholar]
- 8.Nakhaee S, Nasiri A, Waghei Y, Morshedi J. Comparison of Avena sativa, vinegar, and hydroxyzine for uremic pruritus of hemodialysis patients: A crossover randomized clinical trial. Iran J Kidney Dis. 2015;9:316–22. [PubMed] [Google Scholar]
- 9.Tarng DC, Cho YL, Liu HN, Huang TP. Hemodialysis-related pruritus: A double-blind, placebo-controlled, crossover study of capsaicin 0.025% cream. Nephron. 1996;72:617–22. doi: 10.1159/000188949. [DOI] [PubMed] [Google Scholar]
- 10.Lu PH, Tai YC, Yu MC, Lin IH, Kuo KL. Western and complementary alternative medicine treatment of uremic pruritus: A literature review. Tzu Chi Med J. 2021;33:350–8. doi: 10.4103/tcmj.tcmj_151_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sinawang GW, Faizah R, Alfaqih MR, Hermanto A. Efficacy of topical applications on reducing uremic pruritus: A systematic review. J Ners. 2019;14:252–5. [Google Scholar]
- 12.Kimmel M, Alscher DM, Dunst R, Braun N, Machleidt C, Kiefer T, et al. The role of micro-inflammation in the pathogenesis of uraemic pruritus in haemodialysis patients. Nephrol Dial Transplant. 2006;21:749–55. doi: 10.1093/ndt/gfi204. [DOI] [PubMed] [Google Scholar]
- 13.Castellsague J, Kuiper JG, Pottegård A, Anveden Berglind I, Dedman D, Gutierrez L, et al. A cohort study on the risk of lymphoma and skin cancer in users of topical tacrolimus, pimecrolimus, and corticosteroids (Joint European Longitudinal Lymphoma and Skin Cancer Evaluation - JOELLE study) Clin Epidemiol. 2018;10:299–310. doi: 10.2147/CLEP.S146442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Badiee Aval S, Ravanshad Y, Azarfar A, Mehrad-Majd H, Torabi S, Ravanshad S. A systematic review and meta-analysis of using acupuncture and acupressure for uremic pruritus. Iran J Kidney Dis. 2018;12:78–83. [PubMed] [Google Scholar]
- 15.Xue W, Zhao Y, Yuan M, Zhao Z. Chinese herbal bath therapy for the treatment of uremic pruritus: Meta-analysis of randomized controlled trials. BMC Complement Altern Med. 2019;19:103. doi: 10.1186/s12906-019-2513-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kalili H, Dashti S, Poor PA, Babaei MH, Abdollahi F. Efficacy of anti-pruritis drugs in chronic renal failure: A comparative study. Tehran Univ Med J TUMS Publ. 2006;64:36–42. [Google Scholar]
- 17.Jaiswal D, Uzans D, Hayden J, Kiberd BA, Tennankore KK. Targeting the opioid pathway for uremic pruritus: A systematic review and meta-analysis. Can J Kidney Health Dis. 2016;3:2054358116675345. doi: 10.1177/2054358116675345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Friedman A, Moe S. Review of the effects of omega-3 supplementation in dialysis patients. Clin J Am Soc Nephrol. 2006;1:182–92. doi: 10.2215/CJN.00740805. [DOI] [PubMed] [Google Scholar]
- 19.Shahidi F, Ambigaipalan P. Omega-3 polyunsaturated fatty acids and their health benefits. Annu Rev Food Sci Technol. 2018;9:345–81. doi: 10.1146/annurev-food-111317-095850. [DOI] [PubMed] [Google Scholar]
- 20.Paixão E, Oliveira AC, Pizato N, Muniz-Junqueira MI, Magalhães KG, Nakano EY, et al. The effects of EPA and DHA enriched fish oil on nutritional and immunological markers of treatment naïve breast cancer patients: A randomized double-blind controlled trial. Nutr J. 2017;16:71. doi: 10.1186/s12937-017-0295-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Uwaezuoke SN, Muoneke UV, Mbanefo NR. The supportive treatment of IgA nephropathy and idiopathic nephrotic syndrome: How useful are omega-3 polyunsaturated fatty acids? Int J Nephrol Renovasc Dis. 2020;13:27–35. doi: 10.2147/IJNRD.S237527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Balić A, Vlašić D, Žužul K, Marinović B, Bukvić Mokos Z. Omega-3 versus omega-6 polyunsaturated fatty acids in the prevention and treatment of inflammatory skin diseases. Int J Mol Sci. 2020;21:741. doi: 10.3390/ijms21030741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Koch C, Dölle S, Metzger M, Rasche C, Jungclas H, Rühl R, et al. Docosahexaenoic acid (DHA) supplementation in atopic eczema: A randomized, double-blind, controlled trial. Br J Dermatol. 2008;158:786–92. doi: 10.1111/j.1365-2133.2007.08430.x. [DOI] [PubMed] [Google Scholar]
- 24.Jeong SK, Park HJ, Park BD, Kim IH. Effectiveness of topical chia seed oil on pruritus of end-stage renal disease (ESRD) patients and healthy volunteers. Ann Dermatol. 2010;22:143–8. doi: 10.5021/ad.2010.22.2.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Panahi Y, Dashti-Khavidaki S, Farnood F, Noshad H, Lotfi M, Gharekhani A. Therapeutic effects of omega-3 fatty acids on chronic kidney disease-associated pruritus: A literature review. Adv Pharm Bull. 2016;6:509–14. doi: 10.15171/apb.2016.064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Peck LW, Monsen ER, Ahmad S. Effect of three sources of long-chain fatty acids on the plasma fatty acid profile, plasma prostaglandin E2 concentrations, and pruritus symptoms in hemodialysis patients. Am J Clin Nutr. 1996;64:210–4. doi: 10.1093/ajcn/64.2.210. [DOI] [PubMed] [Google Scholar]
- 27.Begum R, Belury MA, Burgess JR, Peck LW. Supplementation with n-3 and n-6 polyunsaturated fatty acids: Effects on lipoxygenase activity and clinical symptoms of pruritus in hemodialysis patients. J Ren Nutr. 2004;14:233–41. [PubMed] [Google Scholar]
- 28.Ristić-Medić D, Perunicić-Peković G, Rasić-Milutinović Z. PUFA status and omega-3 fatty acid supplementation in hemodialysis patients: Pathophysiological aspects and clinical outcomes. Nutr Ther Metab. 2011;29:178–91. [Google Scholar]
- 29.Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. 2nd. Chichester (UK): John Wiley and Sons; 2019. Cochrane handbook for systematic reviews of interventions. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi: 10.1136/bmj.b2700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Laska E, Meisner M, Kushner HB. Optimal crossover designs in the presence of carryover effects. Biometrics. 1983;39:1087–91. [PubMed] [Google Scholar]
- 32.Liou JP, Mahindroo N, Chang CW, Guo FM, Lee SW, Tan UK, et al. Structure-activity relationship studies of 3-aroylindoles as potent antimitotic agents. Chem Med Chem. 2006;1:1106–18. doi: 10.1002/cmdc.200600125. [DOI] [PubMed] [Google Scholar]
- 33.Mettang T. Uremic itch management. Curr Probl Dermatol. 2016;50:133–41. doi: 10.1159/000446056. [DOI] [PubMed] [Google Scholar]
- 34.Kosmadakis GC, Zerefos N. Uremic pruritus. Int J Artif Organs. 2006;29:938–43. doi: 10.1177/039139880602901003. [DOI] [PubMed] [Google Scholar]
- 35.Vergili-Nelsen JM. Benefits of fish oil supplementation for hemodialysis patients. J Am Diet Assoc. 2003;103:1174–7. doi: 10.1016/s0002-8223(03)00984-2. [DOI] [PubMed] [Google Scholar]
- 36.Ristic-Medic D, Perunicic-Pekovic G, Rasic-Milutinovic Z, Takic M, Popovic T, Arsic A, et al. Effects of dietary milled seed mixture on fatty acid status and inflammatory markers in patients on hemodialysis. ScientificWorldJournal. 2014;2014:563576. doi: 10.1155/2014/563576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Siemens W, Xander C, Meerpohl JJ, Buroh S, Antes G, Schwarzer G, et al. Pharmacological interventions for pruritus in adult palliative care patients. Cochrane Database Syst Rev. 2016;11:CD008320. doi: 10.1002/14651858.CD008320.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Miller ER, 3rd, Juraschek SP, Anderson CA, Guallar E, Henoch-Ryugo K, Charleston J, et al. The effects of n-3 long-chain polyunsaturated fatty acid supplementation on biomarkers of kidney injury in adults with diabetes: Results of the GO-FISH trial. Diabetes Care. 2013;36:1462–9. doi: 10.2337/dc12-1940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Burrowes JD, Van Houten G. Use of alternative medicine by patients with stage 5 chronic kidney disease. Adv Chronic Kidney Dis. 2005;12:312–25. doi: 10.1016/j.ackd.2005.04.001. [DOI] [PubMed] [Google Scholar]
- 40.The Effect of Omega-3 and Hydroxyzine on the Degree and Severity of Pruritus in Hemodialysis Patients. 2018. Available from: http://wwwwhoint/trialsearch/Trial2aspx?TrialID=IRCT20180103038196N3 . [Last accessed on 2020 Apr 22]
- 41.Effect of Omega-3 on Uremic Pruritus Hemodialysis Patients. 2018. Available from: http://wwwwhoint/trialsearch/Trial2aspx?TrialID=IRCT20171220037968N1 . [Last accessed on 2020 Apr 22]
- 42.Effect of Omega-3 Fatty Acids on Uremic Pruritus. 2018. Available from: http://wwwwhoint/trialsearch/Trial2aspx?TrialID=IRCT20170609034406N2 . [Last accessed on 2020 Apr 22]
- 43.The Effect of Omega3 Supplementation on Uremic Pruritus and Sleep Quality. 2017. [Last accessed on 2020 Apr 22]. Available from: http://wwwwhoint/trialsearch/Trial2aspx?TrialID=IRCT2017040433206N1 .
- 44.Mortazavi M. Effect of Omega-3 on Pruritus Scale in Hemodialysis Patients. 2016. [Last accessed on 2020 Apr 22]. Available from: https://Ensearchirctir/view/15812 .
- 45.Effect of Omega-3 on Pruritus Scale in Hemodialysis Patients. 2016. [Last accessed on 2020 Apr 22]. Available from: http://wwwwhoint/trialsearch/Trial2aspx?TrialID=IRCT201311152417N14 .
- 46.Center A-HM. Treatment of Uremic Pruritus by Olive-omega 3 Ointment. 2011. [Last accessed on 2020 Apr 22]. Available from: https://www.clinicaltrials.gov/ct2/show/NCT01447693 .
- 47.Mojgan M, Masoud M, Shahrzad S, Zahra PH, Firouzeh M, Jinoos Z, et al. Pruritus-reducing effects of omega-3 fatty acids in hemodialysis patients. Iran J Kidney Dis. 2017;11:7–8. [Google Scholar]
- 48.Ghanei E, Zeinali J, Borghei M, Homayouni M. Efficacy of omega-3 fatty acids supplementation in treatment of uremic pruritus in hemodialysis patients: A double-blind randomized controlled trial. Iran Red Crescent Med J. 2012;14:515–22. [PMC free article] [PubMed] [Google Scholar]
- 49.Lahiji AP, Mortazavi M, Tirani SA, Moeinzadeh F, Bidaki EZ, Naini AE, et al. Omega-3 supplementation improves pruritus in continuous ambulatory peritoneal dialysis patients: A crossover randomized pilot clinical trial. J Res Pharm Pract. 2018;7:195–9. doi: 10.4103/jrpp.JRPP_18_64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Shayanpour S, Mousavi SS, Rizi PL, Cheraghian B. The effect of the omega-3 supplement on uremic pruritus in hemodialysis patients; a double-blind randomized controlled clinical trial. J Nephropathol. 2019;8:e13. [Google Scholar]
- 51.Duo LJ. Electrical needle therapy of uremic pruritus. Nephron. 1987;47:179–83. doi: 10.1159/000184487. [DOI] [PubMed] [Google Scholar]
- 52.Elman S, Hynan L, Gabriel V, Mayo M. The 5-D itch scale: A new measure of pruritus. Br J Dermatol. 2010;162:587–93. doi: 10.1111/j.1365-2133.2009.09586.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Patel TS, Freedman BI, Yosipovitch G. An update on pruritus associated with CKD. Am J Kidney Dis. 2007;50:11–20. doi: 10.1053/j.ajkd.2007.03.010. [DOI] [PubMed] [Google Scholar]
- 54.Wu HY, Peng YS, Chen HY, Tsai WC, Yang JY, Hsu SP, et al. A comparison of uremic pruritus in patients receiving peritoneal dialysis and hemodialysis. Medicine (Baltimore) 2016;95:e2935. doi: 10.1097/MD.0000000000002935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Rayner H, Baharani J, Smith S, Suresh V, Dasgupta I. Uraemic pruritus: Relief of itching by gabapentin and pregabalin. Nephron Clin Pract. 2012;122:75–9. doi: 10.1159/000349943. [DOI] [PubMed] [Google Scholar]
- 56.Thomsen BJ, Chow EY, Sapijaszko MJ. The potential uses of omega-3 fatty acids in dermatology: A review. J Cutan Med Surg. 2020;24:481–94. doi: 10.1177/1203475420929925. [DOI] [PubMed] [Google Scholar]
- 57.Balbás GM, Regaña MS, Millet PU. Study on the use of omega-3 fatty acids as a therapeutic supplement in treatment of psoriasis. Clin Cosmet Investig Dermatol. 2011;4:73–7. doi: 10.2147/CCID.S17220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Healy E, Newell L, Howarth P, Friedmann PS. Control of salicylate intolerance with fish oils. Br J Dermatol. 2008;159:1368–9. doi: 10.1111/j.1365-2133.2008.08830.x. [DOI] [PubMed] [Google Scholar]
- 59.Barcelos RC, de Mello-Sampayo C, Antoniazzi CT, Segat HJ, Silva H, Veit JC, et al. Oral supplementation with fish oil reduces dryness and pruritus in the acetone-induced dry skin rat model. J Dermatol Sci. 2015;79:298–304. doi: 10.1016/j.jdermsci.2015.06.015. [DOI] [PubMed] [Google Scholar]
- 60.Ständer S, Augustin M, Reich A, Blome C, Ebata T, Phan NQ, et al. Pruritus assessment in clinical trials: Consensus recommendations from the international forum for the study of itch (IFSI) special interest group scoring itch in clinical trials. Acta Derm Venereol. 2013;93:509–14. doi: 10.2340/00015555-1620. [DOI] [PubMed] [Google Scholar]
- 61.Lai JW, Chen HC, Chou CY, Yen HR, Li TC, Sun MF, et al. Transformation of 5-D itch scale and numerical rating scale in chronic hemodialysis patients. BMC Nephrol. 2017;18:56. doi: 10.1186/s12882-017-0475-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Khan TM, Al-Haider I, Syed Sulaiman SA, Hassali MA. Linguistic validation of the 5D itching scale to Arabic in patients with end-stage kidney disease. J Ren Care. 2013;39:222–7. doi: 10.1111/j.1755-6686.2013.12038.x. [DOI] [PubMed] [Google Scholar]
- 63.Park SY, Park EJ, Suh HS, Ha D, Lee EK. Development of a transformation model to derive general population–based utility: Mapping the pruritus–visual analog scale (VAS) to the EQ-5D utility. J Eval Clin Pract. 2017;23:755–61. doi: 10.1111/jep.12711. [DOI] [PubMed] [Google Scholar]