

Introduction
Glomus tumours are rare benign, mesenchymal soft tissue neoplasms of vascular origin constituting 1.6% of all soft tissue tumors.[1] They arise from modified smooth muscle cells present in the walls of specialized arterio-venous anastomoses (Sucquet-Hoyer canal) that are located in the subcutaneous tissue and are normally responsible for the regulation of temperature and blood pressure.[2] These tumors usually present as painful subcutaneous nodules in the subungual area of the digits and rarely involve extra-digital sites that are often misdiagnosed clinically.[3] In the present study, all the cases of digital and extra digital glomus tumours reported during the 5 year study period are analysed for all the salient clinical and pathological features.
Materials and Methods
A retrospective study of all lesions diagnosed as glomus tumor in the histopathological evaluation during the period between October 2015 and November 2020 was carried out in a tertiary care hospital. Glomus tumours involving both the digital and extra-digital sites were included. The clinical parameters and histopathological features were analysed with review of literature. Immunohistochemistry was carried out for confirmation.
Results
Total number of glomus tumors encountered in this study was six. Among them four tumors occurred in male with male: female ratio of 2:1 and the common age group affected was 20-40 years. [Table 1]
These tumors showed equal distribution in digital and extra-digital sites with two lesions located in the proximal interphalangeal joint of fingers, two lesions in the arm, one in the great toe and one in the post-auricular region. [Figure 1]
All the tumours presented clinically as reddish nodules associated with pain. Two of these lesions showed variation in the pain intensity relative to tactile stimulation (point tenderness) and temperature (cold sensitivity). [Table 2]
The size of these tumours varied from 0.5 cm to 5 cm in diameter. [Table 3]
Microscopically, all the six cases were of solid glomus tumour subtype with no glomangioma or glomangiomyoma reported in this study. They were well circumscribed tumor masses composed of monotonous population of round to ovoid cells with moderate eosinophilic cytoplasm and central round uniform nuclei arranged in sheets and nests separated by large number of thin walled compressed vessels and myxoid stroma. [Figures 2 and 3]
Immunohistochemistry was carried out to differentiate from other vascular lesions. Smooth Muscle Actin (SMA) showed diffuse strong cytoplasmic positivity in the tumor cells around the vessels while CD34 was negative in the tumor cells and it stained the normal endothelium alone. These features were consistent with that of Glomus tumor. [Figures 4 and 5]
All the six cases were treated by surgical excision following which they showed complete cure and were free of recurrences in the post-operative period.
Table 1.
Age distribution
| Number of cases | Percentage | |
|---|---|---|
| Age group | ||
| 0-20 years | 1 | 16.7% |
| 21-40 years | 5 | 83.3% |
| Total | 6 cases | 100% |
Figure 1.
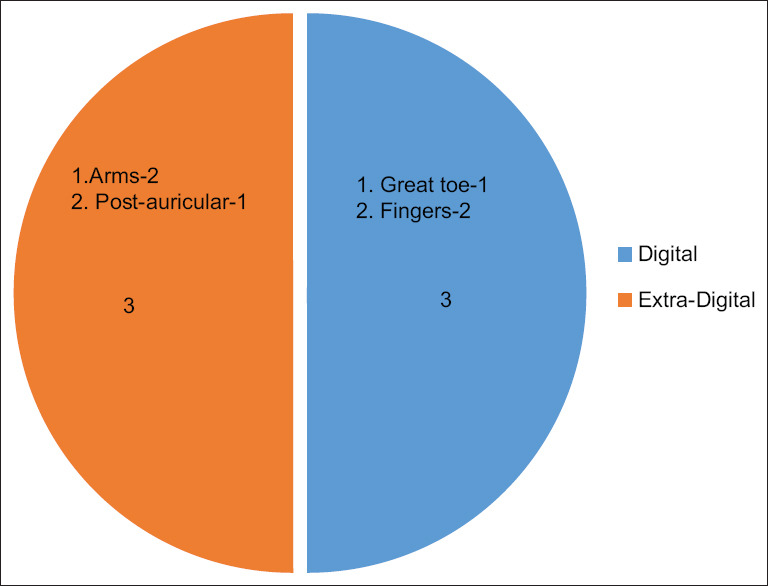
Site distribution of Glomus tumors
Table 2.
Clinical Presentation
| Clinical presentation | Present (No of Cases) | Absent (No of Cases) |
|---|---|---|
| Reddish nodule | 6 | - |
| Pain | 6 | - |
| More Pain on tactile stimulation | 2 | 4 |
| Cold sensitivity | 2 | 4 |
Table 3.
Tumor size
| Number of cases | Percentage | |
|---|---|---|
| Tumor size | ||
| ≤0.5 cm | 1 | 16.7% |
| >0.5 cm-2 cm | 4 | 66.6% |
| >2 cm | 1 | 16.7% |
| Total | 6 cases | 100% |
Figure 2.
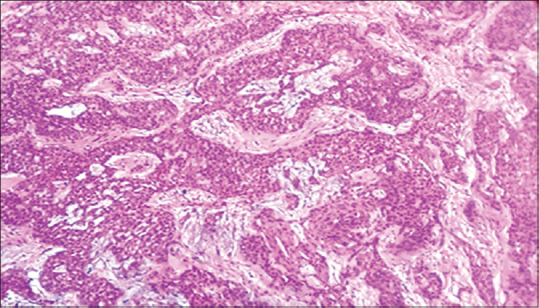
H and E, 10×- Solid sheets of tumor cells around compressed vessels and myxoid stroma
Figure 3.
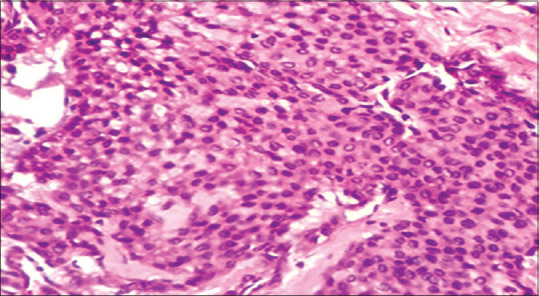
H and E, 40×- Tumor cells are round to ovoid with eosinophilic cytoplasm and central round nuclei
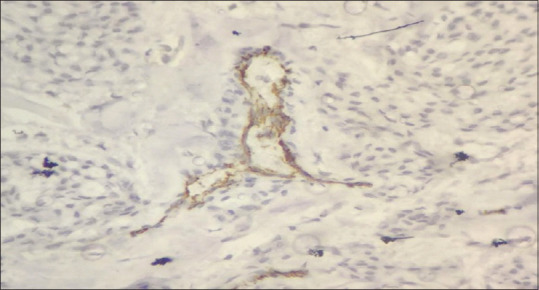
Figure 4.
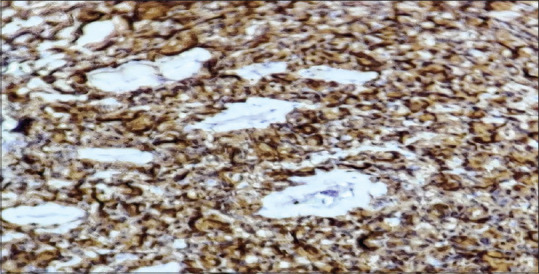
IHC, 40×- Smooth Muscle Actin positivity in tumor cells
Figure 5.
IHC, 40×- CD34 negative in tumor cells
Discussion
Glomus tumor is known as a benign and vascular hamartoma containing all the neuromyoarterial cells of the normal glomus apparatus.[1] These glomus bodies are contractile tissue and they are primarily responsible for the local temperature and blood pressure modulation and they accomplish this by controlling blood flow through microvasculature.[4] The aetiology of glomus tumors is unknown and it may be related to sex, age, trauma or inheritance. BRAF mutations are seen in some tumors.[2] Most of these tumors occur in adults aged 20-40 years similar to the present study with no sex predilection.[2] In the present study, male predominance was noted.
The common presentation of the tumor is painful red blue or purple coloured, subcutaneous nodules with a hard consistency.[5,6] Glomus tumours are mainly reported as small nodules which rarely exceed a diameter of 1 cm associated with paroxysmal pain in relation to tactile stimulation or temperature variation (cold sensitivity).[7] All these findings were in concurrence with the present study.
Glomus tumours mainly arise in the dermis or subcutaneous tissues of the hands and feet, especially the tips of fingers and toes. Extra-digital glomus tumours are rare; less than 1% of glomus tumours are found in the head region.[8,9] In the present study, there was an equal incidence of glomus tumours in digital and extra-digital sites.
Histological study reveals a variable composition of glomus cells, blood vessels and smooth muscles. Based on the relative proportion of the three constituents, glomus tumours are categorised into three subtypes-Glomangiomas with an abundance of vessels; solid glomus tumour which is chiefly composed of glomus cells and Glomangiomyomas showing a predominance of smooth muscles.[10,11] In the present study, all belonged to the subtype of solid glomus tumor. A typical solid glomus tumour is composed of small vascular channels surrounded by clusters of well-defined round cells with lightly eosinophilic cytoplasm and a large central round or oval nucleus with no atypia.[11,12]
The immunohistochemical profile of glomus tumour cells includes positivity for vimentin, smooth muscle actin, and muscle-specific actin.[13] Some of the tumours showed positive results for desmin and CD34. Conversely, these tumours yield negative results for S-100, myoglobin, neurofilaments and factor VIII-related antigen.[14]
Complete surgical excision is the curative treatment of choice for glomus tumours. Incomplete excision is considered the main cause of recurrence.[14] Malignant transformation is uncommon and usually carries a benign course.[15]
Various clinical differential diagnoses include a neural tumor such as a neurofibroma, vascular tumor including haemangioma, angioma or haemangiopericytoma, plantar fasciitis, leiomyoma or metastasis.[11] Thus, glomus tumour should be considered in the differential diagnosis of any painful soft tissue mass.[15]
Conclusion
Glomus tumours are rare tumours with a classic clinical presentation and typical symptoms of long-term pain and sensitivity to touch. The diagnosis of extra-digital glomus tumours remains a challenge for clinicians. Their unusual location and non-specific clinical findings, except for pain, make the diagnosis difficult. Therefore, proper history, clinical examination and high index of suspicion are essential for the correct clinical diagnosis, while histopathology confirms the diagnosis of glomus tumour. Inspite of its rare occurrence, glomus tumour should always be kept in mind for the differential diagnosis of all painful subcutaneous lesions especially for those with purple reflection on the skin surface so that proper treatment could be offered to the patient following proper diagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Friske JE, Sharma V, Kolpin SA, Webber NP. Extradigital glomus tumor: A rare etiology for wrist soft tissue mass. Radiol Case Rep. 2016;11:195–200. doi: 10.1016/j.radcr.2016.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fletcher CDM. Pathology and genetics of tumours of soft tissue and bone. Lyon: IARC Press; 2013. [Google Scholar]
- 3.Liapiavgeri G, Karabelabouropoulou V, Agnanti N. Glomus tumor. A histological, histochemical and immunohistochemical study of the various types. Pathol Res Pract. 1994;190:2–10. doi: 10.1016/S0344-0338(11)80490-5. [DOI] [PubMed] [Google Scholar]
- 4.Weiss SW, Goldblum JR. Perivascular tumors Enzinger and Weiss's Soft tissue tumors. 5th ed. Maryland Heights, MO: Mosby; 2007. pp. 751–6. [Google Scholar]
- 5.Temiz G, Şirinoğlu H, Demirel H, Yeşiloğlu N, Sarıcı M, Filinte GT. Extradigital glomus tumor revisited: Painful subcutaneous nodules located in various parts of the body. Indian J Dermatol. 2016;61:118. doi: 10.4103/0019-5154.174080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Calonje E. 10th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2009. Vascular Tumors: Tumors and Tumor-Like Conditions of Blood Vessels and Lymphatics-Lever's Histopathology of the Skin; pp. 1047–9. [Google Scholar]
- 7.Gombos Z, Zhang PJ. Glomus tumor. Archiv Pathol Lab Med. 2008;132:1448–52. doi: 10.5858/2008-132-1448-GT. [DOI] [PubMed] [Google Scholar]
- 8.Zou H, Song L, Jia M, Wang L, Sun Y. Glomus tumor in the floor of the mouth: A case report and review of the literature. World J Surg Oncol. 2018;16:201. doi: 10.1186/s12957-018-1503-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Caughey DE, Highton TC. Glomus tumour of the knee. Report of a case. J Bone Joint Surg Br. 1966;48:134–7. [PubMed] [Google Scholar]
- 10.Morey VM, Garg B, Kotwal PP. Glomus tumours of the hand: Review of literature. J Clin Orthop Trauma. 2016;7:286–91. doi: 10.1016/j.jcot.2016.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Perks FJ, Beggs I, Lawson GM, Davie R. Juxtacortical glomus tumor of the distal femur adjacent to the popliteal fossa. Am J Roentgenol. 2003;181:1590–92. doi: 10.2214/ajr.181.6.1811590. [DOI] [PubMed] [Google Scholar]
- 12.Chakrapani A, Warrick A, Nelson D, Beadling C, Corless CL. BRAF and KRAS mutations in sporadic glomus tumors. Am J Dermatopathol. 2012;34:533–5. doi: 10.1097/DAD.0b013e31823931b4. [DOI] [PubMed] [Google Scholar]
- 13.Rallis G, Komis C, Mahera H. Glomus tumor: A rare location in the upper lip. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2004;98:327–36. doi: 10.1016/S1079210404001027. [DOI] [PubMed] [Google Scholar]
- 14.El Jouari O, Gallouj S, Elloudi S, Senhaji G, Rimani M, Mernissi FZ. A painless glomus tumor: A case report. J Med Case Rep. 2018;12:302. doi: 10.1186/s13256-018-1837-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Amillo S, Arriola FJ, Munoz G. Extradigital glomus tumour causing thigh pain. Bone Joint J. 1997;79:104–6. doi: 10.1302/0301-620x.79b1.6951. [DOI] [PubMed] [Google Scholar]