

Abstract
Objectives
Self‐compassion constitutes a positive way of relating towards the self that enables emotional regulation and reduces emotional distress. This research first explored differences among a sample of persons with social anxiety disorder (SAD) and groups of high socially anxious (HSA) and low socially anxious (LSA) students on self‐compassion, emotion regulation, and social anxiety. We then investigated emotional regulation as a mediator of the prediction of social anxiety by self‐compassion and the influence of depressed mood on those relationships.
Design
Study 1 compared a SAD group to matched groups of HSA and LSA students. Study 2 utilized the total sample (n = 330 students and n = 33 SAD) to test mediation. Self‐compassion and emotion regulation were predictors of social anxiety and depression a covariate.
Results
In Study 1, the SAD group did not differ from the HSA group on most aspects of self‐compassion and emotional regulation but was higher on depression. Both were lower on most measures and higher on depression than the LSA group. In Study 2, higher self‐compassion predicted lower social interaction anxiety, and emotional regulation strategies mediated this effect, regardless of depression. However, for social performance anxiety, controlling for depression removed mediation. Refraining from uncompassionate responses was directly connected to social anxiety, whereas compassionate responses influenced social anxiety via emotional regulation.
Conclusions
Results affirm the ameliorative role of self‐compassion on social anxiety and emotion regulation strategies as mechanisms of that influence. However, self‐compassion's influence was affected by depression and type of social anxiety. Also, refraining from uncompassionate self‐responding appears to be of prime importance in predicting social anxiety, whereas compassionate self‐responding influences social anxiety via emotion regulation.
Keywords: attitude to self, depression, emotion regulation, self‐compassion, social anxiety
Practitioner points.
Self‐compassion can alleviate social anxiety directly and indirectly via the emotional regulation strategies of activating cognitive reappraisal and limiting expressive suppression.
The benefits of self‐compassion and emotion regulation are influenced by depression and the type of social anxiety experienced. Depression has a stronger influence on social performance anxiety than social interaction anxiety.
Refraining from uncompassionate self‐judgement, overidentification with emotions, and emphasizing a sense of isolation directly reduce symptoms of social anxiety.
Acts of self‐kindness, mindful balanced thinking, and a sense of common humanity influence social anxiety via emotional regulation strategies, especially cognitive reappraisal.
BACKGROUND
Social anxiety is characterized by a pervasive fear of behaving in a way that garners negative evaluation from others (American Psychiatric Association, 2022). As a clinical condition, social anxiety disorder (SAD) is one of the most frequently diagnosed anxiety disorders (Crome et al., 2015; McEvoy et al., 2011), with an estimated lifetime prevalence of 8.4% (Crome et al., 2015). The level of distress caused by social anxiety across the community ranges from subthreshold to clinical levels, and impairment in social and occupational functioning can be mild to severe (Fehm et al., 2008). SAD is often comorbid with other conditions, especially depression (Belzer & Schneier, 2004; Dryman & Heimberg, 2018). Longitudinal research shows that a primary diagnosis of SAD increases the risk of subsequent depression (Beesdo et al., 2007) and when depression and SAD co‐occur, functional impairment is greater and the prognosis is poorer (Adams et al., 2016; Koyuncu et al., 2015; Norton et al., 2008).
Several theoretical models have identified impaired emotional regulation as important in the development and maintenance of SAD (e.g., Heimberg et al., 2010; Hofmann et al., 2012). Socially anxious individuals demonstrate great difficulty in identifying, understanding, and tolerating their negative emotions and experience low levels of positive emotion. As similar impairments are evident in depression, poor emotion regulation has been suggested as a common underlying mechanism in the co‐occurrence of social anxiety and depression (Dryman & Heimberg, 2018). There are, however, differences in the deficits in emotion regulation associated with the two conditions. For example, whereas individuals with SAD consistently engage in attempts to suppress the expression of their emotions, expressive suppression is not universal among depressed individuals and is heavily influenced by the context and symptom severity. Moreover, the limited positive affect in those with SAD remains evident controlling for depression.
This study was a replication and extension of a recent study by Bates et al. (2021) who identified self‐compassion as a form of emotional regulation that predicted social anxiety and was partially mediated by the specific emotion regulation strategies of cognitive reappraisal and expressive suppression of emotion. Given the substantial overlap between social anxiety and depression, we also examined the influence of depressed mood on these relationships.
Self‐compassion and social anxiety
Although defined in many ways (Gilbert, 2017), self‐compassion is generally seen as a positive way of reducing emotional distress that involves a sensitivity to the experience of suffering coupled with a desire to alleviate that suffering (Gilbert, 2014a). Two alternative models have been formulated to describe how self‐compassion influences emotional distress. Gilbert's developmental model of compassion proposes that self‐compassion incorporates the capacity to self‐soothe when distressed and the inhibition of self‐criticism. These capacities are believed to be determined by early attachment experiences with caregivers. Effective parenting creates securely attached children through consistent soothing of distress and assistance with environmental mastery and is the basis of self‐soothing in adulthood. It also affects the capacity to receive compassion from others and to act compassionately towards others. However, ineffective parenting, which is commonly the case in people who develop SAD (Spence & Rapee, 2016), inhibits the capacity to self‐soothe and this underlies deficiencies in emotional regulation.
Neff's alternative model shares Gilbert's definition of self‐compassion and acknowledges attachment experiences as the source of compassionate response (Neff & Dahm, 2015). However, Neff's model focuses on self‐directed compassion. Drawing on Buddhist philosophy, Neff specifies three ways in which people act to protect their personal health and well‐being in times of stress (Neff, 2003; Neff et al., 2018). In Neff's model, self‐compassion involves acting with self‐kindness by emphasizing self‐understanding and warmth and refraining from negative self‐judgement and self‐criticism. Self‐compassion also involves an ability to connect with the universality of human suffering by recognizing that difficult experiences are common to all and to resist feelings of being isolated from others. The third component of self‐compassion in Neff's model is the capacity to keep negative experiences in mindful awareness rather than over‐identifying with the negative emotions and feeling overwhelmed by distress. Together, these elements of self‐compassion help the person to identify constructive actions that alleviate distress. These actions are not aimed at feeling good but rather are directed at acting in ways that are necessary to address problems. As such, self‐compassion can involve approaching rather than avoiding difficult situations when this is deemed necessary (Adie et al., 2021).
There is evidence that self‐compassion is linked to social anxiety and treatments aimed at increasing self‐compassion can produce reductions in symptoms of social anxiety. Using Neff's measure of self‐compassion, Werner et al. (2012) reported lower levels of self‐compassion in a clinical sample of clients with SAD relative to a group of people without psychiatric diagnoses. In the Werner et al. study, the total self‐compassion score was not correlated with social anxiety symptoms in the clinical sample and only the subscales of self‐judgement and isolation showed significant negative correlations with symptoms. However, significant negative correlations have been reported between self‐compassion and social anxiety symptoms in samples of college students receiving counselling (Hayes et al., 2016) and in outpatients with SAD (Makadi & Koszycki, 2020). In addition, Blackie and Kocovski (2018) found self‐compassion to be associated with increased post‐event processing by socially anxious individuals characterized by prolonged negative rumination. Findings that self‐compassion interventions can significantly reduce such post‐event processing and alleviate symptoms of social anxiety (Boersma et al., 2015; Stevenson et al., 2019) attest to the strength of the association between self‐compassion and social anxiety.
Self‐compassion, emotion regulation strategies, and social anxiety
In validating her measure of self‐compassion, Neff (2003) reported significant positive correlations between self‐compassion and adaptive emotion regulation strategies (e.g., emotion approach coping) and negative correlations with maladaptive strategies (e.g., rumination and suppression). However, until recently, the effects of specific emotion regulation strategies on social anxiety have been investigated independently of self‐compassion. The most prominent model of emotion regulation explored in relation to SAD has been the Revised Process Model of Emotion Regulation (RPMER; Gross, 2015) and the specific strategies of cognitive reappraisal and expressive suppression (Dryman & Heimberg, 2018). In the RPMER cognitive reappraisal reframes appraisals of a situation to alter their emotional impact, thus changing negative emotions to neutral or positive emotions. Expressive suppression is a behavioural strategy that inhibits outward emotional expression.
While cognitive reappraisal is usually adaptive for socially anxious people, expressive suppression is not. Trying to conceal experiences of emotion increases the intensity of anxious emotion by exacerbating negatively focused self‐consciousness (Jazaieri et al., 2015) and dampens the experience of positive emotions in social situations (Gilboa‐Schechtman et al., 2020). Not surprisingly, a review of the literature by Dryman and Heimberg (2018) found that socially anxious individuals consistently engage in expressive suppression. However, there is evidence that socially anxious individuals utilize cognitive reappraisal less frequently than non‐socially anxious people, but this is not always the case. Dryman and Heimberg suggested that socially anxious individuals utilize cognitive reappraisal in response to negative emotions, but the strategy is less effective because they lack confidence in their ability to influence their negative emotions.
By definition, self‐compassion involves a commitment to act to decrease suffering (Gilbert, 2014a). It is an active approach‐oriented approach to emotional regulation (Neely et al., 2009) which, theoretically, should be connected to the use of specific strategies to reduce negative emotions (Berking & Whitley, 2014; Finlay‐Jones, 2017). There is some evidence that emotional regulation strategies and deficiencies mediate the effect of self‐compassion on symptoms of psychopathology. Inwood and Ferrari's (2018) systematic review of five published studies established that deficiencies in emotional regulation partially mediate the impact of self‐compassion on depression (Diedrich et al., 2017), stress (Finlay‐Jones et al., 2015), and PTSD symptoms (Barlow et al., 2017). Subsequently, Bates et al. (2021) examined the mediational role of cognitive reappraisal and expressive suppression in relation to social anxiety. They found that overall self‐compassion alleviated social anxiety directly and indirectly through expressive suppression but not through cognitive reappraisal. Exploratory analyses of self‐compassion divided into subcomponents of compassionate self‐responding (CSR) and refraining from uncompassionate responding (RUSR) suggested a mediational role for cognitive reappraisal as well as expressive suppression. RUSR was a direct and indirect predictor of social anxiety via cognitive reappraisal and expressive suppression whereas CSR was fully mediated by cognitive reappraisal. The use of the short form of the self‐compassion scale precluded further examination of the individual subcomponents of self‐compassion and Bates et al. (2021) encouraged the incorporation of the full measure of self‐compassion to explicate these relationships. They also recommended further examination of potential differences between clinical and non‐clinical samples on self‐compassion and emotional regulation.
The present study
The present study builds on Bates et al. (2021) by further examining relationships among self‐compassion, emotional regulation, and social anxiety. In this study, we utilized the long form of Neff's measure of self‐compassion (Neff, 2003) to investigate relationships among the individual components of self‐compassion as well as total scores. We also investigated the influence of depressed mood on those relationships. In addition, we conducted a comparison of scores on self‐compassion and emotion regulation in a treatment‐seeking clinical group of persons with SAD with matched groups of high socially anxious (HAS) and low socially anxious (LSA) students.
The research was conducted in two studies. As a preliminary study, Study 1 examined differences in self‐compassion and emotional regulation between a treatment‐seeking clinical group of persons with SAD and matched groups of HSA and LSA students. The SAD group was expected to display the lowest levels of self‐compassion, followed by the HSA group, then the LSA group. Similarly, the SAD group was expected to use Expressive Suppression most frequently and Cognitive Reappraisal least frequently, followed by the HSA group, then the LSA group. Study 2 used mediation analysis to investigate self‐compassion and emotional regulation as predictors of social anxiety. Based on Bates et al. (2021), total self‐compassion was expected to directly predict social anxiety and Expressive suppression to provide an indirect pathway for total self‐compassion to reduce social anxiety. Depressed mood was expected to correlate with social anxiety and was included as a covariate to identify unique and shared relationships among the forms of emotional regulation. Exploratory analyses examined the predictive role of the six individual components in the mediation models.
METHOD
Participants and procedure
Participants included undergraduate students and treatment‐seeking individuals with SAD, constituting a total sample of 164 men and 197 women aged from 18 to 73 years (N = 363, M = 28.40, SD = 12.31). Undergraduate students were invited to participate in a well‐being project conducted over two semesters in 2019 and 2020. All enrolled higher education students received an email describing the questionnaire, and those choosing to participate accessed an online survey containing the measures examined in this study. An information sheet explained that consent was implied by submitting the completed survey. The student sample comprised 145 men and 183 women ranging from 18 to 73 years of age (M = 28.05, SD = 12.46, n = 330).
The clinical group comprised treatment‐seeking individuals diagnosed with SAD in mid‐January 2020 (n = 33). Referrals came from health professionals or were self‐referrals in response to online advertisements. SAD diagnoses were established by a clinical interview for social anxiety and the Mini International Neuropsychiatric Interview‐5 (Sheehan et al., 1998) administered by provisional clinical psychologists. Participants with high depression, alcohol use, or suicidality were excluded. The sample comprised 19 men and 14 women ranging from 19 to 62 years of age (M = 31.85, SD = 10.27). These participants completed the measures examined in this study as part of an online questionnaire administered during the selection process.
Measures
Social anxiety
The Social Interaction Anxiety Scale (SIAS) and Social Phobia Scale (SPS) developed by Mattick and Clarke (1998) measured social anxiety. These measures are frequently used with non‐clinical and clinical samples and together provide a comprehensive assessment of social anxiety symptoms (Heimberg & Becker, 2002). Internal consistency, test–retest reliability and construct validity have been demonstrated across many studies (Modini et al., 2015). The SIAS is a 20‐item scale measuring social anxiety in social interactions including dyads and groups. Items are rated on a 5‐point Likert‐type scale ranging from 0 (Not at all characteristic or true of me) to 4 (Extremely characteristic or true of me) with three items reverse scored. The SPS is a 20‐item scale measuring fears of being observed or scrutinized during routine activities (e.g., eating, drinking, and writing) that uses the same 5‐point Likert‐type scale as the SIAS. The measures differ by the contingency of the social interaction. SIAS taps anxiety within contingent interactions that require continuous monitoring of one's behaviour in accordance with how others behave. Fears underpinning SPS emerge in non‐contingent interactions where behaviour is predominantly guided by one's own plans and is minimally affected by the behaviour of others (Reilly et al., 2012). As shown in Table 3, in this study Cronbach's alpha was .93 for the SIAS and .94 for the SPS.
TABLE 3.
Descriptive statistics, Cronbach's alpha reliability coefficients, and correlations for all variables
| Variable | α | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. SIAS | .93 | 34.96 | 16.9 | – | |||||||||||
| 2. SPS | .94 | 24.25 | 16.2 | .73** | – | ||||||||||
| 3. Depression | .92 | 8.25 | 8.1 | .64** | .58** | – | |||||||||
| 4. Self‐Compassion Total | .79 | 17.68 | 4.1 | −.60** | −.46** | −.53** | – | ||||||||
| 5. Common Humanity | .82 | 3.01 | 0.97 | −.36** | −.20** | −.36** | .72** | – | |||||||
| 6. Mindfulness | .79 | 3.15 | 0.80 | −.34** | −.31** | −.40** | .75** | .69** | – | ||||||
| 7. Self‐Kindness | .83 | 2.96 | 0.87 | −.42** | −.28** | −.42** | .80** | .75** | .77** | – | |||||
| 8. Self‐Judgement | .87 | 2.85 | 0.94 | −.53** | −.41** | −.39** | .79** | .30** | .37** | .49** | – | ||||
| 9. Over‐Identification | .80 | 2.86 | 0.93 | −.52** | −.43** | −.41** | .79** | .33** | .40** | .42** | .72** | – | |||
| 10. Isolation | .74 | 2.85 | 0.94 | −.51** | −.42** | −.40** | .66** | .20** | .20** | .25** | .65** | .63** | – | ||
| 11. Cognitive Reappraisal | .89 | 27.82 | 7.22 | −.48** | −.40** | −.47** | .61** | .44** | .54** | .54** | .42** | .46** | .34** | – | |
| 12. Expressive Suppression | .76 | 15.87 | 5.32 | .37** | .24** | .26** | −.27** | −.23** | −.09 | −.30** | −.27** | −.13* | −.19** | −.09 | – |
p < .05.
p < .01.
Self‐Compassion scale
The Self‐Compassion Scale (SCS; Neff, 2003) is a 26‐item self‐report measure employing a 5‐point Likert‐type scale ranging from 1 (Almost never) to 5 (Almost always). Three of the six subscales are positively worded: Self‐Kindness, Common Humanity, and Mindfulness, and three are negatively worded: Isolation, Over‐Identification, and Self‐Judgement. An overall self‐compassion score is calculated by reverse coding responses to the negatively worded items, calculating the mean for each of the six subscales and summing the means. The SCS has demonstrated good to excellent internal consistency for total scores (alpha ranging from .75 to .92) and its subscales (alpha ranges from .75 to .81) and has excellent test–retest reliability (r = .93 total score and from r = .80 to .88 for subscales; Neff, 2003; Neff et al., 2018). Neff and colleagues have reported strong convergent validity with measures of emotional well‐being, emotional intelligence, and positive self‐concept (Neff, 2016; Neff et al., 2018). Although some studies have identified a two‐factor structure related to positively and negatively worded items (Muris & Petrocchi, 2017) Neff et al. (2019) confirmed a single and six‐factor solution in a sample of 11,685 participants across 20 countries. In the present study Cronbach's alpha was .79 for the total score and ranged from .74 to .87 for the subscales (see Table 3).
Emotion Regulation Questionnaire (ERQ)
The Emotion Regulation Questionnaire (Gross & John, 2003) is a 10‐item measure rated on a 7‐point scale ranging from 1 ‘Strongly disagree’ to 7 ‘Strongly agree’, that assesses the emotion regulation strategies of cognitive reappraisal and expressive suppression. Gross and John (2003) reported good Cronbach's alpha reliability and construct validity with a clear two‐factor structure. Other studies report good to excellent internal consistency in student and community samples ranging from .89 to .90 for Cognitive Reappraisal and .76 to .84 for Expressive Suppression (De Castella et al., 2013; Kneeland et al., 2016; Zahniser & Conley, 2018). In this study, Cronbach's alpha was .89 for Cognitive Reappraisal and .76 for Expressive Suppression.
Depression Subscale of the Depression Anxiety Stress Scales‐21
The Depression Subscale of the Depression Anxiety Stress Scale (DASS; Lovibond & Lovibond, 1995) depression subscale is a 7‐item self‐report measure of depressive symptoms experienced over the past week. Items are rated on a 4‐point severity‐frequency scale ranging from 0 ‘Strongly disagree’ to 4 ‘Strongly agree’. Internal consistency and concurrent validity of the DASS‐21 are acceptable to excellent (Akin & Çetın, 2007). In this study, Cronbach alpha was .92.
Statistical analyses
All measures were checked for outliers and kurtosis and skewness. The measures were found to be approximately normally distributed.
Study 1 included the SAD group and two groups of students taken from the student sample. These groups were formed using SIAS and SPS scores. Participants scoring 34 or more on the SIAS and 24 or more on the SPS were above established social anxiety cut‐offs (Heimberg & Becker, 2002) and formed a ‘high socially anxious’ (HSA) group. Participants scoring below those cut‐offs formed a ‘low socially anxious’ (LSA) group. The three groups were matched on age (F[2, 98] = .060, p = .942) and gender (X 2 [2, N = 101] = .03, p = .987). Overall, Study 1 involved 101 participants aged between 19 and 62 (M = 31.44, SD = 9.96), including 57 men and 44 women. The SAD group included 33 participants, and the LSA and HSA groups each had 34 participants. Although one treatment‐seeking individual with SAD was removed from the analysis due to missing data, there were no other missing data. A MANOVA examined group differences on SIAS, SPS, and depression. Depression was then entered as a covariate in all subsequent analyses. A one‐way between groups univariate ANOVA and an ANCOVA compared groups on total self‐compassion. Two MANOVAS and MANCOVAs were computed: The first analysis involved the six self‐compassion subscales as dependent variables and the second used CR and ES as dependent variables. Repeated contrasts were used to compare the LSA group to the HSA group, and the HSA group to the SAD group. A simple contrast was used to compare the SAD group to the LSA group.
The student sample and the SAD sample were combined in Study 2 creating a total sample of 363 (n = 330 students, n = 33 SAD). Relationships among measures were first examined using bivariate Pearson correlations. The mediation of Cognitive reappraisal and Expressive suppression for self‐compassion and social anxiety were then investigated with non‐parametric mediation analyses using the PROCESS v3.5 (Model 4) macro for SPSS (Hayes, 2017). Separate mediation analyses were conducted for SIAS and SPS, with self‐compassion as the predictor and Cognitive reappraisal and Expressive suppression mediators. Depression was a covariate in both analyses. This model used 5000 bootstrapped samples and percentile‐based 95% confidence intervals. Mediation analysis was repeated for each self‐compassion subscale.
A priori Power analyses were conducted using G*Power's procedure for MANOVA comparisons (Faul et al., 2007). For three groups with two, three, and six measures the required sample sizes were 66, 75, and 93 participants with power (0.95) to detect a medium effect (ƒ2 = 0.15) at an alpha of .05. For the mediations, we applied a rule of thumb of 20 participants for each parameter in the model (Kline, 2005) which yielded a required total of 180 participants.
RESULTS
Study 1: Group differences on depression, self‐compassion, and emotional regulation
A MANOVA yielded a significant group difference on depression and social anxiety, Pillai's Trace = 1.15, F(6, 194) = 43.54, p < .001, η2 = .57. For both measures of social anxiety, repeated contrasts indicated that the SAD group did not differ from the HSA group and these two groups were significantly higher than the LSA group. Repeated contrasts also indicated that depression was significantly higher in the SAD group compared to HSA and LSA groups (see Table 1). This justified entering depression as a covariate in all subsequent analyses.
TABLE 1.
Descriptive statistics by group
| Variables | Low SA group | High SA group | SAD group | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| Social Interaction Anxiety | 16.82** | 8.35 | 52.35 | 10.33 | 53.88 | 9.06 |
| Social Phobia | 8.26** | 6.77 | 38.85 | 15.90 | 35.48 | 14.33 |
| Depression | 3.56** | 4.38 | 13.53** | 4.96 | 24.79 | 10.29 |
| Self‐Compassion Total | 20.30** | 3.51 | 14.04 | 4.76 | 14.33 | 2.80 |
| Common Humanity | 3.13* | 0.96 | 2.52 | 1.16 | 2.35 | 0.72 |
| Mindfulness | 3.35 | 0.82 | 2.85 | 0.91 | 2.47 | 0.71 |
| Self‐Kindness | 3.18** | 0.75 | 2.21 | 0.87 | 2.30 | 0.68 |
| Self‐Judgement | 3.62** | 0.70 | 1.95** | 0.73 | 2.48 | 0.78 |
| Over‐Identification | 3.43** | 0.92 | 2.28 | 0.81 | 2.32 | 0.77 |
| Isolation | 3.60** | 0.79 | 2.24* | 0.99 | 2.41 | 0.84 |
| Cognitive Reappraisal | 31.26* | 6.43 | 21.76 | 10.42 | 21.58 | 7.02 |
| Expressive Suppression | 13.62 | 5.55 | 16.65 | 5.54 | 17.12 | 5.87 |
Note: N = 101; *p < .05, **p < .001. A significant effect for the low SA group represents a significant difference between the low and high SA group. A significant effect for the high SA group represents a significant difference between the high SA group and the SAD group.
Abbreviations: SA, Social Anxiety; SAD, Social Anxiety Disorder.
A between‐groups ANCOVA revealed a group difference on total self‐compassion, F(2, 98) = 29.51, p < .001, η2 = .38. Repeated contrasts indicated that the LSA group scored significantly higher on total self‐compassion than the HSA group. However, contrary to expectation, there was no difference between the HSA and SAD groups. The pattern of group differences was the same without the depression covariate, F(2, 97) = 12.72, p < .001, η2 = .21.
A MANOVA examining the subcomponents of self‐compassion revealed a significant overall group difference, Pillai's Trace = .676, F(12, 188) = 8.00, p < .001, η2 = .338. All univariate results were significant. As expected, the LSA group was significantly higher on each component of self‐compassion than the HSA and SAD groups. Once more, contrary to prediction, the HSA and SAD groups did not differ on five of the six components. Interestingly, on self‐judgement, the HSA group scored lower than the SAD group (indicative of higher self‐judgement). A MANCOVA also revealed a significant overall group difference, Pillai's Trace = .50, F(12, 186) = 5.22, p < .001, η2 = .25. However, there were no group differences for mindfulness and common humanity in the univariate analyses (see Table 2). The LSA group scored higher than the SAD and HSA groups on all subscales except mindfulness (p > .05). Compared to the SAD group, the HSA group was significantly lower on the self‐compassion subscales of refraining from self‐judgement and isolation.
TABLE 2.
Between‐subjects effects by group controlling for depression
| Variable | F | p | η2 |
|---|---|---|---|
| Social Interaction Anxiety | (2, 98) = 172.34* | <.001** | .78 |
| Social Phobia | (2, 98) = 56.86* | <.001** | .54 |
| Depression | (2, 98) = 76.58* | <.001** | .61 |
| Self‐Compassion Total | (2, 97) = 12.72* | <.001** | .21 |
| Common Humanity | (2, 97) = 2.38 | .098 | .05 |
| Mindfulness | (2, 97) = 1.77 | .18 | .04 |
| Self‐Kindness | (2, 97) = 7.76* | <.001** | .14 |
| Self‐Judgement | (2, 97) = 30.44* | <.001** | .39 |
| Over‐Identification | (2, 97) = 8.59* | <.001** | .15 |
| Isolation | (2, 97) = 10.98* | <.001** | .19 |
| Cognitive Reappraisal | (2, 97) = 4.79* | <.01* | .09 |
| Expressive Suppression | (2, 97) = 0.83 | .44 | .02 |
p < .05.
p < .001.
In the second MANOVA, there was a significant overall group difference for Cognitive Reappraisal and Expressive Suppression Pillai's Trace = .299, F(4, 196) = 8.61, p < .001, η2 = .15. As expected, the LSA group scored higher than the HSA and SAD groups on Cognitive Reappraisal and lower on Expressive Suppression. Again, contrary to prediction, the HSA and SAD groups did not differ on either measure. A MANCOVA also yielded a significant group difference, Pillai's Trace = .11, F(4, 194) = 2.93, p = .022, η2 = .06. Univariate analyses showed the same pattern of results as in the MANOVA for Cognitive Reappraisal with the LSA group scoring higher than the HSA and SAD groups and no difference between the HSA and SAD groups. However, the univariate result for Expressive suppression became non‐significant with the inclusion of the depression covariate.
Study 2: Total self‐compassion predicting social anxiety via emotional regulation controlling for depression
Table 3 presents bivariate Pearson correlations among variables and Cronbach's alpha for all variables. All correlations were significant and in the expected direction (p < .001) except for mindfulness and Expressive Suppression. Total self‐compassion displayed a moderately strong negative association with SIAS and a similar but weaker association with SPS. All individual subscales of self‐compassion displayed stronger connections to SIAS (rs − .28 to −.54) than SPS (rs = −.17 to −.45). The RUSR subscales (self‐judgement, over‐identification, and isolation) showed negative associations with both measures of social anxiety (rs − .42 to −.54), whereas the CSR subscales (self‐kindness, mindfulness, and common humanity) showed significant but weaker negative associations (rs − .17 to −.38). For relationships with emotional regulation, Cognitive reappraisal displayed stronger associations than Expressive suppression on measures of social anxiety, depression, and all self‐compassion measures.
Depression was positively correlated with both measures of social anxiety (p < .001), had a negative correlation with self‐compassion (p < .001), and was positively correlated with Cognitive Reappraisal and Expressive Suppression (p's < .001).
Emotional regulation mediates the effect of self‐compassion on social interaction anxiety independent of the depression covariate
As depicted in Figure 1, total self‐compassion significantly predicted SIAS, Cognitive Reappraisal, and Expressive Suppression. Cognitive Reappraisal and Expressive Suppression also significantly predicted SIAS and the direct effect of self‐compassion on SIAS was significant controlled for Cognitive Reappraisal and Expressive Suppression. The indirect effects of self‐compassion on SIAS via Cognitive Reappraisal and Expressive Suppression were significant (p's < .01). Although significant, the depression covariate did not impact these relationships.
FIGURE 1.
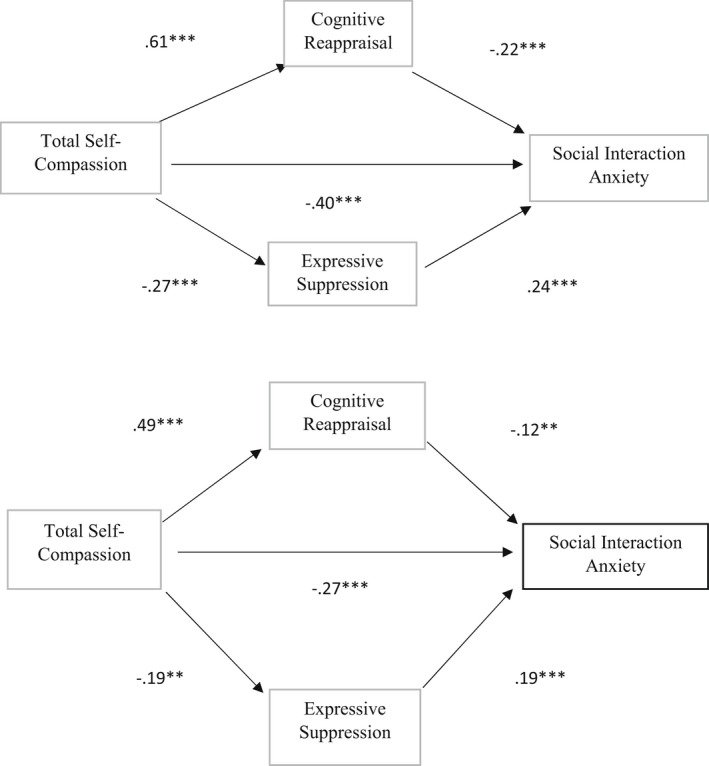
Standardized regression coefficients for the self‐compassion and social interaction anxiety mediation model without controlling for depression (upper panel) versus controlling for depression (lower panel). Self‐compassion significantly predicts SIAS in both analyses. *p < .05, **p < .01, ***p < .001. N = 363
Depression eliminates the mediating effect of emotional regulation on social performance anxiety
As shown in Figure 2, without controlling for depression, all pathways were significant for SPS (all p's < .01). Unlike SIAS, however, the inclusion of the depression covariate removed mediation effects for Cognitive Reappraisal and Expressive Suppression which no longer directly predicted SPS (p > .05). Only self‐compassion remained a direct predictor of SPS (p < .01).
FIGURE 2.
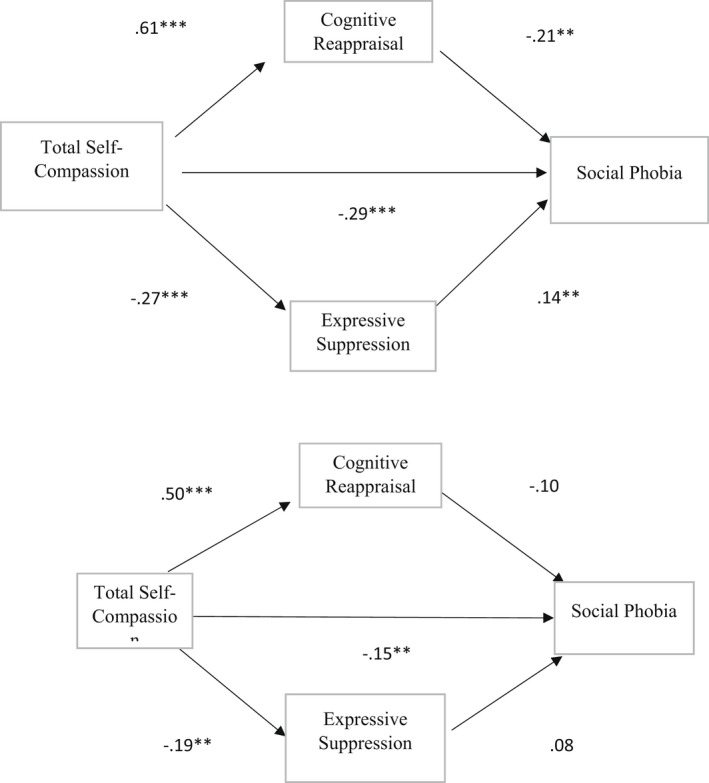
Standardized regression coefficients for the self‐compassion and social performance anxiety mediation model without controlling for depression (upper panel) versus controlling for depression (lower panel). Indirect effects are insignificant with depression entered as a covariate. *p < .05, **p < .01, ***p < .001. N = 363
Individual subscales of self‐compassion, emotional regulation, and social anxiety
Table 4 presents mediation analyses for all self‐compassion subscales on SIAS and SPS. As shown in Table 4, all three subscales related to RUS (self‐judgement, overidentification, and separation) directly predicted both forms of social anxiety with or without controlling for depression (all p's < .05). However, for the subscales of compassionate self‐responding (CSR; self‐kindness, mindfulness, and common humanity), the direct prediction was significant only for two subscales in the models which did not control for depression. Self‐kindness directly predicted SIAS and mindfulness directly predicted SPS (p's < .05). However, both effects became non‐significant in the mediation analyses that controlled for depression. The indirect effect of Cognitive reappraisal with SIAS and SPS was significant for all subscales not controlling for depression. When depression was controlled these effects remained significant for all subscales except overidentification in predicting SPS. Unlike Cognitive Reappraisal, the indirect effect of Expressive Suppression on the RUSR subscales was substantially influenced by depression. In the models that did not control for depression, Expressive suppression was a significant indirect predictor for all subscales except mindfulness for both SIAS and SPS. Controlling for depression, significant indirect effects of Expressive suppression in predicting SIAS were only evident for self‐judgement, self‐kindness, and common humanity. For SPS only self‐kindness and common humanity remained significant.
TABLE 4.
Direct and indirect effects for SCS‐SIAS and SCS‐SPS mediation models for self‐compassion subscales
| Not controlling for depression | Controlling for depression | |||||||
|---|---|---|---|---|---|---|---|---|
| Direct effect (c′): Subscales | Total indirect effect: SCS | Indirect effect: SCS→CR | Indirect effect: SCS→ES | Direct effect (c′): SCS | Total indirect effect: SCS | Indirect effect: SCS→CR | Indirect effect: SCS→ES | |
| SIAS | ||||||||
| Self‐Judgement | −5.91*** | −3.63* | −2.41* | −1.22* | −4.49*** | −1.48* | −.84* | −.65* |
| Overidentification | −6.32*** | −3.13* | −2.45* | −.68* | −4.66*** | −1.01* | −.91* | −.10 |
| Isolation | −6.18*** | −3.00* | −2.07* | −.93* | −4.50*** | −1.02* | −.64* | −.38 |
| Self‐Kindness | −2.31* | −5.82* | −4.11* | −1.71* | −.72 | −2.83* | −1.86* | −.97* |
| Mindfulness | −1.83 | −5.24* | −4.61* | −.63 | .03 | −2.13* | −2.18* | .05 |
| Common Humanity | −1.83 | −4.35* | −3.10* | −1.25* | −.63 | −1.87* | −1.24* | −.63* |
| SPS | ||||||||
| Self‐Judgement | −4.49*** | −2.65* | −1.97* | −.68* | −3.06** | −.78* | −.54* | −.25 |
| Overidentification | −5.18*** | −2.33* | −1.94* | −.40* | −3.51*** | −.59 | −.54 | −.04 |
| Isolation | −4.93*** | −2.18* | −1.66* | −.52* | −3.22*** | −.56* | −.41* | −.16 |
| Self‐Kindness | −.28 | −4.85* | −3.74* | −1.11* | 1.33 | −2.07* | −1.56* | −.51* |
| Mindfulness | −2.43* | −3.78* | −3.41* | −.37 | −.64 | −1.27* | −1.30* | .02 |
| Common Humanity | .22 | −3.61* | −2.79* | −.82* | 1.43 | −1.33* | −1.01* | −.32* |
Note: For direct effects *p < .05, **p < .01, ***p < .001. *Indirect effect significant based on 95% confidence interval of bootstrapped estimates. SCS→CR represents the effect of the self‐compassion subscale on social anxiety via cognitive reappraisal; SCS→ES represents the effect of the self‐compassion subscale on social anxiety via expressive suppression.
Abbreviations: CR, cognitive reappraisal; ES, expressive suppression.
DISCUSSION
The purpose of this study was to build on research by Bates et al. (2021) on the role of self‐compassion and emotional regulation as predictors of social anxiety. As an extension of Bates et al., we compared scores on each of the measures from a group with SAD and matched samples of students with high and low social anxiety. In addition, using the full‐scale SCS we explored relationships among all six subcomponents of self‐compassion within Neff's (2003) model. As a further extension, we measured depressed mood to account for the close association between social anxiety and depression. Our findings suggest that higher self‐compassion alleviates social anxiety and that emotional regulation strategies act as mechanisms of that influence. Our findings were broadly consistent with Bates et al. (2021) but we extend their findings by demonstrating that several of these relationships are influenced by depression and we identify differences in relationships based on the type of social anxiety being assessed. The discussion considers the implications of our findings for group differences, and prediction of the two forms of social anxiety we examined and recommends directions for future work.
Differences between socially anxious and non‐anxious groups
As expected, consistent with past research (Dryman & Heimberg, 2018; Werner et al., 2012), the LSA student group scored higher on the measures of self‐compassion and Cognitive Reappraisal and lower on Expressive Suppression compared to the SAD group and the HSA student group. Yet, contrary to expectation, the HSA group did not differ from the SAD group on most measures. In general, this pattern of differences was evident independent of depressed mood. This suggests that students identified as socially anxious via established self‐report measure cut‐offs show reductions in self‐compassion and levels of ineffective emotional regulation comparable to people with clinical disorders. However, as hypothesized, the SAD group scored higher on depression than the HSA and LSA groups and the HSA group scored higher than the LSA group. Comorbid depression may therefore be a distinguishable feature of clinical groups with social anxiety.
Depression also impacted group differences on the RUSR subscales of self‐compassion and emotion regulation by Expressive Suppression. Controlling for depression, the HSA group scored significantly lower than the SAD group on refraining from self‐judgement and isolation. This is surprising given that the clinical group scored higher on depression. As the clinical group comprised treatment‐seeking individuals with a clinical diagnosis of SAD, this group difference may relate to their commitment to change and possible insight into their need to reduce self‐judgement and engage with others. Alternatively, the difference may reflect a tendency for the students to make more negative self‐appraisals on self‐report scales. Further research with in‐depth interview assessments of the students might help to elucidate the nature of this group difference. In addition, for emotional regulation, while the group difference on cognitive reappraisal remained significant, the group difference on expressive suppression became non‐significant controlling for depression. This suggests that individual differences in the use of expressive suppression may be influenced more by depressed mood than the level of social anxiety.
Mediation analyses for total self‐compassion and social anxiety
Before inclusion of depressed mood as a covariate the results were generally as hypothesized. As expected, consistent with Bates et al. (2021), higher total self‐compassion predicted lower social anxiety directly and indirectly via reduced Expressive Suppression for both measures of social anxiety. Importantly, however, and distinct from Bates et al. (2021), prior to controlling for depression, Cognitive Reappraisal was also a mechanism of change in the relationship between total self‐compassion and both forms of social anxiety. It is possible that these different results emanate from differences in sample composition and our use of the long form of the Self‐compassion scale (SCS). However, while we included a small SAD group, our sample was predominantly comprised of students from the same University as Bates et al. and there were few differences between the self‐report scores of highly socially anxious students and SAD clients. Moreover, the full SCS measure correlates strongly with the short form of the scale (r = .97, Raes et al., 2011) making measurement variance an unlikely explanation. Self‐efficacy is one external factor that may have contributed to the different findings. Dryman and Heimberg (2018) noted that the frequency of usage of cognitive reappraisal does not predict social anxiety in all samples. They suggested that, rather than frequency, the socially anxious person's confidence that they can change their negative emotions through reappraisal may be a more sensitive measure of the influence of cognitive appraisal. Thus, it is possible that our participants had a higher sense of self‐efficacy for cognitive reappraisal than participants in the Bates et al study. This possibility invites further research.
The inclusion of depression as a covariate identified an important and previously unexplored influence on the indirect relationships of self‐compassion and emotional regulation with social anxiety. Interestingly, the influence of depression differed according to the form of social anxiety being assessed. For SIAS while the covariate was significant, the direct and indirect pathways remained significant indicating they predict lower social anxiety levels independent of depression. In contrast, for the SPS, while self‐compassion remained a significant direct predictor of lower social anxiety, the indirect pathways through cognitive reappraisal and expressive suppression became non‐significant with the depression covariate. Earlier work on the factor structure of SIAS and SPS by Carleton et al. (2009) found that the scales were associated with three different factors. The SIAS comprised one factor and focused on internal discomfort experienced in social situations (e.g., “when mixing socially I am uncomfortable”). In contrast, the SPS comprised two factors focused on external scrutiny and social performance. One factor reflected a fear of external evaluation (e.g., “I get nervous when people are staring at me as I walk down the street”) and the other was a fear of attracting attention (e.g., “I worry I might do something to attract the attention of others”). Thus, given our results, it appears that whereas the mediational influence on self‐compassion of cognitive appraisal and expressive suppression may operate independently of depression for more inwardly focused social concerns, this is not true for externally focused concerns related to performance in social situations. This difference may stem from the greater cognitive load placed on the individual in externally focused performance concerns. Makkar and Grisham (2011) argued that an emphasis on external scrutiny and judging the likely consequences of negative evaluation by others requires more cognitive resources than general social interactions. Therefore, as a depressed mood reduces cognitive resources by increasing task‐irrelevant processing (Gotlib & Joormann, 2010), the higher the depression the lower the capacity for selection and implementation of emotion regulation strategies in such performance situations.
Exploratory analysis of the individual subscales of self‐compassion
Our mediation analyses for each subscale of self‐compassion explored the specificity of the findings for each component of self‐compassion. This extends the work of Bates et al. (2021) whose analysis was confined to the grouped compassionate responding scales and the scales reflecting refrain from uncompassionate responding. Once more, while our results were similar to Bates et al., we identified differences when we accounted for the effects of depression and distinct patterns of results for the two types of social anxiety.
Consistent with Bates et al. (2021), all three self‐compassion subscales capturing the capacity to refrain from uncompassionate self‐responding directly predicted lower social anxiety. These subscales remained significant controlling for depressed mood indicating and thus predicting depression independent of the depression. In the main, the compassionate responding scales did not directly predict either form of social anxiety, again consistent with Bates et al. (2021). Although self‐kindness directly predicted SIAS and Mindfulness directly predicted SPS prior to controlling for depression, these relationships became non‐significant when the depressed mood was added as a covariate. This aligns with previous findings that refraining from uncompassionate behaviour is more closely associated with reducing psychological distress and symptoms of psychopathology, in this case, social anxiety, than are the components of compassionate responding (Chio et al., 2021; MacBeth & Gumley, 2012; Neff et al., 2018). That these predictive relationships remain when controlling for depression and apply to both forms of social anxiety attests to the strength of the relationship.
Analysis of the indirect pathways yielded a more complex pattern of results when considering the effects of depression and the form of social anxiety being predicted. There was, however, a consistent pattern of findings for the relationships among the subcomponents and social anxiety with mediation by cognitive reappraisal. All the components of compassionate responding and of refraining from uncompassionate responding showed significant indirect effects via cognitive reappraisal without controlling for depression. Except for overidentification in the prediction of SPS (which bordered on significance), these pathways remained significant controlling for depression. These findings replicate those of Bates et al. and suggest that compassionate responding is important in the prediction of social anxiety by virtue of its relationship with cognitive reappraisal and this effect is independent of depression.
The mediation effect of expressive suppression was more affected by the effect of depressed mood and by the type of social' anxiety being assessed. Consistent with Bates et al. (2021), prior to controlling for depression, the three forms of refraining from uncompassionate responding demonstrated a significant indirect prediction of both forms of social anxiety with mediation by expressive suppression. However, unlike Bates et al., there were significant indirect effects on the compassionate responding components of Self‐kindness and Common Humanity. Thus, the motivation to attend to one's needs in a stressful situation and to accept one's distress as an experience shared with others also reduced the tendency to suppress the expression of feelings and thereby decreasing social anxiety. Interestingly, mindfulness did not have a significant indirect effect via expressive suppression and was uncorrelated with expressive suppression (r = −.09). In Neff's model, the concept of mindfulness is confined to a motivation to take a balanced view of difficult situations (Neff, 2003). That such attempts to keep responses in balance correlated significantly with cognitive reappraisal (r = .54) suggests this approach may be most relevant at the cognitive appraisal stage of the emotion generation process (Gross, 2015) which occurs earlier in the cycle than behavioural strategies such as expressive suppression that are invoked when the emotion is clearly present. The absence of correlation suggests that there is no pattern of relationship so attempts to balance emotional responses are unrelated to how the person acts when experiencing symptoms of social anxiety.
Inclusion of the depression covariate had a marked effect on the mediation effects for expressive suppression. Controlling for depression removed all the indirect effects for the refraining from uncompassionate responding in predicting SPS and only refraining from self‐judgement retained a significant indirect pathway to SIAS via expressive suppression. In contrast, the indirect effects on self‐kindness and common humanity remained significant for both forms of social anxiety. This suggests that along with depression these specific components of self‐compassion may be crucial in reducing the influence of expressive suppression.
Methodological considerations and directions for future research
Strengths of the current study include the use of a large sample, a roughly equal number of male and female participants, the use of the full self‐compassion scale, and the inclusion of a matched clinical group as well as HSA and LSA students in Study 1. Nevertheless, some methodological limitations warrant consideration and suggest directions for research. As the present study was cross‐sectional, while our results were broadly consistent with previous research (Bates et al., 2021), causal relationships among the variables cannot be assumed and the relationships we found require confirmation in studies utilizing longitudinal and experimental designs. In addition, the clinical group included in the mediation models was relatively small (n = 33). Replication with a larger clinical sample could clarify the clinical relevance of the relationships identified in this study. This would also permit examination of whether the mediation relationships identified in this study can be extended to a clinical group of people with SAD. The present study also relied on self‐report measures of general behavioural patterns. Self‐report measures may not reflect actual behaviour in social situations and can be influenced by response bias. Research employing observational, physiological, or behavioural performance measures would help establish the strength of the findings. In addition, given the differences we found between the predictive relationships for the SIAS and SPS, assessments of social anxiety with other measures which more clearly differentiate performance‐related social anxiety from non‐performance anxiety (e.g., Liebowitz Social Anxiety Scale; Heimberg et al., 1999) would help elucidate the influence of self‐compassion and emotion regulation on different types of social anxiety.
A further limitation was our focus on self‐compassion within Neff's conception of the construct. Future research could extend the scope of our work by incorporating the other forms of compassionate behaviour identified by Gilbert including the capacity to receive compassion and to act compassionately towards other people (Gilbert et al., 2017). Kirby et al. (2019) argued that these aspects of compassion exist in a dynamic reciprocal relationship in which compassion can flow from one to another. Thus, whereas self‐compassion involves a flow of compassion from self‐to‐self, compassion can also flow from self‐to‐others, and from others‐to‐the self. Our data suggest that, in conjunction with specific strategies of emotion regulation, self‐compassion is important in emotional regulation to reduce social anxiety. However, in the tripartite system of compassion, social anxiety can also be influenced by emotion regulation coming from receiving support from others or by extending compassion to others. Notably, Hofmann et al. (2016) have developed a measure of interpersonal emotional regulation to capture the capacity to draw on the support of others reflecting the other‐to‐self flow of compassion. Moreover, Gilbert's treatment model for social anxiety recommends the adoption of a more compassionate attitude towards other people (i.e., self‐to‐others flow) to overcome the negatively self‐focused attention that characterizes problematic social anxiety (Clark & Wells, 1995; Gilbert, 2014a, 2014b).
Another promising direction for future work utilizing the tripartite view of compassion relates to the fear of compassion that inhibits compassion towards the self or others and prevents the receipt of compassion from others. A fear of self‐compassion is a concern that directing compassion towards the self reflects weakness or self‐indulgence (Gilbert et al., 2011) and the fear of receiving compassion is linked to the activation of past negative memories (e.g., memories of parental neglect or social trauma, Gilbert, 2014a, 2014b). The fear of being compassionate to others relates to concerns that compassionate behaviour will be negatively received. Recently Merritt and Purdon (2020) found that whereas socially anxious patients did not differ from controls or other clinical groups on a fear of extending compassion towards others they experienced high levels of fear of self‐compassion and of receiving compassion from others. Further, the fear of receiving compassion was associated with higher symptom severity and this relationship remained when depression was controlled. Such fears are clearly likely to disrupt attempts to regulate emotions and warrant attention in future research.
In conclusion, this study affirms the ameliorative role of self‐compassion on social anxiety and the importance of the emotional regulation strategies of cognitive reappraisal and expressive suppression as mechanisms of this influence. Moreover, whereas refraining from uncompassionate self‐responding reduces social anxiety directly, the effect of compassionate self‐responding is determined through emotional regulation. Moreover, depression can have a considerable influence on these relationships. Comorbid depression subsumes the mediational influence of emotional regulation on self‐compassion, especially for social performance anxiety.
AUTHOR CONTRIBUTIONS
Brad Elphinstone: Data curation; investigation; writing – review and editing. Richard Whitehead: Data curation; investigation; writing – review and editing.
CONFLICT OF INTEREST
All authors report no conflict of interests.
ACKNOWLEDGEMENT
Open access publishing facilitated by Swinburne University of Technology, as part of the Wiley ‐ Swinburne University of Technology agreement via the Council of Australian University Librarians.
McBride, N. L. , Bates, G. W. , Elphinstone, B. , & Whitehead, R. (2022). Self‐compassion and social anxiety: The mediating effect of emotion regulation strategies and the influence of depressed mood. Psychology and Psychotherapy: Theory, Research and Practice, 95, 1036–1055. 10.1111/papt.12417
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- Adams, G. C. , Balbuena, L. , Meng, X. , & Asmundson, G. J. G. (2016). When social anxiety and depression go together: A population study of comorbidity and associated consequences. Journal of Affective Disorders, 206, 48–54. 10.1016/j.jad.2016.07.031 [DOI] [PubMed] [Google Scholar]
- Adie, T. , Steindl, S. R. , Kirby, J. N. , Kane, R. T. , & Mazzuchelli, T. G. (2021). The relationshipbetween self‐compassion and depressive symptoms: Avoidance and activation as mediators. Mindfulness, 12, 1748–1756. 10.1007/s1267-021-01637-1 [DOI] [Google Scholar]
- Akin, A. , & Çetın, B. (2007). The depression anxiety and stress scale (DASS): The study of validity and reliability. Educational Sciences: Theory & Practice, 7(1), 260–268. [Google Scholar]
- American Psychiatric Association . (2022). Diagnostic and statistical manual of mental disorders fifth edition, text revision (DSM‐5‐TR). Author. [Google Scholar]
- Barlow, M. R. , Turow, R. E. G. , & Gerhart, J. (2017). Trauma appraisals, emotion regulation difficulties, and self‐compassion predict posttraumatic stress symptoms following childhood abuse. Child Abuse & Neglect, 65, 37–47. 10.1016/j.chiabu.2017.01.006 [DOI] [PubMed] [Google Scholar]
- Bates, G. W. , Elphinstone, B. , & Whitehead, R. (2021). Self‐compassion and emotional regulation in social anxiety. Psychology and Psychotherapy: Theory, Research and Practice, 94, 426–442. 10.1111/papt.12318 [DOI] [PubMed] [Google Scholar]
- Beesdo, K. , Bittner, A. , Pine, D. S. , Stein, M. B. , Höfler, M. , Lieb, R. , & Wittchen, H.‐U. (2007). Incidence of social anxiety disorder and the consistent risk for secondary depression in the first three decades of life. Archives of General Psychiatry, 64(8), 903–912. 10.1001/archpsyc.64.8.903 [DOI] [PubMed] [Google Scholar]
- Belzer, K. , & Schneier, F. R. (2004). Comorbidity of anxiety and depressive disorders: Issues in conceptualization, assessment, and treatment. Journal of Psychiatric Practice, 10(5), 296–306. 10.1097/00131746-200409000-00003 [DOI] [PubMed] [Google Scholar]
- Berking, M. , & Whitley, B. (2014). Affect regulation training (ART). Springer. [Google Scholar]
- Blackie, R. A. , & Kocovski, N. L. (2018). Forgive and let go; effect of self‐compassion on post‐event processing in social anxiety. Mindfulness, 9, 654–663. 10.1007/s12671-017-0808-9 [DOI] [Google Scholar]
- Boersma, K. , Hakanson, A. , Salmonsson, E. , & Johansson, I. (2015). Compassion focused therapy to counteract shame, self‐criticism and isolation. A replicated single case experimental study for individuals with social anxiety. Journal of Contemporary Psychotherapy, 45, 89–98. 10.1007/s10879-014-9286-8 [DOI] [Google Scholar]
- Carleton, R. N. , Collimore, K. C. , Asmundson, G. J. , McCabe, R. E. , Rowa, K. , & Antony, M. M. (2009). Refining and validating the social interaction anxiety scale and the social phobia scale. Depression and Anxiety, 26(2), 71–81. 10.1002/da.20480 [DOI] [PubMed] [Google Scholar]
- Chio, F. H. N. , Mak, W. W. S. , & Yu, B. C. L. (2021). Meta‐analytic review on the differential effects of self‐compassion components on well‐being and psychological distress: The moderating role of dialecticism on self‐compassion. Clinical Psychology Review, 85, 101986. 10.1016/j.cpr.2021.101986 [DOI] [PubMed] [Google Scholar]
- Clark, D. M. , & Wells, A. (1995). A cognitive model of social phobia. Social Phobia: Diagnosis, Assessment, and Treatment, 41(68), 22–23. [Google Scholar]
- Crome, E. , Grove, R. , Baillie, A. J. , Sunderland, M. , Teesson, M. , & Slade, T. (2015). DSM‐IV and DSM‐5 social anxiety disorder in the Australian community. Australian and New Zealand Journal of Psychiatry, 49(3), 227–235. 10.1177/0004867414546699 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Castella, K. , Goldin, P. , Jazaieri, H. , Ziv, M. , Dweck, C. S. , & Gross, J. J. (2013). Beliefs about emotion: Links to emotion regulation, well‐being, and psychological distress. Basic and Applied Social Psychology, 35(6), 497–505. 10.1080/01973533.2013.840632 [DOI] [Google Scholar]
- Diedrich, A. , Burger, J. , Kirchner, M. , & Berking, M. (2017). Adaptive emotion regulation mediates the relationship between self‐compassion and depression in individuals with unipolar depression. Psychology and Psychotherapy: Theory, Research and Practice, 90(3), 247–263. 10.1111/papt.12107 [DOI] [PubMed] [Google Scholar]
- Dryman, M. T. , & Heimberg, R. G. (2018). Emotion regulation in social anxiety and depression: A systematic review of expressive suppression and cognitive reappraisal. Clinical Psychology Review, 65, 17–42. 10.1016/j.cpr.2018.07.004 [DOI] [PubMed] [Google Scholar]
- Faul, F. , Erdfelder, E. , Lang, A. G. , & Buchner, A. (2007). G*power 3: A flexible statistical power analysis program for the social, behavioural and biomedical sciences. Behaviour Research Methods, 39, 175–191. 10.3758/bf03193146 [DOI] [PubMed] [Google Scholar]
- Fehm, L. , Beesdo, K. , Jacobi, F. , & Fiedler, A. (2008). Social anxiety disorder above and below the diagnostic threshold: Prevalence, comorbidity and impairment in the general population. Social Psychiatry and Psychiatric Epidemiology, 43(4), 257–265. 10.1007/s00127-007-0299-4 [DOI] [PubMed] [Google Scholar]
- Finlay‐Jones, A. L. (2017). The relevance of self‐compassion as an intervention target in mood and anxiety disorders: A narrative review based on an emotion regulation framework. Clinical Psychologist, 21(2), 90–103. 10.1371/journal.pone.0133481 [DOI] [Google Scholar]
- Finlay‐Jones, A. L. , Rees, C. S. , & Kane, R. T. (2015). Self‐compassion, emotion regulation and stress among Australian psychologists: Testing an emotion regulation model of self‐compassion using structural equation modeling. PLoS One, 10(7), e0133481. 10.1371/journal.pone.0133481 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gilbert, P. (2014a). The origins and nature of compassion focused therapy. British Journal of Clinical Psychology, 53, 6–41. 10.1111/bjc.12043 [DOI] [PubMed] [Google Scholar]
- Gilbert, P. (2014b). Evolutionary models. Practical and conceptual utility for the treatment and study of social anxiety disorder. In Weeks J. W. (Ed.), The Wiley Blackwell handbook of social anxiety disorder (pp. 24–52). J.Wiley. [Google Scholar]
- Gilbert, P. (2017). Compassion: Definitions and controversies. In Gilbert P. (Ed.), Compassion:Concepts, research and applications (pp. 3–15). Routledge. 10.4324/9781315564296-1 [DOI] [Google Scholar]
- Gilbert, P. , Catarino, F. , Duarte, C. , Matos, M. , Kolts, R. , Stubbs, J. , Ceresatto, L. , Duarte, J. , Pinto‐Gouveia, J. , & Basran, J. (2017). The development of compassionate engagement and action scales for self and others. Journal of Compassionate Health Care, 4(1), 1–24. 10.1186/s40639-017-0033-3 [DOI] [Google Scholar]
- Gilbert, P. , McEwan, K. , Matos, M. , & Rivis, A. (2011). Fears of compassion: Development of three self‐report measures. Psychology and Psychotherapy: Theory, Research and Practice, 84(3), 239–255. 10.1348/147608310X526511 [DOI] [PubMed] [Google Scholar]
- Gilboa‐Schechtman, E. , Keshet, H. , Peschard, V. , & Azoulay, R. (2020). Self and identity in social anxiety disorder. Journal of Personality, 88(1), 106–121. 10.1111/jopy.12455 [DOI] [PubMed] [Google Scholar]
- Gotlib, I. H. , & Joormann, J. (2010). Cognition and depression: Current status and future directions. Annual Review of Clinical Psychology, 6, 285–312. 10.1146/annurev.clinpsy.121208.131305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gross, J. J. (2015). Emotion regulation: Current status and future prospects. Psychological Inquiry, 26(1), 1–26. 10.1080/1047840X.2014.940781 [DOI] [Google Scholar]
- Gross, J. J. , & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships and well‐being. Journal of Personality and Social Psychology, 85(2), 348–362. 10.1037/0022-3514.85.2.348 [DOI] [PubMed] [Google Scholar]
- Hayes, A. F. (2017). Introduction to mediation, moderation, and conditional process analysis: A regression‐based approach. Guilford Publications. [Google Scholar]
- Hayes, J. A. , Lockard, A. J. , Janis, R. A. , & Locke, B. D. (2016). Construct validity of the self‐compassion scale‐short form among psychotherapy clients. Counselling Psychology Quarterly, 29(4), 405–422. 10.1080/09515070.2016.1138397 [DOI] [Google Scholar]
- Heimberg, R. G. , & Becker, R. E. (2002). Cognitive‐behavioural group therapy for social phobia. Guilford. [Google Scholar]
- Heimberg, R. G. , Brozovich, F. A. , & Rapee, R. M. (2010). A cognitive behavioral model of social anxiety disorder: Update and extension. In Hofmann S. G. & DiBartolo P. M. (Eds.), Social anxiety: Clinical, developmental, and social perspectives (pp. 395–422). Elsevier Academic Press. 10.1016/B978-0-12-375096-9.00015-8 [DOI] [Google Scholar]
- Heimberg, R. G. , Horner, K. , Juster, H. , Safren, S. , Brown, E. , Schneier, F. , & Liebowitz, M. (1999). Psychometric properties of the Liebowitz social anxiety scale. Psychological Medicine, 29(1), 199–212. 10.1017/s0033291798007879 [DOI] [PubMed] [Google Scholar]
- Hofmann, S. G. , Carpenter, J. K. , & Curtiss, J. (2016). Interpersonal emotion regulation questionnaire (IERQ): Scale development and psychometric characteristics. Cognitive Therapy and Research, 40, 341–356. 10.1007/s10608-016-97562 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmann, S. G. , Sawyer, A. T. , Fang, A. , & Asnanni, A. (2012). Emotion dysregulation model of mood and anxiety disorders. Depression and Anxiety, 29, 409–416. 10.1002/da.21888 [DOI] [PubMed] [Google Scholar]
- Inwood, E. , & Ferrari, M. (2018). Mechanisms of change in the relationship between self‐compassion, emotion regulation, and mental health: A systematic review. Applied Psychology. Health and Well‐Being, 10(2), 215–235. 10.1111/aphw.12127 [DOI] [PubMed] [Google Scholar]
- Jazaieri, H. , Morrison, A. S. , Goldin, P. R. , & Gross, J. J. (2015). The role of emotion and emotion regulation in social anxiety disorder. Current Psychiatry Reports, 17(1), 1–9. 10.1007/s11920-014-0531-3 [DOI] [PubMed] [Google Scholar]
- Kirby, J. N. , Day, J. , & Sagar, V. (2019). The ‘flow’ of compassion: A meta‐analysis of the fears of compassion scales and psychological functioning. Clinical Psychology Review, 70, 26–39. 10.1016/j.cpr.2019.03.001 [DOI] [PubMed] [Google Scholar]
- Kline, R. B. (2005). Principles and practice of structural equation modelling (2nd ed.). Guilford Press. [Google Scholar]
- Kneeland, E. T. , Noelen‐Hoeksema, S. , & Dovidio, J. F. (2016). Emotion malleability beliefs influence the spontaneous regulation of social anxiety. Cognitive Therapy and Research, 40, 496–509. 10.1007/s10608-016-9765-1 [DOI] [Google Scholar]
- Koyuncu, A. , Ertekin, E. , Deveci, E. , Ertekin, B. A. , Yüksel, Ç. , Çelebi, F. , Binbay, Z. , Demir, E. Y. , & Tükel, R. (2015). Age of onset in social anxiety disorder: Relation to clinical variables and major depression comorbidity. Annals of Clinical Psychiatry, 27(2), 84–89. [PubMed] [Google Scholar]
- Lovibond, P. F. , & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behaviour Research and Therapy, 33(3), 335–343. 10.1016/0005-7967(94)00075-U [DOI] [PubMed] [Google Scholar]
- MacBeth, A. , & Gumley, A. (2012). Exploring compassion: A meta‐analysis of the association between self‐compassion and psychopathology. Clinical Psychology Review, 32(6), 545–552. 10.1016/j.cpr.2012.06.003 [DOI] [PubMed] [Google Scholar]
- Makadi, E. , & Koszycki, D. (2020). Exploring connections between self‐compassion, mindfulness and social anxiety. Mindfulness, 11, 480–492. 10.1007/s1267-019-01270-z [DOI] [Google Scholar]
- Makkar, S. R. , & Grisham, J. R. (2011). The predictors and contents of post‐event processing in social anxiety. Cognitive Therapy and Research, 35(2), 118–133. 10.1007/s10608-011-9357-z [DOI] [Google Scholar]
- Mattick, R. P. , & Clarke, J. C. (1998). Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behaviour Research and Therapy, 36(4), 455–470. 10.1016/S0005-7967(97)10031-6 [DOI] [PubMed] [Google Scholar]
- McEvoy, P. M. , Grove, R. , & Slade, T. (2011). Epidemiology of anxiety disorders in the Australian general population. Findings of the 2007 Australian national survey of mental health and well‐being. Australian and New Zealand Journal of Psychiatry, 4, 957–967. 10.3109/00048674.2011.624083 [DOI] [PubMed] [Google Scholar]
- Merritt, O. A. , & Purdon, C. L. (2020). Scared of compassion: Fear of compassion in anxiety, mood, and non‐clinical groups. British Journal of Clinical Psychology, 59, 354–368. 10.1111/bjc.12250 [DOI] [PubMed] [Google Scholar]
- Modini, M. , Abbott, M. J. , & Hunt, C. (2015). A systematic review of the psychometric properties of trait social anxiety self‐report measures. Journal of Psychopathology and Behavioral Assessment, 37(4), 645–662. 10.1007/s10862-015-9483-0 [DOI] [Google Scholar]
- Muris, P. , & Petrocchi, N. (2017). Protection or vulnerability? A meta‐analysis of the realtions between positive and negative componentsof self‐compassion and psychopathology. Clinical Psychology & Psychotherapy, 24, 373–383. 10.1002/cpp.2005 [DOI] [PubMed] [Google Scholar]
- Neely, M. E. , Schallert, D. L. , Mohammed, S. S. , Roberts, R. M. , & Chen, Y.‐J. (2009). Self‐kindness when facing stress: The role of self‐compassion, goal regulation, and support in college students' well‐being. Motivation and Emotion, 33(1), 88–97. 10.1007/s11031-008-9119-8 [DOI] [Google Scholar]
- Neff, K. D. (2003). The development and validation of a scale to measure self‐compassion. Self and Identity, 2(3), 223–250. 10.1080/15298860309027 [DOI] [Google Scholar]
- Neff, K. D. (2016). The self‐compassion scale is a valid and theoretically coherent measure of self‐compassion. Mindfulness, 7(1), 264–274. 10.1007/s12671-015-0479-3 [DOI] [Google Scholar]
- Neff, K. D. , & Dahm, K. A. (2015). Self‐compassion: What it is, what it does, and how it relates to mindfulness. In Handbook of mindfulness and self‐regulation (pp. 121–137). Springer. [Google Scholar]
- Neff, K. D. , Long, P. , Knox, M. C. , Davidson, O. , Kuchar, A. , Costigan, A. , Williamson, Z. , Rohleder, N. , Tóth‐Király, I. , & Breines, J. G. (2018). The forest and the trees: Examining the association of self‐compassion and its positive and negative components with psychological functioning. Self and Identity, 17(6), 627–645. 10.1080/15298868.2018.1436587 [DOI] [Google Scholar]
- Neff, K. D. , Toth‐kiraly, I. , Yarnell, L. M. , Arimitsu, K. , Castilho, P. , Ghorbani, N. , Guo, H. X. , Hirsch, J. K. , Hupfield, J. , Hutz, C. S. , Kotsou, I. , Lee, W. K. , Montero‐Marin, J. , Sirios, F. , de Sousa, L. K. , Svendsen, J. L. , Wilkinson, R. B. , & Mantzios, M. (2019). Examining the factor structure of the self‐compassion scale in 20 diverse samples: Support for the use of a total score and six subscale scores. Psychological Assessment, 31, 27–35. 10.1037/pas0000629 [DOI] [PubMed] [Google Scholar]
- Norton, P. J. , Temple, S. R. , & Pettit, J. W. (2008). Suicidal ideation and anxiety disorders: Elevated risk or artifact of comorbid depression? Journal of Behavior Therapy and Experimental Psychiatry, 39(4), 515–525. 10.1016/j.jbtep.2007.10.010 [DOI] [PubMed] [Google Scholar]
- Raes, F. , Pommier, E. , Neff, K. D. , & Van Gucht, D. (2011). Construction and factorial validation of a short form of the self‐compassion scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. 10.1002/cpp.702 [DOI] [PubMed] [Google Scholar]
- Reilly, A. R. , Carleton, R. N. , & Weeks, J. W. (2012). Psychometric evaluation of the social interaction phobia scale. Anxiety, Stress, and Coping, 25(5), 529–542. 10.1080/10615806.2011.598150 [DOI] [PubMed] [Google Scholar]
- Sheehan, D. V. , Lecrubier, Y. , Sheehan, K. H. , Amorim, P. , Janavs, J. , Weiller, E. , & Dunbar, G. C. (1998). The mini‐international neuropsychiatric interview (M.I.N.I): The development and validation of a structured diagnostic psychiatric interview for DSM‐IV and ICD‐10. The Journal of Clinical Psychiatry, 59(Suppl 20), 22–33. [PubMed] [Google Scholar]
- Spence, S. H. , & Rapee, R. M. (2016). The etiology of social anxiety disorder. An evidence‐based model. Behaviour Research and Therapy, 86, 50–67. 10.1016/j.brat.2016.06.007 [DOI] [PubMed] [Google Scholar]
- Stevenson, J. , Mattiske, J. K. , & Nixon, R. D. (2019). The effect of a brief online self‐compassion versus cognitive restructuring intervention on trait social anxiety. Behaviour Research and Therapy, 123, 103492. 10.1016/j.brat.2019.103492 [DOI] [PubMed] [Google Scholar]
- Werner, K. H. , Jazaieri, H. , Goldin, P. R. , Ziv, M. , Heimberg, R. G. , & Gross, J. J. (2012). Self‐compassion and social anxiety disorder. Anxiety, Stress, and Coping, 25(5), 543–558. 10.1080/10615806.2011.608842 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zahniser, E. , & Conley, C. S. (2018). Interactions of emotion regulation and perceived stress in predicting emerging adults' subsequent internalizing symptoms. Motivation and Emotion, 42(5), 763–773. 10.1007/s11031-018-9696-0 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.