

Abstract
Although 10% of pregnancies following treatment of Asherman's syndrome are estimated to have abnormal placental adhesion, there is a paucity of reports describing imaging features in such cases. We describe ultrasound and MRI features in one of such cases, showing a peculiar pattern of shallow but diffuse abnormally adherent placenta.
Keywords: cesarean hysterectomy, hysteroscopic adhesiolysis, intrauterine adhesion, magnetic resonance imaging, placenta accreta
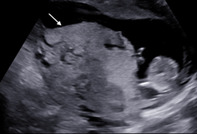
A 41‐year‐old woman gravida 2 para 1 had a previous diagnosis of Asherman's syndrome, developed after an intrauterine curettage for retained placental tissue. Between pregnancies, 6 hysteroscopic adhesiolysis procedures were performed, followed by estrogen treatment. At 12 weeks of gestation, the placenta appeared bilobed; the posterior lobe was dishomogeneous, with abnormal lacunae, and intensely vascularized on ultrasound examination (Figure 1A,B). At 25 weeks, ultrasound showed a left lateral, bilobed placenta with multiple abnormal placental lacunae in the posterior lobe; the hypoechoic retroplacental zone appeared normal in the anterior lobe but could not be assessed in the posterior lobe due to fetal interposition. At 28 weeks an MRI scan showed placental heterogeneity, T2‐dark bands, multiple lacunae, irregularity of retroplacental clear zone with some interruptions, mostly located in the posterior wall of the uterus (Figure 1C); the vesicouterine space was hypervascular without bladder tenting. After an otherwise unremarkable pregnancy, a planned cesarean delivery was performed at 38+3 weeks: a healthy male newborn weighing 3350 g was delivered. The anterior placental lobe detached easily, but the posterior lobe was indissociable from the uterus. A hysterectomy was performed. Total blood loss was 1800 ml. At histological examination the villi of the posterior lobe left in situ adhered directly to the myometrium in several inclusions (Figure 1D); the diagnosis of diffuse abnormally adherent placenta was confirmed.
FIGURE 1.
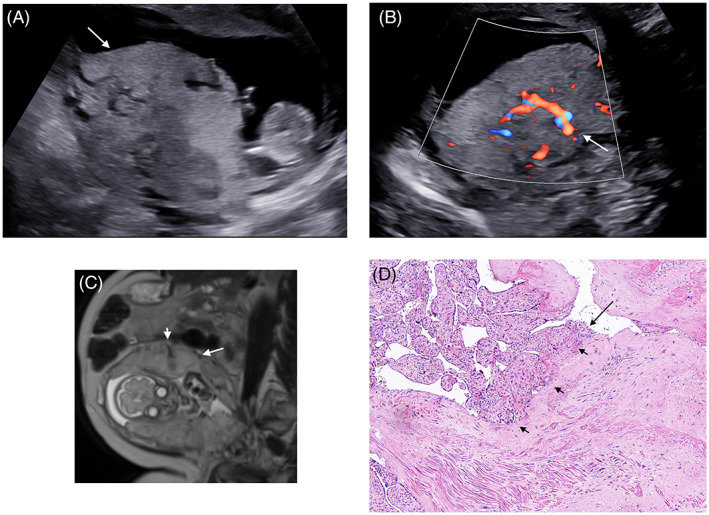
Gray‐scale ultrasound at 12 weeks showing the posterior lobe of the placenta (arrow) with loss of the hypoechoic retroplacental (clear) zone, numerous large or irregular lacunae (A); color Doppler ultrasound shows a feeding vessel with flow velocity >20 cm/s (arrow) (B); MRI T2‐weighed image at 28 weeks showing the bilobed placenta with heterogeneous posterior lobe (arrow), multiple placental lacunae, irregularity of retroplacental clear zone and a feeding vessel (small arrow) (C); histological image (hematoxylin and eosin) showing a section of the placenta with trophoblasts (arrow) directly attached to the myometrium (small arrows) without the presence of the Nitabuch layer (D)
Asherman's syndrome is defined as intrauterine adhesions accompanied by symptoms such as infertility or amenorrhea, the diagnosis and the therapy of this disease is hysteroscopic evaluation and adhesiolysis, respectively. 1 It develops mostly in women who underwent intrauterine curettage after delivery. 2 Following adhesiolysis, approximately 50% of women achieve a pregnancy; of those who reach viability, 10% are estimated to have abnormal placental adhesion. 3 However, there is a paucity of reports describing imaging features in such cases.
The typical ultrasound signs of abnormally adherent and invasive placenta are the loss of the hypoechoic retroplacental zone, numerous large or irregular lacunae connected to a feeding vessel, hyper‐vascularization patterns within the placenta and between the placental basal plate or subplacental zone and underlying structures (myometrium, bladder wall) 4 ; MRI features are placental bulging, bladder wall interruptions, T2‐dark bands, placental heterogeneity, loss of T2 hypointense interface. 4
The peculiarity of our case is the extension of the direct adhesion of the villi to the myometrium, with an extended infiltration of the Nitabuch layer without significative myometrial invasion. This condition was likely caused by the previous Asherman's syndrome and the multiple adhesiolysis, which induced a widespread alteration of the endometrial‐myometral junction.
FUNDING INFORMATION
This research did not receive any specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors.
CONFLICT OF INTEREST
The authors declare no potential conflict of interest.
ETHICS STATEMENT
No Ethics Committee approval was necessary for this study.
PATIENT CONSENT STATEMENT
The patient gave her written informed consent.
ACKNOWLEDGMENT
Open Access Funding provided by Universita degli Studi di Brescia within the CRUI‐CARE Agreement.
Marasciulo F, Gambarini S, Drera E, Prefumo F. Ultrasound and MRI appearance of abnormally adherent placenta in a woman with Asherman's syndrome. J Clin Ultrasound. 2022;50(9):1320‐1321. doi: 10.1002/jcu.23247
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Surgery AEG. AAGL practice report: practice guidelines on intrauterine adhesions developed in collaboration with the European Society of Gynaecological Endoscopy (ESGE). J Minim Invasive Gynecol. 2017;24:695‐705. [DOI] [PubMed] [Google Scholar]
- 2. Sonan Y, Aoki S, Enomoto K, Seki K, Miyagi E. Placenta accreta following hysteroscopic lysis of adhesions caused by Asherman's syndrome: a case report and literature review. Case Rep Obstet Gynecol. 2018;2018:6968382‐6968384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Guo EJ, Chung JPW, Poon LCY, Li TC. Reproductive outcomes after surgical treatment of Asherman syndrome: a systematic review. Best Pract Res Clin Obstet Gynaecol. 2019;59:98‐114. [DOI] [PubMed] [Google Scholar]
- 4. Jauniaux E, Bhide A, Kennedy A, Woodward P, Hubinont C, Collins S. FIGO placenta accreta diagnosis and management expert consensus panel. FIGO consensus guidelines on placenta accreta spectrum disorders: prenatal diagnosis and screening. Int J Gynaecol Obstet. 2018;140:274‐280. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.