

Abstract
Background
Previous studies have reported a potential negative correlation between physical activity (PA) and mobile phone addiction (MPA) among adolescents and young adults. To date, the strength of this correlation has not been well characterized.
Objective
This review and meta-analysis aimed to synthesize available empirical studies to examine the correlations between PA and MPA among adolescents and young adults. We also explored several potential moderators, including time of data collection, country or region, and type of population, associated with the relationship between PA and MPA.
Methods
Four electronic databases (PubMed, Scopus, PsycINFO, and Web of Science) were searched from database inception to March 2022 to identify relevant studies. The pooled Pearson correlation coefficients and their corresponding 95% CIs for the relationship between PA and MPA were calculated using the inverse variance method. The methodological quality of the included cross-sectional studies was determined based on the Joanna Briggs Institute appraisal checklist. The study conformed to the PRISMA (Preferred Reporting Items for Systematic Review and Meta-analyses) guidelines.
Results
In total, 892 relevant articles were identified, of which 22 were selected based on the inclusion and exclusion criteria. The final meta-analysis included 17 of the 22 studies. Results of random effects modeling revealed a moderate correlation between PA and MPA among adolescents and young adults (summary r=–0.243, P<.001). Sensitivity and publication bias analyses further demonstrated the robustness of our results. All the included studies were scored as high quality with a low risk of bias. Subgroup analysis further indicated that none of the hypothesized moderators (time of data collection, country or region, and type of population) significantly affected the relationship between PA and MPA, as confirmed by the mixed effects analysis. In addition, in the data collection subgroups, medium effect sizes were obtained for data collected before COVID-19 (r=–0.333, P<.001) and data collected during COVID-19 (r=–0.207, P<.001). In subgroup analyses for country or region, the correlation coefficient for China and other developing regions showed a similarly moderate effect size (r=–0.201, P<.001 and r= –0.217, P<.001, respectively). However, the effect sizes for developed regions were not significant (r=–0.446, P=.39). In a subgroup analysis based on the type of population, we found that the effect size for young adults was moderate (r=–0.250, P<.001). However, that of adolescents was not significant (r=–0.129, P=.24).
Conclusions
Our results demonstrate a moderately negative relationship between PA and MPA among young adults. The strength of this relationship was not influenced by the time of data collection, country or region, or type of population.
Keywords: mobile phone addiction, physical activity, adolescents, young adults, systematic review, phone addiction, association, correlation, phone use
Introduction
Mobile phone addiction (MPA) is defined as an addictive behavior in which individuals show uncontrollable use of mobile phones that severely impairs their physical, psychological, and social functions [1,2]. Generally, MPA is considered a negative behavior that is socially inappropriate, or even hazardous, in circumstances such as driving, walking, and unauthorized live streaming [3]. It is also categorized as a behavioral addiction (ie, a nonsubstance addiction) that can potentially cause physical, emotional, and financial harm [4,5].
Previous epidemiological surveys of MPA in different countries and regions in the past 5 years have revealed a high rate of MPA among adolescents and young adults. Recent surveys have also found that the rate of MPA among Brazilian adolescents aged 15 to 18 years was approximately 70.3% [6]. The rate of MPA among college students in Hainan province in China aged 18 to 26 years was 40.5% [7], the rate among Egyptian college students with average age of 18 to 21 years was 64.2% [8], and the rate among college students in a regional city in India with a mean age of 20.1 (SD 1.3) years was 39% to 44% [9].
Numerous investigations have demonstrated that MPA negatively affects mental health by causing anxiety [10] and depression [11,12], affecting sleep quality [13-15] and cognitive function [16], and causing muscle pain [17,18], thereby affecting work productivity and the quality of life of individuals. Thus, MPA is now considered an important worldwide public health topic [19]. MPA has been exacerbated by the spread of SARS-CoV-2 in the recent past and restrictions imposed on social gatherings. This has caused negative psychological effects (eg, anxiety, depression, frustration, fear, and stress) in many individuals [20,21]. As a consequence, the overuse of smartphones, social media, and video gaming has increased as people have found mobile phones to be a coping mechanism to alleviate negative emotions [22,23]. It has been shown that adolescents and young adults are more likely to use mobile phones excessively [24] due to their mental immaturity and lower ability to self-regulate compared to middle-aged and older adults [25,26].
A variety of factors that influence MPA have been explored to develop interventions for preventing MPA in young populations, including physical activity (PA). Data show that PA has broad health benefits, including prolonged life expectancy and better physical and psychological well-being [27]. The World Health Organization recommends that adolescents participate in at least 60 minutes of moderate to vigorous PA daily and 150 to 300 minutes of moderate to vigorous PA per week [28]. A previous meta-analysis showed that PA, including tai chi, basketball, badminton, dance, running, and bicycling, had positive effects on individuals with smartphone addiction [29].
Some cross-sectional studies have predicted that higher levels of PA may reduce rates of MPA among adolescents and young adults, suggesting that there might be a negative correlation between PA and MPA [30-32]. A study in China found a significant negative correlation between PA and MPA in adolescents (ie, people aged 10 to 19 years), which indicates that active participation in PA is a potential strategy to reduce MPA levels [33]. Similar findings were obtained in a study of young adults [30,34]. However, a weak relationship has been reported between PA and MPA among young adults aged 18 to 24 years in other research [35]. Physical inactivity (ie, sedentariness) has been demonstrated to increase the risk of MPA due to the prolonged use of mobile phones. There is evidence that sedentary behaviors and low PA levels are strong predictors of time spent using smartphones [36-38] in adolescents and adults.
To the best of our knowledge, no systematic review and meta-analysis has been conducted to examine the correlation between PA and MPA. Thus, an up-to-date literature review of previous findings on the relationship between PA and MPA is needed. This review identified three knowledge gaps. First, previous findings regarding the strength of the correlation coefficient between PA and MPA in adolescents and young adults are inconsistent. Only one, small-scale systematic review [39] reported a negative correlation between PA and MPA in adolescents. This finding cannot be explained without a quantitative analysis [39]. Second, during the COVID-19 pandemic, isolation policies reduced outdoor PA and increased psychological stress among young adults, which may have increased MPA. However, whether the correlation between PA and MPA was influenced by the pandemic is unclear. Third, as mentioned above, the prevalence of MPA differs across countries and regions. Nevertheless, the question of whether the correlation between PA and MPA is influenced by country or region has remained underexplored.
Therefore, this systematic review and meta-analysis is timely. We sought to examine the overall correlation between PA and MPA and address an important research topic. Furthermore, factors such as the time of data collection (ie, before or during COVID-19), country or region, and type of population (adolescents and young adults) are potential variables influencing the correlation between PA and MPA that we explored and examined with a subgroup analysis.
Methods
Protocol Registration
This systematic review and meta-analysis was conducted in line with the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) guidelines [40].
Search Strategy
We searched 4 electronic databases (PubMed, Scopus, PsycINFO, and Web of Science) from database inception until March 26, 2022, to identify relevant studies. A manual search was conducted of the retrieved publications to identify potentially missing studies. The search strategy consisted of 2 strings of keywords, including PA- and MPA-related terms. These included the following: (“cell phone” OR “cell phones” OR “cellular phone” OR “cellular phones” OR “cellular telephone” OR “cellular telephones” OR “mobile devices” OR “mobile phone” OR “smart phone” OR “smartphone”) AND (“addiction” OR “dependence” OR “dependency” OR “abuse” OR “addicted to” OR “overuse” OR “problem use” OR “compensatory use”) OR (“problematic smartphone use” OR “problematic smart phone use” OR “problematic mobile phone use” OR “problematic cell phone use” OR “problematic cellular phone use” OR “Nomophobia” OR “Phubbing” OR “fear of missing out” OR “FoMO” OR “smartphone separation anxiety” OR “smartphone use disorder” OR “compulsive mobile phone use”) AND (“physical activity” OR “walk*” OR “exercise*” OR “physical activity*” OR “strength training” OR “resistance training” OR “resistance exercise*” OR “conditioning muscle” OR “training” OR “leisure training” OR “leisure activities” OR “physical fitness” OR “motor activity”). The detailed search strategy is presented in Multimedia Appendix 1. We manually performed a complementary Google search using the abovementioned keyword combinations to broaden the results on September 20, 2022. Secondary searches were performed by manually screening reference lists of included studies and tracking cited articles to ensure no relevant study was omitted.
The identified and retrieved studies were imported into EndNote X7 software (Thompson Reuters). Duplicates were excluded using the deduplication function in Endnote. This screening and processing was conducted by 2 reviewers, who independently read the titles and abstracts and assessed the studies against predetermined inclusion criteria. The full text of the included studies was also independently examined by the 2 reviewers. Inclusion checklists were completed for each study, along with details on the decision to exclude. The reference list of each included study and the articles cited were thoroughly reviewed to ensure that no relevant studies were missed. At all stages, any discrepancies in the results obtained were resolved through consensus or by involving a third reviewer.
Inclusion Criteria and Study Selection
Population
A study was deemed eligible if it included healthy adolescents or young adults aged between 11 and 24 years [41].
Exposure and Outcome
Data on PA were collected using measurement tools that included self-reported scales, questionnaires, and accelerometers. Data on different aspects of PA, such as steps taken; time spent each day engaging in light, moderate, and vigorous PA; and PA in different scenarios (ie, for leisure, with family, during active travel, or for work) were recorded. Measurements of MPA levels were collected using internationally used scales or questionnaires (eg, the MPA tendency scale, the mobile phone addiction tendency scale, or the smartphone addiction scale). The contents of the MPA measurement questionnaires or other questionnaires were required to include withdrawal, loss of control and escape, and other MPA symptoms. Studies that only provided data on the duration of mobile phone use were excluded.
Study Design
Quantitative observational (cross-sectional and cohort/longitudinal) studies were included.
Other Criteria
Studies were included if they were published in peer-reviewed journals and were written in English. If 2 studies were based on the same data set, the study published earlier was selected for inclusion in the review.
Exclusion Criteria
Case-control studies were excluded because they examined specific groups that were beyond the scope of this review. Furthermore, reviews, meta-analyses, commentaries, replies, clinical guidelines, conference abstracts, theses, and book chapters were also excluded.
Data Extraction and Synthesis
A total of 892 studies were identified by reading the titles and abstracts. Among these, 46 candidate studies were identified after reading their full text. At this stage, 24 studies were excluded based on the above criteria. The remaining 22 studies were deemed eligible and included in the systematic review. The final meta-analysis included 17 of the 22 studies (Figure 1 shows the details of the article screening process).
Figure 1.
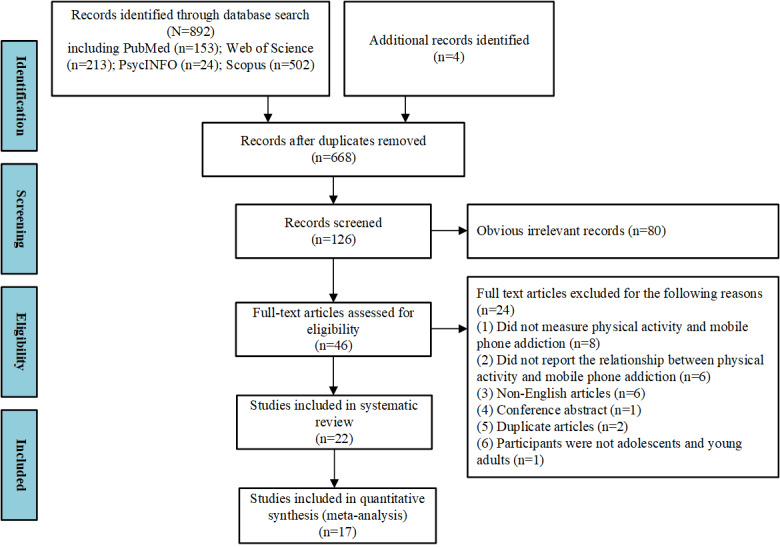
Flow diagram of article screening process.
Two reviewers independently extracted data from the included articles and entered the data into a form tailored to the requirements of this review. The extracted data included (1) publication details (author, year, and country); (2) sample characteristics (sample size, sex of participants, and type of participant); (3) time of data collection; (4) measurements of PA and MPA; and (5) the main study outcome (ie, correlation coefficient).
Methodological Quality Assessment
The Joanna Briggs Institute (JBI) appraisal checklist, which has 10 items, was used to examine the methodological quality of the included cross-sectional studies [42]. The studies were given a score of 0 to 2 for each item. Studies with an overall score higher than 70% were considered high quality with a low risk of bias. Details of the scoring criteria applied in the JBI appraisal checklist are presented in Multimedia Appendix 2.
Data Analysis
All statistical analyses were conducted with Comprehensive Meta-Analysis software (version 3; Biostat Inc).
All data were extracted from the included studies. The pooled Pearson correlation coefficients (with the corresponding 95% CIs) between PA and MPA were calculated with the inverse variance method. Subsequently, the Pearson correlation coefficients were transformed to Fisher z scores before the pooled estimate was obtained to calculate variance-stabilized correlation coefficients, as described previously [43] The effect sizes were interpreted in line with recent suggestions concerning correlations for psychometrics with r: small (r=0.10-0.20), medium (r=0.21-0.35), and large (r>0.35) [44].
The Cochran Q test and the I2 statistic were employed to measure heterogeneity across studies. The Cochran Q determines the conformity to the normal distribution of effect sizes. A significant value (P<.10) indicates heterogeneity. I2 is an estimate of the ratio of true heterogeneity in the observed variation. I2>50% reflects statistically significant between-study heterogeneity [45]. For such studies, the random effects model was used to calculate the summary of the Pearson correlation coefficients with a P value <.05 or I2>50% [44]. Otherwise, the fixed effects model was used [44].
To determine potential moderators of heterogeneity, subgroup analyses were carried out for country or region, population (college students and adolescents), and time of data collection (before or during COVID-19). All subgroup analyses were conducted with a mixed effects analysis. The random effects model was used to summarize the studies within the respective subgroups, and the fixed effects model was used to test for significant differences between the subgroups [46]. Full details of coding forms for the subgroups are provided in Multimedia Appendix 3.
To determine the influence of individual studies on the summary correlation coefficients and test the robustness of the correlations between PA and MPA, sensitivity analyses were conducted by sequentially omitting one study at time [11].
Funnel plots were established to determine the existence of potential publication bias. Additionally, the Begg rank correlation test and Egger linear regression test were performed to determine publication bias, with P<.05 indicating significant publication bias [47,48]. In the case of publication bias, the trim-and-fill method was used to adjust for funnel plot asymmetry [11].
Other statistical analyses performed included valid measures of the association between PA and MPA, measured with the correlation coefficient (r), standardized regression coefficient (b), unstandardized regression coefficient (β), odds ratio (OR), mean, and SD. To include as many eligible studies as possible, several data transformation steps were used. For studies that reported the mean and SD, the Cohen d effect size was calculated and converted to a correlation [49]. Studies that reported relevant ORs with 95% CIs were converted to Cohen d effect estimates and then to correlations [50]. The authors of the eligible studies were contacted if potentially relevant data were missing.
Results
Descriptive Characteristics
Table 1 presents a summary of the characteristics of the included studies. Overall, 23,365 participants aged between 15 and 26 years were included. Eighteen studies (numbers 1 to 22) were included in the systematic review, and 17 studies (numbers 1 to 17) were included in the meta-analysis. Moreover, 17 studies reported a correlation between PA and MPA. Considering the high heterogeneity among studies (Q=468.050, P<.001; I2=96.582), the random effects model was used to estimate the effect size of summary r (r=–0.243; 95% CI –0.309 to –0.175; P<.001; Table 2 and Figure 2). This result showed that PA was moderately negatively correlated with MPA.
Table 1.
Characteristics of the studies included in the review.
| Study | Country | Size, n | Male, n | Population | Age (years) | Time period | MPAa measurement | PAb measurement | r |
| 1. Kim et al, 2015 [30] |
South Korea | 110 | 67 | College students | Mean 21.03 (SD 1.61) | 2015 | SAPSc | 3D sensor pedometer | –0.798 |
| 2. Haug et al, 2015 [34] |
Switzerland | 1519 | 732 | Adolescents | Range 16-21 | Feb 2015 to Jun 2015 | SAS-SVd | “Outside school: How many hours a week do you exercise or participate in sports that make you sweat or become out of breath?” | –0.019 |
| 3. Yang et al, 2019 [32] |
China | 608 | 158 | College students | —e | Dec 2018 to Jan 2019 | MPATSf | PARS-3g | –0.124 |
| 4. Haripriya et al, 2019 [51] | India | 113 | 63 | College students | Mean 22.15 (SD 1.69) | Apr 2019 to May 2019 | SAPS | IPAQ-SFh | –0.335 |
| 5. Numanoğlu- Akbaş et al, 2020 [52] |
Turkey | 388 | 129 | College students | Range 17-25 | Jan 2019 to Jun 2019 | SASi | IPAQ-SF | –0.112 |
| 6. Zhong et al, 2021 [31] |
China | 394 | 115 | College students | — | Jul 29, 2020 | CSMDQj | PARS-3 | –0.190 |
| 7. Hosen et al, 2021 [53] |
Bangladesh | 601 | 344 | College students | — | Oct 2020 to Nov 2020 | SABASk | Physical exercise questions (eg, at least 30 minutes daily walking, cycling, swimming, or other activities regularly) | –0.249 |
| 8. Li et al, 2021 [33] |
China | 2407 | 280 | Adolescents | Mean 16.27 (SD 1.02) | Dec 2020 to Feb 2021 | Self-rating questionnaire for adolescent problematic mobile phone use | PA questionnaire Al | –0.235 |
| 9. Buke et al, 2021 [54] |
Turkey | 300 | 166 | College students | Mean 21.36 (SD 2.33) | Apr 2020 | SAS-SV | IPAQm | –0.262 |
| 10. Abbasi et al, 2021 [35] | Malaysia | 250 | 145 | College students | — | May 2020 | SAS-SV | Physical activity questionnaire Bn | –0.201 |
| 11. Islam et al, 2021 [55] |
Bangladesh | 5511 | 3254 | College students | Mean 21.20 (SD 1.70) | Jul 2020 | SABAS | Questions were asked regarding the engagement in infrequent activities (including home quarantine regular/frequent activities (ie, academic/other studies, social-media use, watching television, household chores, and professional activities) | –0.238 |
| 12. Ding et al, 2021 [56] |
China | 1724 | 740 | College students | Mean 19.56 (SD 0.95) | Sep 2020 | MPATS | PARS-3 | –0.445 |
| 13. Halil, 2021 [57] |
Pakistan | 236 | 123 | College students | — | 2020 to 2021 | SAS-SV | IPAQ-SF | –0.258 |
| 14. Guo et al, 2022 [58] |
China | 1433 | 704 | College students | Mean 19.67 (SD 1.62) | Dec 2020 to Feb 2021 | MPATS | PARS-3 | –0.158 |
| 15. Saffari et al, 2022 [59] |
Taiwan | 391 | 0 | College students | Mean 22.85 | Aug 2021 to Sep 2021 | SABAS | IPAQ-SF | –0.255 |
| 16. Lin et al, 2022 [60] |
China | 1787 | 628 | College students | Range 18-22 | Aug 2020 to Sep 2021 | SAS | IPAQ-SF | –0.153 |
| 17. Chen et al, 2022 [61] |
China | 9406 | 3516 | College students | Mean 19.58 (SD 1.07) | Mar 2022 to Apr 2022 | MPASo | IPAQ-Lp | –0.060 |
| 18. Venkatesh et al, 2019 [62] |
Saudi Arabia | 205 | 101 | College students | Mean 23.28 | Jan 2016 to Mar 2016 | SAS-SV | “Outside school: How many hours a week do you exercise or participate in sports that make you sweat or become out of breath?” | — |
| 19. Xie et al, 2019 [63] |
China | 2134 | 917 | College students | Mean 19.25 (SD 1.42) | Jun 2014 to Dec 2014 | Self-rating questionnaire for adolescent problematic mobile phone use | During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day? | — |
| 20. Pereira et al, 2020 [64] | Brazil | 667 | 308 | Adolescents | Range 13-18 | — | SAS-SV | IPAQ-SF | — |
| 21. Tao et al, 2020 [65] |
China | 4624 | 2057 | College students | Mean 19.91 (SD 1.27) | May 2018 to Jun 2018 | Self-rating questionnaire for adolescent problematic mobile phone use | IPAQ-SF | — |
| 22. Zou et al, 2021 [66] |
China | 251 | 52 | College students | Mean 19.01 (SD 0.85) | Apr 2019 to Jun 2019 | Self-rating questionnaire for adolescent problematic mobile phone use | IPAQ-Cq | — |
aMPA: mobile phone addiction.
bPA: physical activity.
cSAPS: Smartphone Addiction Proneness Scale.
dSAS-SV: Smartphone Addiction Scale–Short Version.
eNot available.
fMPATS: Mobile Phone Addiction Tendency Scale.
gPARS-3: Physical Activity Rating Scale–3.
hIPAQ-SF: International Physical Activity Questionnaire–Short Form.
iSAS: Smartphone Addiction Scale.
jCSMDQ: College Students Mobile Phone Dependence Questionnaire.
kSABAS: Smartphone Application-Based Addiction Scale.
lPhysical activity questionnaire A was derived from [67].
mIPAQ: International Physical Activity Questionnaires.
nPhysical activity questionnaire B was derived from [68].
oMPAS: Mobile Phone Addiction Scale.
pIPAQ-L: International Physical Activity Questionnaire–Long Form.
qIPAQ C: International Physical Activity Questionnaire–Chinese.
Table 2.
Statistics for each studya.
| Study | r (total r=0.243) | 95% CI (total 95% CI –0.309 to –0.175) | z (total z=–6.810) | P value (total P<.001) | Weight (total 100%) |
| Kim et al, 2015 [30] | –0.798 | –0.190 to 0.184 | –0.031 | .98 | 4.48% |
| Haug et al, 2015 [34] | –0.019 | –0.069 to 0.031 | –0.740 | .46 | 6.35% |
| Yang et al, 2019 [32] | –0.124 | –0.202 to –0.045 | –3.066 | .002 | 6.06% |
| Haripriya et al, 2019 [51] | –0.335 | –0.486 to –0.165 | –3.753 | <.001 | 4.60% |
| Numanoğlu-Akbaş et al, 2020 [52] | –0.112 | –0.209 to –0.013 | –2.207 | .03 | 5.81% |
| Zhong et al, 2021 [31] | –0.190 | –0.283 to –0.093 | –3.803 | <.001 | 5.82% |
| Hosen et al, 2021 [53] | –0.249 | –0.323 to –0.172 | –6.220 | <.001 | 6.05% |
| Li et al, 2021 [33] | –0.235 | –0.272 to –0.197 | –11.742 | <.001 | 6.42% |
| Buke et al, 2021 [54] | –0.262 | –0.364 to –0.153 | –4.623 | <.001 | 5.62% |
| Abbasi et al, 2021 [35] | –0.201 | –0.317 to –0.079 | –3.203 | <.001 | 5.46% |
| Islam et al, 2021 [55] | –0.238 | –0.263 to –0.213 | –18.009 | <.001 | 6.50% |
| Ding et al, 2021 [56] | –0.445 | –0.482 to –0.406 | –19.848 | <.001 | 6.37% |
| Halil, 2021 [57] | –0.258 | –0.373 to –0.135 | –4.029 | <.001 | 5.41% |
| Guo et al, 2022 [58] | –0.158 | –0.208 to –0.107 | –6.025 | <.001 | 6.34% |
| Saffari et al, 2022 [59] | –0.255 | –0.345 to –0.160 | –5.136 | <.001 | 5.81% |
| Lin et al, 2022 [60] | –0.153 | –0.198 to –0.107 | –6.513 | <.001 | 6.38% |
| Chen et al, 2022 [61] | –0.060 | –0.080 to –0.040 | –5.825 | <.001 | 6.52% |
aHeterogeneity: Q=468.050; P<.001; I²=96.582.
Figure 2.
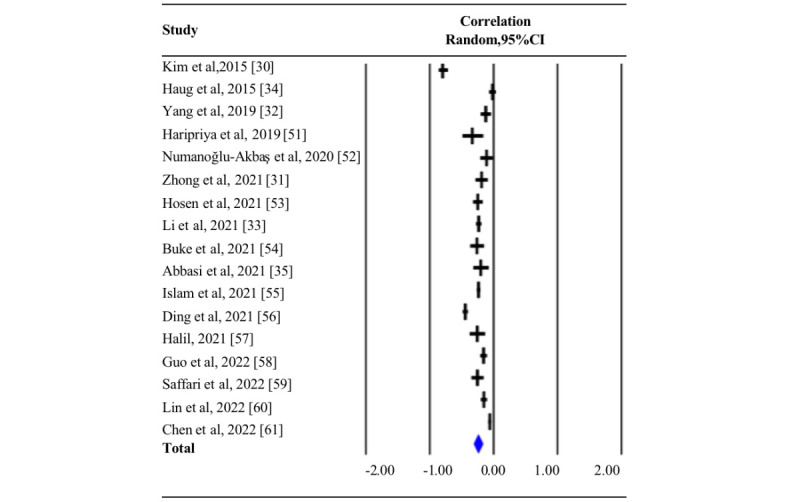
Summary of pooled correlation between physical activity and mobile phone addiction. The blue diamond represents the overall pooled correlation for the random effects model [30-35,51-61].
Subgroup Analysis
As shown in Table 3, the summary correlation coefficient between PA and MPA did not change when stratified by time of data collection, country or region, or type of population (all Pb>.05). However, to allow comparison with other studies, we present model-implied effect sizes for each level of the moderator.
Table 3.
Subgroup analyses of summary correlation between PA and MPA. Pa values for the within-subgroup effect sizes were calculated with the z test; Pb values for between-subgroup differences were calculated with the Q test; and Pc values for heterogeneity within subgroups were calculated with the Q test.
| Moderator | Studies, n | Summary r (95% CI) | Pa value | Heterogeneity | Pb value | ||
|
|
I2 (%) | Pc value |
|
||||
| Time of data collection | .14 | ||||||
|
|
Before COVID-19 | 4 | –0.333 (–0.466 to –0.187) | <.001 | 97.555 | <.001 |
|
|
|
During COVID-19 | 13 | –0.207 (–0.285 to –0.126) | <.001 | 96.438 | <.001 |
|
| Country or region | .71 | ||||||
|
|
Developed regions | 2 | –0.446 (–0.616 to 0.236) | .39 | 99.133 | <.001 |
|
|
|
China | 7 | –0.201 (–0.311 to –0.127) | <.001 | 97.873 | <.001 |
|
|
|
Other developing regions | 8 | –0.217 (–0.326 to –0.103) | <.001 | 63.310 | <.001 |
|
| Population | .26 | ||||||
|
|
Young adults | 15 | –0.250 (–0.325 to –0.173) | <.001 | 96.681 | <.001 |
|
|
|
Adolescents | 2 | –0.129 (–0.333 to 0.086) | .24 | 97.787 | <.001 |
|
The time of data collection did not significantly moderate the effect sizes (between-subgroup Pb=.14). Notably, the summary correlation coefficient of the studies reporting on data collected before COVID-19 was slightly higher compared with that for data collected during COVID-19. Specifically, the effect sizes for data collection before COVID-19 were moderate, with a 95% CI that did not overlap with 0 (r=–0.333, 95% CI –0.466 to –0.187; k=4; Pa<.001), whereas the effect sizes for data collected during COVID-19 were also moderate, with 95% CIs that overlapped with 0 (r=–0.207, 95% CI –0.285 to –0.126, k=13; Pa<.001).
Similarly, we did not find significant moderator effect sizes for country or region (between-subgroup Pb=.71). The summary correlation coefficient for both China and other developing regions showed a similarly moderate effect size (China: r=–0.201, 95% CI –0.311 to –0.127; k=7; Pa<.001; other developing regions: r= –0.217, 95% CI –0.326 to –0.103; k=8; Pa<.001). However, the effect sizes for developed regions with a 95% CI that overlapped with 0 (r=–0.446, 95% CI –0.616 to 236, k=2; Pa=.24) were not significant.
In addition, there were no significant moderator effect sizes for the type of population (between-subgroup: Pb=.26). Specifically, we found that the effect sizes for young adults were moderate, with a 95% CI that did not overlap with 0 (r=0.250, 95% CI –0.325 to –0.173, k=15; Pa<.001). However, the effect sizes for adolescents were not significant, with a 95% CI that overlapped with 0 (r=–0.129, 95% CI –0.333 to 0.086, k=2, Pa=.24).
Sensitivity Analyses and Publication Bias
In the analysis that removed studies one at a time, no evident outliers were identified. Thus, the correlation coefficient for removing each study was in the range of r=–0.195 to –0.248. This shows that no one study significantly skewed or changed the correlation coefficient or influenced the overall results of the meta-analysis. Therefore, the results were reliable.
Subjectively speaking, we could not determine the existence of publication bias from the funnel plots for the summary correlation coefficients, as shown in Figure 3A. Studies with a small sample size are unlikely to result in symmetrical distributions of scattered points. The Begg rank correlation tests and Egger linear regression tests showed no significant publication bias (P=.62 and P=.14, respectively). After the trim-and-fill analysis, the correlation between PA and MPA remained statistically significant (number to trim and fill 6, summary r=–0.319, 95% CI –0.40552 to –0.22771; Figure 3B). Therefore, the overall modeling results after correction remained unchanged. Thus, we concluded that there was no publication bias.
Figure 3.
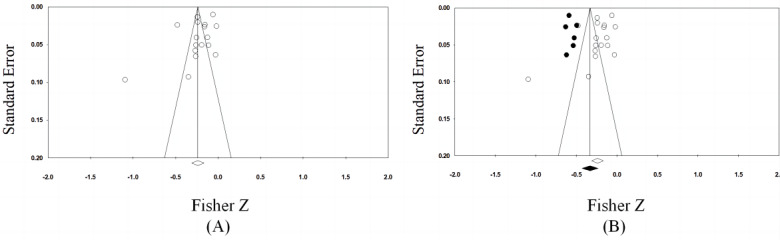
Funnel plots of (A) publication bias and (B) publication bias with trim and fill.
Methodological Quality Assessment
The methodological quality assessment results are shown in Table 4. Notably, the mean scores of the included studies and the other studies were 15.29 (SD 1.53) and 15.40 (SD 0.89), respectively. All included studies were of high quality with a low risk of bias.
Table 4.
Methodological quality of the studies.
| Number | Study | Joanna Briggs Institute appraisal checklist items | Total score (%) | Overall risk of bias | |||||||||||
|
|
|
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|
|
||
| 1 | Kim et al, 2015 [30] | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 1 | 15 (75) | Low | ||
| 2 | Haug et al, 2015 [34] | 2 | 0 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 16 (80) | Low | ||
| 3 | Yang et al, 2019 [32] | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 18 (80) | Low | ||
| 4 | Haripriya et al, 2019 [51] | 2 | 0 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 1 | 15 (75) | Low | ||
| 5 | Numanoğlu-Akbaş et al, 2020 [52] | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 1 | 2 | 13 (65) | Mid | ||
| 6 | Zhong et al, 2021 [31] | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 2 | 2 | 2 | 16 (80) | Low | ||
| 7 | Hosen et al, 2021 [53] | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 1 | 2 | 14 (70) | Low | ||
| 8 | Li et al, 2021 [33] | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 17 (85) | Low | ||
| 9 | Buke et al, 2021 [54] | 1 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 1 | 15 (75) | Low | ||
| 10 | Abbasi et al, 2021 [35] | 2 | 1 | 1 | 1 | 2 | 2 | 0 | 1 | 1 | 1 | 15 (75) | Low | ||
| 11 | Islam et al, 2021 [55] | 1 | 0 | 1 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 15 (75) | Low | ||
| 12 | Ding et al, 2021 [56] | 2 | 1 | 1 | 1 | 2 | 2 | 0 | 2 | 2 | 1 | 14 (70) | Low | ||
| 13 | Halil, 2021 [57] | 2 | 0 | 1 | 1 | 2 | 2 | 0 | 2 | 2 | 2 | 14 (70) | Low | ||
| 14 | Guo et al, 2022 [58] | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 18 (80) | Low | ||
| 15 | Saffari et al, 2022 [59] | 2 | 0 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 17 (85) | Low | ||
| 16 | Lin et al, 2022 [60] | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 1 | 13 (65) | Mid | ||
| 17 | Chen et al, 2022 [61] | 2 | 2 | 0 | 1 | 2 | 2 | 0 | 2 | 2 | 2 | 15 (75) | Low | ||
| 18 | Venkatesh et al, 2019 [62] |
1 | 0 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 1 | 14 (70) | Low | ||
| 19 | Xie et al, 2019 [63] | 1 | 0 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 16 (80) | Low | ||
| 20 | Pereira et al, 2020 [64] | 1 | 0 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 16 (80) | Low | ||
| 21 | Tao et al, 2020 [65] | 2 | 1 | 1 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 15 (75) | Low | ||
| 22 | Zou et al, 2021 [66] | 2 | 0 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 16 (80) | Low | ||
Discussion
Meta-analytic Findings
To the best of our knowledge, this is the first meta-analysis to explore pooled correlation coefficients of PA and MPA. Our analysis of 17 studies found a moderately negative correlation between PA and MPA, with a summary Pearson correlation coefficient of r=–0.243. This is in line with a previous review [40]. Sensitivity analyses did not find significant publication bias, indicating that the pooled analyses of the correlation coefficients provided reliable and convincing results. In addition, all the included studies were high quality with a low risk of bias. Subgroup analysis showed that none of the hypothesized moderators (data collection, country or region, and type of population) significantly influenced the relationship between PA and MPA, as confirmed with a mixed effects analysis.
The target subjects of research into MPA are adolescents and young adults, who are relatively less self-disciplined in controlling their frequency of mobile phone use and are more susceptible to smartphone use addiction compared to middle-aged or older adults [29]. Lack of self-control is an essential factor influencing MPA among adolescents and young adults. Previous studies found that self-control regulates the correlation between PA and MPA. Factors such as negative emotions (eg, anxiety [69,70] and loneliness [71,72]) and mental toughness [73,74] have been shown to affect the relationship between PA and MPA. We speculate that these factors may modulate the relationship between PA and MPA.
Results of magnetic resonance imaging studies suggest that MPA is associated with structural brain abnormalities, like other types of addiction dependence. For example, the insula cortex participates in the formation of addictive behaviors, because these behaviors may influence the decision-making process in terms of choosing immediate rewards that are always associated with physiological state while eliciting strong interoceptive signals [75]. Two recent studies reported changes in gray matter volume in this region (ie, the insula cortex) among people with MPA [66,76]. Exercise has been shown to improve brain health [77,78]. Therefore, we hypothesize that the relationship between PA and MPA might be influenced by the structure and function of the insula and even other brain regions.
Differences in Subgroup Analysis
Notably, the time of data collection did not significantly influence the relationship between PA and MPA. Moreover, a moderate negative relationship was found between PA and MPA among adolescents and young adults before and during the COVID-19 pandemic. According to the compensatory internet use theory, when people encounter psychosocial problems in the real world, they are likely to use the internet or smartphones as a coping mechanism to alleviate negative emotions [79]. The restrictions imposed on participation in social activities and gatherings during the COVID-19 pandemic increased anxiety, depression, and stress levels in people [80]. Therefore, they were more likely to overly rely on their mobile phones to cope with stress. Moreover, recent studies have shown that adolescents and young adults have had low PA levels during the COVID-19 pandemic [81,82]. The target subjects in our study were adolescents and young adults, who are more inclined to use social media for physical training. A previous study found that young-adult Spanish university students used social media apps to improve their high-intensity interval training [82], mind-body activities, and strength exercises. In other words, adolescents and young adults used social media to facilitate their participation in PA during the pandemic [82]. This reduced the time spent sitting for long periods of time and reduced leisure-time screen activities, subsequently reducing the risk of MPA in young people [30].
The present findings demonstrate that country or region do not have a significant moderating role on the relationship between PA and MPA. Notably, a medium-strength negative relationship between PA and MPA has been reported in China and other developing counties among adolescents and young adults. However, this correlation was not found in developed countries. This finding should be interpreted with caution, because it is based on 2 studies from developed countries. These 2 studies were carefully reviewed elsewhere [30,34]. In addition, we found that one of these studies reported a weak negative correlation between PA and MPA [34], whereas the other found a significant, strong negative correlation [30]. It should be noted that the 2 studies were published around the same time. The difference in the correlation results may be due to the type of PA measurement tools used. For instance, one of the studies used a pedometer sensor to measure the level of PA, which is more precise [30]. The influence of measurement errors associated with self-reported PA questionnaires also needs to be acknowledged. The majority of the reviewed studies used self-reported scales or questionnaires; thus, we suggest that accelerometry should be adopted in future studies to obtain more reliable data.
Further analysis revealed that population type did not significantly affect the relationship between PA and MPA. This may be explained by the widespread use of mobile phones. This is especially true for young people, as their ownership rate for smartphones is very high. Additionally, subgroup analysis revealed that there was no significant correlation between PA and MPA among adolescents (P=.26). We presume that this might be influenced by the degree of external restrictions on the use of mobile phones. Compared with adults (eg, college students), adolescents are subjected to more control and restriction measures on mobile phone use by their parents, schools, and even by the mobile phone apps themselves. Therefore, they are less likely to influence the correlation [83]. These findings, however, should be interpreted with caution, because only 2 studies on adolescents were analyzed.
Limitations and Strengths
In conclusion, our study indicates that a low PA level contributes to MPA behavior. This is because low PA encourages a sedentary lifestyle among young adults. The PA guidelines of the World Health Organization encourage individuals of different ages to participate in PA. Previous studies have shown that increasing the PA level of young adults can reduce MPA behavior. We recommend higher PA levels than those stipulated in the guidelines of the World Health Organization, because more PA could bring more mental health benefits. From a practical perspective, the findings of this study may help to inform countermeasures to prevent MPA behavior among adolescents and young adults amid the COVID-19 pandemic and future public health crises.
All previous findings were objectively stated, analyzed, and interpreted using an appropriate research design. All original data were retained to provide a reference for future research. The repeatability and reproducibility of our analyses have been ensured. However, there are some limitations and potential sources of bias that need to be noted. First, only studies published in English were included in our meta-analysis. Second, the studies mainly provided cross-sectional data, which do not allow determination of causality in the relationship between PA and MPA. Third, we only analyzed a young population. Fourth, no study reported moderating variables between PA and MPA. Finally, although a sensitivity analysis was conducted, sources of bias were identified, and our results should thus be interpreted with caution. Further case-control and cohort studies are needed to test the benefits of PA on MPA in young adults.
Conclusion
Our findings demonstrate a moderate negative relationship between PA and MPA among young adults. The strength of the relationship between PA and MPA did not differ by time of data collection, country or region, or type of population.
Acknowledgments
This study received funding from the Research Foundation for Young Teachers of Shenzhen University (grant QNJS0274), the High-level Scientific Research Foundation for the Introduction of Talent of Shenzhen University (grant RC00228), the Natural Science Featured Innovation Projects in Ordinary Universities in Guangdong Province (grant 2021KTSCX297), and the Scientific Research Platform and Project of Colleges and Universities of the Education Department of Guangdong Province (grant 2022ZDZX2087).
Abbreviations
- JBI
Joanna Briggs Institute
- MPA
mobile phone addiction
- OR
odds ratio
- PA
physical activity
- PRISMA
Preferred Reporting Items for Systematic Review and Meta-analyses
Detailed search strategy.
Details of the scoring criteria in the JBI appraisal checklist. JBI: Joanna Briggs Institute.
Full details of coding forms for the subgroups.
Footnotes
Authors' Contributions: WX and ZR were responsible for conceptualization of the research, investigation, and forming the hypothesis. JW and WX conducted the systematic search, data extraction, and quality assessment and data analyses. JW and WX wrote the first draft of the manuscript. JY, QS, LP, QEL, and ZR reviewed and edited the initial draft and its revisions. All authors agree with the results and conclusions. All authors read and approved the final manuscript.
Conflicts of Interest: None declared.
References
- 1.Billieux J, Maurage P, Lopez-Fernandez O, Kuss DJ, Griffiths MD. Can disordered mobile phone use be considered a behavioral addiction? an update on current evidence and a comprehensive model for future research. Curr Addict Rep. 2015 Jun 01;2(2):156–162. doi: 10.1007/s40429-015-0054-y. https://link.springer.com/content/pdf/10.1007/s40429-015-0054-y.pdf . [DOI] [Google Scholar]
- 2.Sert H, Taskin Yilmaz F, Karakoc Kumsar A, Aygin D. Effect of technology addiction on academic success and fatigue among Turkish university students. Fatigue: Biomed Health Behav. 2019 Feb 26;7(1):41–51. doi: 10.1080/21641846.2019.1585598. [DOI] [Google Scholar]
- 3.Battle DE. Diagnostic and Statistical Manual of Mental Disorders (DSM) Codas. 2013;25(2):191–2. doi: 10.1590/s2317-17822013000200017. https://www.scielo.br/scielo.php?script=sci_arttext&pid=S2317-17822013000200017&lng=en&nrm=iso&tlng=en .S2317-17822013000200017 [DOI] [PubMed] [Google Scholar]
- 4.Zou Z, Wang H, d'Oleire Uquillas Federico, Wang X, Ding J, Chen H. Definition of substance and non-substance addiction. Adv Exp Med Biol. 2017;1010:21–41. doi: 10.1007/978-981-10-5562-1_2. [DOI] [PubMed] [Google Scholar]
- 5.Amiri M, Dowran B, Salimi H, Zarghami MH. The problematic use of mobile phone and mental health: A review study in Iran. J Educ Health Promot. 2020;9:290. doi: 10.4103/jehp.jehp_268_20. https://europepmc.org/abstract/MED/33282995 .JEHP-9-290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nunes PPDB, Abdon APV, Brito CBD, Silva FVM, Santos ICA, Martins DDQ, Meira PMF, Frota MA. Factors related to smartphone addiction in adolescents from a region in Northeastern Brazil. Cien Saude Colet. 2021 Jul;26(7):2749–2758. doi: 10.1590/1413-81232021267.08872021. https://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232021000702749&lng=en&nrm=iso&tlng=en .S1413-81232021000702749 [DOI] [PubMed] [Google Scholar]
- 7.Zou Y, Chen S, Dong Q, Wang H, Xie X, Ji S. Current situation of mobile phone addiction and its relationship with personality among college students in Hainan Province. China Journal of Health Psychology. 2017;25:025–5. doi: 10.13342/j.cnki.cjhp.2017.09.025. [DOI] [Google Scholar]
- 8.Soliman Elserty N, Ahmed Helmy N, Mohmed Mounir K. Smartphone addiction and its relation to musculoskeletal pain in Egyptian physical therapy students. Eur J Physiother. 2018 Dec 31;22(2):70–78. doi: 10.1080/21679169.2018.1546337. [DOI] [Google Scholar]
- 9.Jahagirdar V, Rama K, Soppari P, Kumar M. Mobile phones: vital addiction or lethal addiction? mobile phone usage patterns and assessment of mobile addiction among undergraduate medical students in Telangana, India. J Addict. 2021;2021:8750650. doi: 10.1155/2021/8750650. doi: 10.1155/2021/8750650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kim K, Yee J, Chung JE, Kim HJ, Han JM, Kim JH, Lee KE, Gwak HS. Smartphone addiction and anxiety in adolescents - a cross-sectional study. Am J Health Behav. 2021 Sep 30;45(5):895–901. doi: 10.5993/AJHB.45.5.9. [DOI] [PubMed] [Google Scholar]
- 11.Li Y, Li G, Liu L, Wu H. Correlations between mobile phone addiction and anxiety, depression, impulsivity, and poor sleep quality among college students: A systematic review and meta-analysis. J Behav Addict. 2020 Oct 12;9(3):551–571. doi: 10.1556/2006.2020.00057. https://europepmc.org/abstract/MED/32903205 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ivanova A, Gorbaniuk O, Błachnio A, Przepiórka Aneta, Mraka N, Polishchuk V, Gorbaniuk J. Mobile phone addiction, phubbing, and depression among men and women: a moderated mediation analysis. Psychiatr Q. 2020 Sep;91(3):655–668. doi: 10.1007/s11126-020-09723-8. https://europepmc.org/abstract/MED/32146681 .10.1007/s11126-020-09723-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Matar Boumosleh J, Jaalouk D. Depression, anxiety, and smartphone addiction in university students- A cross sectional study. PLoS One. 2017;12(8):e0182239. doi: 10.1371/journal.pone.0182239. https://dx.plos.org/10.1371/journal.pone.0182239 .PONE-D-16-41014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mohammadbeigi A, Absari R, Valizadeh F, Saadati M, Sharifimoghadam S, Ahmadi A, Mokhtari M, Ansari H. Sleep quality in medical students; the impact of over-use of mobile cell-phone and social networks. J Res Health Sci. 2016;16(1):46–50. https://europepmc.org/abstract/MED/27061997 .2484 [PMC free article] [PubMed] [Google Scholar]
- 15.Lane H, Chang C, Huang C, Chang Y. An investigation into smartphone addiction with personality and sleep quality among university students. Int J Environ Res Public Health. 2021 Jul 16;18(14):7588. doi: 10.3390/ijerph18147588. https://europepmc.org/abstract/MED/34300037 .ijerph18147588 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhang T, Gong N, Jia R, Li H, Ni X. Stroop effect in smartphone addiction among college students. Medicine (Baltimore) 2021 Jul 30;100(30):e26741. doi: 10.1097/MD.0000000000026741. https://europepmc.org/abstract/MED/34397714 .00005792-202107300-00035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shah PP, Sheth MS. Correlation of smartphone use addiction with text neck syndrome and SMS thumb in physiotherapy students. Int J Community Med Public Health. 2018 May 22;5(6):2512. doi: 10.18203/2394-6040.ijcmph20182187. https://www.ijcmph.com/index.php/ijcmph/article/view/2970/2118 . [DOI] [Google Scholar]
- 18.Alotaibi MS, Fox M, Coman R, Ratan ZA, Hosseinzadeh H. Smartphone addiction prevalence and its association on academic performance, physical health, and mental well-being among university students in Umm Al-Qura University (UQU), Saudi Arabia. Int J Environ Res Public Health. 2022 Mar 21;19(6):3710. doi: 10.3390/ijerph19063710. https://europepmc.org/abstract/MED/35329397 .ijerph19063710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Public health implications of excessive use of the internet, computers, smartphones and similar electronic devices: Meeting report, Main Meeting Hall, Foundation for Promotion of Cancer Research, National Cancer Research Centre, Tokyo, Japan, 27-29 August 2014. World Health Organization. 2015. [2022-12-05]. https://apps.who.int/iris/bitstream/handle/10665/184264/9789241509367_eng.pdf?sequence=1&isAllowed=y .
- 20.Banerjee D. The COVID-19 outbreak: crucial role the psychiatrists can play. Asian J Psychiatr. 2020 Apr;50:102014. doi: 10.1016/j.ajp.2020.102014. https://europepmc.org/abstract/MED/32240958 .S1876-2018(20)30125-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Islam MS, Potenza MN, van Os J. Posttraumatic stress disorder during the COVID-19 pandemic: upcoming challenges in Bangladesh and preventive strategies. Int J Soc Psychiatry. 2021 Mar;67(2):205–206. doi: 10.1177/0020764020954469. [DOI] [PubMed] [Google Scholar]
- 22.Brand M, Young KS, Laier C, Wölfling Klaus, Potenza MN. Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: An Interaction of Person-Affect-Cognition-Execution (I-PACE) model. Neurosci Biobehav Rev. 2016 Dec;71:252–266. doi: 10.1016/j.neubiorev.2016.08.033. https://linkinghub.elsevier.com/retrieve/pii/S0149-7634(16)30262-7 .S0149-7634(16)30262-7 [DOI] [PubMed] [Google Scholar]
- 23.Elhai JD, Yang H, McKay D, Asmundson GJG. COVID-19 anxiety symptoms associated with problematic smartphone use severity in Chinese adults. J Affect Disord. 2020 Sep 01;274:576–582. doi: 10.1016/j.jad.2020.05.080. https://europepmc.org/abstract/MED/32663990 .S0165-0327(20)31228-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Li L, Xu D, Chai J, Wang D, Li L, Zhang L, Lu L, Ng CH, Ungvari GS, Mei S, Xiang Y. Prevalence of Internet addiction disorder in Chinese university students: A comprehensive meta-analysis of observational studies. J Behav Addict. 2018 Sep 01;7(3):610–623. doi: 10.1556/2006.7.2018.53. https://europepmc.org/abstract/MED/30010411 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lian S, Sun X, Niu G, Yang X, Zhou Z, Yang C. Mobile phone addiction and psychological distress among Chinese adolescents: The mediating role of rumination and moderating role of the capacity to be alone. J Affect Disord. 2021 Jan 15;279:701–710. doi: 10.1016/j.jad.2020.10.005. https://europepmc.org/abstract/MED/33197839 .S0165-0327(20)32849-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Long J, Liu T, Liao Y, Qi C, He H, Chen S, Billieux J. Prevalence and correlates of problematic smartphone use in a large random sample of Chinese undergraduates. BMC Psychiatry. 2016 Nov 17;16(1):408. doi: 10.1186/s12888-016-1083-3. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-016-1083-3 .10.1186/s12888-016-1083-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kuan G, Abdullah N, Kueh YC, Ismail M, Shafei MN, Morris T. Co-curricular activities and motives for participating in physical activity among health sciences students at Universiti Sains Malaysia, Malaysia. Malays J Med Sci. 2019 Jan;26(1):138–146. doi: 10.21315/mjms2019.26.1.13. https://europepmc.org/abstract/MED/30914901 .13mjms26012019_oa10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.WHO guidelines on physical activity and sedentary behaviour: web annex: evidence profiles. World Health Organization. 2020. [2022-12-05]. https://apps.who.int/iris/handle/10665/336657 . [PubMed]
- 29.Liu S, Xiao T, Yang L, Loprinzi PD. Exercise as an alternative approach for treating smartphone addiction: a systematic review and meta-analysis of random controlled trials. Int J Environ Res Public Health. 2019 Oct 15;16(20):3912. doi: 10.3390/ijerph16203912. https://europepmc.org/abstract/MED/31618879 .ijerph16203912 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kim S, Kim J, Jee Y. Relationship between smartphone addiction and physical activity in Chinese international students in Korea. J Behav Addict. 2015 Sep;4(3):200–5. doi: 10.1556/2006.4.2015.028. https://europepmc.org/abstract/MED/26551911 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zhong W, Wang Y, Zhang G. The impact of physical activity on college students’ mobile phone dependence: the mediating role of self-control. Int J Ment Health Addiction. 2020 Jul 29;19(6):2144–2159. doi: 10.1007/s11469-020-00308-x. [DOI] [Google Scholar]
- 32.Yang G, Tan G, Li Y, Liu H, Wang S. Physical exercise decreases the mobile phone dependence of university students in China: the mediating role of self-control. Int J Environ Res Public Health. 2019 Oct 24;16(21):4098. doi: 10.3390/ijerph16214098. https://europepmc.org/abstract/MED/31652978 .ijerph16214098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Li Y, Sun Q, Sun M, Sun P, Sun Q, Xia X. Physical exercise and psychological distress: the mediating roles of problematic mobile phone use and learning burnout among adolescents. Int J Environ Res Public Health. 2021 Sep 02;18(17):9261. doi: 10.3390/ijerph18179261. https://europepmc.org/abstract/MED/34501851 .ijerph18179261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Haug S, Castro RP, Kwon M, Filler A, Kowatsch T, Schaub MP. Smartphone use and smartphone addiction among young people in Switzerland. J Behav Addict. 2015 Dec;4(4):299–307. doi: 10.1556/2006.4.2015.037. https://europepmc.org/abstract/MED/26690625 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Abbasi GA, Jagaveeran M, Goh Y, Tariq B. The impact of type of content use on smartphone addiction and academic performance: Physical activity as moderator. Technol Soc. 2021 Feb;64:101521. doi: 10.1016/j.techsoc.2020.101521. [DOI] [Google Scholar]
- 36.Fennell C, Barkley JE, Lepp A. The relationship between cell phone use, physical activity, and sedentary behavior in adults aged 18–80. Comput Hum Behav. 2019 Jan;90:53–59. doi: 10.1016/j.chb.2018.08.044. [DOI] [Google Scholar]
- 37.Barkley JE, Lepp A. Mobile phone use among college students is a sedentary leisure behavior which may interfere with exercise. Comput Hum Behav. 2016 Mar;56:29–33. doi: 10.1016/j.chb.2015.11.001. [DOI] [Google Scholar]
- 38.Xiang M, Lin L, Wang Z, Li J, Xu Z, Hu M. Sedentary behavior and problematic smartphone use in Chinese adolescents: the moderating role of self-control. Front Psychol. 2019;10:3032. doi: 10.3389/fpsyg.2019.03032. https://europepmc.org/abstract/MED/32038398 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Zagalaz-Sánchez María Luisa, Cachón-Zagalaz Javier, Sánchez-Zafra María, Lara-Sánchez Amador. Mini review of the use of the mobile phone and its repercussion in the deficit of physical activity. Front Psychol. 2019 Jun 6;10:1307. doi: 10.3389/fpsyg.2019.01307. https://europepmc.org/abstract/MED/31244720 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009 Jul 21;6(7):e1000097. doi: 10.1371/journal.pmed.1000097. https://dx.plos.org/10.1371/journal.pmed.1000097 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Adhia A, Kernic MA, Hemenway D, Vavilala MS, Rivara FP. Intimate partner homicide of adolescents. JAMA Pediatr. 2019 Jun 01;173(6):571–577. doi: 10.1001/jamapediatrics.2019.0621. https://europepmc.org/abstract/MED/30985886 .2730578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. Adelaide, Australia: The Joanna Briggs Institute; 2017. [Google Scholar]
- 43.Zhang Y, Long G, Ding B, Sun G, Ouyang W, Liu M, Ye Z, Xu H, Li H. The impact of ambient temperature on the incidence of urolithiasis: a systematic review and meta-analysis. Scand J Work Environ Health. 2020 Mar 01;46(2):117–126. doi: 10.5271/sjweh.3866. https://www.sjweh.fi/article/3866 .3866 [DOI] [PubMed] [Google Scholar]
- 44.Polanin JR, Snilstveit B. Converting between effect sizes. Campbell Syst Rev. 2016;12:1–13. doi: 10.4073/CMPN.2016.3. [DOI] [Google Scholar]
- 45.Heeke C, Kampisiou C, Niemeyer H, Knaevelsrud C. A systematic review and meta-analysis of correlates of prolonged grief disorder in adults exposed to violent loss. Eur J Psychotraumatol. 2019;10(1):1583524. doi: 10.1080/20008198.2019.1583524. https://europepmc.org/abstract/MED/30949303 .1583524 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Fu Z, Burger H, Arjadi R, Bockting CLH. Effectiveness of digital psychological interventions for mental health problems in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Psychiatry. 2020 Oct;7(10):851–864. doi: 10.1016/S2215-0366(20)30256-X. https://europepmc.org/abstract/MED/32866459 .S2215-0366(20)30256-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994 Dec;50(4):1088–101. [PubMed] [Google Scholar]
- 48.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997 Sep 13;315(7109):629–34. doi: 10.1136/bmj.315.7109.629. https://europepmc.org/abstract/MED/9310563 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Xin F, Chen S, Clark C, Hong J, Liu Y, Cai Y. Relationship between fundamental movement skills and physical activity in preschool-aged children: a systematic review. Int J Environ Res Public Health. 2020 May 19;17(10):3566. doi: 10.3390/ijerph17103566. https://europepmc.org/abstract/MED/32438736 .ijerph17103566 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta-Analysis. Hoboken, NJ: John Wiley & Sons; 2021. [Google Scholar]
- 51.Haripriya S, Samuel SE, Megha M. Correlation between smartphone addiction, sleep quality and physical activity among young adults. J Clin Diagn Res. 2019;13(10):5–9. doi: 10.7860/jcdr/2019/42168.13212. [DOI] [Google Scholar]
- 52.Numanoğlu-Akbaş A, Suner-Keklik S, Yakut H. Investigation of the relationship between smart phone addiction and physical activity in university students. Balt J Health Phys Act. 2020 Dec 31;Supplement 1(1):63–73. doi: 10.29359/bjhpa.2020.suppl.1.07. https://www.balticsportscience.com/cgi/viewcontent.cgi?article=1186&context=journal . [DOI] [Google Scholar]
- 53.Hosen I, Al Mamun F, Sikder MT, Abbasi AZ, Zou L, Guo T, Mamun MA. Prevalence and associated factors of problematic smartphone use during the COVID-19 pandemic: a Bangladeshi study. Risk Manag Healthc Policy. 2021;14:3797–3805. doi: 10.2147/RMHP.S325126. https://europepmc.org/abstract/MED/34548828 .325126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Buke M, Egesoy H, Unver F. The effect of smartphone addiction on physical activity level in sports science undergraduates. J Bodyw Mov Ther. 2021 Oct;28:530–534. doi: 10.1016/j.jbmt.2021.09.003.S1360-8592(21)00204-7 [DOI] [PubMed] [Google Scholar]
- 55.Islam MS, Sujan MSH, Tasnim R, Mohona RA, Ferdous MZ, Kamruzzaman S, Toma TY, Sakib MN, Pinky KN, Islam MR, Siddique MAB, Anter FS, Hossain A, Hossen I, Sikder MT, Pontes HM. Problematic smartphone and social media use among Bangladeshi college and university students amid COVID-19: the role of psychological well-being and pandemic related factors. Front Psychiatry. 2021;12:647386. doi: 10.3389/fpsyt.2021.647386. https://europepmc.org/abstract/MED/33935834 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Ding Z, Yan J, Fu J. Internet and Mobile Phone Addiction Self-Control Mediate Physical Exercise and Subjective Well-Being in Young Adults Using IoT. Mob Inf Syst. 2021 May 18;2021:1–6. doi: 10.1155/2021/9923833. https://downloads.hindawi.com/journals/misy/2021/9923833.pdf . [DOI] [Google Scholar]
- 57.Halil T. The risk of physical activity and smart phone addiction in sports high school students: an example of a state school. Pakistan J Medical Health Sci. 2021;15(2):706–11. https://pjmhsonline.com/2021/feb/706.pdf . [Google Scholar]
- 58.Guo K, Ma QS, Yao SJ, Liu C, Hui Z, Jiang J, Lin X. The relationship between physical exercise and mobile phone addiction tendency of university students in China: a moderated mediation model. Front Psychol. 2022;13:730886. doi: 10.3389/fpsyg.2022.730886. https://europepmc.org/abstract/MED/35237204 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Saffari M, Chen J, Wu H, Fung XCC, Chang C, Chang Y, Kamolthip R, Potenza MN, Lin I, Lin C. Effects of weight-related self-stigma and smartphone addiction on female university students' physical activity levels. Int J Environ Res Public Health. 2022 Feb 24;19(5):2631. doi: 10.3390/ijerph19052631. https://europepmc.org/abstract/MED/35270328 .ijerph19052631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Lin B, Teo EW, Yan T. The impact of smartphone addiction on Chinese university students' physical activity: exploring the role of motivation and self-efficacy. Psychol Res Behav Manag. 2022;15:2273–2290. doi: 10.2147/PRBM.S375395. https://europepmc.org/abstract/MED/36039111 .375395 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Chen H, Wang C, Lu T, Tao B, Gao Y, Yan J. The relationship between physical activity and college students' mobile phone addiction: the chain-based mediating role of psychological capital and social adaptation. Int J Environ Res Public Health. 2022 Jul 29;19(15):9286. doi: 10.3390/ijerph19159286. https://europepmc.org/abstract/MED/35954644 .ijerph19159286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Venkatesh E, Al Jemal MY, Samani ASA. Smart phone usage and addiction among dental students in Saudi Arabia: a cross sectional study. Int J Adolesc Med Health. 2017 Apr 06;31(1):20160133. doi: 10.1515/ijamh-2016-0133.ijamh-2016-0133 [DOI] [PubMed] [Google Scholar]
- 63.Xie H, Tao S, Zhang Y, Tao F, Wu X. Impact of problematic mobile phone use and insufficient physical activity on depression symptoms: a college-based follow-up study. BMC Public Health. 2019 Dec 05;19(1):1640. doi: 10.1186/s12889-019-7873-z. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-7873-z .10.1186/s12889-019-7873-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Pereira FS, Bevilacqua GG, Coimbra DR, Andrade A. Impact of problematic smartphone use on mental health of adolescent students: association with mood, symptoms of depression, Cyberpsychol Behav Soc Netw. 2020 Sep;23(9):619–626. doi: 10.1089/cyber.2019.0257. [DOI] [PubMed] [Google Scholar]
- 65.Tao S, Wu X, Yang Y, Tao F. The moderating effect of physical activity in the relation between problematic mobile phone use and depression among university students. J Affect Disord. 2020 Aug 01;273:167–172. doi: 10.1016/j.jad.2020.04.012.S0165-0327(20)30199-3 [DOI] [PubMed] [Google Scholar]
- 66.Zou L, Wu X, Tao S, Yang Y, Zhang Q, Hong X, Xie Y, Li T, Zheng S, Tao F. Neural correlates of physical activity moderate the association between problematic mobile phone use and psychological symptoms. Front Behav Neurosci. 2021;15:749194. doi: 10.3389/fnbeh.2021.749194. https://europepmc.org/abstract/MED/35177970 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Yuan J, Liwei Z, Zhixiong M. Physical exercise and mental health: the effect of emotion regulation self-efficacy and emotion regulation strategy. Studies of Psychology and Behavior. 2018;16(4):570–576. https://psybeh.tjnu.edu.cn/EN/Y2018/V16/I4/570#1 . [Google Scholar]
- 68.Arneklev BJ, Grasmick HG, Tittle CR, Bursik RJ. Low self-control and imprudent behavior. J Quant Criminol. 1993 Sep;9(3):225–247. doi: 10.1007/bf01064461. [DOI] [Google Scholar]
- 69.Yang N, Yang X. Anxiety and depression in graduating university students during the COVID-19 pandemic: a longitudinal study. Am J Transl Res. 2022;14(4):2668–2676. https://europepmc.org/abstract/MED/35559421 . [PMC free article] [PubMed] [Google Scholar]
- 70.Zhang C, Hao J, Liu Y, Cui J, Yu H. Associations between online learning, smartphone addiction problems, and psychological symptoms in Chinese college students after the COVID-19 pandemic. Front Public Health. 2022;10:881074. doi: 10.3389/fpubh.2022.881074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Pinto ADA, Oppong Asante K, Puga Barbosa RMDS, Nahas MV, Dias DT, Pelegrini A. Association between loneliness, physical activity, and participation in physical education among adolescents in Amazonas, Brazil. J Health Psychol. 2021 Apr;26(5):650–658. doi: 10.1177/1359105319833741. [DOI] [PubMed] [Google Scholar]
- 72.Li X, Feng X, Xiao W, Zhou H. Loneliness and mobile phone addiction among Chinese college students: the mediating roles of boredom proneness and self-control. Psychol Res Behav Manag. 2021;14:687–694. doi: 10.2147/PRBM.S315879. https://europepmc.org/abstract/MED/34149289 .315879 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Lancaster MR, Callaghan P. The effect of exercise on resilience, its mediators and moderators, in a general population during the UK COVID-19 pandemic in 2020: a cross-sectional online study. BMC Public Health. 2022 Apr 25;22(1):827. doi: 10.1186/s12889-022-13070-7. https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-022-13070-7 .10.1186/s12889-022-13070-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Li S, Cui G, Yin Y, Tang K, Chen L, Liu X. Prospective association between problematic mobile phone use and eating disorder symptoms and the mediating effect of resilience in Chinese college students: a 1-year longitudinal study. Front Public Health. 2022;10:857246. doi: 10.3389/fpubh.2022.857246. https://europepmc.org/abstract/MED/35570941 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Benarroch EE. Insular cortex: Functional complexity and clinical correlations. Neurology. 2019 Nov 19;93(21):932–938. doi: 10.1212/WNL.0000000000008525.WNL.0000000000008525 [DOI] [PubMed] [Google Scholar]
- 76.Horvath J, Mundinger C, Schmitgen MM, Wolf ND, Sambataro F, Hirjak D, Kubera KM, Koenig J, Christian Wolf R. Structural and functional correlates of smartphone addiction. Addict Behav. 2020 Jun;105:106334. doi: 10.1016/j.addbeh.2020.106334.S0306-4603(19)31380-2 [DOI] [PubMed] [Google Scholar]
- 77.Wrann CD, White JP, Salogiannnis J, Laznik-Bogoslavski D, Wu J, Ma D, Lin JD, Greenberg ME, Spiegelman BM. Exercise induces hippocampal BDNF through a PGC-1α/FNDC5 pathway. Cell Metab. 2013 Nov 05;18(5):649–59. doi: 10.1016/j.cmet.2013.09.008. https://linkinghub.elsevier.com/retrieve/pii/S1550-4131(13)00377-X .S1550-4131(13)00377-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Urdinguio RG, Tejedor JR, Fernández-Sanjurjo Manuel, Pérez Raúl F, Peñarroya Alfonso, Ferrero C, Codina-Martínez Helena, Díez-Planelles Carlos, Pinto-Hernández Paola, Castilla-Silgado J, Coto-Vilcapoma A, Díez-Robles Sergio, Blanco-Agudín Noelia, Tomás-Zapico Cristina, Iglesias-Gutiérrez Eduardo, Fernández-García Benjamín, Fernandez AF, Fraga MF. Physical exercise shapes the mouse brain epigenome. Mol Metab. 2021 Dec;54:101398. doi: 10.1016/j.molmet.2021.101398. https://linkinghub.elsevier.com/retrieve/pii/S2212-8778(21)00256-8 .S2212-8778(21)00256-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Kardefelt-Winther D. A conceptual and methodological critique of internet addiction research: Towards a model of compensatory internet use. Comput Human Behav. 2014 Feb;31:351–354. doi: 10.1016/j.chb.2013.10.059. https://www.sciencedirect.com/science/article/pii/S0747563213004093/pdfft?md5=df0ac813588f363af237dd894ed5d722&pid=1-s2.0-S0747563213004093-main.pdf . [DOI] [Google Scholar]
- 80.GebreEyesus FA, Tarekegn TT, Amlak BT, Shiferaw BZ, Emeria MS, Geleta OT, Terefe TF, Mammo Tadereregew M, Jimma MS, Degu FS, Abdisa EN, Eshetu MA, Misganaw NM, Chanie ES. Levels and predictors of anxiety, depression, and stress during COVID-19 pandemic among frontline healthcare providers in Gurage zonal public hospitals, Southwest Ethiopia, 2020: A multicenter cross-sectional study. PLoS One. 2021;16(11):e0259906. doi: 10.1371/journal.pone.0259906. https://dx.plos.org/10.1371/journal.pone.0259906 .PONE-D-21-20584 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Tison GH, Avram R, Kuhar P, Abreau S, Marcus GM, Pletcher MJ, Olgin JE. Worldwide effect of COVID-19 on physical activity: a descriptive study. Ann Intern Med. 2020 Nov 03;173(9):767–770. doi: 10.7326/M20-2665. https://www.acpjournals.org/doi/abs/10.7326/M20-2665?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Rodríguez-Larrad Ana, Mañas Asier, Labayen I, González-Gross Marcela, Espin A, Aznar S, Serrano-Sánchez José Antonio, Vera-Garcia FJ, González-Lamuño Domingo, Ara I, Carrasco-Páez Luis, Castro-Piñero José, Gómez-Cabrera Mari Carmen, Márquez Sara, Tur JA, Gusi N, Benito PJ, Moliner-Urdiales D, Ruiz JR, Ortega FB, Jiménez-Pavón David, Casajús José Antonio, Irazusta J. Impact of COVID-19 confinement on physical activity and sedentary behaviour in Spanish university students: role of gender. Int J Environ Res Public Health. 2021 Jan 06;18(2):369. doi: 10.3390/ijerph18020369. https://europepmc.org/abstract/MED/33418907 .ijerph18020369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Alavi SS, Ghanizadeh M, Mohammadi MR, Mohammadi Kalhory S, Jannatifard F, Sepahbodi G. The survey of personal and national identity on cell phone addicts and non-addicts. Iran J Psychiatry. 2018 Jan;13(1):15–21. https://europepmc.org/abstract/MED/29892313 . [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Detailed search strategy.
Details of the scoring criteria in the JBI appraisal checklist. JBI: Joanna Briggs Institute.
Full details of coding forms for the subgroups.