

The state of cancer research and care is the result of the effort and contributions of the pioneers who established the discipline of oncology and the many thought leaders who followed. Many of them preceded me on this podium as Karnofsky lecturers.
Much progress was made over the past five decades, resulting in significant reductions in cancer mortality in general, and breast cancer mortality in particular.1 It is an enormous privilege to have been in cancer research during these times, when arguably more progress was made than in the previous many centuries. Let me take you through the journey I and my colleagues took over these decades, and summarize where we came from, where we are today, and where we must go to continue progress in research and improve care of our patients.
By the time I started my career in oncology, surgery and radiation therapy were mature disciplines, while medical oncology was a young specialty with much promise but relatively few accomplishments (Fig 1). The war on cancer was just 3 years old.2
FIG 1.
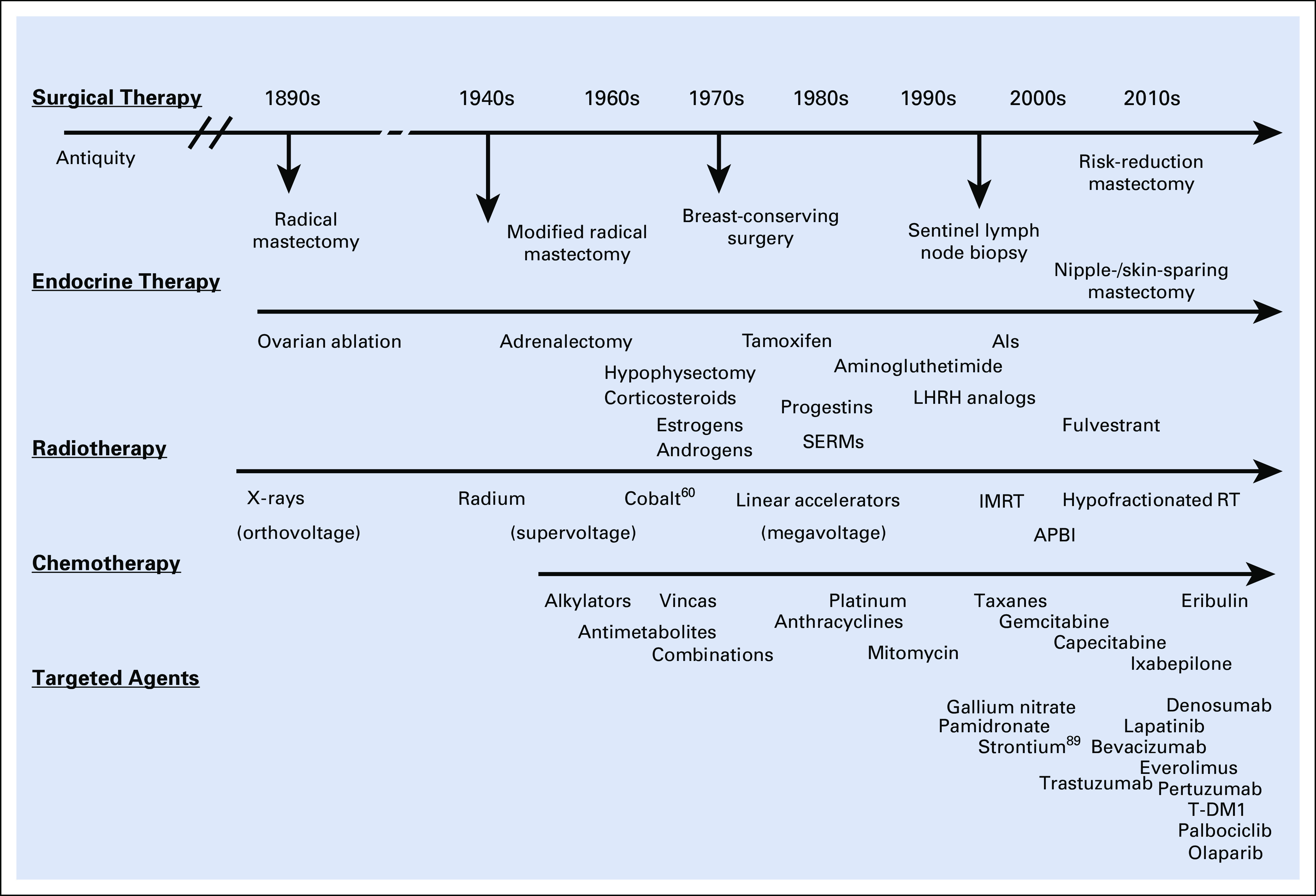
History of breast cancer treatment: Timeline. Integration of various discoveries that led to changes in the standard of care. Discoveries are displayed by approximate year of incorporation into practice. AI, aromatase inhibitor; APBI, accelerated partial breast irradiation; IMRT, intensity-modulated radiotherapy; LHRH, luteinizing hormone-releasing hormone; RT, radiotherapy; SERM, selective estrogen receptor modulator; T-DM1, trastuzumab emtansine.
Our understanding of the biology of breast cancer was primitive, and we had few tools to manage it. Detection was made by palpation. The diagnosis was made by an incisional or excisional biopsy, and often patients went to surgery for a biopsy and woke up having had a mastectomy. Radical mastectomy was king, as it had been for the previous 70 years.3 While new radiotherapy technology was in progress, the standard was the Cobalt 60 machine. Endocrine therapy was largely based on major ablative procedures, which, although effective, had lifetime consequences for the patients.4 Chemotherapy was in its infancy, with few drugs available to the clinician.5
The dominant research themes focused on the development of new drugs. The National Cancer Institute had a massive screening program that tested tens of thousands of compounds of diverse origins on various in vitro models in the absence of a clear understanding of molecular targets.6 Clinical pharmacology and permutations of dose and schedule guided clinical trials. There was much hope in developing immunotherapy, but our rudimentary understanding of the immune system condemned early efforts to failure.7 Cell lines and experimental animals were developed to explore mechanistic concepts, as well as sensitivity and resistance to emerging therapies. Relda Cailleau, in my department, developed more than 20 breast cancer cell lines, the MDA-MB series, which is still in widespread use today.8 The concept of familial or hereditary disposition was starting to be appreciated based on the work of Lynch,9 Anderson,10 and others, and the earliest steps in identifying therapeutic targets led to the identification of the estrogen receptor.11
Over the past five decades, major progress in breast cancer research transformed the standard of care. Some advances resulted in significant improvements in survival and reductions in mortality, while others led to enhanced quality of life (Table 1).
TABLE 1.
Advances in Breast Cancer Management and Research Between the 1970s and the Present
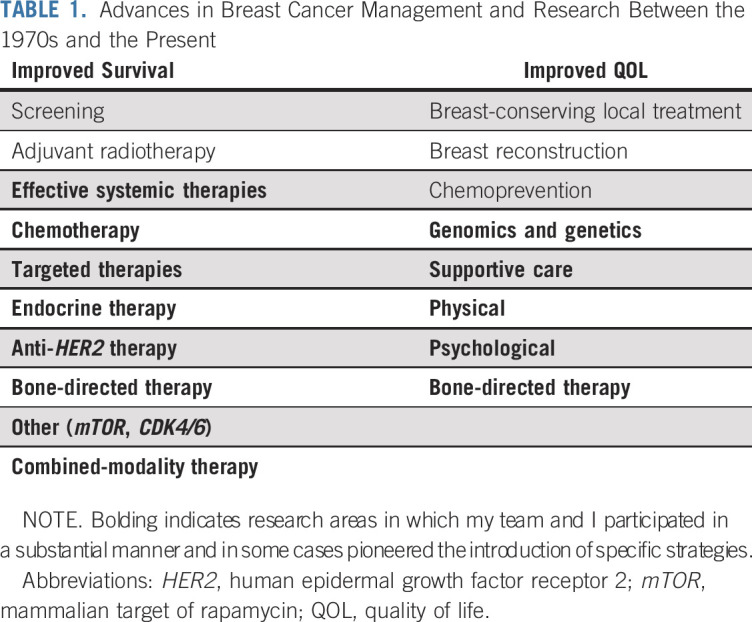
My team and I participated in a substantial manner in the research areas highlighted in bold, and in some cases pioneered the introduction of specific strategies. Our early emphasis on patient-centered care transformed the interaction between specialties and led to the redesigning of our clinical infrastructure.12
In the area of systemic therapy, our team contributed to the development of anthracyclines,13 taxanes,14,15 capecitabine,16 and aromatase inhibitors.17 We initiated combined modality therapy based on neoadjuvant chemotherapy in 1974 and established it as the new standard of care for patients with locally advanced and inflammatory breast cancer.12,18 Our interest in bone metastases guided our work with bisphosphonates, which resulted in the incorporation of these agents in the management of metastatic disease.19 We also contributed to the early development of gene expression technology and the early steps in targeted and gene therapies.20,21 On the organizational side, I contributed to the establishment of research nurse and midlevel practitioner programs at my institution, and worked with the state legislature to create the appropriate regulatory environment for these programs. Early on, we established multidisciplinary planning clinics several times per week, and this interaction eventually led to the development of shared, patient-centered breast care, research programs, and clinic space.
The early steps in the development of breast cancer chemotherapy were tentative, and required the courageous and persistent efforts of a group of pioneers. It took more than 20 years for combination chemotherapy to be adapted in standard practice. The introduction of anthracyclines gave added optimism to breast oncology, and hope and hype followed the introduction of dose intensity–based regimens.
The greatest success of chemotherapy followed its introduction in the adjuvant setting. Based on impeccable preclinical investigations, Fisher22 and Bonadonna23 electrified the community with the presentation of the initial clinical trial results. The two pioneering publications represented the first evidence that chemotherapy could improve the cure rate of a common human solid tumor and encouraged the development of multiple prospective clinical trials. These early trials explored fundamental questions and led to the development of well-powered and better-designed definitive randomized trials.
Perhaps less noticed was the simultaneous development of the concept of potentially curative combined-modality treatment of patients with metastatic breast cancer and limited metastatic burden, who could be rendered clinically disease free with local therapy and treated with systemic therapy either before or after such local treatment. We labeled this group stage IV, no evident disease or NED, and demonstrated over the next several decades that 25% to 50% of them would remain without additional recurrences or metastases for extended periods, exceeding 20 years.24 This clinical situation was renamed oligometastases by Hellman and colleagues,25 some 15 years later. Today, there is much enthusiasm for completing definitive clinical trials in these patients, with the availability of more effective systemic therapy and more precise and less invasive local treatments.
We initiated clinical trials of neoadjuvant chemotherapy for locally advanced breast cancers in 1974.12,18 This strategy, which paralleled the introduction of adjuvant chemotherapy, took much longer to be adopted by the breast cancer community, but today is a standard of care for larger tumors, especially of the HER2 (human epidermal growth factor receptor 2) -positive and triple-negative subsets. It also became a favored strategy for drug evaluation and biologic exploration.
The 1980s were lean years for new drug development. We evaluated many candidates, but no new drug was approved for breast cancer; however, important technological progress occurred in imaging, diagnostic biopsies, and radiation therapy (Fig 1). Based on preclinical experiments, the Halstedian dogma was challenged and there was a gradual departure from the radical mastectomy toward the two-step diagnostic strategy.26 Patients would no longer wake up from anesthesia wondering whether they had lost the breast or not. Adjuvant systemic therapies were broadly and rapidly adopted for intermediate- to high-risk patients.
The same decade witnessed important improvements in supportive care. Central venous catheters27 and infusion pumps28 became standard, and effective antiemetics and analgesics improved symptom control.29 Bone-directed therapies improved control of hypercalcemia and transformed the clinical course of bone metastases.19 Collection, preservation, and reinfusion of autologous bone marrow30—and later peripheral stem cells31—removed barriers to dose intensification, while growth factor support dramatically reduced infectious complications of chemotherapy.32
Breast cancer research also evolved toward molecular biology. The development of preclinical models facilitated prehuman experimentation. The metastatic process and the cell cycle became targets of intense investigation, and the realization that genes contributed to susceptibility, as well as malignant behavior, led the way to karyotyping cancer cells and studying putative cancer genes, such as EGFR, HER2, and c-MYC, among others.
In the early 1980s, the Oxford Statistical group pioneered the technique of meta-analysis.33 The Early Breast Cancer Trialists Collaborative Group collected patient-based information of hundreds of randomized trials, including hundreds of thousands of patients, and performed analyses that led to definitive answers for a number of critically important clinical questions related to breast cancer surgery, radiotherapy, chemotherapy, and endocrine therapy.33 These analyses transformed the standards of care for patients with breast cancer around the world.
The initial attempts of adjuvant endocrine therapy used ovarian ablation or tamoxifen in a series of small, underpowered clinical trials that provided mixed answers. Eventually, better-designed trials, as well as meta-analyses, led to definitive conclusions about the value of these interventions, including a significant prolongation of overall survival.34
A summary of these pooled clinical trials indicated that adjuvant tamoxifen given for 5 years resulted in a 12.6% absolute reduction in recurrences, while ovarian ablation resulted in a similar 20-year reduction in recurrences.34 Two decades later, the modest superiority of aromatase inhibitors over tamoxifen would be established with the same methodology.35
The field was now poised to demonstrate population-based improvements in the length and quality of life of our patients.
The decade of the 1990s was certainly more rewarding and we harvested the results of the substantial investments in research during the previous two decades (Fig 1). We started with the rapid clinical development of the taxanes, arguably the most effective cytotoxic agents against breast cancer, and their incorporation into adjuvant therapy.14,15 We also generated level I evidence of the important role of bisphosphonates in the management of metastatic breast cancer to bone, hypercalcemia, and the prevention and management of osteoporosis.19,36 Almost unnoticed, capecitabine completed clinical trials and received regulatory approval.16
Molecular biologists identified a number of oncogenes, tumor suppressor genes, and tentative molecular targets in the 1980s. Among the targets, EGFR became a prototype.37 John Mendelsohn and colleagues38 developed a therapeutic strategy based on a humanized monoclonal antibody directed against EGFR. It eventually became an US Food and Drug Administration–approved drug, cetuximab, still in use today.39 Based on this work—and preclinical and clinical work performed on HER2 by Dennis Slamon,40 Mark Green, and Bob Weinberg’s group—HER2-directed antibodies were developed by Genentech scientists and taken to clinical trials.41 The anti-HER2 antibody trastuzumab completed randomized clinical trials in metastatic breast cancer, demonstrating a favorable effect on overall survival.42 This led to randomized trials in the adjuvant setting (Table 2). The 30% to 40% relative reduction in odds of recurrence translated into a 6.0 to 6.8 absolute benefit in terms of recurrence and a 6.5% to 6.6% reduction in 10-year mortality.43,44
TABLE 2.
Adjuvant Trastuzumab Trials: Disease-Free and Overall Survival—Summary of Pivotal Trials

In parallel to the development of the taxanes and trastuzumab, our group completed two pivotal trials for the aminobisphosphonate pamidronate combined with chemotherapy or endocrine therapy in patients with metastatic breast cancer to the bony skeleton.19,45 The highly significant reduction in skeletal-related events and skeletal morbidity, and a significant prolongation in time to next skeletal complication led to rapid US Food and Drug Administration approval of pamidronate, which became an integral part of the treatment of bone metastases.
These events take us to the origins of the concept of personalized breast oncology. In the early 1990s, we partnered with Millennium Diagnostics to develop clinical applications for gene expression profiling.21 We validated the technology, its clinical and analytical accuracy, and reproducibility, and initiated a number of clinically relevant studies. The ability to simultaneously assess the expression level of thousands of genes was quite attractive to us, and remains so 25 years later.
We were able to correlate the expression of specific groups of genes with outcomes, and using hierarchical clustering were able to classify breast cancer into various molecularly defined subgroups.20,46 Further developed and refined by other groups,47 this technology led to the development of various genomic profiles in use today to classify patients into various prognostic groups and assist the clinician with the selection of optimal therapies.48,49
While my comments focused on systemic therapies, much was changing in surgery and radiation therapy. Both disciplines undertook concerted efforts to tailor treatment to risk and, more recently, biologic characteristics. The result was the downsizing of surgical interventions to breast-conserving surgery and sentinel lymph node biopsy, and alteration of radiation therapy to hypofractionated schedules as well as accelerated partial breast irradiation.
The timeline now reached the year 2000, and our tools included sentinel lymph node biopsy, aromatase inhibitors, fulvestrant, intensity-modulated radiation therapy, APBI, capecitabine and aminobisphosphonates.
The dominant event at the beginning of the new millennium was the completion of the Human Genome Project, a visionary enterprise with amazing results.50,51 This project, the result of the work of hundreds of scientists in North America and around the world, provided a wealth of new information as well as a variety of technological advancements that continue to feed biologic research today.
Of immediate relevance to breast cancer, our ability to classify breast cancer according to molecular profiles allowed us to modify our conceptual framework of the disease.47 Breast cancer is a conglomerate of multiple molecularly defined syndromes that originate in the same organ. The various molecular subsets have different clinical behaviors, metastatic patterns, and sensitivity to existing therapies.
Gene expression can be paired with other -omics and moved from static observations to mechanistic views of pathways and, eventually, systems biology. This leads to better understanding of biologically dominant processes, identification of driver molecular events, and validation of molecular therapeutic targets.
The timeline now takes us to the present (Fig 1). Modern surgery, radiotherapy, chemotherapy, and endocrine therapy have clearly had a major impact on breast cancer mortality and quality of life. We are now poised to take the next step toward personalized medicine.
There is broad recognition and acceptance of the molecular subtypes described by Sørlie et al.47 While gene expression profiling is not widely available in clinical practice, surrogate biomarkers allow us to identify clinical subsets that correspond largely, although not completely, to this classification. These subsets benefit from different interventions, so the classification also serves to select optimal therapy. Within each subset, molecular markers might identify even more discrete therapeutic subsets. As an example, the Vanderbilt group identified a few years ago six distinct categories of triple-negative breast cancer.52 Characterization of these categories and identification of the optimal treatment of these categories is still in progress.
Since molecular characterization of breast cancers opens the door to personalized therapy, I’d like to expand on an area of science that has occupied my research efforts for the past decade. Endocrine therapy has been the backbone of breast cancer treatment of the past several decades and my group has published extensively on this topic. Serial biopsies of hormone receptor–positive breast cancers evidenced the molecular anomalies that exist at the time of diagnosis and the changes that take place during the development of clinically evident metastases. They also show the molecular effects of treatment, suggesting potential mechanisms of resistance.
The Human Genome Project and Translational Studies associated with large clinical trials demonstrated a number of genomic anomalies found in various breast cancer subtypes. The most common molecular anomaly for Luminal A and B subtypes is a PIK3CA mutation, present in 45% and 29% of cases, respectively, followed in order of frequency by mutations in p53, amplifications of cyclin D1 and FGFR1, and a number of less frequent anomalies. These findings provided the rationale for targeting the PI3K pathway.
Our first strategy, based on these genomic observations and the availability of mammalian target of rapamycin inhibitors, was to combine everolimus with an aromatase inhibitor. The BOLERO-2 trial, which I co-led with Jose Baselga, was a randomized trial in patients with aromatase inhibitor–resistant metastatic breast cancer. All patients received exemestane and were randomly assigned to everolimus or placebo. The study met its primary end point, with a hazard ratio of 0.43 for progression-free survival, indicating the major therapeutic impact of everolimus.53 This combination gained regulatory approval and is part of our standard of care today. Subsequent trials targeted PI3K, leading to the approval of alpelisib.54
Our next strategy was to incorporate a CDK4/6 inhibitor, in this case ribociclib, into first-line endocrine therapy, based on cyclin D1 amplification and proliferation being a prominent contributor to resistance to endocrine therapy. Ribociclib combined with an aromatase inhibitor resulted in an almost doubling of the median time to progression (hazard ratio, 0.58) and improvement in overall response rate and clinical benefit rate.55
Table 3 summarizes the highly reproducible effect of the available CDK4/6 inhibitors in metastatic breast cancer. These results were transformative and altered the standard of care for metastatic, hormone receptor–positive breast cancer. These same agents are currently being tested in the adjuvant setting.
TABLE 3.
Randomized Trials With CDK4/6 Inhibitors in First-Line Metastatic, Hormone Receptor–Positive Breast Cancer

As a result of scientific progress, the landscape of breast cancer management has changed dramatically. Figure 2 summarizes our current standard of care by clinical subtype. No doubt, this algorithm will continue to evolve.
FIG 2.

Systemic management of primary breast cancer. The four generally accepted clinical-molecular subtypes are shown, along with standard-of-care therapeutic approaches to each subtype. AI, aromatase inhibitor; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; RS, recurrence score; SERM, selective estrogen receptor modulator.
Similarly, clinical and molecular subtypes guide our approach to systemic therapy of primary breast cancer. It is in this setting that our discoveries in the metastatic setting carry the biggest effect, transforming improvements in palliation into enhanced cure rates.
I will use the population-based observations made yearly by the National Cancer Institute and the American Cancer Society to summarize the effects of the scientific progress we have made over the past five decades. Table 3 shows the changes in relative survival over the past 46 years, representing my career in medical oncology1,56 (Fig 3). The numerical changes are clear and represent significant relative and absolute improvement in outcomes in localized, regional, and distant breast cancer.
FIG 3.

Five-year relative survival rates for breast cancer: 1973-2019. Numbers represent 5-year relative survival figures. The change between 1973 and 2019 reflects the progress in detection and treatment. Data are given as percent 5-year survival.
On a population-based estimation, this translates into a 35% reduction in breast cancer mortality in the United States between 1984 and 2014,57 and similar reductions have been reported from other industrialized nations. In view of the marked disparities in access to modern technology and therapeutic agents, one can only speculate how many additional lives could be saved if currently existing knowledge were applied evenly across the globe.
Just as important as improved length of life and cure rates, the progress in quality of life has been quite prominent (Table 4). Symptom control made disease and its treatment more tolerable and enhanced compliance with therapy. Growth factor use reduced the frequency of severe complications, and the introduction of bone-directed therapies reduced skeletal-related events.
TABLE 4.
Improved Quality of Life
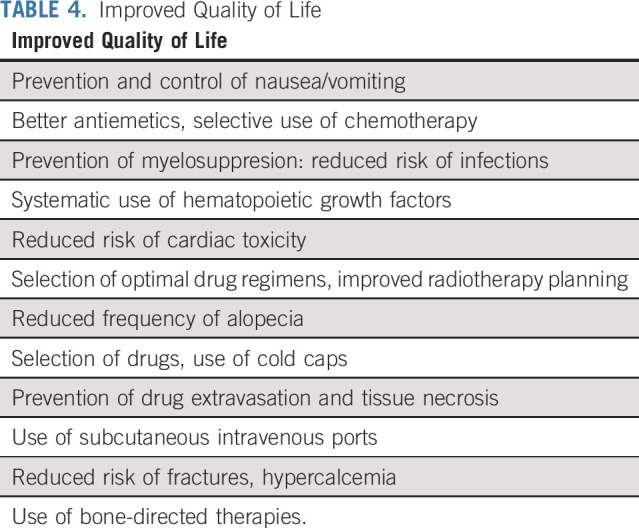
Table 5 shows a rapidly growing and probably incomplete list of molecular anomalies associated with breast cancer and representing potential therapeutic targets. Listing them is easier that validating them and demonstrating that relevant targeted therapies will provide incremental clinical benefit. The even faster growing list of targeted therapeutic agents indicates our conviction that we are on the right track. Those involved in the clinical trials enterprise understand that this will take much effort, time, and a major commitment of resources.
TABLE 5.
Genomic Aberrations in Breast Cancer That Guide Precision Medicine

There is much ongoing research in the fields of breast surgery and radiotherapy, but time prevents me from reviewing those efforts.
My colleague, Jim Allison, recently stated that research success is largely incremental and what we have today is the result of the work of thousands of investigators and the participation of hundreds of thousands of courageous patients who participated in hundreds of clinical trials.
I will also quote Arti Hurria, a bright light we lost in the prime of her life last year: “If you want to go fast, go alone, but if you want to go far, go together.” This clearly applies to breast cancer research, where team science is the key to success.
I’ll borrow Newton’s words: If I have seen further it is by standing upon the shoulders of giants. Many creative colleagues preceded me and many will follow and contribute to progress in our field and the betterment of our patients’ outcomes.
I am privileged to have worked in one of the greatest cancer research institutions in the world. I am much indebted to my colleagues and mentors for the opportunities I had to contribute to progress. They taught me, guided me, and opened doors for me. I am thankful to all of them.
Our work was supported over the years by a number of agencies, foundations, and companies. Philanthropy also played a major role and the progress we made would not have been possible without it.
My parents remain my greatest role models. They taught me the value of curiosity, persistence, hard work, and respect.
Finally, it is thanks to my wonderful family that I stand before you. The loving and continued support of my wife, Agnes, our three daughters and our 7 grandchildren were a critical ingredient to my success and my ability to dedicate much time and effort to my professional interests.
Thank you, Dr Johnson, for the very kind introduction. Also, my thanks to the ASCO Special Awards Selection Committee for my selection as the 2019 Karnofsky lecturer. I am deeply honored and humbled by the decision of my peers.
Thanks again to the ASCO Special Award selection committee for this amazing recognition, and thank you for listening.
Supplementary Material
{kind=link}
Footnotes
Presented as the 51st David A. Karnofsky Memorial Lecture at the 2019 American Society of Clinical Oncology Annual Meeting, Chicago, IL, June 1, 2019.
AUTHOR’S DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Breast Cancer: 45 Years of Research and Progress
The following represents disclosure information provided by the author of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Gabriel N. Hortobagyi
Consulting or Advisory Role: Novartis, Peregrine Pharmaceuticals, Agendia
Research Funding: Novartis (Inst)
Travel, Accommodations, Expenses: Novartis
No other potential conflicts of interest were reported.
REFERENCES
- 1.Siegel RL, Miller KD, Jemal A: Cancer statistics, 2019. CA Cancer J Clin 69:7-34, 2019 [DOI] [PubMed] [Google Scholar]
- 2.National Cancer Institute : National Cancer Act of 1971. https://dtp.cancer.gov/timeline/flash/milestones/M4_Nixon.htm
- 3.Fisher B, Wolmark N: New concepts in the management of primary breast cancer. Cancer 36:627-632, 1975. (suppl) [DOI] [PubMed] [Google Scholar]
- 4.Welbourn RB, Burn JI: Treatment of advanced mammary cancer. N Engl J Med 287:398-400, 1972 [DOI] [PubMed] [Google Scholar]
- 5.Carter SK: The chemical therapy of breast cancer. Semin Oncol 1:131-144, 1974 [PubMed] [Google Scholar]
- 6.Driscoll JS: The preclinical new drug research program of the National Cancer Institute. Cancer Treat Rep 68:63-76, 1984 [PubMed] [Google Scholar]
- 7.Mastrangelo MJ, Berd D, Bellet RE: Critical review of previously reported clinical trials of cancer immunotherapy with nonspecific immunostimulants. Ann N Y Acad Sci 277:94-123, 1976 [DOI] [PubMed] [Google Scholar]
- 8.Cailleau R, Olivé M, Cruciger QV: Long-term human breast carcinoma cell lines of metastatic origin: Preliminary characterization. In Vitro 14:911-915, 1978 [DOI] [PubMed] [Google Scholar]
- 9.Lynch HT, Guirgis HA, Albert S, et al. : Familial association of carcinoma of the breast and ovary. Surg Gynecol Obstet 138:717-724, 1974 [PubMed] [Google Scholar]
- 10.Anderson DE: Genetic study of breast cancer: Identification of a high risk group. Cancer 34:1090-1097, 1974 [DOI] [PubMed] [Google Scholar]
- 11.Jensen EV, De Sombre ER: Oestrogen-receptor interaction in target tissues. Biochem J 115:28P-29P, 1969 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Buzdar AU, Montague ED, Barker JL, et al. : Management of inflammatory carcinoma of breast with combined modality approach: An update. Cancer 47:2537-2542, 1981 [DOI] [PubMed] [Google Scholar]
- 13.Gottlieb JA, Rivkin SE, Spigel SC, et al. : Proceedings: Superiority of adriamycin over oral nitrosoureas in patients with advanced breast carcinoma. A Southwest Cancer Chemotherapy Study Group study. Cancer 33:519-526, 1974 [DOI] [PubMed] [Google Scholar]
- 14.Holmes FA, Walters RS, Theriault RL, et al. : Phase II trial of taxol, an active drug in the treatment of metastatic breast cancer. J Natl Cancer Inst 83:1797-1805, 1991 [DOI] [PubMed] [Google Scholar]
- 15.Valero V, Holmes FA, Walters RS, et al. : Phase II trial of docetaxel: A new, highly effective antineoplastic agent in the management of patients with anthracycline-resistant metastatic breast cancer. J Clin Oncol 13:2886-2894, 1995 [DOI] [PubMed] [Google Scholar]
- 16.Blum JL, Jones SE, Buzdar AU, et al. : Multicenter phase II study of capecitabine in paclitaxel-refractory metastatic breast cancer. J Clin Oncol 17:485-493, 1999 [DOI] [PubMed] [Google Scholar]
- 17.Buzdar A, Jonat W, Howell A, et al. : Anastrozole, a potent and selective aromatase inhibitor, versus megestrol acetate in postmenopausal women with advanced breast cancer: Results of overview analysis of two phase III trials. J Clin Oncol 14:2000-2011, 1996 [DOI] [PubMed] [Google Scholar]
- 18.Hortobagyi GN, Blumenschein GR, Spanos W, et al. : Multimodal treatment of locoregionally advanced breast cancer. Cancer 51:763-768, 1983 [DOI] [PubMed] [Google Scholar]
- 19.Hortobagyi GN, Theriault RL, Porter L, et al. : Efficacy of pamidronate in reducing skeletal complications in patients with breast cancer and lytic bone metastases. Protocol 19 Aredia Breast Cancer Study Group. N Engl J Med 335:1785-1791, 1996 [DOI] [PubMed] [Google Scholar]
- 20.Buchholz TA, Stivers DN, Stec J, et al. : Global gene expression changes during neoadjuvant chemotherapy for human breast cancer. Cancer J 8:461-468, 2002 [DOI] [PubMed] [Google Scholar]
- 21.Symmans WF, Ayers M, Clark EA, et al. : Total RNA yield and microarray gene expression profiles from fine-needle aspiration biopsy and core-needle biopsy samples of breast carcinoma. Cancer 97:2960-2971, 2003 [DOI] [PubMed] [Google Scholar]
- 22.Fisher B, Carbone P, Economou SG, et al. : L-Phenylalanine mustard (L-PAM) in the management of primary breast cancer. A report of early findings. N Engl J Med 292:117-122, 1975 [DOI] [PubMed] [Google Scholar]
- 23.Bonadonna G, Brusamolino E, Valagussa P, et al. : Combination chemotherapy as an adjuvant treatment in operable breast cancer. N Engl J Med 294:405-410, 1976 [DOI] [PubMed] [Google Scholar]
- 24.Buzdar AU, Blumenschein GR, Smith TL, et al. : Adjuvant chemoimmunotherapy following regional therapy for isolated recurrences of breast cancer (stage IV NED). J Surg Oncol 12:27-40, 1979 [DOI] [PubMed] [Google Scholar]
- 25.Hellman S, Weichselbaum RR: Oligometastases. J Clin Oncol 13:8-10, 1995 [DOI] [PubMed] [Google Scholar]
- 26.Fisher B, Bauer M, Margolese R, et al. : Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med 312:665-673, 1985 [DOI] [PubMed] [Google Scholar]
- 27.Daly JM, Lawson M, Speir A, et al. : Angioaccess in cancer patients. Curr Probl Cancer 5:1-37, 1981 [DOI] [PubMed] [Google Scholar]
- 28.Plasse T, Ohnuma T, Bruckner H, et al. : Portable infusion pumps in ambulatory cancer chemotherapy. Cancer 50:27-31, 1982 [DOI] [PubMed] [Google Scholar]
- 29.Cunningham D, Hawthorn J, Pople A, et al. : Prevention of emesis in patients receiving cytotoxic drugs by GR38032F, a selective 5-HT3 receptor antagonist. Lancet 1:1461-1463, 1987 [DOI] [PubMed] [Google Scholar]
- 30.Dicke KA, Vellekoop L, Spitzer G, et al. : Autologous bone marrow transplantation in neoplasia. Transplant Proc 13:267-269, 1981 [PubMed] [Google Scholar]
- 31.Kessinger A, Armitage JO, Landmark JD, et al. : Autologous peripheral hematopoietic stem cell transplantation restores hematopoietic function following marrow ablative therapy. Blood 71:723-727, 1988 [PubMed] [Google Scholar]
- 32.American Society of Clinical Oncology : Recommendations for the use of hematopoietic colony-stimulating factors: Evidence-based, clinical practice guidelines. J Clin Oncol 12:2471-2508, 1994 [DOI] [PubMed] [Google Scholar]
- 33.Early Breast Cancer Trialists’ Collaborative Group : Effects of adjuvant tamoxifen and of cytotoxic therapy on mortality in early breast cancer. An overview of 61 randomized trials among 28,896 women. N Engl J Med 319:1681-1692, 1988 [DOI] [PubMed] [Google Scholar]
- 34.Early Breast Cancer Trialists’ Collaborative Group : Tamoxifen for early breast cancer: An overview of the randomised trials. Lancet 351:1451-1467, 1998 [PubMed] [Google Scholar]
- 35.Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) : Aromatase inhibitors versus tamoxifen in early breast cancer: Patient-level meta-analysis of the randomised trials. Lancet 386:1341-1352, 2015 [DOI] [PubMed] [Google Scholar]
- 36.[No authors listed]: Osteoporosis prevention, diagnosis, and therapy. NIH Consens Statement 17:1-45, 2000 [PubMed] [Google Scholar]
- 37.Das M, Miyakawa T, Fox CF, et al. : Specific radiolabeling of a cell surface receptor for epidermal growth factor. Proc Natl Acad Sci USA 74:2790-2794, 1977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kawamoto T, Sato JD, Le A, et al. : Growth stimulation of A431 cells by epidermal growth factor: Identification of high-affinity receptors for epidermal growth factor by an anti-receptor monoclonal antibody. Proc Natl Acad Sci USA 80:1337-1341, 1983 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Frieze DA, McCune JS: Current status of cetuximab for the treatment of patients with solid tumors. Ann Pharmacother 40:241-250, 2006 [DOI] [PubMed] [Google Scholar]
- 40.Slamon DJ, Clark GM, Wong SG, et al. : Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 235:177-182, 1987 [DOI] [PubMed] [Google Scholar]
- 41.Pegram MD, Lipton A, Hayes DF, et al. : Phase II study of receptor-enhanced chemosensitivity using recombinant humanized anti-p185HER2/neu monoclonal antibody plus cisplatin in patients with HER2/neu-overexpressing metastatic breast cancer refractory to chemotherapy treatment. J Clin Oncol 16:2659-2671, 1998 [DOI] [PubMed] [Google Scholar]
- 42.Slamon DJ, Leyland-Jones B, Shak S, et al. : Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 344:783-792, 2001 [DOI] [PubMed] [Google Scholar]
- 43.Lambertini M, Pondé NF, Solinas C, et al. : Adjuvant trastuzumab: A 10-year overview of its benefit. Expert Rev Anticancer Ther 17:61-74, 2017 [DOI] [PubMed] [Google Scholar]
- 44.Hortobagyi GN: Trastuzumab in the treatment of breast cancer. N Engl J Med 353:1734-1736, 2005 [DOI] [PubMed] [Google Scholar]
- 45.Theriault RL, Lipton A, Hortobagyi GN, et al. : Pamidronate reduces skeletal morbidity in women with advanced breast cancer and lytic bone lesions: A randomized, placebo-controlled trial. Protocol 18 Aredia Breast Cancer Study Group. J Clin Oncol 17:846-854, 1999 [DOI] [PubMed] [Google Scholar]
- 46.Pusztai L, Ayers M, Stec J, et al. : Gene expression profiles obtained from fine needle aspirations of breast cancer reliably identify routine prognostic markers and reveal large-scale molecular differences between estrogen-negative and estrogen-positive tumors. Clin Cancer Res 9:2406-2415, 2003 [PubMed] [Google Scholar]
- 47.Sørlie T, Perou CM, Tibshirani R, et al. : Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA 98:10869-10874, 2001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Paik S, Shak S, Tang G, et al. : A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med 351:2817-2826, 2004 [DOI] [PubMed] [Google Scholar]
- 49.van de Vijver MJ, He YD, van’t Veer LJ, et al. : A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med 347:1999-2009, 2002 [DOI] [PubMed] [Google Scholar]
- 50.Venter JC, Adams MD, Myers EW, et al. : The sequence of the human genome. Science 291:1304-1351, 2001 [DOI] [PubMed] [Google Scholar]
- 51.Lander ES, Linton LM, Birren B, et al. : Initial sequencing and analysis of the human genome. Nature 409:860-921, 2001. [Errata: Nature 412:565, 2001; Nature 411:720, 2001] [DOI] [PubMed] [Google Scholar]
- 52.Lehmann BD, Bauer JA, Chen X, et al. : Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Invest 121:2750-2767, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Baselga J, Campone M, Piccart M, et al. : Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med 366:520-529, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.André F, Ciruelos E, Rubovszky G, et al. : Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced breast cancer. N Engl J Med 380:1929-1940, 2019 [DOI] [PubMed] [Google Scholar]
- 55.Hortobagyi GN, Stemmer SM, Burris HA, et al. : Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med 375:1738-1748, 2016 [DOI] [PubMed] [Google Scholar]
- 56.Silverberg E, Holleb AI: Cancer statistics 1973. CA Cancer J Clin 23:1-27, 1973 [PubMed] [Google Scholar]
- 57.Office on Women’s Health : Decrease in breast cancer deaths. https://www.womenshealth.gov/30-achievements/07
- 58.Perez EA, Romond EH, Suman VJ, et al. : Trastuzumab plus adjuvant chemotherapy for human epidermal growth factor receptor 2-positive breast cancer: Planned joint analysis of overall survival from NSABP B-31 and NCCTG N9831. J Clin Oncol 32:3744-3752, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. : Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med 353:1659-1672, 2005 [DOI] [PubMed] [Google Scholar]
- 60.Slamon DJ, Eiermann W, Robert NJ, et al. : Ten-year follow-up of the BCIRG-006 trial comparing doxorubicin plus cyclophosphamide followed by docetaxel (ACT) with doxorubicin plus cyclophosphamide followed by docetaxel and trastuzumab (ACTH) with docetaxel, carboplatin and trastuzumab (TCH) in HER2+ early breast cancer patients. Cancer Res 76, 2016. (suppl 4; abstr S5–04) [Google Scholar]
- 61.Joensuu H, Bono P, Kataja V, et al. : Fluorouracil, epirubicin, and cyclophosphamide with either docetaxel or vinorelbine, with or without trastuzumab, as adjuvant treatments of breast cancer: Final results of the FinHer trial. J Clin Oncol 27:5685-5692, 2009 [DOI] [PubMed] [Google Scholar]
- 62.Spielmann M, Roché H, Delozier T, et al. : Trastuzumab for patients with axillary-node-positive breast cancer: Results of the FNCLCC-PACS 04 trial. J Clin Oncol 27:6129-6134, 2009 [DOI] [PubMed] [Google Scholar]
- 63.Finn RS, et al. : Lancet Oncol 16:25-35, 2015 [DOI] [PubMed] [Google Scholar]
- 64.Finn RS, et al. : N Engl J Med 375:1925-1936, 2016 [DOI] [PubMed] [Google Scholar]
- 65.Hortobagyi GN, et al. : N Engl J Med 375:1738-1748, 2016 [DOI] [PubMed] [Google Scholar]
- 66.Slamon DJ, Neven P, Chia S, et al. : Overall survival with ribociclib plus fulvestrant in advanced breast cancer. N Engl J Med 382:514-524, 2020 [DOI] [PubMed] [Google Scholar]
- 67.Tripathy D, Im SA, Colleoni M, et al. : Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor positive, advanced breast cancer (MONALEESA-7): A randomised phase 3 trial. Lancet Oncol 19:904-915, 2018 [DOI] [PubMed] [Google Scholar]
- 68.Goetz MP, et al. : J Clin Oncol 35:3638-3646, 2017 [DOI] [PubMed] [Google Scholar]