

Abstract
Background
the timing of incident injurious falls at different stages of dementia diagnosis is unclear.
Objectives
to identify when the occurrence of injurious falls begins to increase among individuals who are going to develop dementia, to explore the time point at which people living with dementia are at highest risk of injurious falls and to ascertain differences in fall-related factors pre- and post-dementia diagnosis.
Design
this study included 2,707 participants with incident dementia and 2,707 1:1 matched (i.e. same birth year and sex) controls without dementia.
Methods
dementia diagnosis and date of onset were identified from the National Patient Registry (NPR) and the Swedish Cause of Death Register following international criteria. Information on injurious falls and history of chronic disease was obtained from the NPR. Data were analysed using conditional Poisson regression and generalized estimating equation models.
Results
compared with controls, the incidence of injurious falls among participants with dementia started to increase beginning 4 years pre-diagnosis (incidence rate ratio [IRR] 1.70, 95% confidence interval [CI] 1.30–2.22), reaching a peak (IRR 3.73, 95% CI 3.16–4.41) in the year of dementia diagnosis. Heavy drinking, physically active and cardiometabolic diseases (CMDs) were associated with incident falls among those with dementia.
Conclusion
people with dementia have a higher incidence of injurious falls beginning 4 years leading up to diagnosis and peaking during the year of diagnosis. Older age, female, heavy drinking, physically active and CMDs may predict injurious falls among people with dementia.
Keywords: injurious fall, incident dementia, matched case–control analysis, population-based study, older people
Key Points
People with dementia have a higher incidence of injurious falls beginning 4 years pre-diagnosis.
The incidence of injurious falls in people with dementia peaks in the year of diagnosis.
Older age, female sex, heavy drinking, being physically active and the presence of cardiometabolic diseases may predict falls in people with dementia.
There is a need for targeted fall prevention strategies for people with dementia, especially soon after dementia diagnosis.
Introduction
Approximately 28–35% of people above the age of 65 experience one or more falls per year, and the incidence of falls increases with age [1]. Falls can result in fractures and other injuries, leading to disability, functional dependence and premature death [2, 3]. Notably, Sweden has one of the highest rates of fall-related injuries and mortality in the world [4, 5]. Reducing and preventing the occurrence of falls therefore plays a major role in the well-being and quality of life of older adults.
Falls and dementia often co-exist in older adults and can affect one another. Growing evidence has suggested that falls may be a potential behavioural marker of preclinical Alzheimer’s disease (ad), the most common type of dementia [6, 7]. A cohort study showed that participants who fell more than twice in a year had faster cognitive decline than those who had no falls [8]. Meanwhile, dementia has also been linked to an increased risk of falls [9]. Several longitudinal studies have shown that people living with dementia or cognitive impairment have a 2- to 8-fold higher risk of falls compared with those with normal cognition [10, 11]. Therefore, ascertaining the time window in which dementia-free older adults experience an uptick in fall incidence may help identify individuals at risk for conversion to dementia and support the development of intervention strategies. To date, changes in the incidence of falls around the onset of dementia are unknown.
After developing dementia, older adults experience more cognitive and functional decline, can develop activity disturbances (such as wandering), take on a more sedentary lifestyle and feel more loss, denial, anger and apathy [12, 13]. Such changes may have an impact on physical and mental health and could influence the subsequent occurrence of falls. Therefore, it is clinically relevant to examine the occurrence of falls and related factors before and after dementia diagnosis. The time from the presentation of an individual’s first dementia symptoms to a formal diagnosis of dementia ranges from an average of 1 to 2.8 years in clinical settings [14–16]. Considering the changes in physical and mental function that occur during dementia progression and the delay between the emergence of dementia symptoms and dementia diagnosis, we aimed to compare the patterns of falls incidence both pre- and post-dementia diagnosis in order to identify a time window for effective prevention of falls among people with dementia. Many early studies of falling in older adults systematically excluded those with cognitive deficits or dementia [13, 17] or focused only on falls after dementia onset [18, 19], limiting their ability to evaluate fall risk across the full cognitive spectrum. Thus far, no population-based studies have explored the longitudinal changes in fall-related factors across dementia-free and dementia stages.
In the present study, we aimed to (i) identify when the occurrence of injurious falls starts to increase before dementia onset, (ii) ascertain when people with dementia are at highest risk of injurious falls and (iii) examine the differences in fall-related factors before and after dementia diagnosis using data from a large, nationally representative population-based cohort.
Methods
Study population
Participants were derived from the nationwide Swedish Twin Registry (STR) [20]. From 1998 to 2002, all living twins in the STR who were born in 1958 or earlier were invited to participate in the Screening Across the Lifespan Twin Study (SALT), a full-scale screening via computer-based telephone interviews. A total of 44,919 twin individuals participated in the telephone interview. Of them, 3,493 developed dementia between 1998 and 2016. From this group, we excluded 785 participants with unclear onset of dementia (n = 551), prevalent dementia at baseline (n = 152) or baseline age < 55 years (n = 82), leaving 2,708 with dementia to be included in the present study. Controls were selected from the remaining dementia-free individuals. First, we excluded participants with a baseline age < 55 years. Then, controls were matched 1:1 with the sample cohort according to birth year and sex; all matched controls were alive at the time when participants were diagnosed with dementia (one person with dementia who was not matched was excluded). Finally, a total of 5,414 individuals (2,707 with and 2,707 without dementia) were included in the current study (Figure 1).
Figure 1.

Flowchart of the study population. Abbreviations: D, died. Note: Year 0 was the year of dementia diagnosis for participants with dementia and the year at the corresponding matched age for those without dementia.
Informed consent was obtained from all participants. The study was approved by the Regional Ethics Board at Karolinska Institutet, Stockholm, Sweden and by the Institutional Review Board of the University of Southern California, USA.
Data collection
Information on age, sex, education, marital status, smoking status, alcohol consumption, physical activity, zygosity, height and weight were collected through the SALT survey. Education was dichotomized as <8 years and ≥8 years based on the maximum years of formal education received [21, 22]. Zygosity was categorized as monozygotic, dizygotic or undefined zygosity. Marital status was defined as married/cohabitating or single (including divorced and widowed). Smoking status was dichotomized as non-smokers or former/current smokers. Alcohol consumption was categorized as no/mild drinking or heavy drinking. Physical activity was defined based on a question about annual exercise patterns and grouped as active (including the responses ‘more than average’, ‘much more than average’ and ‘maximum’) and inactive (including the responses ‘almost never’, ‘much less than average’, ‘less than average’ and ‘average’) [23]. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters (kg/m2) and classified as underweight (<20.0), normal weight (20.0–24.9), overweight (25.0–29.9) and obese (≥30).
Information on hypertension and cardiometabolic diseases (CMDs) including type 2 diabetes mellitus (T2DM), heart disease and stroke [24] was derived from the Swedish National Patient Registry (NPR), which covers all inpatient diagnoses from the 1960s and outpatient care (specialist clinic) from 2001 until 2016 [25, 26]. The diagnosis of diseases was made according to International Classification of Disease (ICD) codes, as detailed in Supplementary Table 1. The seventh revision (ICD-7) was used until 1968, and from 1969 to 1986, the eighth revision (ICD-8) was applied. Between 1987 and 1996, the ninth revision (ICD-9) was used, and the tenth revision (ICD − 10) has been employed from 1997 through to the end of available follow-up in 2016.
For participants who died during follow-up, information on cause of death and date of death was extracted via linkage with the Swedish Cause of Death Register, which contains all deaths reported to the tax authorities since 1997 [27].
Assessment of dementia
Information on dementia (ICD-8 code 290; ICD-9 codes 290.0-290.1, 290.4, 290.8-290.9, 331.0 and 331.2; ICD-10 codes F00.0, F01, F02, F03, F05, G30, G31.0 and G31.8) was derived from the NPR and the Swedish Cause of Death Register. The age at onset of dementia was estimated based on the earliest date of dementia diagnosis in the NPR.
Assessment of injurious falls
In this study, injurious falls were defined as a fall resulting in the need for medical care, whether outpatient care or hospitalization. Information on the injurious falls diagnoses and their corresponding recorded time was obtained from the NPR records and identified by ICD-10 codes W00-W19 since 1997. Participants who fell one or more times in the corresponding year were defined as fallers and the earliest recorded date of those falls in that year was used as their fall time.
Statistical analysis
Baseline characteristics of the study participants by dementia status were compared using χ2 tests for categorical variables and t-tests for continuous variables.
Incidences of injurious falls were ascertained from a bidirectional timescale. That is, year 0 was the year of dementia diagnosis for participants with dementia and the year at the corresponding matched age for those without dmentia. The period ranging from 1 to 10 years before dementia diagnosis was defined as the pre-diagnostic period (year −10 to year −1) and the period ranging from 1 to 10 years after dementia diagnosis was correspondingly defined as the post-diagnostic period (year 1 to year 10).
In the primary analysis, we first calculated the age- and sex-standardized incidence rates (IRs) of injurious falls from 10 years before dementia diagnosis (year −10), through the period of diagnosis (year 0), to 10 years after dementia diagnosis (year 10). Conditional Poisson regression was used to calculate the incidence rate ratios (IRRs) and 95% confidence interval (CIs) for injurious falls.
In the secondary analysis, we used generalized estimating equation (GEE) model to estimate odds ratios (ORs) and 95% CIs for possible fall-related factors in people with dementia. There were 2,704 individuals with dementia who had information about injurious falls both pre- and post-diagnosis (three individuals with dementia only had injurious falls information since their dementia diagnosis year and were deleted). Therefore, we included only these 2,704 participants when exploring potential factors associated with injurious falls. The factors associated with injurious falls in the pre- (year −10 to year −1) and post-diagnostic (year 1 to year 10) periods were evaluated using GEE models, separately. We used GEE rather than logistic regression to control for yearly changes in injurious falls in the pre-and post-diagnostic periods. Age, hypertension, and CMDs in pre- and post-diagnostic analyses were measured at the year −10 or year 1 of dementia diagnosis, respectively. Sex, education level, marital status, smoking status, alcohol consumption, physical activity, and BMI were assessed before year −10 of dementia diagnosis. These were considered as potential fall-related factors and were mutually adjusted in the GEE models.
Missing values for education (n = 242), marital status (n = 159), smoking status (n = 236), alcohol consumption (n = 243), physical activity (n = 1,189) and BMI (n = 336) were imputed by Rubin’s rule for pooling estimates to obtain valid statistical inferences. P-values <0.05 were considered statistically significant. All statistical analyses were performed using Stata SE 15.0 (StataCorp, College Station, TX, USA).
Results
Characteristics of the study population
Among the 5,414 participants in the study, 3,190 (58.9%) were female and 2,224 (41.1%) were male. The mean age at year −10 was 71.7 ± 7.2 years. Compared with dementia-free participants, those with dementia were more likely to have hypertension and CMDs (Table 1). There were no significant differences between the two groups in terms of age, sex, education, marital status, smoking status, alcohol consumption, physical activity level and BMI.
Table 1.
Basic characteristics of the study population by dementia statusa (N = 5,414)
| Characteristics | Dementia-free (n = 2,707) | Dementia (n = 2,707) | P-value |
|---|---|---|---|
| Age (years), mean ± SD | 71.7 ± 7.2 | 71.7 ± 7.2 | 1.000 |
| Female, n (%) | 1,595 (58.9) | 1,595 (58.9) | 1.000 |
| Education, n (%) | 0.399 | ||
| <8 years | 1,416 (54.9) | 1,382 (56.1) | |
| ≥8 years | 1,164 (45.1) | 1,083 (43.9) | |
| Marital status, n (%) | 0.260 | ||
| Married/cohabitating | 1,633 (62.1) | 1,620 (63.6) | |
| Single | 998 (37.9) | 928 (36.4) | |
| Zygosity, n (%) | 0.436 | ||
| Monozygotic | 555 (20.5) | 555 (20.5) | |
| Dizygotic | 1896 (70.0) | 1868 (69.0) | |
| Undetermined | 256 (9.5) | 284 (10.5) | |
| Smoking status, n (%) | 0.814 | ||
| Never smoked | 1,558 (60.2) | 1,479 (59.9) | |
| Former/current smoker | 1,031 (39.8) | 992 (40.2) | |
| Alcohol consumption, n (%) | 0.923 | ||
| No/mild drinking | 2,470 (95.6) | 2,353 (95.5) | |
| Heavy drinking | 115 (4.4) | 111 (4.5) | |
| Physical activity, n (%) | 0.342 | ||
| Non-active | 672 (43.3) | 684 (45.1) | |
| Active | 878 (56.7) | 834 (54.9) | |
| BMI, n (%) | 0.236 | ||
| Underweight | 139 (5.6) | 120 (5.0) | |
| Normal weight | 1,142 (45.6) | 1,150 (48.5) | |
| Overweight | 1,017 (40.6) | 912 (38.5) | |
| Obese | 206 (8.2) | 189 (8.0) | |
| Hypertension, n (%) | 194 (7.2) | 225 (8.3) | <0.001 |
| CMDs, n (%) | 611 (22.6) | 729 (26.9) | <0.001 |
| Type 2 diabetes mellitus, n (%) | 176 (6.5) | 249 (9.2) | <0.001 |
| Heart disease, n (%) | 402 (14.9) | 426 (15.7) | 0.365 |
| Stroke, n (%) | 139 (5.1) | 181 (6.7) | 0.015 |
Abbreviation: SD, standard deviation.
aAge, hypertension and CMDs (including type 2 diabetes mellitus, heart disease and stroke) were obtained at 10 years before age of dementia diagnosis or matched age.
Incidence of injurious falls in the study population
Beginning 10 years prior to dementia diagnosis, the incidence of injurious falls steadily increased with age in both persons with and without dementia (Table 2). In Poisson regression analysis, the age- and sex-standardized IRs of injurious falls among persons with and without dementia were similar (around 3.93–10.74 per 1,000 person-years) in the 5–10 years preceding dementia diagnosis (Figure 2). Among controls, the steady increase in the rate of injurious falls lasted until year 4. However, among people with dementia, the incidence of injurious falls increased dramatically beginning 4 years pre-diagnosis (IR, 12.91; 95% CI, 10.82–15.01), reaching very high levels in the year of dementia diagnosis (IR, 54.51; 95% CI, 50.33–58.69) and then droping sharply after dementia diagnosis. In the 5 to 10 years after dementia diagnosis, the incidence of injurious falls among individuals with dementia returned to the same levels as the dementia-free controls (IRs around 1.63–11.04 per 1,000 person-years).
Table 2.
Age- and sex-standardized IRs and 95% CIs per 1,000 person-years and IRRs and 95% CIs of falls before, during and after dementia diagnosis in the study population (dementia-free participants as reference)
| Time in relation to diagnosis (year) | Dementia-free (n = 2,707) | Dementia (n = 2,707) | IRR (95% CI) | ||||
|---|---|---|---|---|---|---|---|
| No. of subjects | Falls n (%) | IR (95% CI) | No. of subjects | Falls n (%) | IR (95% CI) | ||
| −10 | 1897 | 32 (1.7) | 3.93 (2.57–5.29) | 1897 | 36 (1.9) | 4.42 (2.98–5.86) | 1.12 (0.70–1.81) |
| −9 | 2010 | 36 (1.8) | 4.17 (2.80–5.53) | 2010 | 59 (2.9) | 6.83 (5.08–8.57) | 1.64 (1.08–2.48) |
| −8 | 2,125 | 49 (2.3) | 5.33 (3.84–6.83) | 2,125 | 64 (3.0) | 6.97 (5.26–8.67) | 1.31 (0.90–1.89) |
| −7 | 2,270 | 63 (2.8) | 6.39 (4.81–7.97) | 2,270 | 87 (3.8) | 8.83 (6.97–10.68) | 1.38 (0.99–1.91) |
| −6 | 2,384 | 69 (2.9) | 6.65 (5.08–8.21) | 2,384 | 86 (3.6) | 8.28 (6.53–10.04) | 1.25 (0.91–1.71) |
| −5 | 2,501 | 95 (3.8) | 8.72 (6.97–10.48) | 2,501 | 117 (4.7) | 10.74 (8.80–12.69) | 1.23 (0.94–1.61) |
| −4 | 2,586 | 86 (3.3) | 7.61 (6.00–9.21) | 2,586 | 146 (5.6) | 12.91 (10.82–15.01) | 1.70 (1.30–2.22) |
| −3 | 2,650 | 110 (4.2) | 9.46 (7.69–11.22) | 2,650 | 156 (5.9) | 13.41 (11.30–15.51) | 1.42 (1.11–1.81) |
| −2 | 2,685 | 144 (5.4) | 12.18 (10.19–14.17) | 2,685 | 233 (8.7) | 19.70 (17.17–22.23) | 1.62 (1.31–1.99) |
| −1 | 2,704 | 150 (5.5) | 12.57 (10.55–14.58) | 2,704 | 265 (9.8) | 22.20 (19.53–24.87) | 1.77 (1.45–2.16) |
| 0 (diagnosis year) | 2,707 | 175 (6.5) | 14.61 (12.44–16.77) | 2,707 | 653 (24.1) | 54.51 (50.33–58.69) | 3.73 (3.16–4.41) |
| 1 | 2,589 | 176 (6.8) | 15.21 (12.96–17.46) | 2,194 | 281 (12.8) | 29.25 (25.83–32.68) | 1.92 (1.59–2.32) |
| 2 | 2,315 | 140 (6.0) | 13.52 (11.28–15.76) | 1849 | 172 (9.3) | 21.23 (18.05–24.40) | 1.57 (1.26–1.96) |
| 3 | 2037 | 121 (5.9) | 13.22 (10.86–15.58) | 1,559 | 123 (7.9) | 18.05 (14.85–21.24) | 1.36 (1.06–1.76) |
| 4 | 1774 | 88 (5.0) | 11.17 (8.83–13.50) | 1,342 | 93 (6.9) | 15.67 (12.49–18.86) | 1.40 (1.05–1.88) |
| 5 | 1,611 | 59 (3.7) | 8.30 (6.18–10.42) | 1,179 | 58 (4.9) | 11.04 (8.20–13.88) | 1.33 (0.92–1.91) |
| 6 | 1,483 | 45 (3.0) | 6.93 (4.90–8.95) | 1,044 | 46 (4.4) | 9.79 (6.96–12.62) | 1.41 (0.94–2.13) |
| 7 | 1,380 | 28 (2.0) | 4.63 (2.92–6.35) | 944 | 14 (1.5) | 3.28 (1.56–4.99) | 0.71 (0.37–1.34) |
| 8 | 1,311 | 21 (1.6) | 3.66 (2.09–5.23) | 875 | 13 (1.5) | 3.27 (1.49–5.05) | 0.89 (0.45–1.79) |
| 9 | 1,249 | 13 (1.0) | 2.42 (1.10–3.74) | 833 | 9 (1.1) | 2.34 (0.81–3.87) | 0.97 (0.41–2.26) |
| 10 | 1,221 | 12 (1.0) | 2.28 (0.99–3.56) | 796 | 6 (0.8) | 1.63 (0.33–2.93) | 0.72 (0.29–1.91) |
Figure 2.
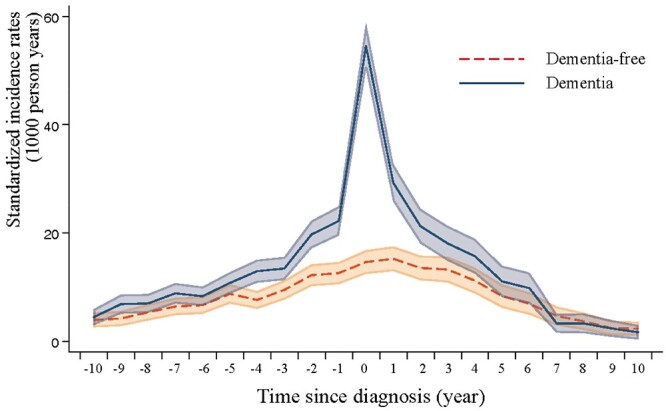
Age- and sex-standardized IRs per 1,000 person-years and 95% CIs of injurious falls by dementia status.
Overall, compared with dementia-free individuals, the incidence of injurious falls among those with dementia started to increase beginning 4 years pre-diagnosis (IRR 1.70, 95% CI 1.30–2.22), reaching a peak in the year of dementia diagnosis (IRR 3.73, 95% CI 3.16–4.41) and declining rapidly 4 years after dementia diagnosis (IRR 1.40, 95% CI 1.05–1.88).
Fall-related factors
The secondary analysis included 2,704 participants with dementia who had information on falls both pre- and post-diagnosis. In multi-adjusted GEE models, older age (OR, 1.04; 95% CI, 1.03–1.05), female sex (OR, 1.79; 95% CI, 1.53–2.10), heavy drinking (OR, 1.94; 95% CI, 1.46–2.58) and a history of CMDs (OR, 1.23; 95% CI, 1.06–1.42) were associated with significantly increased odds of injurious falls among people with dementia during the pre-diagnostic period (Table 3). During the post-diagnostic period, being physically active (OR, 1.20; 95% CI, 1.01–1.42) and having a history of CMDs (OR, 1.24; 95% CI, 1.04–1.48) were associated with a significantly increased odds of injurious falls.
Table 3.
ORs and 95% CIs of fall-related factors in people with dementia during pre- and post-diagnostic periods (N = 2,704)
| Characteristics | Pre-diagnostic perioda | Post-diagnostic periodb | ||||
|---|---|---|---|---|---|---|
| No. of subjects | No. of falls | OR (95% CI)c | No. of subjects | No. of falls | OR (95% CI)c | |
| Age at diagnosis of dementia | ||||||
| ≤75 | 500 | 126 | Reference | 500 | 137 | Reference |
| >75 ~ ≤80 | 539 | 134 | 1.05 (0.82–1.35) | 539 | 134 | 0.98 (0.77–1.27) |
| >80 ~ ≤85 | 709 | 216 | 1.31 (1.04–1.65) | 709 | 173 | 1.08 (0.85–1.37) |
| >85 ~ ≤ 90 | 639 | 234 | 1.62 (1.29–2.03) | 639 | 141 | 1.23 (0.96–1.59) |
| >90 | 317 | 151 | 2.16 (1.69–2.77) | 317 | 47 | 1.07 (0.75–1.51) |
| Sex | ||||||
| Men | 1,111 | 281 | Reference | 1,111 | 207 | Reference |
| Women | 1,593 | 580 | 1.78 (1.53–2.09) | 1,593 | 425 | 1.16 (0.97–1.40) |
| Education | ||||||
| <8 years | 1,557 | 492 | Reference | 1,557 | 357 | Reference |
| ≥8 years | 1,147 | 369 | 1.07 (0.93–1.22) | 1,147 | 275 | 0.95 (0.81–1.13) |
| Marry | ||||||
| Married/cohabited | 1,685 | 508 | Reference | 1,685 | 393 | Reference |
| Single | 1,019 | 353 | 1.04 (0.90–1.20) | 1,019 | 239 | 1.18 (0.99–1.40) |
| Smoking | ||||||
| No | 1,627 | 525 | Reference | 1,627 | 397 | Reference |
| Yes | 1,077 | 336 | 1.11 (0.96–1.29) | 1,077 | 235 | 0.93 (0.78–1.11) |
| Drinking | ||||||
| No | 2,583 | 812 | Reference | 2,583 | 611 | Reference |
| Yes | 121 | 49 | 1.88 (1.41–2.50) | 121 | 21 | 0.82 (0.52–1.31) |
| Physical activity | ||||||
| Non-active | 1,155 | 380 | Reference | 1,155 | 244 | Reference |
| Active | 1,549 | 481 | 0.92 (0.80–1.05) | 1,549 | 388 | 1.21 (1.02–1.43) |
| BMI, (kg/m2) | ||||||
| <20.0 (Underweight) | 144 | 48 | 1.12 (0.84–1.49) | 144 | 29 | 0.95 (0.63–1.42) |
| 20.0-24.9 (Normal weight) | 1,299 | 420 | Reference | 1,299 | 309 | Reference |
| 25.0-29.9 (Overweight) | 1,048 | 332 | 0.95 (0.82–1.10) | 1,048 | 249 | 1.00 (0.84–1.20) |
| ≥30 (Obese) | 213 | 61 | 0.99 (0.76–1.28) | 213 | 45 | 0.85 (0.61–1.18) |
| Hypertension | ||||||
| No | 2,480 | 781 | Reference | 1,661 | 388 | Reference |
| Yes | 224 | 80 | 1.04 (0.83–1.31) | 1,043 | 244 | 0.96 (0.80–1.14) |
| CMD | ||||||
| No | 1975 | 603 | Reference | 1,113 | 280 | Reference |
| Yes | 729 | 258 | 1.24 (1.07–1.44) | 1,591 | 352 | 1.24 (1.03–1.48) |
aFall-related factors were collected at the year of −10 of dementia diagnosis.
bAge, hypertension and CMD were collected 1 year after the diagnosis of dementia. In addition to these, other characteristics were collected before year −10 of dementia diagnosis.
cModel adjusted for age, sex, education, marital status, smoking status, alcohol consumption, physical activity, BMI, hypertension and CMD.
Discussion
In this large population-based study of older adults, we found that people diagnosed with dementia had an increased incidence of injurious falls relative to dementia-free individuals starting 4 years pre-diagnosis, peaking at the year of diagnosis and decreasing rapidly during the 4 years post-diagnosis. Risk factors associated with injurious falls among people with dementia were older age, female sex, heavy drinking and a history of CMDs during the pre-diagnostic period, and physically active and a history of CMDs during the post-diagnostic period.
The impact of falls on dementia has been extensively investigated, and it is widely agreed that persons with dementia have a higher risk of falls [28, 29]. As for the impact of falls on cognitive health, recent studies have associated a history of multiple falls with faster cognitive decline [8, 30], but not with a greater risk of incident dementia [30]. Separately, a few cohort studies have suggested that falls could be a potential behavioural marker of preclinical ad [6, 7]. A cross-sectional study showed that falls were associated with smaller hippocampal volume, a biomarker of neurodegeneration usually seen in the preclinical stage of ad [31]. Overall, previous evidence has indicated that falls and dementia are interrelated. Our study extends previous observations by exploring the time window of the incidence of injurious falls across the timeline of dementia development and found that the injurious falls rate increased beginning 4 years pre-diagnosis and declined during the 4 years post-diagnosis. To our knowledge, this is the first study to comprehensively examine the incidence of injurious falls before, during and after the diagnosis of dementia and identify the time window in which the incidence of injurious falls starts to rise.
The World Health Organization (WHO) has identified four categories of risk factors for falls in older age: biological (e.g. age and sex), behavioural (e.g. excess alcohol intake), environmental (e.g. slippery floors and stairs) and socioeconomic factors (e.g. low income and education levels) [1]. In addition, individuals with dementia experience a range of biological (e.g. decline of cognitive), behavioural (e.g. the intake of multiple medications) [32] and socioeconomic changes (e.g. a more sedentary lifestyle, impaired gait and reduced social interactions) [33] that may cause them to have different fall-related risk factors than the dementia-free population. However, most studies on risk factors for falls were conducted in the cognitively intact population [13, 17] or only among people with dementia or ad during their post-diagnostic period [18, 19]. No studies have specifically compared the risk factors for injurious falls among those with dementia before and after their dementia diagnosis. Consistent with other studies [34, 35], we found that older age, female sex and heavy drinking were associated with injurious falls before dementia diagnosis. We also found that being physically active was related to increased odds of injurious falls after a dementia diagnosis. This could be explained by progressive physical function decline among those with dementia [36–38]. This finding highlights the need for fall prevention among people with dementia doing physical activities. A history of CMDs was also associated with increased odds of injurious falls both pre- and post-diagnosis. This may reflect a worsening of overall health condition among people with CMDs [39]. Medication side effects (including blurred vision and hypotension) [40], as well as hypoglycemia-induced attention deficit and slowed psychomotor speed (for T2DM) [41], can cause falls.
The mechanisms underlying the occurrence of injurious falls are multifactorial. First, declines in motor and sensory function precede cognitive impairment [42, 43]. Thus, participants before dementia diagnosis may already have impaired gait and balance, leading to a greater risk of falls [7, 44]. As dementia progresses, the frequency of falls increases, which may further bring about a diagnosis of dementia. Falls can be a sign of an underlying health disorder, especially in the older population [45]. For older adults who fall frequently, they are more likely to receive comprehensive assessment and medical care in an inpatient or outpatient setting, in which case they are more likely to be found to have dementia. Moreover, some dysfunctions associated with dementia—including visual impairment, attention-related cognitive deficits and gait/motor disorders—could contribute to reduced muscle strength, decreased physical fitness and poor postural control, thereby increasing the incidence of falls [9, 46]. Second, individuals with dementia are commonly suffered from additional diseases (such as diabetes and postural hypotension) [47, 48] and may prescribe multiple medications that impair balance and coordination (such as antidepressants, antipsychotics and sedatives) [32, 49], making them more vulnerable to falls. Third, the progression of white matter changes [50] and subcortical infarcts [51] may disrupt the integrity of neural networks including long-descending motor fibres and frontal–subcortical circuits that control motor and cognitive function, leading to falls [52]. Finally, the decrease in fall incidence after dementia diagnosis might be partially driven by an increase in hospitalization and death among people with dementia [53, 54]. Moreover, people diagnosed with dementia often receive a variety of health care and home care services, such as personal care, house cleaning, laundry and accompanying walks, which may be beneficial in reducing the incidence of falls [55, 56].
A major strength of this study is the availability of longitudinal registry data on injurious falls and the relatively long follow-up period, which allowed us to compare the incidence of injurious falls over the entire time course of dementia diagnosis. However, some limitations should also be noted. First, we lack detailed information on injurious falls before 1997, which may have led to an underestimation of the injurious falls rate prior to this year. However, these missing records are more likely to be non-differential between participants with and without dementia due to the birth-year-matched case–control design. Second, dementia diagnoses in our study came from medical records in the NPR, which includes records of people seeking treatment in an inpatient or outpatient setting. Therefore, some participants with undiagnosed dementia may have been misclassified as dementia-free, leading to a possible underestimation of the difference in fall rates between the dementia and dementia-free groups. Another point to note is that we used the earliest date of dementia diagnosis recorded in the NPR as the age of dementia onset. Some people may have had dementia well before the date of diagnosis in the NPR, though the NPR showed high validity for the diagnosis of dementia [57]. Still, caution is required when generalizing our results to other populations. Third, information on lifestyle-related factors was collected only at baseline, making it difficult to capture potential variations in these factors during the follow-up. Finally, in the analysis of factors potentially related to falls, some factors (such as cognitive function and social support) could not be considered due to data unavailability.
In conclusion, our study provides evidence that older adults with dementia have a higher incidence of injurious falls than those without dementia beginning 4 years pre-diagnosis and peaking during the year of diagnosis. Among people with dementia, heavy drinking, physically active and a history of CMDs may predict injurious falls. Our findings suggest that injurious falls may be an early indicator of dementia in the coming years and highlight the importance of a tailored preventive strategy against falls among people with dementia at different stages of the diagnosis.
Supplementary Material
Acknowledgement
We would like to thank the Swedish Twin Registry for access to data and are grateful to all the twins who took part in the study, as well as the members of the survey teams. The Swedish Twin Registry is managed by Karolinska Institutet.
Contributor Information
Lulu Zhang, Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, China; Tianjin Key Laboratory of Environment, Nutrition and Public Health, Tianjin, China; Center for International Collaborative Research on Environment, Nutrition and Public Health, Tianjin, China.
Jiao Wang, Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, China; Tianjin Key Laboratory of Environment, Nutrition and Public Health, Tianjin, China; Center for International Collaborative Research on Environment, Nutrition and Public Health, Tianjin, China.
Abigail Dove, Aging Research Center, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden.
Wenzhe Yang, Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, China; Tianjin Key Laboratory of Environment, Nutrition and Public Health, Tianjin, China; Center for International Collaborative Research on Environment, Nutrition and Public Health, Tianjin, China.
Xiuying Qi, Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, China; Tianjin Key Laboratory of Environment, Nutrition and Public Health, Tianjin, China; Center for International Collaborative Research on Environment, Nutrition and Public Health, Tianjin, China.
Weili Xu, Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, China; Tianjin Key Laboratory of Environment, Nutrition and Public Health, Tianjin, China; Center for International Collaborative Research on Environment, Nutrition and Public Health, Tianjin, China; Aging Research Center, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicts of Interest
None.
Declaration of Sources of Funding
Weili Xu received grants from the Swedish Research Council (No. 2017-00981 and No. 2021-01647), Swedish Council for Health Working Life and Welfare (2021-01826), Karolinska Institutet Research Foundation (2020-01660), Lindhés Advokatbyrå AB (2021-0134) and Stiftelsen För Gamla Tjänarinnor (2021-2022).
The funding source had no role in the design and conduct of the study, the collection, management, analysis and interpretation of the data, the preparation, review and approval of the manuscript, or the decision to submit the manuscript for publication.
References
- 1. World Health Organization . WHO Global Report on Falls Prevention in Older Age. Geneva: WHO Press, 2017. [Google Scholar]
- 2. Trevisan C, Rizzuto D, Maggi Set al. Impact of social network on the risk and consequences of injurious falls in older adults. J Am Geriatr Soc 2019; 67: 1851–8. [DOI] [PubMed] [Google Scholar]
- 3. Gill TM, Murphy TE, Gahbauer EA, Allore HG. The course of disability before and after a serious fall injury. JAMA Intern Med 2013; 173: 1780–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Haagsma JA, Olij BF, Majdan Met al. Falls in older aged adults in 22 European countries: incidence, mortality and burden of disease from 1990 to 2017. Inj Prev 2020; 26: i67–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Haagsma JA, Graetz N, Bolliger Iet al. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the global burden of disease study 2013. Inj Prev 2016; 22: 3–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bollinger RM, Keleman A, Thompson Ret al. Falls: a marker of preclinical Alzheimer disease: a cohort study protocol. BMJ Open 2021; 11: e050820. 10.1136/bmjopen-2021-050820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Stark SL, Roe CM, Grant EAet al. Preclinical Alzheimer disease and risk of falls. Neurology 2013; 81: 437–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Padubidri A, Al Snih S, Samper-Ternent R, Markides KS, Ottenbacher KJ, Raji MA. Falls and cognitive decline in Mexican Americans 75 years and older. Clin Interv Aging 2014; 9: 719–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Buchner DM, Larson EB. Falls and fractures in patients with Alzheimer-type dementia. JAMA 1987; 257: 1492–5. [PubMed] [Google Scholar]
- 10. Delbaere K, Kochan NA, Close JCet al. Mild cognitive impairment as a predictor of falls in community-dwelling older people. Am J Geriatr Psychiatry 2012; 20: 845–53. [DOI] [PubMed] [Google Scholar]
- 11. Allan LM, Ballard CG, Rowan EN, Kenny RA. Incidence and prediction of falls in dementia: a prospective study in older people. PLoS One 2009; 4: e5521. 10.1371/journal.pone.0005521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Gerlach LB, Kales HC. Managing Behavioral and psychological symptoms of dementia. Psychiatr Clin North Am 2018; 41: 127–39. [DOI] [PubMed] [Google Scholar]
- 13. Rodrigues A, Assef JC, Lima CB. Assessment of risk factors associated with falls among the elderly in a municipality in the state of Paraíba, Brazil. A cross-sectional study. Sao Paulo Med J 2019; 137: 430–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Wolff F, Dietzel N, Karrer Let al. Timely diagnosis of dementia: results of the Bavarian dementia survey (BayDem). Gesundheitswesen 2020; 82: 23–9. [DOI] [PubMed] [Google Scholar]
- 15. Vliet D, Vugt ME, Bakker Cet al. Time to diagnosis in young-onset dementia as compared with late-onset dementia. Psychol Med 2013; 43: 423–32. [DOI] [PubMed] [Google Scholar]
- 16. Wilkinson D, Stave C, Keohane D, Vincenzino O. The role of general practitioners in the diagnosis and treatment of Alzheimer's disease: a multinational survey. J Int Med Res 2004; 32: 149–59. [DOI] [PubMed] [Google Scholar]
- 17. Herman T, Mirelman A, Giladi N, Schweiger A, Hausdorff JM. Executive control deficits as a prodrome to falls in healthy older adults: a prospective study linking thinking, walking, and falling. J Gerontol A Biol Sci Med Sci 2010; 65: 1086–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Härlein J, Dassen T, Halfens RJ, Heinze C. Fall risk factors in older people with dementia or cognitive impairment: a systematic review. J Adv Nurs 2009; 65: 922–33. [DOI] [PubMed] [Google Scholar]
- 19. Meyer C, Hill S, Dow B, Synnot A, Hill K. Translating falls prevention knowledge to community-dwelling older PLWD: a mixed-method systematic review. Gerontologist 2015; 55: 560–74. [DOI] [PubMed] [Google Scholar]
- 20. Lichtenstein P, De Faire U, Floderus B, Svartengren M, Svedberg P, Pedersen NL. The Swedish twin registry: a unique resource for clinical, epidemiological and genetic studies. J Intern Med 2002; 252: 184–205. [DOI] [PubMed] [Google Scholar]
- 21. Xu W, Caracciolo B, Wang HXet al. Accelerated progression from mild cognitive impairment to dementia in people with diabetes. Diabetes 2010; 59: 2928–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Zhang L, Yang W, Li Xet al. Association of life-course traumatic brain injury with dementia risk: a nationwide twin study. Alzheimers Dement 2022. 10.1002/alz.12671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Yang R, Xu H, Pedersen NLet al. A healthy lifestyle mitigates the risk of heart disease related to type 2 diabetes: a prospective nested case-control study in a nationwide Swedish twin cohort. Diabetologia 2021; 64: 530–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Keenan T, Zhao W, Rasheed Aet al. Causal assessment of serum urate levels in Cardiometabolic diseases through a Mendelian randomization study. J Am Coll Cardiol 2016; 67: 407–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Rahman I, Humphreys K, Bennet AM, Ingelsson E, Pedersen NL, Magnusson PK. Clinical depression, antidepressant use and risk of future cardiovascular disease. Eur J Epidemiol 2013; 28: 589–95. [DOI] [PubMed] [Google Scholar]
- 26. Patientregistret-Socialstyrelsen . Available:https://www.socialstyrelsen.se/statistik-och-data/register/alla-register/patientregistret/(Accessed 20 October 2020).
- 27. Brooke HL, Talbäck M, Hörnblad Jet al. The Swedish cause of death register. Eur J Epidemiol 2017; 32: 765–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Doorn C, Gruber-Baldini AL, Zimmerman Set al. Dementia as a risk factor for falls and fall injuries among nursing home residents. J Am Geriatr Soc 2003; 51: 1213–8. [DOI] [PubMed] [Google Scholar]
- 29. Lach HW, Harrison BE, Phongphanngam S. Falls and fall prevention in older adults with early-stage dementia: an integrative review. Res Gerontol Nurs 2017; 10: 139–48. [DOI] [PubMed] [Google Scholar]
- 30. Jayakody O, Blumen HM, Breslin Met al. Longitudinal associations between falls and future risk of cognitive decline, the motoric cognitive risk syndrome and dementia: the Einstein ageing study. Age Ageing 2022; 51: 1–7. 10.1093/ageing/afac058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Keleman A, Wisch JK, Bollinger RMet al. Falls associate with neurodegenerative changes in ATN framework of Alzheimer's disease. J Alzheimers Dis 2020; 77: 745–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Sterke CS, Beeck EF, Velde Net al. New insights: dose-response relationship between psychotropic drugs and falls: a study in nursing home residents with dementia. J Clin Pharmacol 2012; 52: 947–55. [DOI] [PubMed] [Google Scholar]
- 33. Hartman YAW, Karssemeijer EGA, Diepen LAM, Olde Rikkert MGM, Thijssen DHJ. Dementia patients are more sedentary and less physically active than age- and sex-matched cognitively healthy older adults. Dement Geriatr Cogn Disord 2018; 46: 81–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Stenbacka M, Jansson B, Leifman A, Romelsjö A. Association between use of sedatives or hypnotics, alcohol consumption, or other risk factors and a single injurious fall or multiple injurious falls: a longitudinal general population study. Alcohol 2002; 28: 9–16. [DOI] [PubMed] [Google Scholar]
- 35. Ambrose AF, Paul G, Hausdorff JM. Risk factors for falls among older adults: a review of the literature. Maturitas 2013; 75: 51–61. [DOI] [PubMed] [Google Scholar]
- 36. Wang L, Belle G, Kukull WB, Larson EB. Predictors of functional change: a longitudinal study of nondemented people aged 65 and older. J Am Geriatr Soc 2002; 50: 1525–34. [DOI] [PubMed] [Google Scholar]
- 37. Agüero-Torres H, Fratiglioni L, Guo Z, Viitanen M, Strauss E, Winblad B. Dementia is the major cause of functional dependence in the elderly: 3-year follow-up data from a population-based study. Am J Public Health 1998; 88: 1452–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Guideline for the prevention of falls in older persons . American Geriatrics Society, British geriatrics society, and American Academy of orthopaedic surgeons panel on falls prevention. J Am Geriatr Soc 2001; 49: 664–72. [PubMed] [Google Scholar]
- 39. Pirrie M, Saini G, Angeles R, Marzanek F, Parascandalo J, Agarwal G. Risk of falls and fear of falling in older adults residing in public housing in Ontario, Canada: findings from a multisite observational study. BMC Geriatr 2020; 20: 11. 10.1186/s12877-019-1399-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Loke MY, Yen Gan LL, Islahudin F. Awareness of medication related falls and preferred interventions among the elderly. Pak J Pharm Sci 2018; 31: 359–64. [PubMed] [Google Scholar]
- 41. Kodl CT, Seaquist ER. Cognitive dysfunction and diabetes mellitus. Endocr Rev 2008; 29: 494–511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Camicioli R, Howieson D, Oken B, Sexton G, Kaye J. Motor slowing precedes cognitive impairment in the oldest old. Neurology 1998; 50: 1496–8. [DOI] [PubMed] [Google Scholar]
- 43. Albers MW, Gilmore GC, Kaye Jet al. At the interface of sensory and motor dysfunctions and Alzheimer's disease. Alzheimers Dement 2015; 11: 70–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. O'Keeffe ST, Kazeem H, Philpott RM, Playfer JR, Gosney M, Lye M. Gait disturbance in Alzheimer's disease: a clinical study. Age Ageing 1996; 25: 313–6. [DOI] [PubMed] [Google Scholar]
- 45. Khow KSF, Visvanathan R. Falls in the aging population. Clin Geriatr Med 2017; 33: 357–68. [DOI] [PubMed] [Google Scholar]
- 46. Mesbah N, Perry M, Hill KD, Kaur M, Hale L. Postural stability in older adults with Alzheimer disease. Phys Ther 2017; 97: 290–309. [DOI] [PubMed] [Google Scholar]
- 47. Schubert CC, Boustani M, Callahan CMet al. Comorbidity profile of dementia patients in primary care: are they sicker? J Am Geriatr Soc 2006; 54: 104–9. [DOI] [PubMed] [Google Scholar]
- 48. Shaw FE. Prevention of falls in older people with dementia. Journal of neural transmission (Vienna, Austria: 1996) 2007; 114: 1259–64. [DOI] [PubMed] [Google Scholar]
- 49. Milos V, Bondesson Å, Magnusson M, Jakobsson U, Westerlund T, Midlöv P. Fall risk-increasing drugs and falls: a cross-sectional study among elderly patients in primary care. BMC Geriatr 2014; 14: 40. 10.1186/1471-2318-14-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Srikanth V, Phan TG, Chen J, Beare R, Stapleton JM, Reutens DC. The location of white matter lesions and gait--a voxel-based study. Ann Neurol 2010; 67: 265–9. [DOI] [PubMed] [Google Scholar]
- 51. Callisaya ML, Srikanth VK, Lord SRet al. Sub-cortical infarcts and the risk of falls in older people: combined results of TASCOG and Sydney MAS studies. Int J Stroke 2014; 9: 55–60. [DOI] [PubMed] [Google Scholar]
- 52. Choi P, Ren M, Phan TGet al. Silent infarcts and cerebral microbleeds modify the associations of white matter lesions with gait and postural stability: population-based study. Stroke 2012; 43: 1505–10. [DOI] [PubMed] [Google Scholar]
- 53. Broulikova HM, Arltova M, Kuklova M, Formanek T, Cermakova P. Hospitalizations and mortality of individuals with dementia: evidence from Czech National Registers. J Alzheimers Dis 2020; 75: 1017–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Lyketsos CG, Sheppard JM, Rabins PV. Dementia in elderly persons in a general hospital. Am J Psychiatry 2000; 157: 704–7. [DOI] [PubMed] [Google Scholar]
- 55. Sandberg L, Nilsson I, Rosenberg L, Borell L, Boström AM. Home care services for older clients with and without cognitive impairment in Sweden. Health Soc Care Community 2019; 27: 139–50. [DOI] [PubMed] [Google Scholar]
- 56. Nilsson I, Luborsky M, Rosenberg L, Sandberg L, Boström AM, Borell L. Perpetuating harms from isolation among older adults with cognitive impairment: observed discrepancies in homecare service documentation, assessment and approval practices. BMC Health Serv Res 2018; 18: 800. 10.1186/s12913-018-3616-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Rizzuto D, Feldman AL, Karlsson IK, Dahl Aslan AK, Gatz M, Pedersen NL. Detection of dementia cases in two Swedish health registers: a validation study. J Alzheimers Dis 2018; 61: 1301–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.