

Abstract
Background
Child sexual abuse is a significant global problem in both magnitude and sequelae. The most widely used primary prevention strategy has been the provision of school‐based education programmes. Although programmes have been taught in schools since the 1980s, their effectiveness requires ongoing scrutiny.
Objectives
To systematically assess evidence of the effectiveness of school‐based education programmes for the prevention of child sexual abuse. Specifically, to assess whether: programmes are effective in improving students' protective behaviours and knowledge about sexual abuse prevention; behaviours and skills are retained over time; and participation results in disclosures of sexual abuse, produces harms, or both.
Search methods
In September 2014, we searched CENTRAL, Ovid MEDLINE, EMBASE and 11 other databases. We also searched two trials registers and screened the reference lists of previous reviews for additional trials.
Selection criteria
We selected randomised controlled trials (RCTs), cluster‐RCTs, and quasi‐RCTs of school‐based education interventions for the prevention of child sexual abuse compared with another intervention or no intervention.
Data collection and analysis
Two review authors independently assessed the eligibility of trials for inclusion, extracted data, and assessed risk of bias. We summarised data for six outcomes: protective behaviours; knowledge of sexual abuse or sexual abuse prevention concepts; retention of protective behaviours over time; retention of knowledge over time; harm; and disclosures of sexual abuse.
Main results
This is an update of a Cochrane Review that included 15 trials (up to August 2006). We identified 10 additional trials for the period to September 2014. We excluded one trial from the original review. Therefore, this update includes a total of 24 trials (5802 participants). We conducted several meta‐analyses. More than half of the trials in each meta‐analysis contained unit of analysis errors.
1. Meta‐analysis of two trials (n = 102) evaluating protective behaviours favoured intervention (odds ratio (OR) 5.71, 95% confidence interval (CI) 1.98 to 16.51), with borderline low to moderate heterogeneity (Chi² = 1.37, df = 1, P value = 0.24, I² = 27%, Tau² = 0.16). The results did not change when we made adjustments using intraclass correlation coefficients (ICCs) to correct errors made in studies where data were analysed without accounting for the clustering of students in classes or schools.
2. Meta‐analysis of 18 trials (n = 4657) evaluating questionnaire‐based knowledge favoured intervention (standardised mean difference (SMD) 0.61, 95% CI 0.45 to 0.78), but there was substantial heterogeneity (Chi² = 104.76, df = 17, P value < 0.00001, I² = 84%, Tau² = 0.10). The results did not change when adjusted for clustering (ICC: 0.1 SMD 0.66, 95% CI 0.51 to 0.81; ICC: 0.2 SMD 0.63, 95% CI 0.50 to 0.77).
3. Meta‐analysis of 11 trials (n =1688) evaluating vignette‐based knowledge favoured intervention (SMD 0.45, 95% CI 0.24 to 0.65), but there was substantial heterogeneity (Chi² = 34.25, df = 10, P value < 0.0002, I² = 71%, Tau² = 0.08). The results did not change when adjusted for clustering (ICC: 0.1 SMD 0.53, 95% CI 0.32 to 0.74; ICC: 0.2 SMD 0.60, 95% CI 0.31 to 0.89).
4. We included four trials in the meta‐analysis for retention of knowledge over time. The effect of intervention seemed to persist beyond the immediate assessment (SMD 0.78, 95% CI 0.38 to 1.17; I² = 84%, Tau² = 0.13, P value = 0.0003; n = 956) to six months (SMD 0.69, 95% CI 0.51 to 0.87; I² = 25%; Tau² = 0.01, P value = 0.26; n = 929). The results did not change when adjustments were made using ICCs.
5. We included three studies in the meta‐analysis for adverse effects (harm) manifesting as child anxiety or fear. The results showed no increase or decrease in anxiety or fear in intervention participants (SMD ‐0.08, 95% CI ‐0.22 to 0.07; n = 795) and there was no heterogeneity (I² = 0%, P value = 0.79; n=795). The results did not change when adjustments were made using ICCs.
6. We included three studies (n = 1788) in the meta‐analysis for disclosure of previous or current sexual abuse. The results favoured intervention (OR 3.56, 95% CI 1.13 to 11.24), with no heterogeneity (I² = 0%, P value = 0.84). However, adjusting for the effect of clustering had the effect of widening the confidence intervals around the OR (ICC: 0.1 OR 3.04, 95% CI 0.75 to 12.33; ICC: 0.2 OR 2.95, 95% CI 0.69 to 12.61).
Insufficient information was provided in the included studies to conduct planned subgroup analyses and there were insufficient studies to conduct meaningful analyses.
The quality of evidence for all outcomes included in the meta‐analyses was moderate owing to unclear risk of selection bias across most studies, high or unclear risk of detection bias across over half of included studies, and high or unclear risk of attrition bias across most studies. The results should be interpreted cautiously.
Authors' conclusions
The studies included in this review show evidence of improvements in protective behaviours and knowledge among children exposed to school‐based programmes, regardless of the type of programme. The results might have differed had the true ICCs or cluster‐adjusted results been available. There is evidence that children's knowledge does not deteriorate over time, although this requires further research with longer‐term follow‐up. Programme participation does not generate increased or decreased child anxiety or fear, however there is a need for ongoing monitoring of both positive and negative short‐ and long‐term effects. The results show that programme participation may increase the odds of disclosure, however there is a need for more programme evaluations to routinely collect such data. Further investigation of the moderators of programme effects is required along with longitudinal or data linkage studies that can assess actual prevention of child sexual abuse.
Keywords: Adolescent; Child; Humans; Schools; Child Abuse, Sexual; Child Abuse, Sexual/prevention & control; Health Knowledge, Attitudes, Practice; Program Evaluation; Randomized Controlled Trials as Topic
Plain language summary
School‐based programmes for the prevention of child sexual abuse
Background and review question
School‐based education programmes for the prevention of child sexual abuse have been implemented on a large scale in some countries. We reviewed the evidence for the effectiveness of these programmes in the following areas: (i) children's skills in protective behaviours; (ii) children's knowledge of child sexual abuse prevention concepts; (iii) children's retention of protective behaviours over time; (iv) children's retention of knowledge over time; (v) parental or child anxiety or fear as a result of programme participation; and (vi) disclosures of past or current child sexual abuse during or after programmes. The evidence is current to September 2014.
Study characteristics
This review included 24 studies, conducted with a total of 5802 participants in primary (elementary) and secondary (high) schools in the United States, Canada, China, Germany, Spain, Taiwan, and Turkey. The duration of interventions ranged from a single 45‐minute session to eight 20‐minute sessions on consecutive days. Although a wide range of programmes were used, there were many common elements, including the teaching of safety rules, body ownership, private parts of the body, distinguishing types of touches and types of secrets, and who to tell. Programme delivery formats included film, video or DVD, theatrical plays, and multimedia presentations. Other resources used included songs, puppets, comics, and colouring books. Teaching methods used in delivery included rehearsal, practice, role‐play, discussion, and feedback.
Key results
This review found evidence that school‐based sexual abuse prevention programmes were effective in increasing participants' skills in protective behaviours and knowledge of sexual abuse prevention concepts (measured via questionnaires or vignettes). Knowledge gains (measured via questionnaires) were not significantly eroded one to six months after the intervention for either intervention or control groups. In terms of harm, there was no evidence that programmes increased or decreased children's anxiety or fear. No studies measured parental anxiety or fear. Children exposed to a child sexual abuse prevention programme had greater odds of disclosing their abuse than children who had not been exposed, however we were more uncertain about this effect when the analysis was adjusted to account for the grouping of participants in classes or schools. Studies have not yet adequately measured the long‐term benefits of programmes in terms of reducing the incidence or prevalence (or both) of child sexual abuse in programme participants.
Quality of the evidence
The quality of the evidence for all outcomes included in the meta‐analyses (combining of data) was moderate. Study quality was compromised in about half of the included studies, due to suboptimal data collection methods for study outcomes and inappropriate data analysis.
Summary of findings
for the main comparison.
| School‐based programme for the prevention of child sexual abuse compared with no intervention or standard school curriculum | ||||||
|
Patient or population: children (aged 5 to 12) and adolescents (aged 13 to 18) Settings: primary (elementary) or secondary (high) schools Intervention: school‐based education programmes for the prevention of child sexual abuse Comparison: no intervention or standard school curriculum | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control group | Intervention group | |||||
| Protective behaviours (self protective events measured using a stranger simulation test immediately post intervention) | 390 per 1000 | 795 per 1000 (559 to 914) |
OR 5.71 (1.98 to 16.51) |
102 (2 studies) | ⊕⊕⊕⊝ moderate1 | Results favoured intervention |
|
Questionnaire‐based knowledge (factual knowledge measured by assessing responses to items on a questionnaire or multi‐choice test, immediately post intervention) (higher score = higher knowledge) |
The mean knowledge score measured using a variety of scales across control groups ranged from 3 to 64 | The mean knowledge score in the intervention groups was 0.61 standard deviations higher (0.45 higher to 0.78 higher) | 4657 (18) | ⊕⊕⊕⊝ moderate2 | Results favoured intervention | |
|
Vignette‐based knowledge (applied knowledge measured by assessing responses to hypothetical scenarios, immediately post intervention) (higher score = higher knowledge) |
The mean knowledge score measured using a variety of instruments across control groups ranged from 1 to 42 | The mean knowledge score in the intervention groups was 0.45 standard deviations higher (0.24 higher to 0.65 higher) | 1688 (11) | ⊕⊕⊕⊝ moderate2 | Results favoured intervention | |
| Harm (measured using anxiety or fear questionnaires) | The mean anxiety or fear score measured using a variety of scales across control groups ranged from 2 to 7 | The mean anxiety or fear score in the intervention groups was 0.08 standard deviations lower (0.22 lower to 0.07 higher) | 795 (3) | ⊕⊕⊕⊝ moderate3 | Results showed no increase or decrease in anxiety or fear | |
| Disclosures (of past or current child sexual abuse made during or after programme completion) | 4 per 1000 | 14 per 1000 (5 to 45) |
OR 3.56 (1.13 to 11.24) |
1788 (3) | ⊕⊕⊕⊝ moderate4 | Results favoured intervention, however when adjusted for unit of analysis errors, this effect disappeared |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio; OR: odds ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1Downgraded one level due to imprecision (wide confidence intervals). 2Downgraded one level due to risk of bias: unclear or high risk of bias for randomisation and allocation concealment, and blinding of participants or personnel 3Downgraded one level due to imprecision: 95% CIs around pooled estimate include both effect and no effect. 4 Downgraded one level following sensitivity analysis using ICCs of 0.1 and 0.2 to adjust for the effect of clustering on the results.
Background
Description of the condition
Child sexual abuse is a problem of considerable magnitude with short‐ and long‐term repercussions for those victimised. There is no universal definition of child sexual abuse (Macdonald 2001; Trickett 2006). It is a term used to describe a range of experiences involving a child in unwanted, inappropriate, coercive, and unlawful sexual exploitation by an adult or older child. The World Health Organization (WHO) definition states that "child sexual abuse is the involvement of a child in sexual activity that he or she does not fully comprehend, is unable to give informed consent to, or for which the child is not developmentally prepared and cannot give consent, or that violates the laws or social taboos of society" (WHO 1999, p 15). Child sexual abuse is categorised along a continuum according to the type of abuse experienced by the child: involving physical body contact (using the term 'contact child sexual abuse') or not involving physical body contact (using the term "non‐contact child sexual abuse"). Contact acts include unwanted touching, fondling, masturbation, frottage, oral‐genital contact, and vaginal or anal penetration by a penis, finger or other object. Non‐contact acts include making sexual comments, voyeurism ('peeping'), exhibitionism ('flashing'), exposing a child to pornography, or making pornography (Finkelhor 2008; Putnam 2003). Recent meta‐analyses of data collected from retrospective studies of adults in countries and cultures worldwide estimate that 10% to 20% of female children, and 5% to 10% of male children, have experienced child sexual abuse on a spectrum from exposure through unwanted touching to penetrative assault before the age of 18 years (Barth 2013; Ji 2013; Pereda 2009; Stoltenborgh 2011). These data are likely to underestimate its true prevalence because two‐thirds of individuals never disclose their victimisation (London 2005) and most cases go unreported to authorities (Wyatt 1999). The WHO estimates that child sexual abuse contributes to seven to eight per cent of the global burden of disease for females, and four to five per cent for males (Andrews 2004).
Child sexual abuse is associated with adverse psychosocial outcomes such as depression (Roosa 1999), post‐traumatic stress disorder (Widom 1999), antisocial and suicidal behaviours (Bensley 1999), eating disorders (Perkins 1999), alcohol and substance abuse (Spak 1998), post‐partum depression and parenting difficulties (Buist 1998), sexual re‐victimisation, and sexual dysfunction (Fleming 1999). A recent meta‐analysis found child sexual abuse was also associated with higher rates of physical health conditions, including gastrointestinal, gynaecological, and cardiovascular problems, and obesity (Irish 2010). A longitudinal analysis of the association between childhood sexual abuse and educational achievement found a clear linear relationship between increasing severity of child sexual abuse and poorer educational achievement, however the relationship was confounded by sociodemographic characteristics (e.g. lower maternal age and qualifications) and family functioning variables (e.g. inter‐parental violence) known to be associated with child maltreatment (Boden 2007). These consequences are far‐reaching into families and communities, with significant costs for institutions in terms of primary and rehabilitative health care, education and welfare assistance, child protection, and justice system costs (Fang 2012).
Given the retrospective nature of many studies, it is unclear what proportion of survivors go on to experience adverse outcomes and how sexual abuse interacts with other potential risk factors for these adverse outcomes. However, outcomes are known to vary for individuals according to: child age and gender; perpetrator age and gender; the relationship between child and perpetrator; the severity, duration, and/or frequency of the abusive act(s); accompanying physical or emotional violence and/or force; and the presence of other forms of victimisation (Putnam 2003; Trickett 1997). Sexual abuse has been reported across all socioeconomic and ethnic groups, in both males and females, and perpetrators can include those outside the family as well as within it (Finkelhor 1993); they can be adults or other young people (Turner 2011). However, all children are not at equal risk. Risk factors for child sexual abuse, mainly identified in Western countries, include being female (Fergusson 1996), having a physical or mental disability (Westcott 1999), living without a natural parent (Finkelhor 1986; Finkelhor 1990), parental mental illness, parental alcohol or drug dependency, and young maternal age (Fergusson 1996; Holmes 1998; MacMillan 2013). Girls appear to be more likely to be sexually abused by family members and boys by non‐family members (Finkelhor 1990). The time of greatest vulnerability for child sexual abuse is between 7 and 12 years of age (Finkelhor 1986).
Description of the intervention
This review focuses on the most widely used strategy for the prevention of child sexual abuse: the provision of school‐based programmes. Some terms commonly used to describe these programmes include: personal safety education (NCMEC 1999); protective behaviours (Flandreau‐West 1984); personal body safety (Miller‐Perrin 1990); body safety (Wurtele 2007); and child assault prevention and child protection education (NSW Department of School Education 1998). These programmes target children and adolescents aged 5 to 18 years who are students in primary (elementary) or secondary (high) schools. Support for interventions of this type can be found in Article 19 of the United Nations Convention on the Rights of the Child, an international law, which states that governments should "take all appropriate legislative, administrative, social and educational measures to protect the child from all forms of physical or mental violence, injury or abuse, neglect or negligent treatment, maltreatment or exploitation, including sexual abuse" (United Nations 1989).
Education programmes to reduce the occurrence of sexual abuse in children and adolescents were first developed by women's rape prevention collectives in the United States of America (USA) in the 1970s (Berrick 1991). School‐based programmes for the prevention of child sexual abuse were rapidly and widely adopted across the USA, assisted in some states by policy mandates, and by the mid 1990s it was estimated that two‐thirds of 10‐ to 16‐year olds in the USA had participated in such programmes (Finkelhor 1995c). Schools are a logical choice for teaching children about sexual abuse and its prevention, given their primary function is to educate (Wurtele 2009), and the content of prevention programmes aligns with proscribed school health curricula (Walsh 2013). Hence, schools have emerged as an important primary and secondary prevention setting providing access to large populations of children and adolescents, and relatively economical service delivery, without stigmatising those who may be at particular risk (Wurtele 2010).
School‐based child sexual abuse prevention programmes are typically presented to groups of students and are tailored to ages and cognitive levels. Programme content covers themes such as body ownership; distinguishing types of touches; identifying potential abuse situations; avoiding, resisting, or escaping such situations; secrecy; and how and whom to tell if abuse has occurred (Duane 2002; Topping 2009). Many programmes also stress that the child or adolescent is not to blame. Programmes vary in the number of, and extent to which these themes are covered. There is considerable variability in programme delivery formats and teaching methods. Formats such as books, comics, dramatic plays, puppet shows, films, lectures, and discussions have been used with some programmes employing single formats, whereas others use combinations of formats (Duane 2002; Topping 2009; Wurtele 1987a). Programme teaching methods have been conceptualised on a continuum from those employing purely didactic approaches, such as a speech, address, or talk, stressing students' passive listening and acquisition of knowledge, to those employing behavioural approaches, such as modelling, and emphasising students' active participation in role‐play, rehearsing, or practising new self protection skills (Wurtele 1987a). The duration and frequency of programmes is diverse, with 30 minutes being a common length as this fits with a standard school lesson period. Programmes also vary in their scope with some programmes dealing only with child sexual abuse, whereas others integrate these themes into programmes covering broader issues such as general safety education, social and emotional learning, mental health and well being, respectful relationships, and sexuality education. This review focuses only upon interventions in which prevention of child sexual abuse is the main goal.
How the intervention might work
The ultimate goal of child sexual abuse prevention education is to prevent children from ever experiencing abuse. It is also important, in cases where children have experienced abuse, for adults to respond quickly and effectively to disclosures, to protect them from further victimisation, and to limit the harm caused. From a public health perspective (Rosenberg 1991), comprehensive approaches to child sexual abuse would involve multiple "prevention targets", including (i) offenders and potential offenders, (ii) children and adolescents, (iii) situations, and (iv) communities (Smallbone 2008, p 47). Although not yet rigorously researched, it appears that school‐based programmes may also work to enhance community capacity for sexual abuse prevention by raising awareness and delivering information to multiple members of children's social systems (Duane 2002), via provision of information packages to parents, training for teachers, and family participation in homework activities.
School‐based sexual abuse prevention programmes focus on children and adolescents as prevention targets. They seek to prevent child sexual abuse by providing students with knowledge and skills to recognise and avoid potentially sexually abusive situations, and with strategies to physically and verbally repel sexual approaches by offenders. They endeavour to minimise harm by disseminating messages about appropriate help seeking in the event of abuse or attempted abuse. Interventions aim to transfer the knowledge and skills learned by the child or adolescent in the classroom to real‐life situations. Interventions work by capitalising on principles used by classroom teachers, most notably social cognitive learning theories (Bandura 1986; Vygotsky 1986), which stress the social context of learning via the use of instruction, modelling, rehearsal, reinforcement, and feedback (Wurtele 1987a).
Do programmes actually prevent child sexual abuse? There is some evidence from a small group of studies, all of which have been conducted in the USA, that participation in school‐based child sexual abuse prevention programmes may decrease the occurrence of child sexual abuse. A study of 2000 10‐ to 16‐year olds found that those exposed to more comprehensive prevention education were more knowledgeable about sexual abuse, more likely to report using self protection strategies, more likely to report protective efficacy, more likely to have disclosed their victimisation, and less likely to engage in self blame (Finkelhor 1995a). In a follow‐up study, the same individuals were more likely to use the protective strategies they had been taught when confronted with threats and assaults (Finkelhor 1995b). Two studies with high‐school (Ko 2001) and college students (Gibson 2000) showed programmes were associated with reduced incidence of child sexual abuse. However these studies harbour the limitations of retrospective recall and have not been replicated with larger and more diverse samples. Research with sexual offenders on their perceptions of the efficacy of children's self protection strategies in actual abuse situations has found the most effective strategy, reported by three‐quarters of offenders, was to tell the offender they did not want to participate in sexual activities. Girls under the age of 12 years effectively used six strategies to avoid abuse: demanding to be left alone, saying they would tell someone, crying, saying they were scared, saying the they did not want to, and saying "no" (Leclerc 2011). These strategies are key content in school‐based child sexual abuse prevention programmes (Duane 2002).
Why it is important to do this review
Despite widespread adoption into the school curriculum in many countries, conclusions about the effectiveness of school‐based programmes for the prevention of child sexual abuse remain tentative. A number of research synthesis studies have been conducted on this topic in the form of meta‐analyses, and systematic and narrative reviews (see Table 2: Previous reviews). However the findings have been limited by methodological weaknesses in the reviews (e.g. including non‐randomised as well as randomised studies; aggregation of diverse outcomes; inappropriate analytical approaches), and in the individual studies included in the reviews (e.g. use of diverse measures; inadequate measurement of programme fidelity). Additionally, previous meta‐analyses have differed in their parameters and have not been replicated. Further, there are historical distinctions in previous reviews, for example, the classification of programmes as primarily active or passive, behavioural or instructional, that warrant further exploration; this particular distinction seems artificial from an educational perspective because many programmes are, in practice, multifaceted, involving a number of teaching methods that are used in integrated ways to deliver programme content (MacMillan 1994). What is needed is a way of identifying, more precisely, the range of child, programme, and study design characteristics that may moderate programme effectiveness.
1. Previous reviews.
| Meta‐analyses | Systematic reviews | Narrative reviews | Systematic reviews of reviews |
|
Berrick 1992 Davis 2000 Heidotting 1994 Rispens 1997 Zwi 2007 |
Duane 2002 Kenny 2008 MacIntyre 2000 MacMillan 1994 Topping 2009 |
Albers 1991 Carroll 1992 Conte 1986 Daro 1991 Daro 1994 Finkelhor 2007 Finkelhor 1992 Hébert 2004 Kolko 1988 O'Donohue 1992 Reppucci 2005 Reppucci 1991 Roberts 1999 Sanderson 2004 Wurtele 2002 Wurtele 1987b |
Mikton 2009 |
Evaluations of discrete programmes have been limited to authors assessing and reporting on one or more of five measures: (i) knowledge gains, (ii) skills gains, (iii) sexual abuse disclosures, (iv) negative programme effects or harms, and (v) subsequent incidence of child sexual abuse (Smallbone 2008). Consistent with previous reviews, the original Cochrane review found improvements in knowledge and protective behaviours (skills) among children who had received school‐based programmes (Zwi 2007). Findings on disclosures, harm, and retention of knowledge over time were inconclusive. As this was the most rigorous of the reviews ever conducted (Mikton 2009), and is the only review to include risk of bias analyses, the review also uncovered many methodological quality issues that warrant ongoing monitoring and review. This is important because the historical controversy over school‐based child sexual abuse prevention programmes is concentrated on two outcomes: programmes' actual effectiveness in preventing child sexual abuse, and concerns over negative programme effects (Finkelhor 2007). Evidence on programmes' effectiveness with regard to the fifth and arguably the most important measure, the degree to which programmes actually reduce the incidence of child sexual abuse, remains a pressing and unanswered empirical question that requires ongoing review.
It has been suggested that education programmes can cause harm to participating children and adolescents (Taal 1997). This is reported to be a common parental concern (Finkelhor 2007; Tutty 1993). Some studies report few or no evaluated negative effects on children (Tutty 1997), whereas others suggest potentially harmful sequelae. For example, some children report increased worry following programme participation (Finkelhor 1995c) and older children have been found to experience more negative feelings about non‐sexual physical touch (Taal 1997). Therefore, there is a need to rigorously evaluate the evidence for these programmes, both in terms of beneficial and harmful outcomes, and to update the current evidence base on programme effectiveness.
Objectives
To systematically assess evidence of the effectiveness of school‐based education programmes for the prevention of child sexual abuse. Specifically, to assess whether: programmes are effective in improving students' protective behaviours and knowledge about sexual abuse prevention; behaviours and skills are retained over time; and participation results in disclosures of sexual abuse, produces harms, or both.
The original review and the current update do not address whether these programmes or other interventions have reduced the incidence and/or prevalence of child sexual abuse at the population level as reported by official records (e.g. from statutory child protection services, law enforcement, primary care, or hospital data), and/or community prevalence data (e.g. from self report surveys repeated at regular intervals). This objective may be incorporated in future review updates as research advances in this field.
Methods
Criteria for considering studies for this review
Types of studies
We included studies in the original review, and in this update, if they were randomised controlled trials (RCTs), cluster‐RCTs, or quasi‐RCTs where participants were allocated to the intervention or control group by day of the week, alphabetical order, or other sequential allocation such as class or school. In decision making for inclusion in the review, we focused on features of study design rather than design labels.
Types of participants
The study population comprised children (aged 5 to 12 years) and adolescents (aged 13 to 18 years) attending primary (elementary) or secondary (high) schools.
Types of interventions
Included interventions were school‐based education programmes focusing on knowledge of sexual abuse and sexual abuse prevention concepts, or skill acquisition in protective behaviours, or both, compared with no intervention or the standard school curriculum. For this update, we excluded: interventions for preventing relationship and dating violence, and sexually coercive peer relationships, as these were reviewed in another Cochrane review (Fellmeth 2013); interventions for abduction prevention, the aims of which did not clearly refer to prevention of child sexual abuse; interventions aimed broadly at child protection or personal safety in which it was not possible to isolate the effects of the sexual abuse component; and interventions set entirely in before‐ and after‐school programmes, and early childhood programmes that were not in schools (e.g. day‐care settings).
Types of outcome measures
Child outcome measures were:
protective behaviours (as measured by an independently scored simulation test);
knowledge of sexual abuse or knowledge of sexual abuse prevention concepts, or both (as measured by questionnaires or vignettes);
retention of protective behaviours over time;
retention of knowledge over time;
harm, manifest as parental or child anxiety or fear (as measured by questionnaires); and
disclosure of sexual abuse by child or adolescent during or after programmes (as measured by official records of student self reports to school staff, child protective services, or police).
Outcomes measured did not form criteria for inclusion in the review. We included studies meeting the inclusion criteria for types of study, participants, and interventions only.
Search methods for identification of studies
Electronic searches
We completed the most recent searches for this review update on 8 September 2014. We incorporated new search terms to describe recent concepts, such as child sexual abuse in online contexts, and the increasing use of terms such as 'exploitation' and 'victimisation' by researchers when describing child sexual abuse. Searches for the previous review were completed in August 2006. Where possible, we focused on finding new studies and identifying older studies added to databases since that time. We added five new sources (two trials registers, two conference proceedings indexes, and one source of open access dissertations), and searched these for all available years (see Appendix 1). Search strategies used for the original review are in Appendix 2. The list of the databases searched and the time period they cover (for the original review and for this review update) are listed below:
Cochrane Central Register of Controlled Trials (CENTRAL 2014, Issue 8);
Ovid MEDLINE(R), 1946 to August Week 4, 2014;
EMBASE (OVID), 1980 to 2014 Week 36;
PsycINFO (OVID),1967 to September Week 1 2014;
CINAHL (EBSCOhost), 1937 to current;
Social Science Citation Index (SSCI), 1970 to 29 August 2014;
ERIC (EBSCOhost), 1966 to current;
Sociological Abstracts (ProQuest), 1952 to current;
Conference Proceedings Citation Index ‐ Science (CPCI‐S), 1990 to 29 August 2014;
Conference Proceedings Citation Index ‐ Social Sciences & Humanities (CPCI‐SSH), 1990 to 29 August 2014;
Database of Abstracts of Reviews of Effects (DARE) 2014, Issue 3, part of theCochrane Library;
ClinicalTrials.gov (clinicaltrials.gov/);
ICTRP (apps.who.int/trialsearch/);
Australasian Theses (via TROVE) (trove.nla.gov.au/);
Networked Digital Library of Theses and Dissertations (NDLTD) (via SCIRUS) (ndltd.org/serviceproviders/scirus‐etd‐search); last searched September 2013, not available in September 2014.
Searching other resources
Other sources of information searched included the reference lists of previous systematic and narrative reviews, and reference lists of included studies. We also searched databases of programme evaluations such as the Promising Practices Network (RAND Corporation 2013), and Blueprints for Healthy Youth Development (CSPV 2013). To identify unpublished studies, we circulated requests via email to relevant listservs (e.g. Child‐Maltreatment‐Research‐Listerv).
Data collection and analysis
Selection of studies
We conducted selection of studies in three phases. In phase one, we imported titles and abstracts of articles identified in the searches into reference management software and review authors KZ and SW (2007 and 2009 searches), KW and KZ (2013 searches), and KW and AS (2014 searches) independently screened them. We excluded papers if they clearly did not meet the inclusion criteria (i.e. study design, participants, type of intervention, types of comparisons). In phase two, two review authors (KZ and SW in 2007; KZ and KW in 2013; KW and AS in 2014) independently screened the titles, abstracts, and methodology sections of papers appearing to meet inclusion criteria. In phase three, we retrieved the full text of studies meeting all inclusion criteria for data extraction and we linked together multiple reports of the same study (e.g. Blumberg 1991). One study was translated into English (Del Campo Sanchez 2006). In cases where agreement could not be reached during screening, we asked a third and fourth review author to independently assess the study against the inclusion criteria, and we resolved these cases via discussion and consensus.
Data extraction and management
For this update, we used an electronic data extraction proforma adapted from the checklist of items specified in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011, Table 7.3a). Two review authors (KZ and SW in 2007) independently performed data extraction. KW repeated data extraction for all 24 studies in 2013, with KZ extracting data independently for new studies in 2013. No data extraction was required in 2014 as no further studies met the inclusion criteria. The data were entered into RevMan by KZ (Review Manager 4.2 in 2007) and KW (Review Manager 5.2 in 2013), and independently checked for accuracy by a research assistant who was not involved in the review. We resolved discrepancies via discussion. We asked authors of studies in which methods of sequence generation, allocation concealment, or blinding were unclear to provide additional information (see Assessment of risk of bias in included studies). We contacted corresponding authors of studies with insufficient information to allow inclusion in meta‐analyses (Harvey 1988; Saslawsky 1986 in 2007; Chen 2012; Kraizer 1991 in 2013) and studies that used cluster‐randomisation (Dake 2003; see Unit of analysis issues) via email with a request to provide additional data. In some instances, authors were able to provide data as requested, however, the majority did not respond to requests. It is not possible to know for sure that all authors received our correspondence.
Assessment of risk of bias in included studies
In the original review, two review authors (KZ, SW) independently assessed each included study. In the review update, the procedure was repeated by one review author (KW) who independently assessed risk of bias for all included studies and compared these results to those obtained in the original review, with KZ assessing risk of bias independently for new studies in 2013. KW repeated assessment of risk of bias after a six‐month interval. There were no discrepancies. We undertook no 'Risk of bias' assessment in 2014 as no further studies met the inclusion criteria. Review authors assessing risk of bias were not blinded to the names of the authors, institutions, journals, or results of studies.
We assessed risk of bias using the seven domains on the Cochrane revised 'Risk of bias' assessment tool (Higgins 2011, Table 8.5a): (i) random sequence generation; (ii) allocation concealment; (iii) blinding of participants and personnel; (iv) blinding of outcome assessment; (v) incomplete outcome data; (vi) selective reporting; and (vii) other sources of bias. We assessed included studies on each domain as 'low risk', 'high risk', or 'unclear risk' of bias. We made judgements by answering 'yes' (assessed as low risk of bias), 'no' (assessed as high risk of bias) or 'uncertain' (assessed as unclear risk of bias) to pre‐specified questions for each domain. We used verbatim text from study reports as support for each judgement of risk wherever possible. We entered information into RevMan and summarised it in a 'Risk of bias' table for each included study. We generated two summary figures: a 'Risk of bias' summary (Figure 1) visually depicting judgements across all studies, and a 'Risk of bias' graph (Figure 2) illustrating the proportion of studies for each risk of bias criterion. Risk of bias domains are detailed below.
1.
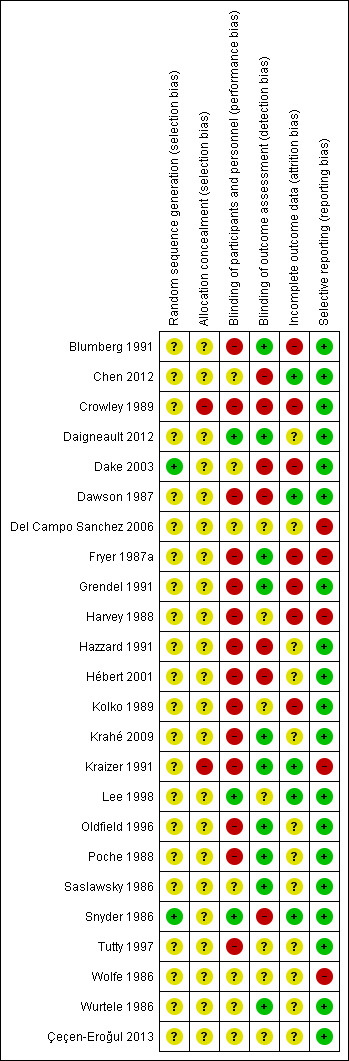
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study
2.
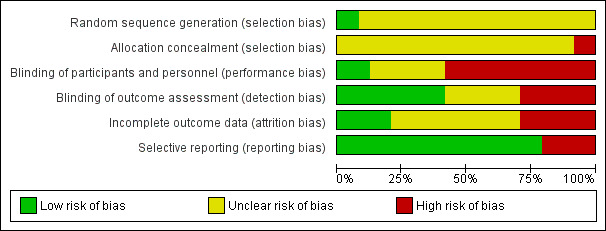
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
Random sequence generation (selection bias)
Description: The method used to generate the allocation sequence was described in sufficient detail to enable assessment of the extent to which it could produce comparable groups. In other words, a rule, based on some chance process, was adequately applied.
Questions: Do study authors make an explicit statement about random assignment? What methods were used to randomly assign participants to intervention and control groups?
Judgement: Was the allocation sequence adequately generated?
Allocation concealment (selection bias)
Description: The method used to conceal the allocation sequence was described in sufficient detail to enable assessment of whether the assignment of participants to groups could have been predicted ahead of time, or during the assignment process. Upcoming allocations were concealed from those allocating participants to groups.
Questions: Do the study authors report a method of concealing allocation of participants to intervention or control groups? Is there evidence that the method was potentially unconcealed?
Judgement: Was allocation adequately concealed?
Blinding of participants and personnel (performance bias)
Description: The measures used to blind study participants and personnel (such as programme facilitators or teachers) from knowledge of participant intervention or control group membership was described in sufficient detail to enable assessment of the effects of this knowledge on study outcomes.
Questions: Do study authors report procedures for blinding? What specific blinding procedures were used? Was blinding achievable for this type of intervention?
Judgement: Was participant and personnel knowledge of the allocation to intervention or control group adequately withheld?
Blinding of outcome assessment (detection bias)
Description: The measures used to blind outcome assessors from knowledge of participant intervention or control group membership were described in sufficient detail to enable assessment of the effects of this knowledge on outcome assessment or data collection, or both.
Questions: Do study authors report procedures for blinding of individuals responsible for outcome assessment or data collection, or both? What specific blinding procedures were used? Was blinding achievable for this type of intervention?
Judgement: Was outcome assessors' knowledge of the allocation to intervention or control group adequately withheld?
Incomplete outcome data (attrition bias)
Description: Complete outcome data are reported for each main outcome in sufficient detail to enable assessment of group differences owing to missing data. Complete outcome data include: attrition, exclusions, numbers of participants in each intervention and control group compared with the total number of participants randomised, and reasons for attrition and exclusions.
Questions: Do study authors report attrition, exclusions, numbers of participants in each intervention and control group compared with the total number of participants randomised, and reasons for attrition and exclusions? Are imputation methods explained?
Judgement: Were outcome data adequately addressed?
Selective reporting (reporting bias)
Description: The extent of outcome reporting is sufficient to enable assessment of the possibility of selective outcome reporting, that is, reporting of some outcomes and not others depending on the nature and direction of results.
Questions: Do study authors report complete outcome data that match the aims or hypotheses of the study? Do study authors report on all pre‐specified outcomes of interest?
Judgement: Are reports of the study free of suggestion of selective outcome reporting?
Other sources of bias
Description: Any other important concerns about bias not addressed in other domains.
Questions: Do study authors report studies in sufficient detail to enable assessment of other important risks of bias (e.g. related to the specific study design, extreme baseline imbalances, or contamination effects)?
Judgement: Was the study free of other problems that could put it at a high risk of bias?
Measures of treatment effect
According to the review protocol (Zwi 2003), for individual trials we planned to report the risk ratio (RR) and risk difference (RD) with 95% confidence intervals (CI) for dichotomous outcomes and mean differences (MD) with 95% CI for continuous variables. For the meta‐analysis, where possible, we planned to report the RR and RD with 95% CI for dichotomous outcomes and MD with 95% CI for continuous variables. Elsewhere in the protocol (e.g. p 4) odds ratios (OR) are also mentioned.
In the original review, and in this review update, we reported the summary of effect for dichotomous outcomes as an OR with 95% CI. Odds ratios are the statistic used most often in this field. For continuous outcomes this was to be reported as the standardised mean difference (SMD) with 95% CI. Standardised mean differences are appropriate for data synthesis where different outcome measures are used across studies.
Unit of analysis issues
In the review protocol (Zwi 2003), in the case of cluster‐RCTs, we planned to adjust for unit of analysis errors where the intraclass correlation coefficient (ICC) was available. In the original review, and in this review update, some included studies involved cluster‐randomisation at the level of the class, school, or district. However, ICCs were not reported in the studies, nor were they available from study authors. No published ICC for school‐based child sexual abuse prevention interventions could be found. We noted that estimates of 0.1 and 0.2 had been used in a review of school‐based violence prevention programmes (Mytton 2006), based on the rationale for a published ICC of 0.15 for similar trials (CPPRG 1999b in Mytton 2006), and was considered a plausible yet conservative estimate for the impact of clustering at the classroom level (Schochet 2008). We reasoned that a suitably conservative approach would be to use the extremes of ICC 0.1 and 0.2 to calculate a design effect for each cluster‐RCT according to the formula given in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011, Section 16.3.4) which is: 1 + (mean cluster size ‐ 1) ICC. We weighted these using the generic inverse variance function and used random‐effect models.
Some studies included in this review had multiple intervention groups (Blumberg 1991; Crowley 1989; Dawson 1987; Krahé 2009; Poche 1988). In these cases, we combined all relevant intervention groups into a single group, and all relevant control groups into a single group. Using the tools available in Review Manager 5.2, we combined means and standard deviations (SD) for continuous outcomes, and summed sample sizes and number of outcomes across groups for dichotomous outcomes. This enabled us to make comparisons between groups using pair‐wise comparisons without risk of double‐counting participants.
Dealing with missing data
Requirements for dealing with missing data in Cochrane Reviews have changed since the protocol for this review was written (Zwi 2003). We identified several types of missing data in this review update: missing outcomes, missing summary data, and missing participants. For missing outcomes (e.g. disclosures, adverse outcomes) and missing summary data (i.e. group size totals, means, SDs), we contacted corresponding study authors to provide the outstanding data. Some authors responded helpfully to these requests, but data could only be provided for the most recent studies; in other cases, data had been collected over two decades ago and were no longer available. In some cases, authors did not respond. If data remained unavailable after these processes, we excluded these studies from the analyses. For missing participants, we reported the attrition rate wherever possible in the 'Risk of bias' tables beneath the Characteristics of included studies table.
Assessment of heterogeneity
We assessed heterogeneity (study diversity) visually and by examining the I² statistic (Higgins 2002), a quantity which describes the proportion of variation in point estimates that is due to heterogeneity rather than sampling error. We supplemented this with a statistical test of homogeneity to determine the strength of evidence for genuine heterogeneity using a significance level of P value > 0.05.
Assessment of reporting biases
To assess reporting biases, we used two approaches to investigate the relationship between effect size and sample size (Borenstein 2009). We drew fixed‐effect forest plots with studies plotted according to weight (i.e. from most to least precise). We noted any trend towards greater effect sizes at the bottom of the plots indicative of bias attributable to missing studies. We also drew fixed‐effect funnel plots and checked them for asymmetry indicating the presence of publication bias. In both approaches, trends or asymmetry could be due to publication or related biases (e.g. language bias, availability bias, citation bias) or due to genuine differences between small and large trials (Borenstein 2009; Egger 1997). If a relationship was identified, we further examined differences between studies as a possible explanation along with comparisons by source (e.g. peer‐reviewed journals; theses). We planned to conduct these analyses only when there was a reasonable number of studies (more than 10) and a reasonable amount of dispersion in sample sizes. To reduce the effects of publication bias, in the review update, we made efforts to retrieve the full texts of unpublished trials (e.g. theses). This was made easier by virtue of the fact that many had been made available on electronic databases since our previous searches were conducted and document delivery services had improved.
Data synthesis
We synthesised the data using tools provided in Review Manger (RevMan) 5.2 (RevMan 2012). We assessed the appropriateness of combining studies based on sufficient comparability with respect to: the type of intervention, the type of outcome measures, and the nominated data collection points pre‐ and post‐intervention. We calculated summary statistics (OR for dichotomous data and SMD for continuous data) with 95% CIs for each study. We had intended to use a fixed effect model to combine data in the first instance and then to adopt a random effects model where the I square value exceeded 30%. On further consideration of the differences between the included studies in terms of their setting and intervention, we decided instead to adopt a random effects model to combine data. In all cases, we generated pooled estimates for those studies for which complete statistical data were available or could be derived (i.e. counts and proportions for dichotomous data, and means and SDs for continuous data). Forest plots are presented for each of the pooled estimates. In all cases, we corrected for small sample size bias by using Hedges' g, which is the default in Review Manager (RevMan) 5.2 (RevMan 2012).
We planned to conduct analyses on the six outcomes nominated above: (i) protective behaviours; (ii) knowledge of sexual abuse or knowledge of sexual abuse prevention concepts, or both; (iii) retention of protective behaviours over time; (iv) retention of knowledge over time; (v) parental or child anxiety or fear; (vi) disclosure of sexual abuse. To manage subtle differences in outcome measurement for (ii) (knowledge), we created subgroups according to the category of measurement instrument used (i.e. questionnaire‐based knowledge or vignette‐based knowledge). There were insufficient data to proceed with analysis for retention of protective behaviours over time. No studies measured parental anxiety or fear.
Subgroup analysis and investigation of heterogeneity
In the review protocol (Zwi 2003), we specified the conduct of subgroup analyses to assess the impact of clinically relevant differences: (i) in the interventions (e.g. passive or active involvement of participants); and (ii) between groups of participants (e.g. gender, school setting). We did not conduct subgroup analyses because there was insufficient information provided in the included studies about issues that were hypothesised as being relevant for subgroup analysis, for example, studies did not always provide a breakdown of student gender by intervention group. Further, upon close scrutiny, interventions did not appear to fit an active/passive dichotomy with many having multiple components of both active and passive types (e.g. a video or DVD presentation may at times require children to sit still and listen, and at other times, to respond, chant, sing, or move). Further, there were insufficient numbers of studies to allow for meaningful comparisons. This will be elaborated further below.
Sensitivity analysis
We conducted sensitivity analysis to explore the extent to which results were influenced by risk of bias. We conducted a series of sensitivity analyses removing from the analyses studies with high risk of bias for: (i) allocation concealment (selection bias); (ii) blinding of outcome assessors (detection bias); (iii) incomplete outcome data (attrition of over 20%), and (iv) selective reporting (reporting bias). We also conducted sensitivity analyses to determine the impact of unit of analysis errors, arising from inadequate adjustment for cluster‐randomisation in published results.
Rating the quality of the evidence
We rated the quality of the evidence for our main outcomes according to methods for rating evidence from randomised controlled trial developed by the GRADE working group (http://www.gradeworkinggroup.org/). For each outcome of interest the evidence started at high quality and could be downgraded to moderate, low or very low quality after consideration of the possible impact of risk of bias, imprecision, inconsistency, indirectness and publication bias on our confidence in the effects of intervention.
We have presented results for the primary analyses, quality ratings, and explanations for downgrading any decisions for the following outcomes in a 'Summary of Findings' table:
Protective behaviours (self protective events measured using a stranger simulation test immediately post intervention)
Questionnaire‐based knowledge (factual knowledge measured by assessing responses to items on a questionnaire or multi‐choice test, immediately post intervention)
Vignette‐based knowledge (applied knowledge measured by assessing responses to hypothetical scenarios, immediately post intervention)
Harm (measured using anxiety or fear questionnaires)
Disclosures (of past or current child sexual abuse made during or after programme completion)
Results
Description of studies
Results of the search
For this update, we searched the period from August 2006 to September 2014 (see Appendix 1). We identified a total of 12,969 records through database searching and a further 58 records from other sources. After duplicates were removed, we screened 10,218 records and excluded 10,161 records. We retrieved and evaluated the full‐text reports of the remaining 57 records for eligibility. Of these, we excluded 43 reports, with reasons reported in the Characteristics of excluded studies table. From the remaining papers, we identified: 10 new included studies, one of which was translated from Spanish into English (Del Campo Sanchez 2006); three additional reports of two included studies from the previous review (Blumberg 1991; Fryer 1987b); and one ongoing study (NCT02181647).
Searches for the original review covered the period up to August 2006 (Appendix 2). The previous review was based on 15 included studies. We excluded one of the previously included studies from this update (Pacifici 2001), because we reassessed it as not meeting the eligibility criterion for type of intervention, being focused on sexual violence prevention in the context of dating relationships for adolescents (see Fellmeth 2013), rather than explicitly on knowledge of child sexual abuse and its prevention. In total, this updated review reports on a total of 24 unique trials reported in 29 papers (Figure 3).
3.
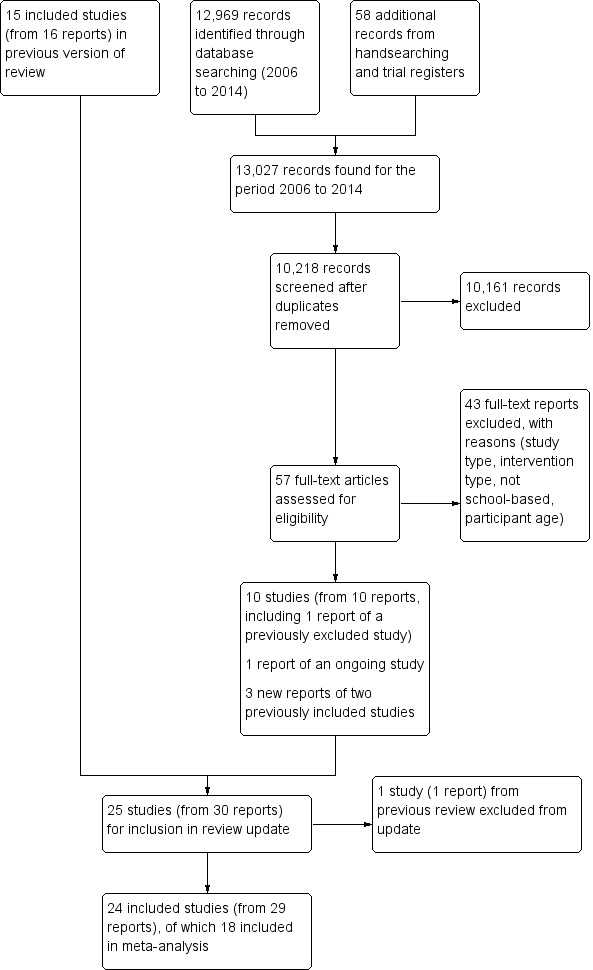
Study flow diagram for searches 2006‐2014
Included studies
The Characteristics of included studies table summarise details for each of the 24 included studies.
Design
Of the 24 included studies, seven were randomised controlled trials (RCTs) (Chen 2012; Fryer 1987a; Harvey 1988; Lee 1998; Tutty 1997; Wurtele 1986; Ҫeҫen‐Eroğul 2013), 11 were cluster‐RCTs (Blumberg 1991; Dake 2003; Dawson 1987; Grendel 1991; Hazzard 1991; Kolko 1989; Krahé 2009; Kraizer 1991; Oldfield 1996; Poche 1988; Wolfe 1986), and six were quasi‐RCTs (Crowley 1989; Daigneault 2012; Del Campo Sanchez 2006; Hébert 2001; Saslawsky 1986; Snyder 1986). Of the quasi‐RCTs, all but Del Campo Sanchez 2006 used a Solomon four‐group design (Campbell 1963; Solomon 1949).
The unit of randomisation in 14 studies was clusters (classrooms, schools, or districts). Of these, 11 were cluster‐RCTs (as above) and three were quasi‐RCTs (Crowley 1989; Daigneault 2012; Hébert 2001). In 10 trials the unit of randomisation was individual school students. Of these, seven were RCTs (as above) and three were quasi‐RCTs (Del Campo Sanchez 2006; Saslawsky 1986; Snyder 1986).
Eighteen studies allocated participants to one of two groups, the intervention (school‐based sexual abuse prevention programme) and a control group (no programme or wait‐listed). Four studies allocated participants to one of three groups, two of which were intervention groups comprising slight variations of the same programme (Krahé 2009; Kraizer 1991), or different programmes (Blumberg 1991; Del Campo Sanchez 2006). Three studies allocated participants to one of four groups, three of which were intervention groups comprising programme variations (Hazzard 1991; Poche 1988; Wurtele 1986).
Location
Sixteen studies were conducted in the USA. Three studies were conducted in Canada (Daigneault 2012; Hébert 2001; Tutty 1997). One study apiece was conducted in China (Lee 1998), Germany (Krahé 2009), Spain (Del Campo Sanchez 2006), Taiwan (Chen 2012), and Turkey (Ҫeҫen‐Eroğul 2013).
Sample sizes
The total number of participants randomised in cluster‐RCTs ranged from 74 (Poche 1988) to 1269 (Oldfield 1996). The total number of students randomised in trials with individuals as the unit of randomisation ranged from 46 (Chen 2012) to 382 (Del Campo Sanchez 2006). The number of participants in the 13 cluster‐RCTs ranged from 74 (Poche 1988) to 1269 (Oldfield 1996), and in the nine RCTs in which participants were randomised as individuals, ranged from 36 (Ҫeҫen‐Eroğul 2013) to 231 (Tutty 1997). Eleven studies (including nine cluster‐RCTs and two studies in which participants were randomised as individuals) each included more than 200 participants.
Settings
All studies were conducted in school settings: 23 in primary (elementary) schools and one in a special school for adolescents with intellectual disabilities. Only six studies were undertaken in single grades: one in kindergarten (Harvey 1988), one in grade one (Grendel 1991), two in grade three (Dake 2003; Kolko 1989), and two in grade four (Snyder 1986; Ҫeҫen‐Eroğul 2013). All other studies involved various combinations of grades to which there was no discernable pattern. It is possible to categorise the studies into three broad age group blocks as follows: (i) 10 studies with younger participants from kindergarten to grade three (Blumberg 1991; Dake 2003; Fryer 1987a; Grendel 1991; Harvey 1988; Hébert 2001; Kolko 1989; Krahé 2009; Kraizer 1991; Poche 1988); (ii) eight studies with older participants from grade four upwards (Crowley 1989; Dawson 1987; Del Campo Sanchez 2006; Hazzard 1991; Lee 1998; Snyder 1986; Wolfe 1986; Ҫeҫen‐Eroğul 2013); and (iii) six studies with younger and older participants together (Chen 2012; Daigneault 2012; Oldfield 1996; Saslawsky 1986; Tutty 1997; Wurtele 1986).
None of the included studies were conducted in secondary (high) school settings.
Participants
A total of 5802 school‐aged participants were included in the 24 trials. Study participants' mean ages at baseline in the included studies ranged from 5.8 years (Harvey 1988) to 13.44 years (Lee 1998). Authors of eight studies did not report the mean age of participants at baseline (Crowley 1989; Del Campo Sanchez 2006; Fryer 1987a; Hazzard 1991; Kraizer 1991; Oldfield 1996; Tutty 1997; Ҫeҫen‐Eroğul 2013).
The proportion of females in the included studies ranged from 45% (Poche 1988; Ҫeҫen‐Eroğul 2013) to 55% (Crowley 1989). One trial enrolled female participants only (Lee 1998). Gender‐specific proportions were not reported in five studies (Chen 2012; Daigneault 2012; Fryer 1987a; Harvey 1988; Kraizer 1991).
Ethnicity data were reported in 13 studies. Two studies reported 100% Chinese participants (Chen 2012; Lee 1998). In five studies the predominant ethnicity reported was White or Caucasian comprising 74% to 97% of participants (Grendel 1991; Oldfield 1996; Poche 1988; Snyder 1986; Tutty 1997). Six studies reported diverse samples comprising participants from different combinations of White or Caucasian, Black or African, Hispanic, Asian, Middle Eastern, or 'other' backgrounds (Blumberg 1991; Daigneault 2012; Dake 2003; Dawson 1987; Harvey 1988; Hazzard 1991). In these six studies, the proportion of non‐White participants ranged from 32% (Hazzard 1991) to 66% (Dake 2003). One of these studies reported country of birth rather than ethnicity (Daigneault 2012). Ethnicity data were not reported in the 10 remaining studies (Del Campo Sanchez 2006; Fryer 1987a; Hébert 2001; Kolko 1989; Krahé 2009; Kraizer 1991; Saslawsky 1986; Wolfe 1986; Wurtele 1986; Ҫeҫen‐Eroğul 2013).
Parental socioeconomic position was not reported in any study. Non‐empirical markers for study locations were used such as "low socioeconomic" (e.g. Daigneault 2012), "middle income" (Grendel 1991; Hébert 2001; Poche 1988), or "lower to middle income" (Saslawsky 1986; Wolfe 1986; Wurtele 1986).
Religious background of study participants was not reported in any study. One study reported data collection in religious schools in Spain (Del Campo Sanchez 2006).
Participants' school achievement data (e.g. grades) at baseline were not reported in any study. In one study, the Peabody Picture Vocabulary Test (PPVT) (Dunn 1981) was used to assess children's receptive and expressive language ability at baseline (Fryer 1987a), and, in another study, Raven's Standard Progressive Matrices (RSPM) (Raven 1960) was used as a measure of general intellectual ability at baseline (Lee 1998); in this study, participants were adolescent Chinese females with mild intellectual disabilities from four special schools in Hong Kong, China.
None of the studies enrolled participants on the basis of previously reported abuse.
Interventions
In all 24 trials, interventions focused specifically on child sexual abuse prevention. The targets of the interventions were school‐aged children who were taught knowledge of sexual abuse, sexual abuse prevention concepts, and/or skill acquisition in self protective behaviours.
A wide range of previously published, modified, and new prevention programmes were used in the trials. Fifteen discrete programmes were identified including: Behavioural Skills Training (BST) (Lee 1998; Wurtele 1986), Good Touch/Bad Touch (Crowley 1989; Harvey 1988; Ҫeҫen‐Eroğul 2013), Red Flag/Green Flag (Chen 2012; Kolko 1989), Child Abuse Primary Prevention Program (CAPPP) (Blumberg 1991), Child Sexual Abuse Prevention Program (Grendel 1991), Children Need to Know Personal Safety Training Programme (Fryer 1987a), ESPACE (Daigneault 2012; Hébert 2001), Good Secrets/Bad Secrets (Snyder 1986), No Child's Play (Krahé 2009), Prevention of Child Sexual Abuse Program (Del Campo Sanchez 2006), Project TRUST (Oldfield 1996), Safe Child Program (Kraizer 1991), Stop, Tell someone, Own your body, Protect yourself (STOP!) (Blumberg 1991), TOUCH (Saslawsky 1986), and Who Do You Tell? (Tutty 1997).
In two trials, combinations of programmes were used in interventions: TOUCH plus BST (Wurtele 1986), and Feeling Yes, Feeling No plus Spiderman and Power Pack Comic Book (Hazzard 1991). Four trials did not identify the programme used (Dake 2003; Dawson 1987; Poche 1988; Wolfe 1986).
Contents of or topics covered in the intervention programmes were not consistently reported in the majority of trials. We could discern that programmes were multifaceted with integrated content, including teaching of safety rules ranging from two to six rules (e.g. Grendel 1991; Poche 1988), with the most common being four rules (Blumberg 1991; Fryer 1987a; Lee 1998; Saslawsky 1986; Wurtele 1986), and prevention concepts such as body ownership, private parts, distinguishing appropriate and inappropriate touches, distinguishing types of secrets, and whom to tell. Programme content was not detailed in eight studies (Crowley 1989; Dake 2003; Dawson 1987; Del Campo Sanchez 2006; Hazzard 1991; Krahé 2009; Snyder 1986; Tutty 1997). Four studies also included abduction prevention content (Chen 2012; Fryer 1987a; Kraizer 1991; Poche 1988).
Teaching methods were more clearly reported than programme contents. Rehearsal, practice, or role‐play was mentioned in 12 studies (Blumberg 1991; Daigneault 2012; Fryer 1987a; Harvey 1988; Hébert 2001; Kraizer 1991; Lee 1998; Poche 1988; Snyder 1986; Tutty 1997; Wurtele 1986; Ҫeҫen‐Eroğul 2013), discussion in 10 studies (Blumberg 1991; Grendel 1991; Hazzard 1991; Hébert 2001; Oldfield 1996; Saslawsky 1986; Snyder 1986; Tutty 1997; Wolfe 1986; Wurtele 1986), and modelling in six studies (Daigneault 2012; Hébert 2001; Lee 1998; Saslawsky 1986; Wurtele 1986; Ҫeҫen‐Eroğul 2013). A specific suite of teaching strategies was designated in four studies, including instruction, modelling, rehearsal, social reinforcement, shaping, feedback, and group mastery (Chen 2012; Lee 1998; Saslawsky 1986; Wurtele 1986). The strategy review, which involved revisiting previous content and summarising new content, was nominated in one study (Grendel 1991). Three studies did not report teaching methods (Crowley 1989; Dake 2003; Del Campo Sanchez 2006).
Programme delivery formats were reported in the majority of studies. These included film, video, and DVD formats in 12 studies (Blumberg 1991; Dawson 1987; Grendel 1991; Harvey 1988; Hazzard 1991; Kolko 1989; Krahé 2009; Poche 1988; Saslawsky 1986; Tutty 1997; Wurtele 1986; Ҫeҫen‐Eroğul 2013), plays in three studies (Krahé 2009; Oldfield 1996; Wolfe 1986), and multimedia in two studies (Blumberg 1991; Hazzard 1991). Additional resources included songs (Blumberg 1991; Harvey 1988; Krahé 2009), puppets (Blumberg 1991; Harvey 1988), comics (Dawson 1987; Hazzard 1991), a colouring book (Kolko 1989), a storybook (Harvey 1988), and games (Harvey 1988). Three studies did not nominate programme delivery formats (Crowley 1989; Dake 2003; Del Campo Sanchez 2006).
No programmes were delivered electronically in web‐ or computer‐based formats.
The duration of the intervention programmes in the included trials ranged from a single 45‐minute session (Oldfield 1996) to eight 20‐minute sessions on consecutive days (Fryer 1987a). Fourteen interventions were brief (i.e. less than 90 minutes total duration) (Blumberg 1991; Crowley 1989; Dawson 1987; Grendel 1991; Harvey 1988; Hébert 2001; Kolko 1989; Krahé 2009; Lee 1998; Oldfield 1996; Poche 1988; Saslawsky 1986; Wolfe 1986; Wurtele 1986), and the remainder were longer, lasting from 90 to 180 minutes in total duration.
In 17 trials, the effectiveness of prevention programmes was compared to that of a wait‐listed control group. In the seven remaining studies, the control group interventions were as follows: discussion about self concept (Saslawsky 1986; Wurtele 1986); multimedia presentation with no child abuse content (Harvey 1988); fire safety (Blumberg 1991); fire or water safety (Hazzard 1991); attention control programme (Lee 1998); and a game of hangman (Snyder 1986).
All programmes were delivered on school premises and during school hours, apart from one study in which the programme was delivered in the morning, before school classes began (Chen 2012).
Outcomes
In this section we summarise six outcome measures of interest that were addressed in the included studies: (i) protective behaviours; (ii) knowledge (questionnaire‐based knowledge and vignette‐based knowledge); (iii) retention of protective behaviours over time; (iv) retention of knowledge over time; (v) harm (manifest as parent or child anxiety or fear); and (vi) disclosures. This information is presented in the Characteristics of included studies tables.
Protective behaviours
Three studies measured change in behaviour using a simulated abuse situation and scored the child's response to the situation (Fryer 1987a; Kraizer 1991; Poche 1988). All three studies used a version of a stranger simulation test to assess children's self protective skills (i.e. whether children could follow the rules they were taught and not interact if approached by a stranger).
Knowledge
Knowledge outcome measures varied between studies. Knowledge measures used were: (i) questionnaire‐based measures, or (ii) vignette‐based measures that used scenarios or visual prompts to elicit a response from the child about safe behaviour in that situation. Only one study did not measure knowledge (Poche 1988), and one study used a vignette‐based measure only (Krahé 2009). Ten studies used both vignette‐ and questionnaire‐based measures (Blumberg 1991; Chen 2012; Daigneault 2012; Grendel 1991; Harvey 1988; Hazzard 1991; Hébert 2001; Lee 1998; Saslawsky 1986; Wurtele 1986). Three studies used a second questionnaire‐based measure to establish construct validity (Chen 2012; Crowley 1989; Del Campo Sanchez 2006).
The use of more than one measure by studies to assess knowledge gain was not anticipated at the outset of this systematic review. The two types of measures were administered differently. Questionnaire‐based measures were administered as self completed measures via individual or group administration. Vignette measures were administered by interview. The different methods of administration and the type of response required from the child means that these two outcomes may measure different aspects of children's knowledge; therefore, we considered them as separate knowledge outcomes.
Knowledge ‐ questionnaire‐based measures
Questionnaire‐based knowledge measures were used in 21 studies. The Personal Safety Questionnaire (PSQ) was used in six (Crowley 1989; Grendel 1991; Hébert 2001; Lee 1998; Saslawsky 1986; Wurtele 1986). The Children's Knowledge of Abuse Questionnaire (CKAQ) and versions thereof (CKAQ‐R, CKAQ‐IIIR) were used in five studies (Daigneault 2012; Del Campo Sanchez 2006; Hébert 2001; Oldfield 1996; Tutty 1997), and the Children Need to Know Knowledge/Attitude Test (CNTKKAT) was used in two (Fryer 1987a; Kraizer 1981). Other custom‐made knowledge scales were also used (Blumberg 1991; Chen 2012; Crowley 1989; Dake 2003; Dawson 1987; Del Campo Sanchez 2006; Harvey 1988; Hazzard 1991; Kolko 1989; Snyder 1986; Wolfe 1986; Ҫeҫen‐Eroğul 2013).
Knowledge ‐ vignette‐based measures
Vignette‐based knowledge measures were used in 11 studies. The What If Situations Test (WIST), comprising six brief verbal vignettes, was used in four studies (Grendel 1991; Lee 1998; Saslawsky 1986; Wurtele 1986). A Chinese version of the WIST was used in one study (Chen 2012), and a French version in another (Daigneault 2012). The Touch Discrimination Task (TDT), based on the WIST and comprising seven verbal vignettes, was used in one study (Blumberg 1991), and an unnamed measure comprising 10 picture vignettes featuring good touch and sexually abusive touch were used in another study (Harvey 1988). Eight cartoon picture vignettes and stories were used in Krahé 2009. Video vignettes entitled What Would You Do? (WWYD) and comprising six 30‐second scenes were used by Hazzard 1991, and an unnamed video measure with five situations was used by Hébert 2001.
Retention of protective behaviours over time
Retention of self protective skills was measured in three studies at one month (Poche 1988), and six months (Fryer 1987a; Kraizer 1991). In Fryer 1987a, no comparison with the control group was available at follow‐up because the control groups had been exposed to the intervention. In Kraizer 1991, data were not reported. In Poche 1988, there was substantial loss to follow‐up.
All three studies measured post‐test protective behaviours within one to two days following the intervention. One study reported following up with assessment of protective behaviours one month after the intervention (Poche 1988), and the two other studies reported following up six months after the intervention (Fryer 1987a; Kraizer 1991). However, follow‐up data were published only for Fryer 1987a; data were not published for Kraizer 1991, and Poche 1988 reported significant loss to follow‐up with only nine of 23 children available for measurement.
Retention of knowledge over time
All of the 21 studies measuring post‐test questionnaire‐based knowledge did so within a two‐week period following intervention. Ten studies also reported short‐term knowledge outcomes one to three months following intervention (Crowley 1989; Dawson 1987; Harvey 1988; Hazzard 1991; Hébert 2001; Lee 1998; Poche 1988; Saslawsky 1986; Wurtele 1986; Ҫeҫen‐Eroğul 2013). One study reported knowledge outcomes at five months (Blumberg 1991), three studies at six months (Fryer 1987a; Kolko 1989; Kraizer 1991), and two studies at eight months (Del Campo Sanchez 2006; Krahé 2009). One study measured long‐term outcomes at 12 months (Hazzard 1991). One study measured long‐term outcomes in "the second year of the study" (Daigneault 2012, p 527), however the precise timing was not reported.
For most studies, no comparison with the control group was available at follow‐up because the control groups had been exposed to the intervention by then. Complete data (for intervention and control groups) were reported in only four studies (Dawson 1987; Hazzard 1991; Kolko 1989; Lee 1998).
Harm ‐ parental or child anxiety or fear
No studies measured parental anxiety or fear. Parent satisfaction questionnaires were used in five studies (Grendel 1991; Hazzard 1991; Hébert 2001; Tutty 1997; Wurtele 1986).
Six studies measured child anxiety or fear via child report (Blumberg 1991; Daigneault 2012; Dawson 1987; Hazzard 1991; Kraizer 1991; Lee 1998), and four studies via parent report (Del Campo Sanchez 2006; Hazzard 1991; Hébert 2001; Tutty 1997). Instruments used with children were the State‐Trait Anxiety Inventory for Children (STAIC) (Dawson 1987; Hazzard 1991; Oldfield 1996), the Revised Children's Manifest Anxiety Scale (RCMAS) (Oldfield 1996), and the Fear Assessment Thermometer Scale (Lee 1998). One study used a "children's feelings of safety" measure (Daigneault 2012, p 530). Instruments used with parents were adapted from the Parental Perception Questionnaire (PPQ) (Miller‐Perrin 1986), a 16‐item measure in which parents rate how often they observed negative and positive behaviours. Included studies variously referred to the measure as a 'parent observation' measure (e.g. Tutty 1997) and a 'side effects' scale (e.g. Del Campo Sanchez 2006).
Disclosures
Children's disclosures of child sexual abuse during or following intervention were reported by five studies (Blumberg 1991; Del Campo Sanchez 2006; Hazzard 1991; Kolko 1989; Oldfield 1996). To record disclosures, two studies used a data collection form completed by staff at the school (Hazzard 1991; Oldfield 1996). Two other studies conducted child protective services (CPS) file searches (Blumberg 1991; Kolko 1989). Blumberg 1991 conducted follow‐up CPS searches at 15 months post‐intervention.
Excluded studies
We excluded 55 studies because they did not meet the inclusion criteria. We excluded 36 studies on the basis of study type (13 pre‐test and post‐test studies without control groups; 11 controlled before‐and‐after studies without random assignment; five post‐test only studies; five quasi‐experimental studies without random assignment; one cross‐sectional comparative study; and one comparative group design). We excluded 14 studies because the intervention was not primarily about child sexual abuse prevention, but was about dating and relationship violence, gendered violence, or sexual harassment in the context of partner relationships (seven of these studies were cited in the Cochrane Review by Fellmeth 2013, including Pacifici 2001, which was included in the original review) or abduction prevention, the aims of which did not mention prevention of child sexual abuse. We excluded four studies because they were not school‐based and one study because participants were outside the age criteria.
Reasons for exclusion are detailed in the Characteristics of excluded studies table.
Risk of bias in included studies
Allocation
Random sequence generation
Twenty studies stated that individuals or groups (classes, schools, or districts) were "randomised", "randomly allocated", or "randomly assigned" to groups, but provided no detail about how the random sequence was generated. Three further studies described a classic experimental design, but did not report details about random assignment (Dake 2003; Kolko 1989; Kraizer 1991). We classified all of these studies as unclear risk of bias. One study reported a random component in the sequence generation, coin tossing (Snyder 1986), and we classified it as low risk of bias. In one study, evidence of computerised randomisation was provided after author contact (Dake 2003). We re‐classified this study as low risk of bias.
Allocation concealment
No studies provided information on methods used to conceal allocation. In all instances we concluded that procedures were potentially unconcealed such that assignment to groups could reasonably have been predicted prior to or during the process. Twelve studies reported tests of baseline imbalances showing no statistical differences between groups, potentially indicating successful randomisation. However, we classified these studies as unclear risk of bias because the method of concealment was not described in sufficient detail for an adequate assessment to be made. Ten studies provided no baseline comparisons and we also classified them as unclear risk of bias. We classified two studies as high risk of bias: one study reported important differences between groups at baseline and concluded failure of randomisation (Crowley 1989, pp 60‐1) and another study revealed school officials were involved in the process (Kraizer 1991, p 27).
Blinding
Blinding of participants and personnel
The school‐based nature of the interventions made blinding of participants receiving the intervention and personnel delivering the intervention impossible. In 14 studies intervention and control groups were located within the same school. In these cases, it was possible that participants experienced 'contamination' effects via contact with each other in the playground or their siblings at home, and/or inadvertent 'exposure' to programme concepts via teachers and other school staff. This is likely to have biased the results towards an underestimation of programme effects, particularly on knowledge outcomes, which would be more susceptible to such contamination and exposure. Personnel delivering the interventions were various study authors, programme facilitators, and classroom teachers. None of these 14 studies described a means by which programme fidelity or integrity was addressed (e.g. via the use of scripts or standardised lesson plans) or measured (e.g. via observation, audio, or video recordings). We classified these 14 studies as high risk of bias. Seven further studies provided no information on blinding procedures and we classified them as unclear risk of bias (Chen 2012; Dake 2003; Del Campo Sanchez 2006; Saslawsky 1986; Wolfe 1986; Wurtele 1986; Ҫeҫen‐Eroğul 2013). We classified three studies as low risk of bias: one study reported that instructors were blind to group conditions (Daigneault 2012), one study reported measures to control for contamination and the use of narrative scripts (Lee 1998), and another study reported that the programme and testing were conducted on the same day to minimise the risk of contamination between groups in the school (Snyder 1986).
Blinding of outcome assessment
Blinding was not reported in seven studies (Del Campo Sanchez 2006; Harvey 1988; Kolko 1989; Lee 1998; Tutty 1997; Wolfe 1986; Ҫeҫen‐Eroğul 2013), which we classified as unclear risk of bias.
We classified 10 studies as low risk of bias (Blumberg 1991; Daigneault 2012; Fryer 1987a; Grendel 1991; Krahé 2009; Kraizer 1991; Oldfield 1996; Poche 1988; Saslawsky 1986; Wurtele 1986). Some studies used multiple strategies for minimising outcome assessment bias. In eight studies, authors reported that outcome assessors were blind to group membership, study hypotheses, or both (Blumberg 1991; Daigneault 2012; Fryer 1987a; Grendel 1991; Krahé 2009; Oldfield 1996; Saslawsky 1986; Wurtele 1986). In three studies, authors noted that participants were not informed that the outcome assessment was related to the intervention (Blumberg 1991; Fryer 1987a; Poche 1988), and in three studies outcome assessors were reported to be different to the personnel delivering the interventions (Blumberg 1991; Fryer 1987a; Kraizer 1991). In two studies, video monitoring was used to collect observational data on the protective behaviours outcome, and coders' inter‐rater reliability was reported (Fryer 1987a; Kraizer 1991). One study reported that participants were assessed only once (either pre‐test or post‐test) by the same outcome assessor to control for potential effects of rapport building (Blumberg 1991). Of these 10 studies, Fryer 1987a implemented more strategies than any other study and we considered it to be at lowest risk of bias in this domain.
We classified seven studies as high risk of bias. In these studies outcome assessment was administered in group format (in class or with a number of children) and there were no strategies in place to blind outcome assessors to group membership or to ensure children completed the assessment independently (Chen 2012; Crowley 1989; Dake 2003; Dawson 1987; Hazzard 1991; Hébert 2001; Snyder 1986). This risk was further heightened when the outcome assessors were the same individuals as those delivering the programme (e.g. Dawson 1987).
Incomplete outcome data
Attrition rates for individual studies are reported in the 'Risk of bias' tables beneath the Characteristics of included studies table. Twelve studies did not report attrition rates (Daigneault 2012; Del Campo Sanchez 2006; Hazzard 1991; Hébert 2001; Krahé 2009; Oldfield 1996; Poche 1988; Saslawsky 1986; Tutty 1997; Wolfe 1986; Wurtele 1986; Ҫeҫen‐Eroğul 2013). We classified these studies as unclear risk of bias. One study reported no attrition or loss to follow‐up (Chen 2012) and we classified it as low risk of bias. We classified four further studies as low risk of bias, reporting attrition rates of less than 10% (Dawson 1987; Kraizer 1991; Lee 1998; Snyder 1986). Seven studies reported attrition rates of more than 10%, ranging from 12% to 24%, all of which we classified as high risk of bias (Blumberg 1991; Crowley 1989; Dake 2003; Fryer 1987a; Grendel 1991; Harvey 1988; Kolko 1989).
Only four studies reported results in such a way that loss to follow‐up for intervention and control groups could be differentiated: Blumberg 1991 (14.1% role‐play, 8.1% multimedia, 3.8% control), Dawson 1987 (7.3% intervention, 2.6% control 1, 3.1% control 2), Fryer 1987a (4% intervention, 12% control), and Grendel 1991 (19% intervention, 22% control).
Reasons for attrition were reported in nine studies (Crowley 1989; Dake 2003; Dawson 1987; Grendel 1991; Harvey 1988; Kraizer 1991; Lee 1998; Poche 1988; Snyder 1986) and included student absence, withdrawal, vacation, illness, and school change, as well as missing or incomplete data on forms, and unmatchable pre‐ and post‐tests.
No study reported analysis on an intention‐to‐treat (ITT) basis.
Selective reporting
Most studies reported complete outcome data that matched the stated aims or hypothesis of the study, and reported on pre‐specified outcomes of interest. We initially classified these studies as low risk of bias. We classified two studies as high risk of bias (Fryer 1987a; Wolfe 1986), because not all measures discussed in the methods section of the paper were also reported in the results. This may be an artefact of publication word limits.
On closer inspection, however, we noted that outcome reporting was incomplete in five studies. One study did not provide a breakdown of data for intervention and control groups (Kraizer 1991). In four studies, outcomes were reported as summary statistics (e.g. F‐tests or T‐tests) without including means and SDs for continuous outcomes (Del Campo Sanchez 2006; Chen 2012, Harvey 1988; Kraizer 1991). Where data were not reported, we contacted study authors with an open‐ended request to provide further information. We received helpful replies from Chen 2012 (additional data provided; study classified as low risk of bias) and Kraizer 1991 (data unable to be retrieved; study classified as high risk of bias).
We classified no studies as unclear risk of bias.
In summary we considered five studies as high risk of bias on this domain (Del Campo Sanchez 2006; Fryer 1987a; Harvey 1988; Kraizer 1991; Wolfe 1986), and we considered the remaining 19 studies low risk of bias.
Other potential sources of bias
The unit of randomisation in 14 studies was clusters. Eleven of these were cluster‐RCTs (Blumberg 1991; Dake 2003; Dawson 1987; Grendel 1991; Hazzard 1991; Kolko 1989; Krahé 2009; Kraizer 1991; Oldfield 1996; Poche 1988; Wolfe 1986), where the unit of allocation was a group (e.g. classroom or school). Three quasi‐RCTs also used groups as the unit of randomisation (Crowley 1989; Daigneault 2012; Hébert 2001). None of these studies reported appropriate analyses accounting for clustering effects. Therefore, we assumed unit of analysis errors in all cases, meaning the original P values would be artificially small. In the subsequent meta‐analysis, studies with unadjusted unit of analysis errors would be incorrectly and more highly weighted than is, in reality, appropriate. This risks biasing results in favour of the intervention.
As noted above, to diminish the risk of publication bias, in the review update we made concerted efforts to retrieve the full texts of unpublished trials (e.g. theses). Seven of 29 records included in this review were unpublished theses (Blumberg 1987; Chadwick 1989; Crowley 1989; Dawson 1987; Grendel 1991; Kraizer 1991; Snyder 1986). We assessed the risk of publication bias by drawing fixed‐effect forest and funnel plots for the two meta‐analyses involving 10 or more trials (questionnaire‐based knowledge, 18 trials; vignette‐based knowledge, 11 trials). Visual inspection of fixed‐effect forest plots revealed no discernable trend towards greater effect sizes in smaller studies. However, our subjective impression of the fixed‐effect funnel plots suggested the presence of slight asymmetry on the lower right (here we found smaller studies with greater effect sizes) indicating the possibility that some studies are missing from the lower left (here we should have found smaller studies with smaller effect sizes) (see Figure 4 and Figure 5). There is also the possibility that smaller studies were of poorer methodological quality (although this is not evident in the 'Risk of bias' assessments), or there may have been genuine differences between studies (e.g. unreported sample differences at baseline; differences in programme duration) (Borenstein 2009). Due to poor reporting of variables that may be responsible for heterogeneity, it was not possible to further explore the sources of variation, for example, via the use of meta‐regression.
4.
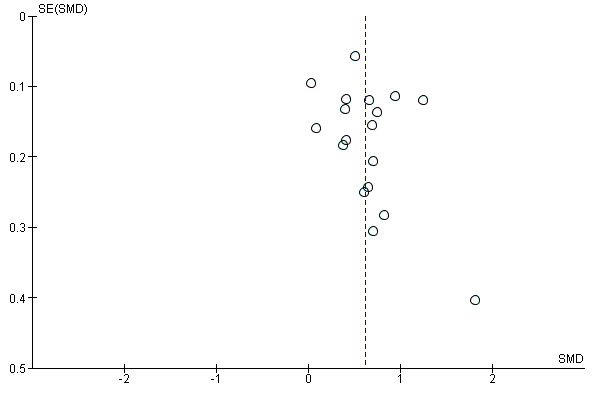
Funnel plot of studies included in meta‐analysis for questionnaire‐based knowledge
5.
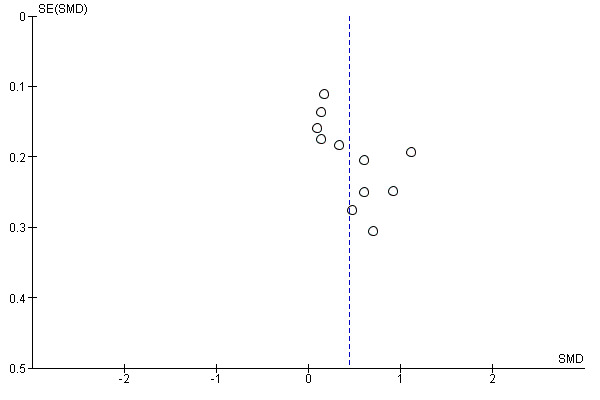
Funnel plot of studies included in meta‐analysis for vignette‐based knowledge
Effects of interventions
See: Table 1
This review sought to assess the evidence of effectiveness of school‐based education programmes for the prevention of child sexual abuse. Specifically, we sought to assess whether: programmes were effective in improving students' protective behaviours and knowledge about sexual abuse prevention; behaviours and skills were retained over time; and programme participation resulted in disclosures of sexual abuse, produced harm, or both. In this section, we present the main findings on the effects of the interventions for six outcomes: (i) protective behaviours; (ii) knowledge (questionnaire‐based knowledge and vignette‐based knowledge); (iii) retention of protective behaviours over time; (iv) retention of knowledge over time; (v) harm (parental or child anxiety or fear); and (vi) disclosures. The analysis results and our GRADE ratings are presented in Table 1.
Protective behaviours
Of the 24 included studies, three studies reported collecting data on protective behaviours (Fryer 1987a; Kraizer 1991; Poche 1988). All used a version of a stranger simulation test involving staging of a simulated abuse or grooming situation with each individual child where a research assistant, posing as a stranger, requested the child's help with a task that required them to go with the stranger (e.g. accompany the stranger to the stranger's car to do a special task). Children's responses were recorded by independent assessors using contemporaneous video monitoring (Fryer 1987a; Kraizer 1991), or by the research assistant (Poche 1988). Scoring was pass or fail. All three studies were conducted with children in lower primary school (kindergarten to grade three).
Only the Fryer 1987a (n = 48; randomised controlled trial (RCT)) and Poche 1988 (n = 74; cluster‐RCT) studies could be included in the meta‐analysis for protective behaviours, as Kraizer 1991 (n = 670; cluster‐RCT) did not report a breakdown of pass or fail scores for intervention and control groups. For the Poche 1988 study, we combined two intervention groups as the self protective knowledge and skills received were considered sufficiently similar to those in Fryer 1987a: teaching rules, group discussion, and practice through role‐play and rehearsal. Data were available for 102 participants. Comparison was with a control group.
In the analysis, heterogeneity approached the moderate range (I² = 27%; Tau² = 0.16) and was non‐significant (P value = 0.24). Protective behaviours were greatly enhanced in intervention groups compared to control groups immediately post‐intervention (odds ratio (OR) 5.71, 95% confidence interval (CI) 1.98 to 16.51; two studies; n = 102) (see Analysis 1.1).
1.1. Analysis.
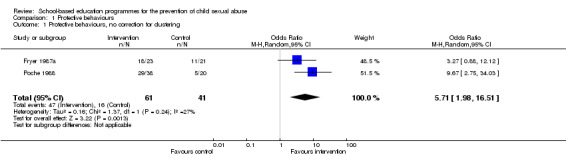
Comparison 1 Protective behaviours, Outcome 1 Protective behaviours, no correction for clustering.
We performed sensitivity analyses to assess the effects of adjusting the Poche 1988 study for cluster‐randomisation. Using this method and an intraclass correlation coefficient (ICC) of 0.1 produced an OR of 5.43 (95% CI 1.88 to 15.65; Analysis 1.2) and an ICC of 0.2 produced an OR of 5.16 (95% CI 1.81 to 14.70; Analysis 1.3). These analyses indicate that adjusting for the effect of clustering have minimal effects on our results.
1.2. Analysis.
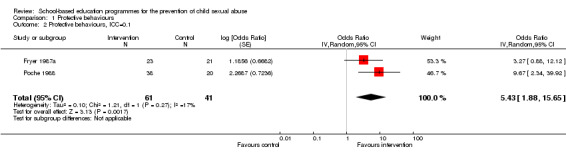
Comparison 1 Protective behaviours, Outcome 2 Protective behaviours, ICC=0.1.
1.3. Analysis.
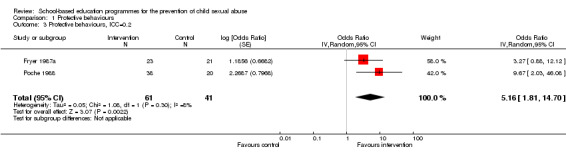
Comparison 1 Protective behaviours, Outcome 3 Protective behaviours, ICC=0.2.
Taken together, results of the more conservative adjustment for clustering show the short‐term (i.e. immediately post‐intervention) superiority of the interventions over control group effects. That is, children who received a school‐based sexual abuse prevention programme were substantially more likely to demonstrate protective behaviours in a simulated situation that was administered immediately after the programme ended.
In addition to the above assessment, Fryer 1987a and Kraizer 1991 assessed the impact of knowledge and self esteem on the use of protective behaviours. Fryer 1987a used the Harter Perceived Competence Scale for Children (HPCS) (Harter 1982), commonly used as a measure of self esteem. Kraizer 1991 used the Battle Culture Free Self‐esteem Inventory (Battle 1981) and the Children Need to Know Knowledge/Attitude Test (CNKKAT) (Kraizer 1981). Results of these measures were reported only for the intervention groups. In both studies, children with high self esteem who had improved knowledge scores post‐intervention were more likely to exhibit protective behaviours. These studies did not report effect sizes to enable assessment of the magnitude of the relationships between self esteem, knowledge, and protective behaviours, although self esteem was identified as a potential "critical path" or moderating variable, which was recommended for further research (Fryer 1987a, p 177).
Knowledge
Questionnaire‐based knowledge
Of the 24 included studies, 21 reported questionnaire‐based knowledge using a range of different measures detailed above. Three of the 21 studies did not provide data in a way that could be included in meta‐analysis (Del Campo Sanchez 2006; Harvey 1988; Kraizer 1991). In three trials, with multiple intervention groups in which interventions were judged to be sufficiently comparable, we combined intervention groups into a single intervention group in the meta‐analysis (Blumberg 1991; Crowley 1989; Dawson 1987). Eighteen studies were included in the meta‐analysis comprising a total of 4657 participants.
In the meta‐analysis, there was evidence of substantial heterogeneity (I² = 84%; Tau² = 0.10). The high Chi² statistic (104.76; df = 17) and low P value (< 0.00001) indicated variation of effect estimates beyond chance. The SMD was 0.61 (95% CI 0.45 to 0.78), reflecting an average 0.61 standard deviation (SD) increase in factual knowledge, across various measures, for the intervention group. These results suggest that children exposed to the interventions tend to display increased factual knowledge about sexual abuse and its prevention, when measured immediately after completion of the programme, and the effect is of a moderate size (see Analysis 2.1).
2.1. Analysis.
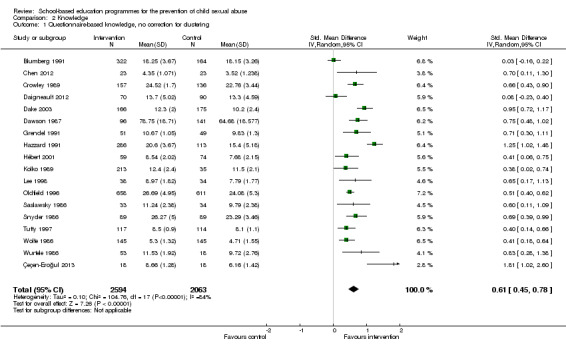
Comparison 2 Knowledge, Outcome 1 Questionnaire‐based knowledge, no correction for clustering.
Of the 18 studies included in this meta‐analysis, 12 were cluster‐randomised studies and all were analysed with unit of analysis errors. Of the cluster‐randomised studies, one was randomised by school district (Kolko 1989), four were randomised by school (Daigneault 2012; Dake 2003; Hazzard 1991; Hébert 2001), and seven by classroom (Blumberg 1991; Crowley 1989; Dawson 1987; Grendel 1991; Oldfield 1996; Snyder 1986; Wolfe 1986). We estimated ICCs, as described above, in sensitivity analyses to adjust for unit of analysis errors. We applied the same ICC to district, school, and class cluster‐RCTs. When adjusted, an ICC of 0.1 produced a SMD of 0.66 (95% CI 0.51 to 0.81; Analysis 2.2) and an ICC of 0.2 produced a SMD of 0.63 (95% CI 0.50 to 0.77; Analysis 2.3). These analyses indicate that adjusting for clustering has very minimal effects on results.
2.2. Analysis.
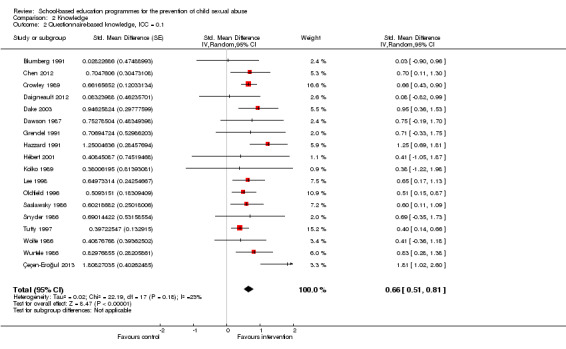
Comparison 2 Knowledge, Outcome 2 Questionnaire‐based knowledge, ICC = 0.1.
2.3. Analysis.
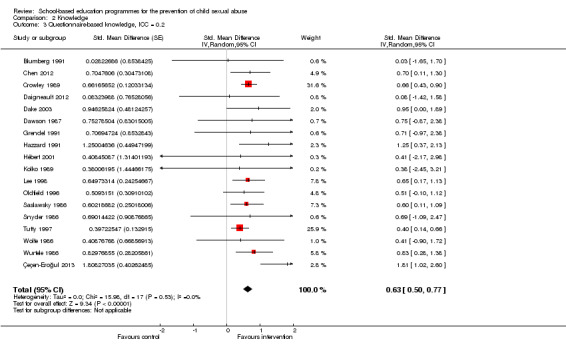
Comparison 2 Knowledge, Outcome 3 Questionnaire‐based knowledge, ICC = 0.2.
We also conducted sensitivity analyses to assess the effects of study exclusion for risk of bias in the two most relevant domains for school‐based studies. First, we examined risk of bias on the blinding of outcome assessment domain. When studies at high risk of bias were excluded (Chen 2012; Crowley 1989; Dake 2003; Dawson 1987; Hazzard 1991; Hébert 2001; Snyder 1986), the SMD was reduced to 0.47 (95% CI 0.29 to 0.66). These results indicate that knowledge scores in these studies may be influenced by assessor bias or contamination from group assessment, or both, such that better controlled studies may generate lower effect sizes in this domain. Second, we examined risk of bias on the attrition bias domain. When studies at high risk of bias were excluded (Blumberg 1991; Crowley 1989; Daigneault 2012; Dake 2003; Grendel 1991; Kolko 1989), the SMD was 0.69 (95% CI 0.59 to 0.88), indicating that children from studies with better follow‐up tended to score somewhat higher in this domain.
We conducted subgroup analyses to assess the effects of participant age. We examined studies in two age‐based subgroups as follows: (i) six studies with only younger participants from kindergarten to grade three (Blumberg 1991; Daigneault 2012; Dake 2003; Grendel 1991; Hébert 2001; Kolko 1989); and (ii) seven studies with only older participants from grade four upwards (Crowley 1989; Dawson 1987; Hazzard 1991; Lee 1998; Snyder 1986; Wolfe 1986; Ҫeҫen‐Eroğul 2013). The SMD was 0.42 (95% CI 0.08 to 0.77) for the younger group and 0.89 (95% CI 0.59 to 1.19) for the older group. The test for subgroup differences was just below the statistically significant cut‐off of 0.05 (Chi² = 4.04, df = 1; P value = 0.04). These results indicate that knowledge may be better gained immediately after the intervention by older children.
Vignette‐based knowledge
Twelve studies used vignette‐based measures in various formats, including verbal, picture, and video vignettes. One study did not report SDs and thus could not be included in a meta‐analysis (Harvey 1988). One study did not report SDs but these could be derived by review authors from other reported statistics to enable inclusion in meta‐analysis (Saslawsky 1986). In Blumberg 1991 and Krahé 2009, we combined two intervention groups into a single intervention group based on our assessment that the interventions were sufficiently similar when compared with other studies. Eleven studies were included in the meta‐analysis with a total of 1688 participants.
There was evidence of substantial heterogeneity (I² = 71%; Tau² = 0.08) in the meta‐analysis. The high Chi² statistic (34.25, df = 10) and low P value (< 0.0002) provide further evidence of variation in effect estimates beyond chance. The SMD was 0.45 (95% CI 0.24 to 0.65) (see Analysis 2.4), indicating that those receiving treatment had an average 0.45 SD increase in applied knowledge as reflected in their responses to vignettes administered post‐intervention, a gain of moderate effect size.
2.4. Analysis.
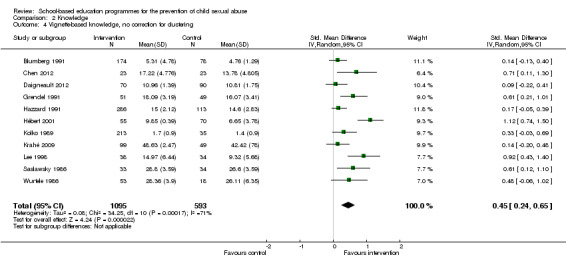
Comparison 2 Knowledge, Outcome 4 Vignette‐based knowledge, no correction for clustering.
Of the 11 studies included in the meta‐analysis, seven studies were of cluster‐randomised design (Blumberg 1991; Daigneault 2012; Grendel 1991; Hazzard 1991; Hébert 2001; Kolko 1989; Krahé 2009). To assess the impact of unit of analysis errors, we conducted sensitivity analyses for estimated ICCs (as above). For an ICC of 0.1, the SMD was 0.53, (95% CI 0.32 to 0.74; Analysis 2.5) and for an ICC of 0.2, the SMD was 0.60 (95% CI 0.31 to 0.89; Analysis 2.6). These analyses suggest that adjusting for clustering has only slight effects on results.
2.5. Analysis.
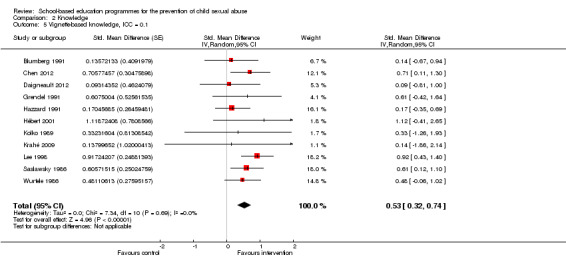
Comparison 2 Knowledge, Outcome 5 Vignette‐based knowledge, ICC = 0.1.
2.6. Analysis.
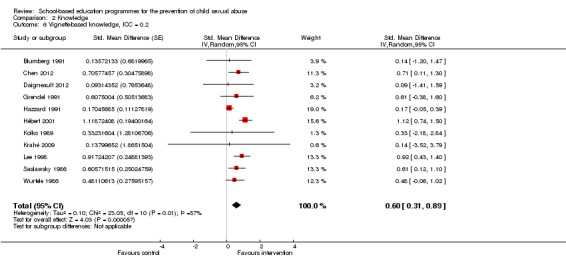
Comparison 2 Knowledge, Outcome 6 Vignette‐based knowledge, ICC = 0.2.
We conducted sensitivity analyses to assess the effects of study exclusion for risk of bias. First, we examined risk of bias on the blinding of outcome assessment domain. When we excluded three studies (Chen 2012; Hazzard 1991; Hébert 2001), the SMD was reduced to 0.36 (95% CI 0.17 to 0.56), indicating a slight testing effect. Second, we examined risk of bias on the attrition bias domain. When we excluded studies at high risk of bias (Blumberg 1991; Daigneault 2012; Grendel 1991; Kolko 1989), the SMD increased to 0.57 (95% CI 0.25 to 0.89), indicating that children from studies with better follow‐up tended to score somewhat higher in this domain.
We conducted subgroup analyses to assess the effects of participant age. We examined studies in two groups: (i) six studies including only participants in kindergarten to grade three (Blumberg 1991; Daigneault 2012; Grendel 1991; Hébert 2001; Kolko 1989; Krahé 2009); and (ii) three studies including only participants in grade four upwards (Chen 2012; Hazzard 1991; Lee 1998). The SMD was 0.39 (95% CI 0.09 to 0.69) for the younger group and 0.56 (95% CI 0.03 to 1.08) for the older group. Thus, older children, on average, may score somewhat better than younger children when they complete these measures of applied knowledge immediately after the intervention. However, the test for subgroup differences was not significant (Chi² = 0.29, df = 1; P value = 0.59).
Retention of protective behaviours over time
Three of the 24 included studies measured retention of protective behaviours over time. Complete data were not available for any of these studies and a meta‐analysis could not be conducted.
Retention of knowledge over time
Questionnaire‐based measures were used in 21 of the 24 included studies. Ten of these studies reported on retention of knowledge over time. Complete data were available for four studies (956 participants) (Dawson 1987; Hazzard 1991; Kolko 1989; Lee 1998). All studies used unique knowledge scales. In three studies, follow‐up periods were one to three months post‐intervention (Dawson 1987; Hazzard 1991; Lee 1998), and in one study, six months post‐intervention (Kolko 1989). These four studies were included in meta‐analysis using a random‐effects model. For comparative purposes we generated two meta‐analyses: one estimating effects for the four studies immediately post‐intervention and one estimating effects at follow‐up. Results suggest that knowledge appeared to deteriorate slightly over time as demonstrated by a decline in the SMD from 0.78 (95% CI 0.38 to 1.17; I² = 84%, Tau² = 0.13, P value = 0.0003) immediately post‐intervention to SMD 0.69 (95% CI 0.51 to 0.87; I² = 25%; Tau² = 0.01, P value = 0.26) at one to three months follow‐up (see Analysis 3.1). However, the test for subgroup differences was not significant (Chi² = 0.14, df = 1; P value = 0.71), suggesting knowledge scores did not deteriorate significantly for intervention or control groups within the one‐ to six‐month follow‐up period.
3.1. Analysis.
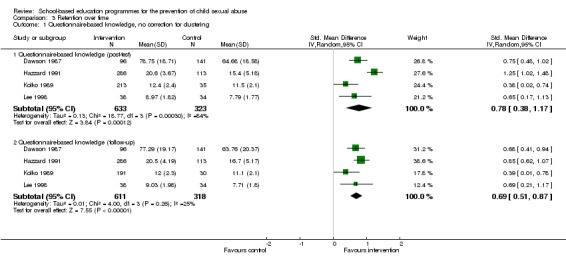
Comparison 3 Retention over time, Outcome 1 Questionnaire‐based knowledge, no correction for clustering.
Of the four studies included in this meta‐analysis, three were cluster‐randomised studies (Dawson 1987; Hazzard 1991; Kolko 1989). Sensitivity analyses, adjusting for clustering yielded very similar results. When adjusted with an ICC of 0.1, knowledge decreased slightly over time as demonstrated by a small decline in the SMD from 0.86 (95% CI 0.53 to 1.20) immediately post‐intervention to 0.73 (95% CI 0.41 to 1.06) at follow‐up (Analysis 3.2). When adjusted with an ICC of 0.2, knowledge decreased slightly over time as demonstrated by a small decline in the SMD from SMD 0.86 (95% CI 0.53 to 1.20) immediately post‐intervention to 0.72 (95% CI 0.32 to 1.11) at follow‐up (Analysis 3.3).
3.2. Analysis.
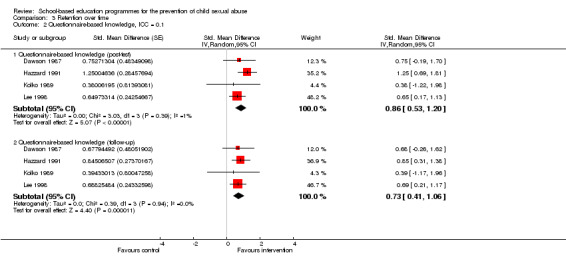
Comparison 3 Retention over time, Outcome 2 Questionnaire‐based knowledge, ICC = 0.1.
3.3. Analysis.
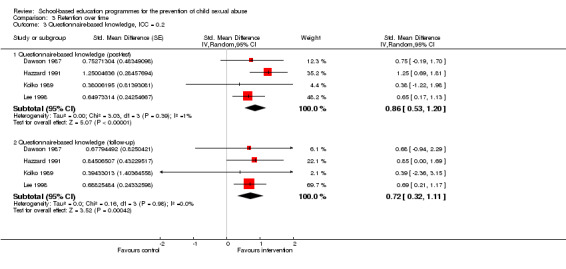
Comparison 3 Retention over time, Outcome 3 Questionnaire‐based knowledge, ICC = 0.2.
Vignette‐based measures were used in 12 of the 24 included studies. Nine of these studies reported on retention of knowledge over time. None of these studies could be included in a meta‐analysis. The reasons for this are twofold: (i) the wait‐list control design of the study meant that the control group received the intervention immediately after the experimental group had finished and, therefore, follow‐up data were unavailable for the control group (Blumberg 1991; Daigneault 2012; Grendel 1991; Hazzard 1991; Saslawsky 1986; Wurtele 1986); or (ii) the study did not provide data in a form useable in meta‐analysis, for example, the study provided a narrative statement or reported summary statistics without providing means and SDs (Hébert 2001; Krahé 2009; Lee 1998). As a narrative synthesis, six studies provided intervention group data only: two studies reported no knowledge gains between post‐test and follow‐up (at five months, Blumberg 1991; at one year, Hazzard 1991), two studies reported maintenance of knowledge gains at two‐month follow‐up (Hébert 2001; Lee 1998), and three studies reported small, but unimportant additional knowledge gains between post‐test and follow‐up (six months, Kolko 1989; three months, Saslawsky 1986; Wurtele 1986).
Harm
A total of six studies had measured harm, but three did not report data in a form that could be used in meta‐analysis (Daigneault 2012; Hazzard 1991; Kraizer 1991). We included three studies (795 participants) in the meta‐analysis for harm in relation to participation in school‐based child sexual abuse prevention programmes (Blumberg 1991; Dawson 1987; Lee 1998). In these studies, harm was measured via child self report anxiety or fear scales, with all studies using unique measures: Dawson 1987 used the State‐Trait Anxiety Inventory for Children (STAIC), Lee 1998 used the Fear Assessment Thermometer Scale (FATS), and Blumberg 1991 used a custom‐made scale. There was no heterogeneity (I² = 0%, P value = 0.79). The SMD was ‐0.08 (95% CI ‐0.22 to 0.07) (see Analysis 4.1). This result reveals evidence of no increases or decreases in anxiety or fear in intervention participants.
4.1. Analysis.
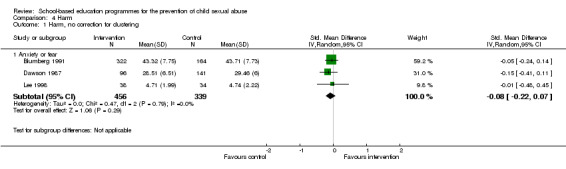
Comparison 4 Harm, Outcome 1 Harm, no correction for clustering.
Two of these three studies were cluster‐randomised studies (Blumberg 1991; Dawson 1987). To assess the impact of unit of analysis errors, we conducted sensitivity analyses for estimated ICCs as above, showing little change in point estimates and slightly widening CIs. For an ICC of 0.1, the SMD was ‐0.04 (95% CI ‐0.42 to 0.33; Analysis 4.2) and for an ICC of 0.2, the SMD was ‐0.03 (95% CI ‐0.46 to 0.40; Analysis 4.3).
4.2. Analysis.
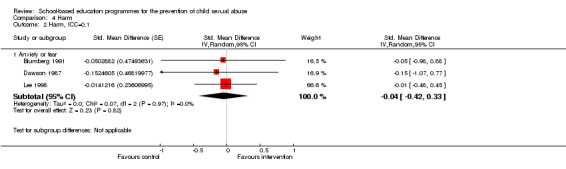
Comparison 4 Harm, Outcome 2 Harm, ICC=0.1.
4.3. Analysis.
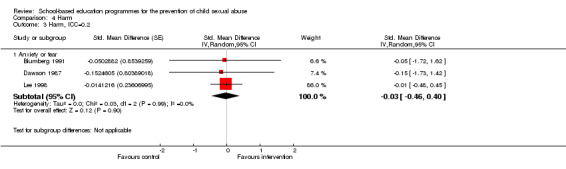
Comparison 4 Harm, Outcome 3 Harm, ICC=0.2.
A narrative synthesis of the studies not included in the meta‐analysis shows that seven studies reported on adverse effects with either child (Hazzard 1991; Kraizer 1991; Oldfield 1996) or parent self reports (Del Campo Sanchez 2006; Hazzard 1991; Hébert 2001; Tutty 1997). Using child self report measures, Hazzard 1991 and Oldfield 1996 reported no important differences in STAIC scores between intervention and control groups (Hazzard 1991, treatment mean 29.7, control mean 29.9; Oldfield 1996, F(1, 593) = 0.05, P value = 0.825). Hazzard 1991 did not report SDs and ANCOVA results. Oldfield 1996 did not report means and SDs. Oldfield 1996 also found no important differences between experimental and control group anxiety scores using the Revised Children's Manifest Anxiety Scale (RCMAS) with younger participants, F(1, 653) = 1.40, P value = 0.248. In one study (Kraizer 1991), children in the intervention group participated in an exit interview (n = 332): 14.8% of the children experienced some anxiety or fear initially but none on programme completion, and 4.5% experienced some anxiety or fear initially and remained a little worried on programme completion.
Using parent self report measures of perceived changes in children's behaviour, Del Campo Sanchez 2006 (n = 193) reported the following in children exposed to the intervention: fear of adults (1%) and increased fighting with peers (1%), but no sleep problems, or rejection of normal affection. Similarly, in intervention group children, Tutty 1997 (n = 231) found worry about scary things happening (1.7%), but no bedwetting, nightmares, crying, rejection of normal affection, or attention seeking behaviour. Hébert 2001 (n = 133) reported intervention group children having increased dependency behaviours (13%), more aggressiveness towards peers (15%) and siblings (29%), and more fearfulness of strangers (25%). Hazzard 1991 (n = 399) reported no important differences between intervention and control group children on parental perceptions of anxiety or fear (summary data not provided).
Disclosure
We included three studies (1788 participants) in the meta‐analysis for disclosures of previous or current sexual abuse (Del Campo Sanchez 2006; Kolko 1989; Oldfield 1996). There was no heterogeneity (I² = 0%, P value = 0.84). Disclosure occurred more often in the intervention group (OR 3.56, 95% CI 1.13 to 11.24). The odds of disclosure were as much as 3.5 times higher in participants exposed to the intervention (see Analysis 5.1).
5.1. Analysis.
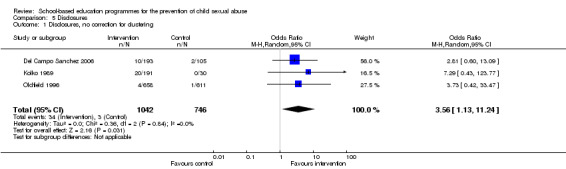
Comparison 5 Disclosures, Outcome 1 Disclosures, no correction for clustering.
We performed sensitivity analyses to assess the effects of adjusting the Kolko 1989 and Oldfield 1996 studies for cluster‐randomisation. Using this method and an ICC of 0.1 produced a non‐significant OR of 3.04, 95% CI 0.75 to 12.33; Analysis 5.2) and an ICC of 0.2 produced an OR of 2.95, 95% CI 0.69 to 12.61; see Analysis 5.3). These analyses, adjusted for unit of analysis errors, indicate that the effect of intervention programmes on disclosure was sensitive to different assumptions regarding the effect of clustering on the results.
5.2. Analysis.
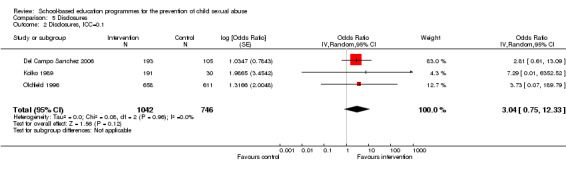
Comparison 5 Disclosures, Outcome 2 Disclosures, ICC=0.1.
5.3. Analysis.
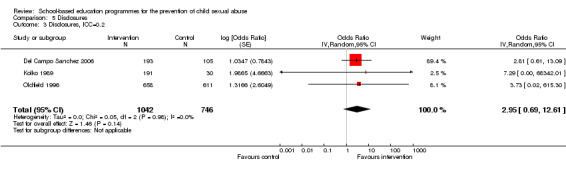
Comparison 5 Disclosures, Outcome 3 Disclosures, ICC=0.2.
Of the studies not included in meta‐analysis, disclosure of past or current abuse was recorded in two studies (Blumberg 1991; Hazzard 1991). One study conducted a search of the files of Child Protective Services (CPS) for names of children in the classrooms who were part of the study (Blumberg 1991). Data event counts were not provided, however the study reported that risk ratios (RR) were calculated for experimental against control conditions. Both ratios "approached 1.0 which one would expect by chance" (Chadwick 1989, p 61). One further study measured disclosures, but was unable to distinguish between treatment and control groups due to data reporting methods (Hazzard 1991). Eight of 526 participants (1.5%) reported ongoing sexual abuse and 20 (3.8%) reported past sexual abuse.
Subgroup analyses
Subgroup analyses are used to compare the mean effect for different subgroups of studies where there are sufficient numbers of studies to allow for meaningful comparisons. We were able to conduct subgroup analyses for age, but only for knowledge outcomes, by categorising studies into two broad groups: younger children and older children as described above. This was because programmes were often delivered to children across multiple consecutive and non‐consecutive school grades. We did not conduct other subgroup analyses in this review because the included studies provided insufficient information about issues that were hypothesised as being relevant for subgroup analysis. In the original study protocol we planned to conduct subgroup analyses for participant age and gender, and programme type and setting (Zwi 2003). We were unable to conduct subgroup analyses for gender owing to poor reporting. We did not conduct subgroup analyses for active or passive involvement as it was not possible to categorise programmes in this way; most were multifaceted, involving both active and passive approaches. What is needed is a way of identifying, more precisely, the range of child, programme, and study design characteristics that may moderate programme effectiveness. We explain this in more detail in the discussion below.
Discussion
Summary of main results
This updated review reported on 24 trials (29 reports) examining the effectiveness of school‐based programmes for the prevention of child sexual abuse. The studies report on data for 5802 child participants of whom 5730 (almost 98.8%) were from primary (elementary) schools. In this review, we assessed programme effectiveness according to six outcomes: (i) protective behaviours; (ii) knowledge (questionnaire‐based knowledge and vignette‐based knowledge); (iii) retention of protective behaviours over time; (iv) retention of knowledge over time; (v) harm manifesting as parental or child anxiety or fear; and (vi) disclosures of past or current child sexual abuse. Below we report on: (i) protective behaviours; (ii) knowledge; (iii) harm; and (iv) disclosures.
Protective behaviours
Meta‐analysis of data from two studies showed significant improvements in protective behaviours in simulated at‐risk situations, measured immediately (up to two weeks) post‐intervention. Follow‐up assessment of protective behaviours was not reported in either of the studies. Simulated situations, used in three of the included studies, were a form of in vivo assessment, which exposed children to potentially stressful situations such as an invitation to go with an unknown adult (Fryer 1987a; Kraizer 1991; Poche 1988). The use of these simulation techniques is difficult to justify and raises important ethical questions about balancing risks against potential benefits for participants. Research of this type also presents significant challenges for voluntary consent where there is active concealment via role‐playing. Although this is arguably as close as researchers can get to testing whether participants' learned skills can be translated into appropriate behaviour, three salient issues must be considered. First, the generalisation of responses from simulated to actual settings cannot be assumed. Second, it is not known if skills taught in the context of approaches from strangers help children deal with threats from familiar adults, who are the most common perpetrators of child sexual abuse. Third, there is the possibility that this type of outcome assessment may desensitise children to similar occurrences in the future. Outcome assessment of this type, therefore, must be rigorously conducted and monitored.
The results of one study suggest that children with greater self esteem (Fryer 1987a), as measured by the Harter Perceived Competence Scale (HPCS) (Harter 1982), exhibited better protective behaviours following intervention. Since self esteem is clinically relevant in child sexual abuse, this finding warrants further investigation to determine whether self esteem training should be included as a component of child sexual abuse prevention interventions. It may be that children with greater self esteem are more likely to display protective behaviours regardless of exposure to programmes. Unfortunately, the psychological literature has been hampered by the use of a confusing array of terms encompassing self esteem (e.g. self belief, self concept, self efficacy, self worth), and there has been extensive debate in the educational psychology literature about its role in children's learning (Valentine 2004). Greater levels of precision in definition and measurement are required in future research.
Knowledge
Meta‐analysis of data from 18 studies for questionnaire‐based knowledge and 11 studies for vignette‐based knowledge suggested gains in factual and applied knowledge immediately (up to two weeks) post‐intervention. Follow‐up assessment of factual knowledge was limited to four studies with our meta‐analyses showing that factual knowledge scores did not deteriorate for either intervention or control groups one to six months after interventions. Follow‐up assessment of applied knowledge was conducted in some studies, however data were incomplete and not suitable for meta‐analysis. Across all of the included studies, less than half of the studies (10 of 24) reported on short‐term knowledge outcomes (within three months of the intervention), three studies reported medium‐term outcomes (up to 12 months post‐intervention), and only one study measured retention of knowledge beyond 12 months. A methodological problem in these studies was data completeness because, at the time of follow‐up, control groups had already been exposed to the programmes and it is unethical to withhold programme delivery. Well‐designed and timely follow‐up is required to determine whether factual and applied knowledge can be sustained over time with the use of boosters and other maintenance strategies (such as reiteration of programme messages by parents and teachers).
An important source of heterogeneity across studies is the knowledge measure used. For the 24 studies included in this review, 15 discrete questionnaire‐based measures and six discrete vignette‐based measures were used to measure children's factual and applied knowledge respectively. For studies included in the meta‐analyses, there were 10 unique questionnaire‐based measures and six unique vignette‐based measures represented. These were pooled using the standardised mean difference (SMD) as a summary statistic. In using SMDs, we treated the different assessment measures as though they were one standardised measure with comparable standard deviations (SDs). It is then difficult to relate this abstract figure back to the original measures to determine what this means in real life. For example, it is not clear what a 0.61 SD increase in factual knowledge or a 0.45 SD increase in applied knowledge translates to in practical knowledge terms. Are these findings sufficient to offer protective effects under threats of sexual abuse? Further research is required to address the magnitude of knowledge improvement required to produce clinically important protective effects. Research would be improved by the use of standardised rather than custom‐made instruments.
Harm
Adverse or negative effects in the form of harm to participants were assessed via measures of child anxiety or fear. Studies examining participants' anxiety or fear were based on child self report and parent report. Meta‐analysis of three studies found no evidence of increased or decreased anxiety or fear in those exposed to programmes and this did not change when adjusted for clustering. Narrative synthesis of included studies revealed that a small proportion of programme participants experienced anxiety or fear but these (anxieties or fears) were mild rather than severe, and short‐ rather than long‐term. There was insufficient information to assess whether harms varied according to participant age or grade level. Although parent satisfaction data were collected in some studies, parental anxiety or fear was not measured in any study. This may be important in future studies for determining the role of parents in moderating programme effects.
Disclosures
The only direct measure of programme effects was participants' disclosures of past or current sexual abuse that were made following interventions. Disclosures were poorly reported or not reported in most studies. Our meta‐analysis of three studies showed greater odds of disclosures by children receiving interventions. However, such disclosures cannot really be considered an adverse event since: (i) the onset of the alleged abuse would have occurred prior to the intervention; (ii) disclosing abuse, while potentially traumatic, can also prompt the provision of treatment; and (iii) the identification and reporting of perpetrators may prevent harm to other children. Details of how disclosures were dealt with were not reported in any of the studies. Appropriate systems for dealing with disclosures are important and must reflect jurisdictional legal reporting obligations (also known as mandatory reporting laws), and school policies for child maltreatment recognition, reporting, and response. Future studies should consider methods for recording and responding to disclosures; data linkage to child protection or police records, or both; and/or interviewing or surveying participants at repeated follow‐up intervals.
Subgroup effects
Demographic characteristics (e.g. participant age, gender, ethnicity, socioeconomic position, and ability level) are potential sources of heterogeneity, and potential effect moderators. If studies do not account for these characteristics, important subgroup effects may be missed. Genuine but unidentified differences in study samples at baseline are potential sources of heterogeneity within and across studies. Baseline characteristics of intervention and control groups were inconsistently and poorly reported in the included studies. Control for baseline characteristics within individual studies is particularly important for criteria that are most relevant to learning such as academic ability, or reading age. These data were not reported or were absent by study design, therefore we were not able to explore whether programme effectiveness varied according to key baseline criteria. These issues have implications for programme delivery.
Demographic characteristics, such as participant age, would appear to be straightforward variables, however, mean age was not reported in eight of 24 included studies and in others was conflated with grade level. Few studies were undertaken with single grades, and most (18 of 24) studies were undertaken with multiple grade levels together. This study design limited the pooling of results across studies in meta‐analysis. Subgroup analyses showed that older children (grades four and above) made greater knowledge gains than younger children (grades kindergarten to three) immediately post‐intervention; results that are congruent with developmental and maturation theories. However, we do not know if younger children would respond differently with differentiated approaches (e.g. reinforcement of skills and knowledge by parents or teachers, or both). We were unable to assess programme effectiveness according to other potentially important participant variables (e.g. child gender, ethnicity, socioeconomic position, and ability level) as few studies reported on these data or provided subgroup effects.
Characteristics of effective programmes
Insufficient data were provided to evaluate the specific effects of programme type, duration, frequency, or setting. These programme characteristics have implications for delivery in schools and the ideal constellation of programme characteristics, which is not yet known. Although there was insufficient information to develop programme typologies and compare effects, we noted that approximately half of the programmes in included studies used content, such as the teaching of safety rules (e.g. "my body belongs to me"), and prevention concepts (e.g. distinguishing appropriate and inappropriate touches), and the use of delivery methods such as discussion, modelling, role‐play, rehearsal, and feedback. Our narrative synthesis of included studies documented multidimensionality in intervention contents, methods, and delivery. This is an important finding in itself. To date, programmes have been categorised dichotomously as active or passive or behavioural or instructional. Our descriptive analysis shows this categorisation to be somewhat artificial as most programmes in this review were multifaceted with multiple components. Programmes covered multiple topics (e.g. body safety rules, distinguishing types of touches, reporting abuse to adults who can help), used teaching strategies in combination (e.g. discussion, modelling, role‐play, rehearsal, and feedback), and integrated active or passive and behavioural or instructional approaches in one session (e.g. a video or DVD presentation encouraged children to listen and then partake in activities). The contribution to effectiveness of programme content, methods, and delivery will require documentation using standardised data collection tools in future studies.
The duration and frequency (dose) of programme interventions varied from one single 45‐minute session to eight 20‐minute sessions. There were insufficient studies to create subgroup analyses for total programme hours, or total number of sessions, or for the presence or absence of booster sessions or reinforcement strategies.
While interventions appear to increase protective behaviours and knowledge about sexual abuse, it is important that this learning is not seen as a replacement for adult responsibility to ensure child safety. Nor should education replace the need for appropriate medical and legal handling of those affected by child sexual abuse. We do not have evidence that these programmes reduce the incidence of child sexual abuse. The findings of this review need to be considered in the context of complementary prevention initiatives. Current child sexual abuse prevention frameworks suggest that strategies must not only target children, but must work on multiple elements of children's social systems to prevent abuse from occurring in the first place, namely at the level of the family, community, and society (Smallbone 2008).
Overall completeness and applicability of evidence
Studies were conducted in countries with high and upper‐middle income economies according to the World Bank's analytical income categories (The World Bank 2013). Most (16 of 24) were conducted in North America, the remainder in Europe, East Asia, and Central Asia. Ethnicity data were poorly or not reported in 10 of the 24 studies. Where data were reported, participants were from a diverse range of ethnicities, increasing the generalisability of the evidence, and also suggesting that concern about child sexual abuse prevention and the delivery of programmes in schools is a wide‐spread phenomenon. Whether similar effects would be seen when programmes are implemented in countries not included is unknown.
All but one of the included studies was conducted in primary (elementary) school settings. There are several possible reasons for this. First, policy makers and school authorities may truly recognise that the age of greatest vulnerability is within the earlier school years (7 to 12 years according to Finkelhor 1986). Second, from our searches, we gleaned that programmes for secondary (high) school students tended to be broader in scope and focused on the prevention of relationship and dating violence, sexually coercive peer relationships, sexual harassment, or sexual assault (see Fellmeth 2013). The purpose of these programmes was not predominantly prevention of child sexual abuse, the focus of this review. In our searches we noted a sizeable group of studies based in preschool settings, the effectiveness of which requires further scrutiny in a separate systematic review given that these programmes have qualitatively different delivery methods and contents, including greater parental participation, which we infer may have a mediating effect.
None of the included studies investigated the effectiveness of a web‐based or online programme. This may be because rigorous programme evaluations have not yet been developed, conducted, or published. Online programmes offer the potential for technology to capture real‐time evaluation data from children as they experience online interventions.
As noted above, the completeness and applicability of evidence was limited by methodology and failure to report the full range of child, intervention, and study design characteristics that could possibly account for variations in programme effects. In the period since the original review was conducted (Zwi 2007), Cochrane Reviews have become more rigorous in identifying methodological limitations in trials via risk of bias analyses, and the CONSORT statement has been developed to provide guidance on the reporting of randomised controlled trials (Shulz 2010). Nevertheless, the methodological quality of trials has not improved substantially. No study in this area has yet published a study protocol, and we found no clinical trials register records pertaining to studies of this type. Researchers must continue testing these interventions, but use study design methodology, data collection tools, registration, and reporting guidelines that enable rigorous scientific evaluation.
Quality of the evidence
Table 1 presents the quality of evidence for each outcome of interest. We downgraded the quality of evidence to moderate quality either due to risk of bias, imprecision, or because of the impact of adjusting for the effect of clustering within some of the studies. Most studies in this review were at an unclear risk of selection bias as illustrated in Figure 1 and Figure 2, due to inadequate information regarding methods of random sequence generation and allocation concealment. Studies which randomised classes within a single school to intervention and control groups were at high risk of contamination effects owing to the interaction of children in school playgrounds, friendship groups and families, and also from chance exposure to programme concepts via teachers and other school staff familiar with programme contents. In addition, there was detection bias due to inadequate or unclear assessor, participant and personnel blinding, and inadequate or unclear reporting of attrition for assessments at post‐test and follow‐up. Double‐blinding to minimise performance bias is seldom possible in school‐based trials as group membership is obvious to participants, programme facilitators, and school staff. Blinding of staff responsible for assessing study outcomes can be controlled with careful planning and implementation. This would be particularly effective where outcome assessments are administered with children individually. However, group administration of self report questionnaires or vignette measures may be more susceptible to bias when used with younger participants who are not yet able to read independently. Alternative administration methods, including the use of digital devices and animations, may go some distance to minimising detection bias.
In 14 of the included studies children were randomised in groups of classrooms, schools, or school districts for ease of implementation. However, the appropriate analysis for cluster‐randomisation was not used in any of the studies resulting in potential for overestimation of the effects of interventions. Initial analyses do not take account of unit of analysis errors that occurred in at least half of the studies in each meta‐analysis. ICCs used in the meta‐analysis are imputed and may not be appropriate for all of the studies included. Therefore, results might have differed had the true ICCs from these studies been available, or had cluster‐adjusted results been provided by the authors. Furthermore, the same ICC was used for studies that had undertaken cluster‐randomisation at class, school, and district level, which could further overestimate the magnitude of the findings.
Potential biases in the review process
In producing this review our aim was to provide an unbiased appraisal of the evidence available. We have attempted, therefore, to be comprehensive in our reporting and transparent in our methodology. The review was conducted in line with criteria in the published protocol (Zwi 2003), and where we deviated from these criteria to accommodate updates in Cochrane review methods or advances in the field, we have documented this in the subsection on Differences between protocol and review. The methodological decision to produce each meta‐analysis was complex, involving a balance between the quest for an easily digestible summary of the information, and the danger of applying results when significant methodological caveats exist. We present the meta‐analyses with accompanying cautions as outlined above, and invite debate and comments regarding the route we have chosen.
Agreements and disagreements with other studies or reviews
Five previous meta‐analyses of sexual abuse prevention programmes exist as noted in Table 2, including the original version of this review (Zwi 2007). Our review differs from previous reviews in that it assesses a broader range of outcomes, applies more rigorous inclusion criteria to select high quality studies, and excludes preschool programmes. Further, all previous reviews included studies with control groups but did not apply randomisation criteria, therefore unlike our review, previous reviews included controlled before‐and‐after studies. All previous reviews have found medium to large effects for knowledge outcomes in favour of intervention groups. These effect sizes ranged from 0.57 (Heidotting 1994, 18 studies), through 0.71 (Rispens 1997, 16 studies) and 0.90 (Berrick 1992, 13 studies) to 1.07 (Davis 2000, 27 studies). Our previous review found a SMD of 0.59 (95% confidence interval (CI) 0.44 to 0.74; nine studies, n = 3022) for the questionnaire‐based knowledge outcome, which is the outcome most comparable to the outcomes reported in previous reviews. The current review found a SMD of 0.61 (95% CI 0.45 to 0.78; 18 studies, n = 4657).
Davis 2000 attempted subgroup analyses to examine moderator effects: age (mean age was divided into three groups: three to five years, 5.1 to eight years, older than eight years of age), level of participation (participation was analysed at three different levels: physical participation, verbal participation, no participation), and number of sessions (three subsets: one session, two to three sessions, more than three sessions). Due to inadequate reporting of study data, we were unable to replicate these meta‐analyses, and would caution against using the broad variable of participation as the only marker for programme variation. Given that most programmes include multiple participatory opportunities, often in combination, it may be more informative to develop and explore the effects of multidimensional programme typologies as noted above.
Authors' conclusions
Implications for practice.
Our overall interpretation is that there is moderate quality evidence that school‐based programmes for the prevention of child sexual abuse, of the types described in this review, are effective in increasing primary (elementary) school‐aged children's protective behaviours and knowledge immediately post‐intervention. Knowledge scores did not deteriorate for intervention participants one to six months after programme participation, signalling that booster sessions or other maintenance strategies for reinforcement of key messages remain appropriate follow‐up strategies. Retention of knowledge should be measured beyond six months. It appears that older children make greater knowledge gains than younger children when tested using questionnaire‐based measures, but not when using vignette‐based measures, indicating the need for caution when interpreting study findings. None of the included studies evaluated programmes delivered via electronic means. On balance of evidence, programmes do not appear to increase or decrease children's fear or anxiety, and may result in greater odds of disclosures of past or current sexual abuse from children who have been programme participants, however results are uncertain because of inappropriate data analysis in individual studies. Hence, there is a need for ongoing monitoring of both positive and negative short‐ and long‐term effects of programmes in more rigorous studies with more detailed reporting of potential moderators of programme effects in the form of child, programme, and contextual characteristics.
Currently, schools implement a variety of interventions aimed at preventing child sexual abuse. It is likely that these interventions will be most useful as part of wider community initiatives promoting the safety of children, the contents, processes, and outcomes of which must be clearly defined and measured in rigorous evaluation designs. Furthermore, children's increased knowledge of abuse should not be seen as a replacement for society's responsibility to ensure child safety. It must be emphasised that increasing children's knowledge in this area does not mean they are in any way responsible for abuse, which might then occur by their not being able to apply this knowledge in an actual abuse situation. Even if successful in only a small proportion of situations, given the prevalence of child sexual abuse, it is possible that the skills and knowledge learned in prevention programmes may be of assistance to a considerable number of children.
Implications for research.
Further evidence is required to assess the effectiveness of school‐based programmes for the prevention of child sexual abuse. The current evidence is primarily focused on improvements in participants' skills (protective behaviours) and knowledge (both factual and applied knowledge), and to a lesser extent on assessing harm (child anxiety or fear) and disclosures of past or current child sexual abuse. Further research is needed to investigate the links (if any) between programme participation and actual prevention of child sexual abuse. This will require large cohort studies with repeated follow‐up into adulthood. However, even large cohort studies may not provide definitive evidence for changes in child sexual abuse incidence, as it is under‐identified and difficult to prove. Further research is also required to address uncertainties about the magnitude of skill or knowledge improvement (or both) that can (if at all) translate to clinically important protective effects. Such evidence is a necessary precursor to assessing programmes' cost‐effectiveness.
Ongoing research is needed to more rigorously evaluate programmes. Research to date suggests several categories of factors that may influence programme effectiveness, such as child factors, including family microsystem factors; programme factors, including school contextual factors; and evaluation design factors (Heidotting 1994; Rispens 1997). These require further investigation in well‐designed experimental studies. Many demographic and other independent variables were poorly reported in the included studies. Reliable evidence of this type will advance assessment of programmes' cultural sensitivity, and the appropriateness of programmes for groups of children considered at greater risk. Future evaluations must be more comprehensive, use valid, reliable, standardised measures, and be more precisely reported, according to evidence‐based guidelines for reporting of clinical trials such as the CONSORT (Consolidated Standards of Reporting Trials) Statement (Shulz 2010).
Further investigation of programme contents, methods, and delivery is required with a view to developing programme typologies that can incorporate the programmes' multidimensionality. To this end, typologies should be developed that capture variables emerging as important in newly developed frameworks for child sexual abuse prevention (Smallbone 2008), such as the extent and nature of parent, teacher, and community education components within programmes.
Future studies should address problems with study design, in particular unit of analysis errors in cluster‐randomised trials. Studies where cluster‐randomisation is used should adjust results with appropriate statistical methods, and publish intra‐class correlation coefficients (ICCs) (Campbell 2004). It may then be possible for meta‐analyses to be more robust, and to overcome inadequate sample size and study power to test for differences in child characteristics and intervention types. Other design features that warrant particular attention in future studies include those domains associated with risk of bias: randomisation of study participants, allocation concealment, blinding of outcome assessors, reporting of attrition, and analysis based on intention‐to‐treat (ITT). Longer follow‐up periods for measurement of study outcomes beyond six months are essential to monitor maintenance effects.
What's new
| Date | Event | Description |
|---|---|---|
| 11 February 2015 | New citation required but conclusions have not changed | We added 10 additional trials. We excluded one trial from the original review. |
| 11 February 2015 | New search has been performed | We conducted an updated search for new studies. |
History
Protocol first published: Issue 3, 2003 Review first published: Issue 3, 2007
| Date | Event | Description |
|---|---|---|
| 25 October 2013 | New search has been performed | Full update. |
| 12 November 2008 | Amended | Converted to new review format. |
| 22 May 2007 | Amended | Minor update. |
| 10 May 2007 | New citation required and conclusions have changed | Substantive amendment. |
Notes
This review is co‐registered within the Campbell Collaboration.
Acknowledgements
In the original review, Danielle M Wheeler acknowledged support from the Financial Markets Foundation for Children and the Nordic Campbell Centre. Dr Andrew Hayen (Australia) and Dr Roger Harbord (UK) provided much valued statistical advice.
In the review update, Kerryann Walsh was funded by a Queensland University of Technology Vice Chancellor's Research Fellowship (2010 to 2012) and acknowledges the Australian Research Council Discovery Projects scheme (DP1093717). Pauline Mulligan and Leisa Brandon provided much valued research assistance. The Australasian Cochrane Centre provided training and review completion workshops.
The authors are especially grateful for the comments of external Cochrane reviewers and statisticians, and for the expert advice from the Cochrane Developmental, Psychosocial and Learning Problems Group editorial base: Professor Geraldine MacDonald (Co‐ordinating Editor), Dr Joanne Wilson (Managing Editor), Gemma O'Loughlin (Assistant Managing Editor), and Margaret Anderson (Trials Search Co‐ordinator) who conducted the searches for this review update. The authors also wish to thank Laura MacDonald, former Managing Editor, Cochrane Developmental, Psychosocial, and Learning Problems Group, for her support during development of the update of this review.
Appendices
Appendix 1. Search strategies for the period 2006 to 2014
CENTRAL 2014, Issue 8, last searched 8 September 2014, limited to publication years 2013 to 2014 (47 records)
Previous searches
CENTRAL 2013(9), searched 2 September 2013, limited to publication years 2012 to 2013 (19 records) CENTRAL 2012(3), searched 4 April 2012, limited to publication years 2006 to 2012 (160 records)
#1 MeSH descriptor Child Abuse, Sexual, this term only
#2 MeSH descriptor Rape, this term only
#3 MeSH descriptor Incest, this term only
#4 MeSH descriptor Sex Offenses, this term only
#5 molest* or rape* or incest*
#6 sex* near/3 (crim* or abuse* or assault* or offen* or exploit* or victim* or coerc* or maltreat*)
#7 (groom* near/3 (child* or online or sex*))
#8 (online near/3 solicit)
#9 (#2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8)
#10 MeSH descriptor Adolescent, this term only
#11 child NEAR MEsh
#12 (child* or boy* or girl* or adolescen* or teen* or youth* or young NEXT people or young NEXT person* OR school* or pupil* or student* or college*)
#13 (#10 OR #11 OR #12)
#14 (#9 AND #13)
#15 (#1 OR #14)
Ovid MEDLINE(R) 1946 to August Week 4 2014, last searched 8 September 2014 (160 records)
Previous searches
1946 to August Week 3 2013, searched 2 September 2013 (258 records) 1946 to March Week 3 2012, searched 4 April 2012 (757 records)
1 Child Abuse, Sexual/
2 sex offenses/
3 rape/
4 incest/
5 molest$.tw.
6 rape$.tw.
7 incest$.tw.
8 (sex$ adj3 crim$).tw.
9 (sex$ adj3 abuse$).tw.
10 (sex$ adj3 assault$).tw.
11 (sex$ adj3 offen$).tw.
12 (sex$ adj3 exploit$).tw.
13 (sex$ adj3 victim$).tw.
14 (sex$ adj3 coerc$).tw.
15 (sex$ adj3 maltreat$).tw.
16 (groom$ adj3 (online or child$ or sex$)).tw.
17 (online adj3 solicit$).tw.
18 or/2‐17
19 exp child/
20 adolescent/
21 (child$ or boy$ or girl$ or adolescen$ or teen$ or youth$ or young people or young person$ or pupil$ or student$ or school$ or college$).tw.
22 or/19‐21
23 18 and 22
24 1 or 23
25 randomized controlled trial.pt.
26 controlled clinical trial.pt.
27 randomi#ed.ab.
28 placebo$.ab.
29 drug therapy.fs.
30 randomly.ab.
31 trial.ab.
32 groups.ab.
33 or/25‐32
34 exp animals/ not humans.sh.
35 33 not 34
36 24 and 35
37 limit 36 to yr="2006 ‐Current" [limits applied April 2012]
38 limit 36 to ed=20120301‐20130902 [limits applied Sept 2013]
39 limit 36 to ed=ed=20130901‐20140908 [limits applied Sept 2014]
EMBASE (OVID) 1980 to 2014 Week 36, searched 8 September 2014 (320 records)
Previous searches
1980 to 2013 Week 35, searched 2 September 2013 (400 records)
1980 to 2012 Week 13, searched 4 April 2012 (1118 records)
1 child sexual abuse/
2 exp sexual crime/
3 rape$.tw.
4 incest$.tw.
5 (sex$ adj3 offen$).tw.
6 (sex$ adj3 abus$).tw.
7 (sex$ adj3 assault$).tw.
8 (sex$ adj3 molest$).tw.
9 (sex$ adj3 coerc$).tw.
10 (sex$ adj3 crim$).tw.
11 (sex$ adj3 victim$).tw.
12 (sex$ adj3 exploit$).tw.
13 (sex$ adj3 maltreat$).tw.
14 (groom$ adj3 (online or child$ or sex$)).tw.
15 (online adj3 solicit$).tw.
16 or/2‐15
17 exp child/
18 adolescent/
19 (child$ or school$ or boy$ or girl$ or adolescen$ or teen$ or youth$ or young people or young person$ or pupil$ or student$ or college$).tw.
20 17 or 18 or 19
21 16 and 20
22 1 or 21
23 exp Clinical trial/
24 Randomized controlled trial/
25 Randomization/
26 Single blind procedure/
27 Double blind procedure/
28 Crossover procedure/
29 Placebo/
30 Randomi#ed.tw.
31 RCT.tw.
32 (random$ adj3 (allocat$ or assign$)).tw.
33 randomly.ab.
34 groups.ab.
35 trial.ab.
36 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw.
37 Placebo$.tw.
38 Prospective study/ (248367)
39 (crossover or cross‐over).tw.
40 prospective.tw.
41 or/23‐40
42 22 and 41
43 limit 42 to yr="2006 ‐Current" [limits applied April 2012]
44 limit 42 to em=201214‐201335 [limits applied Sept 2013]
45 limit 42 to em=201335‐201436 [limits applied Sept 2014]
PsycINFO (OVID) 1967 to September Week 1 2014 (102 records)
Previous searches 1967 to August Week 4 2013, last searched 2 September 2013 (118 records) 1967 to March Week 4, searched 4 April 2012 ( 378 records)
1 exp sexual abuse/ 2 sex offenses/ 3 molest$.tw. 4 rape$.tw. 5 incest$.tw. 6 (sex$ adj3 crim$).tw. 7 (sex$ adj3 abuse$).tw. 8 (sex$ adj3 assault$).tw. 9 (sex$ adj3 offen$).tw. 10 (sex$ adj3 exploit$).tw. 11 (sex$ adj3 victim$).tw. 12 (sex$ adj3 coerc$).tw. 13 (sex$ adj3 maltreat$).tw. 14 (groom$ adj3 (online or child$ or sex$)).tw. 15 (online adj3 solicit$).tw. 16 or/1‐15 17 ("100" or "160" or "180" or "200").ag. 18 (child$ or boy$ or girl$ or adolescen$ or teen$ or youth$ or young people or young person$ or pupil$ or student$ or school$ or college$).tw. 19 17 or 18 20 16 and 19 21 clinical trials/ 22 (randomis$ or randomiz$).tw. 23 (random$ adj3 (allocat$ or assign$)).tw. 24 ((clinic$ or control$) adj trial$).tw. 25 ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw. 26 (crossover$ or "cross over$").tw. 27 random sampling/ 28 Experiment Controls/ 29 Placebo/ 30 placebo$.tw. 31 exp program evaluation/ 32 treatment effectiveness evaluation/ 33 ((effectiveness or evaluat$) adj3 (stud$ or research$)).tw. 34 school based intervention/ 35 or/21‐34 36 20 and 35 37 limit 36 to yr="2006 ‐Current" [limits applied April 2012] 38 limit 36 to up=20120301‐20130902 [limits applied Sept 2013] 39 limit 36 to up=20130901‐20140908 [limits applied Sept 2014]
CINAHL (EBSCOhost) 1937 to current, last searched 8 September 2014 and limited to EM 20130901 onwards (98 records)
Previous searches
1937 to current, searched 2 September 2013 and limited to EM 20120301 onwards (201 records) 1937 to current, searched 4 April 2012 and limited to EM 20060801 onwards (526 records)
S38 S19 and S37
S37 S20 or S21 or S22 or S23 or S24 or S25 or S26 or S27 or S28 or S29 or S30 or S31 or S32 or S33 or S34 or S35 or S36
S36 (MH "Evaluation Research") OR (MH "Summative Evaluation Research") OR (MH "Program Evaluation")
S35 (MH "Treatment Outcomes")
S34 (MH "Comparative Studies")
S33 TI (compar* stud* or compar* research*) or AB (compar* stud* or compar* research*) or TI (evaluat* study or evaluat* research) or AB (evaluate* study or evaluat* research) or TI (effectiv* study or effectiv* research) or AB (effectiv* study or effectiv* research) OR TI (prospectiv* study or prospectiv* research) or AB(prospectiv* study or prospectiv* research) or TI (follow‐up study or follow‐up research) or AB (follow‐up study or follow‐up research)
S32 "cross over*"
S31 crossover*
S30 (MH "Crossover Design")
S29 (tripl* N3 mask*) or (tripl* N3 blind*)
S28 (trebl* N3 mask*) or (trebl* N3 blind*)
S27 (doubl* N3 mask*) or (doubl* N3 blind*)
S26 (singl* N3 mask*) or (singl* N3 blind*)
S25 (clinic* N3 trial*) or (control* N3 trial*)
S24 (random* N3 allocat* ) or (random* N3 assign*)
S23 randomis* or randomiz*
S22 (MH "Meta Analysis")
S21 (MH "Clinical Trials+")
S20 MH random assignment
S19 S1 or S18
S18 S14 and S17
S17 S15 or S16
S16 (child* or schoolchild* or schoolboy* or schoolgirl* or adolescen* or teen* or youth* or young people or young person* or pre‐school* or preschool* or pupil* or student* or kindergarten*)
S15 AG adolescent or AG child
S14 S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11 or S12 or S13
S13 (groom* N3 online) or (groom* N3 child*) or (groom* N3 sex*)
S12 (online N3 solicit*)
S11 (sex* N3 maltreat*)
S10 (sex* N3 coerc*)
S9 (sex* N3 victim*)
S8 (sex* N3 exploit*)
S7 (sex* N3 offen*)
S6 (sex* N3 assault*)
S5 (sex* N3 abuse*)
S4 (sex* N3 crim*)
S3 rape* or incest* or molest*
S2 (MH "Rape") OR (MH "Incest")
S1 (MH "Child Abuse, Sexual")
Social Science Citation Index (SSCI), 1970 to 29 August 2014, last searched 8 September 2014, limited to publication years 2013 to 2014 (777 records)
Previous searches 1970 to 30 August 2013, last searched 2 September 2013, limited by Processing Date 2012‐03‐01 to 2013‐09‐02 (661 records) 1970 to 30 March 2012, searched 4 April 2012, no limits applied as not searched for original review (4543 records)
# 7 #6 AND #5 AND #4
# 6 TS=(random* or control* or trial* or group* or blind* or RCT )
# 5 TS= (child* or boy* or girl* or adolescen* or teen* or youth* or "young person*" or "young people" OR school* or college* OR pupil* or student*)
# 4 #3 OR #2 OR #1
# 3 TS=(online* NEAR/3 solicit*)
# 2 TS=((groom*) NEAR/3 (online* OR child* or sex*))
# 1 TS= ((sex*) NEAR/3 (crime or crimes or abus* OR assault* or offenc* or offens* or exploit* or victim* or coerc* or maltreat*))
Sociological Abstracts (ProQuest), 1952 to current, last searched 3 September 2013, limited by publication year 2012 to current (91 records)
Previous searches 25 July 2012, limited to publication year 2006 to 2012 ( 242 records)
(TI(molest* OR rape* OR incest*) OR AB(molest* OR rape* OR incest*) OR TI((groom* NEAR/3 (child* OR online OR sex*)) OR (online NEAR/3 solicit)) OR AB((groom* NEAR/3 (child* OR online OR sex*)) OR (online NEAR/3 solicit)) OR AB (sex* NEAR/3 (crim* OR abuse* OR assault* OR offen* OR exploit* OR victim* OR coerc* OR maltreat*)) OR TI(sex* NEAR/3 (crim* OR abuse* OR assault* OR offen* OR exploit* OR victim* OR coerc* OR maltreat*)) OR SU.EXACT(Child Sexual Abuse) OR SU.EXACT("Incest")) AND (AB(child* OR school* OR kindergarten* OR boy* OR girl* OR adolescen* OR teen* OR youth* OR "young people" OR "young person*" OR preschool* OR "pre‐school*" OR pupil* OR student* OR college*) OR TI(child* OR school* OR kindergarten* OR boy* OR girl* OR adolescen* OR teen* OR youth* OR "young people" OR "young person*" OR preschool* OR "pre‐school*" OR pupil* OR student* OR college*)) AND (AB(random* OR group* OR trial* OR control* OR placebo* OR prospective OR "cross over" OR crossover OR blind* OR RCT) OR TI(random* OR group* OR trial* OR control* OR placebo* OR prospective OR "cross over" OR crossover OR blind* OR RCT))
Conference Proceedings Citation Indexes (CPCI‐S and CPCI‐SSH), 1990 to 29 August 2014, last searched 8 September 2014 (7 records)
Previous searches 1990 to 30 August 2013, searched 2 September 2013 (15 records) 1970 to 30 March 2012, searched 4 April 2012, no limits applied as not searched for original review. (221 records)
#7 #6 AND #5 AND #4
# 6 TS=(random* or control* or trial* or group* or blind* or RCT )
# 5 TS= (child* or boy* or girl* or adolescen* or teen* or youth* or "young person*" or "young people" OR school* or college* OR pupil* or student*)
# 4 #1 OR #2 OR #1
# 3 TS=(online* NEAR/3 solicit*)
# 2 TS=((groom*) NEAR/3 (online* OR child* or sex*))
# 1 TS= ((sex*) NEAR/3 (crime or crimes or abus* OR assault* or offenc* or offens* or exploit* or victim* or coerc* or maltreat*))
ERIC (EBSCOhost), 1966 to current, last searched 8 September 2014, limited by entry date = 1 January 2013 or later ( 206 records)
S22 S12 AND S15 AND S21 S21 S16 OR S17 OR S18 OR S19 OR S20 S20 random* OR intervention* OR experiment* OR trial* S19 ((evaluat* OR compar* OR blind*) N5 (study OR studies OR research)) S18 "follow up" or followup S17 prospective S16 ((DE "Control Groups" OR DE "Longitudinal Studies" OR DE "Program Effectiveness" OR DE "Program Evaluation" OR DE "Experimental Groups") OR (DE "Followup Studies")) OR (DE "Comparative Analysis") S15 S13 OR S14 S14 (child* OR boy* OR girl* OR adolescen* OR teen* OR youth* OR "young person*" OR "young people" OR school* OR college* OR pupil* OR student*) S13 DE "Children" OR DE "Preadolescents" OR DE "Young Children" OR DE "Preschool Children" OR DE "Adolescents" S12 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 S11 (groom* N3 online) or (groom* N3 child*) or (groom* N3 sex*) S10 (online N3 solicit*) S9 (sex* N3 maltreat*) S8 (sex* N3 coerc*) S7 (sex* N3 victim*) S6 (sex* N3 exploit*) S5 sex* N3 offen* S4 (sex* N3 assault*) S3 (sex* N3 abuse*) S2 (sex* N3 crim*) S1 (DE "Sexual Abuse" OR DE "Child Abuse" OR DE "Rape")
ERIC (ProQuest), 1966 to current, last searched 3 September 2013, limited by PY=2012‐2013 ( 206 records)
Previous searches 1966 to current, searched 15 May 2012, limited to entry date 2006 or later, (1357 records)
(("sex* coerc*" OR "sex* crim*" OR "sex* molest*" OR "sex* assault*" OR "sex* abus*" OR "sex* offen*" OR "sex* victim*" OR "sex* maltreat*" OR incest* OR rape*) OR (SU.EXACT("Sexual Abuse") OR SU.EXACT("Child Abuse") OR SU.EXACT("Rape"))) AND (SU.EXACT("Longitudinal Studies") OR SU.EXACT("Control Groups") OR SU.EXACT("Program Effectiveness") OR SU.EXACT("Experimental Groups") OR SU.EXACT("Followup Studies") OR SU.EXACT("Comparative Analysis") OR prospective OR "follow up" OR ((evaluat* OR compar* OR blind*) NEAR/5 (study OR studies OR research)) OR ((compar* OR control*) NEAR/5 group*) OR random* OR intervention* OR experiment* OR trial*) AND (child* OR boy* OR girl* OR adolescen* OR teen* OR youth* OR "young person*" OR "young people" OR school* OR college* OR pupil* OR student*)
DARE, 2014 (3), part of The Cochrane Library , last searched 8 September 2014 (6 records)
Previous searches
DARE 2013(3), searched 2 September 2013 (5 records) DARE 2012(2), searched 4 April 2012 ( 2 records)
#1 MeSH descriptor Child Abuse, Sexual, this term only
#2 MeSH descriptor Rape, this term only
#3 MeSH descriptor Incest, this term only
#4 MeSH descriptor Sex Offenses, this term only
#5 molest* or rape* or incest*
#6 sex* near/3 (crim* or abuse* or assault* or offen* or exloit* or victim* or coerc* or maltreat*)
#7 (groom* near/3 (child* or online or sex*))
#8 (online near/3 solicit)
#9 (#2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8)
#10 MeSH descriptor Adolescent, this term only
#11 child NEAR MEsh
#12 (child* or boy* or girl* or adolescen* or teen* or youth* or young NEXT people or young NEXT person* OR school* or pupil* or student* or college*)
#13 (#10 OR #11 OR #12)
#14 (#9 AND #13)
#15 (#1 OR #14)
NDLTD (SCIRUS)ndltd.org/serviceproviders/scirus‐etd‐search, last searched 3 September 2013 (no new records). Not available in September 2014 and no longer available via SCIRUS
Previous searches 4 April 2013, all available years (9 records)
title:sex* AND title:abuse* AND (title:school* OR title:college*)
Limited to Theses and dissertations and by year 2012 to 2013
ClinicalTrials.gov,clinicaltrials.gov/, searched 9 September 2014, limited to records added since 1 September 2013 (15 records)
Previous searches 3 September 2013, limited to records added since 1 March 2012 (9 records) 5 April 2012, searched all years as not searched for original review (22 records)
Sex abuse school | Interventional Studies | Child |
ICTRPapps.who.int/trialsearch/, last searched searched 9 September 2014, limited to records registered since 1 September 2013 (1 record)
Previous searches
3 September 2013 (no new records) 3 April 2012, no limits applied as not searched for original review (no records)
Condition: sex abuse
Intervention: School
Australasian Theses (via TROVE)trove.nla.gov.au/, last searched 9 September 2014, limited to publication year 2013 to 2014 (no new records)
Previous searches
3 September 2013, limited to publication year 2012 to 2013 (no new records) 3 April 2012, no limits applied as not searched for original review (9 records)
All words: SEX* ABUSE* SCHOOL* in TITLE and limited to Dissertations
Appendix 2. Search strategies up to August 2006
Cochrane Central Register of Controlled Trials (CENTRAL) (2006, Issue 3) CHILD CHILD* TEENAGE* ADOLESCEN* (((#1 or #2) or #3) or #4) SEX OFFENSES RAPE INCEST* (SEX* near OFFENCE*) (SEX* near OFFENSE*) (SEX* near ABUS*) (SEX* near ASSAULT*) (SEX* near MOLEST*) (SEX* near CRIM*) (SEX* near COERC*) (((((((((#6 or #7) or #8) or #9) or #10) or #11) or #12) or #13) or #14) or #15 (#5 and #16)
MEDLINE (via OVID) searched 1966 to August 2006 1 exp child/ 2 child$.tw. 3 adolescen$.tw. 4 teenage$.tw. 5 1 or 2 or 3 or 4 6 exp Sex offenses/ 7 Incest/ 8 (sex$ adj5 offen$).tw. 9 (sex$ adj5 abus$).tw. 10 (sex$ adj5 assault$).tw. 11 (sex$ adj5 molest$).tw. 12 (sex$ adj5 coerc$).tw. 13 (sex$ adj5 crim$).tw. 14 incest$.tw. 15 rape.tw. 16 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 17 5 and 16 18 randomized controlled trial.pt. 19 controlled clinical trial.pt. 20 Randomized controlled trials/ 21 random allocation.sh. 22 double blind method.sh. 23 single‐blind method.sh. 24 or/18‐23 25 (animal not human).sh. 26 24 not 25 27 clinical trial.pt. 28 exp Clinical trials/ 29 (clin$ adj25 trial$).ti,ab. 30 ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).ti,ab. 31 placebos.sh. 32 placebo08 33 random$.ti,ab. 34 research design.sh. 35 or/27‐34 36 35 not 25 37 36 not 26 38 comparative study.sh. 39 exp evaluation studies/ 40 follow up studies.sh. 41 prospective studies.sh. 42 (control$ or prospectiv$ or volunteer$).ti,ab. 43 or/38‐42 44 43 not 25 45 44 not (26 or 37) 46 26 or 37 or 45 47 17 and 46
EMBASE (via OVID) searched 1980 to August 2006 1 Controlled study/ 2 Clinical trial/ 3 Major clinical study/ 4 random$.tw. 5 Randomized controlled trial/ 6 trial$.tw. 7 compar$.tw. 8 control$.tw. 9 study.tw. 10 follow‐up.tw. 11 clinic$.tw. 12 blind$.tw. 13 Double blind procedure/ 14 placebo$.tw. 15 Clinical article/ 16 Placebo/ 17 doubl$.tw. 18 or/1‐17 19 exp child/ 20 exp adolescent/ 21 child$.tw. 22 adolescen$.tw. 23 teenage$.tw. 24 19 or 20 or 21 or 22 or 23 25 exp sexual abuse/ 26 exp Child abuse/ 27 exp sexual crime/ 28 rape$.tw. 29 incest$.tw. 30 (sex$ adj5 offen$).tw. 31 (sex$ adj5 abus$).tw. 32 (sex$ adj5 assault$).tw. 33 (sex$ adj5 molest$).tw. 34 (sex$ adj5 coerc$).tw. 35 (sex$ adj5 crim$).tw. 36 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 37 24 and 36 38 37 and 18
CINAHL (via OVID) searched 1982 to August 2006 1 Experimental Studies/ 2 exp Clinical trials/ 3 ((control$ or clinic$ or prospectiv$) adj5 (trial$ or study or studies)).tw. 4 ((allocat$ or assign$ or divid$) adj5 (condition$ or experiment$ or treatment$ or control$ or group$)).tw. 5 ((singl$ or doubl$) adj (blind$ or mask$)).tw. 6 cross?over$.tw. 7 placebo$.tw. 8 (compar$ adj5 (trial$ or study or studies)).mp. [mp=title, cinahl subject heading, abstract, instrumentation] 9 exp Clinical research/ 10 Comparative studies/ 11 exp Evaluation research/ 12 exp "control (research)"/ 13 Random assignment/ 14 exp Prospective studies/ 15 exp Evaluation research/ 16 random$.tw. 17 exp Sexual abuse/ 18 rape.tw. 19 incest$.tw. 20 (sex$ adj5 offen$).tw. 21 (sex$ adj5 abus$).tw. 22 (sex$ adj5 assault$).tw. 23 (sex$ adj5 molest$).tw. 24 (sex$ adj5 coerc$).tw. 25 (sex$ adj5 crim$).tw. 26 or/17‐25 27 exp Child/ 28 child$.tw. 29 adolescen$.tw. 30 teenage$.tw. 31 or/27‐30 32 26 and 31 33 or/1‐16 34 32 and 33
PsycINFO searched 1984 to August 2006
1 "RANDOM$".mp. 2 (random$ adj (alloc$ or assign$ or divid$)).mp. [mp=title, abstract, heading word, table of contents, key phrase identifiers] 3 (random$ adj (trial$ or study or studies)).mp. [mp=title, abstract, heading word, table of contents, key phrase identifiers] 4 ((control$ or clinic$ or prospectiv$) adj5 (trial$ or study or studies)).mp. [mp=title, abstract, heading word, table of contents, key phrase identifiers] 5 ((allocat$ or assign$ or divid$) adj5 (condition$ or experiment$ or treatment$ or control$ or group$)).mp. [mp=title, abstract, heading word, table of contents, key phrase identifiers] 6 ((singl$ or double$) adj (blind$ or mask$)).mp. [mp=title, abstract, heading word, table of contents, key phrase identifiers] 7 "CROSS?OVER".mp. 8 exp placebo/ 9 (compar$ adj5 (trial$ or study or studies)).mp. [mp=title, abstract, heading word, table of contents, key phrase identifiers] 10 (health or medicine or illness).sh. 11 8 and 9 12 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 11 13 "child"/ 14 "CHILD$".mp. 15 exp adolescents/ or "teenager".mp. 16 14 or 15 17 exp sexual abuse/ 18 exp incest/ or exp rape/ or exp sex offenses/ or exp victimization/ or "sexual assault".mp. 19 17 or 18 20 12 and 16 and 19
Sociological Abstracts (via Cambridge Scientific Abstracts) searched 1963 to August 2006 ((sex* near3 coerc*) or (sex* near3 crim*) or (sex* near3 assault*) or (sex* near3 abus*) or (sex* near3 molest*) or (sex* near3 offense*) or (sex* near3 offence*) or ("Incest‐" in DE) or (incest*) or ("Rape‐" in DE) or (rape) or (explode "Child‐Sexual‐Abuse" in DE)) and ((( ((control* or clinic* or prospectiv*) near5 (trial* or study or studies)) in AB )or( ((control* or clinic* or prospectiv*) near5 (trial* or study or studies)) in TI )) or (( (random*) in AB )or( (random*) in TI )) or (( (random* near (trial* or study or studies)) in AB )or( (random* near (trial* or study or studies)) in TI )) or (( (random* near (allocat* or assign* or divid*)) in AB )or( (random* near (allocat* or assign* or divid*)) in TI )) or (( (compar* near5 (trial* or study or studies)) in AB )and( compar* near5 (trial* or study or studies) )) or (placebo*) or (( (cross?over) in AB )and( (cross?over) in TI )) or (( ((singl* or doubl*) near (blind* or mask*)) in AB )and( ((singl* or doubl*) near (blind* or mask*)) in TI )) or (( ((allocat* or assign* or divid*) near5 (condition* or experiment* or treatment* or control* or group*)) in AB )and( ((allocat* or assign* or divid*) near5 (condition* or experiment* or treatment* or control* or group*)) in TI ))) and ((adolescen*) or (teen*) or (child*) or (explode "Children‐" in DE) or (explode "Adolescents‐" in DE))
Data and analyses
Comparison 1. Protective behaviours.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Protective behaviours, no correction for clustering | 2 | 102 | Odds Ratio (M‐H, Random, 95% CI) | 5.71 [1.98, 16.51] |
| 2 Protective behaviours, ICC=0.1 | 2 | 102 | Odds Ratio (Random, 95% CI) | 5.43 [1.88, 15.65] |
| 3 Protective behaviours, ICC=0.2 | 2 | 102 | Odds Ratio (Random, 95% CI) | 5.16 [1.81, 14.70] |
Comparison 2. Knowledge.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Questionnaire‐based knowledge, no correction for clustering | 18 | 4657 | Std. Mean Difference (IV, Random, 95% CI) | 0.61 [0.45, 0.78] |
| 2 Questionnaire‐based knowledge, ICC = 0.1 | 18 | Std. Mean Difference (Random, 95% CI) | 0.66 [0.51, 0.81] | |
| 3 Questionnaire‐based knowledge, ICC = 0.2 | 18 | Std. Mean Difference (Random, 95% CI) | 0.63 [0.50, 0.77] | |
| 4 Vignette‐based knowledge, no correction for clustering | 11 | 1688 | Std. Mean Difference (IV, Random, 95% CI) | 0.45 [0.24, 0.65] |
| 5 Vignette‐based knowledge, ICC = 0.1 | 11 | Std. Mean Difference (Random, 95% CI) | 0.53 [0.32, 0.74] | |
| 6 Vignette‐based knowledge, ICC = 0.2 | 11 | Std. Mean Difference (Random, 95% CI) | 0.60 [0.31, 0.89] |
Comparison 3. Retention over time.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Questionnaire‐based knowledge, no correction for clustering | 4 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Questionnaire‐based knowledge (post‐test) | 4 | 956 | Std. Mean Difference (IV, Random, 95% CI) | 0.78 [0.38, 1.17] |
| 1.2 Questionnaire‐based knowledge (follow‐up) | 4 | 929 | Std. Mean Difference (IV, Random, 95% CI) | 0.69 [0.51, 0.87] |
| 2 Questionnaire‐based knowledge, ICC = 0.1 | 4 | Std. Mean Difference (Random, 95% CI) | Subtotals only | |
| 2.1 Questionnaire‐based knowledge (post‐test) | 4 | Std. Mean Difference (Random, 95% CI) | 0.86 [0.53, 1.20] | |
| 2.2 Questionnaire‐based knowledge (follow‐up) | 4 | Std. Mean Difference (Random, 95% CI) | 0.73 [0.41, 1.06] | |
| 3 Questionnaire‐based knowledge, ICC = 0.2 | 4 | Std. Mean Difference (Random, 95% CI) | Subtotals only | |
| 3.1 Questionnaire‐based knowledge (post‐test) | 4 | Std. Mean Difference (Random, 95% CI) | 0.86 [0.53, 1.20] | |
| 3.2 Questionnaire‐based knowledge (follow‐up) | 4 | Std. Mean Difference (Random, 95% CI) | 0.72 [0.32, 1.11] |
Comparison 4. Harm.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Harm, no correction for clustering | 3 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Anxiety or fear | 3 | 795 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.08 [‐0.22, 0.07] |
| 2 Harm, ICC=0.1 | 3 | Std. Mean Difference (Random, 95% CI) | Subtotals only | |
| 2.1 Anxiety or fear | 3 | Std. Mean Difference (Random, 95% CI) | ‐0.04 [‐0.42, 0.33] | |
| 3 Harm, ICC=0.2 | 3 | Std. Mean Difference (Random, 95% CI) | Subtotals only | |
| 3.1 Anxiety or fear | 3 | Std. Mean Difference (Random, 95% CI) | ‐0.03 [‐0.46, 0.40] |
Comparison 5. Disclosures.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Disclosures, no correction for clustering | 3 | 1788 | Odds Ratio (M‐H, Random, 95% CI) | 3.56 [1.13, 11.24] |
| 2 Disclosures, ICC=0.1 | 3 | 1788 | Odds Ratio (Random, 95% CI) | 3.04 [0.75, 12.33] |
| 3 Disclosures, ICC=0.2 | 3 | 1788 | Odds Ratio (Random, 95% CI) | 2.95 [0.69, 12.61] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Blumberg 1991.
| Methods | Design: cluster‐RCT Unit of allocation: classrooms Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 264 kindergarten, 1st, 2nd, and 3rd grade students
Mean age: 7.2 years
Gender: 53% male; 47% female Ethnicity: 51% Caucasian; 18% Black; 17% Hispanic; 7% Asian; 7% Other Setting: 3 city elementary schools in San Diego unified school district, California Country: USA Attrition: intervention group 14/99 = 14.1%; intervention group 7/86 = 8.1%; control group 3/79 = 3.8% |
|
| Interventions | Intervention 1: role‐play programme ("Stop, Tell someone, Own your body, Protect yourself" (STOP))
Intervention 2: multimedia programme ("Child Abuse Primary Prevention Program" (CAPPP))
Control: fire prevention programme Duration: 1 x 1‐hour session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): yes, reported in Chadwick 1989 Knowledge (vignette‐based knowledge): Touch Discrimination Task, comprising 7 vignettes in which an adult touched a child in some way Disclosures: child protective services file search at 15 months post intervention Harm: not reported Other: fear survey, sexual abuse knowledge index, and measure of behavioural acquisition, reported in Chadwick 1989 Last outcome assessment: 3 to 94 days post intervention |
|
| Notes | Author contact: yes This study was part of a larger study (n = 486) reported in Blumberg 1987 and Chadwick 1989 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Classrooms were randomly allocated for treatments. Student participation was based on parental consent" (p 15). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Students within the same school received 1 of 3 interventions (role‐play programme, multimedia programme, or control fire safety). It is possible that children may have been aware of this or exposed to other factors/information apart from the intervention they were receiving, or both (e.g. through treatment‐control contamination via playground, siblings, or friendships). Blinding of key personnel (e.g. teachers) may not have been possible in the school delivery context |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "The children were not informed that the interviews were related to the presentations" (p 20). Outcome assessors were different to the persons providing the interventions. "Interviewers were blind to the group membership of the children, and no child was interviewed more than once by the same interviewer to control for potential effects of rapport building" (p 19) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Attrition: intervention group 1 14/99 = 14.1%; intervention group 2 7/86 = 8.1%; control group 3/79 = 3.8%. Reasons for attrition were not reported |
| Selective reporting (reporting bias) | Low risk | This study reported on data from participants (n = 264) who were part of a larger study (n = 486). The data reported in this trial were for those participants who completed both pre‐test and post‐tests (n = 264). Some children in the larger study completed post‐tests only to control for pre‐test sensitisation (n = 221). In the Blumberg 1991 journal article and the Blumberg 1987 thesis, a broader range of measures was mentioned in the methods section than was reported in the results section. The Chadwick 1989 thesis reported on the full range of measures |
Chen 2012.
| Methods | Design: RCT Unit of allocation: individuals Intention‐to‐treat: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 46 students in grades 1 through 6 Mean age: 9.02 years Gender: not reported Ethnicity: 100% Taiwanese Setting: 1 public elementary school in a rural area in southern Taiwan Country: Taiwan Attrition: 0% |
|
| Interventions | Intervention: child sexual abuse prevention training based on Red Flag/Green Flag People (Rape and Abuse Crisis Center 2008) and Red Flag/Green Flag People II (Grimm 1994)
Control: wait list control Duration: 2 x 50‐minute sessions delivered "at the beginning of the school day… before children began their regular academic classes" (p 628) |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Children's Sexual Knowledge Questionnaire (CSKQ), a 6‐item self report knowledge questionnaire with response items correct/incorrect/I don't know Knowledge (questionnaire‐based knowledge): Children's Awareness of Scary Secrets (CASSQ), a 6‐item self report measure to distinguish okay from not okay secrets. Items scored correct/incorrect Knowledge (vignette‐based knowledge): Chinese What If Situations Test (CWIST), comprising 6 hypothetical situations (3 appropriate and 3 inappropriate) to which children respond okay or not okay and then answer to a standard list of 4 further questions Disclosures: not reported Harm: not reported Other: no Last outcome assessment: 2 to 3 weeks after programme completion |
|
| Notes | Author contact: yes This study is reported as a "pilot" programme |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Children in each group then were randomly assigned to the skills‐based CSA prevention program (n = 23) or the WLC condition (n = 23)…" (p 625). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. Tests for baseline imbalances were conducted. No significant differences between the groups were observed "on the demographic variables (e.g. gender, race, age) or on other measures administered at pretest" (p 632) |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding procedures were not reported |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessment was administered in group format but no further information was reported. The identities of the outcome assessors were not specifically reported however we assume the outcome assessors were the same personnel as those delivering the programme |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The study reported "all children enrolled in the study completed the pre‐ and post‐assessment instruments and completed the treatment" (p 632) |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article were also reported in the results. However, some data were incomplete. Missing data were provided after author contact |
Crowley 1989.
| Methods | Design: quasi‐experimental randomised Solomon 4‐group design Unit of allocation: classes or homerooms Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 293 4th and 5th grade students Mean age: not reported; data provided for grade level only Gender: 45% male; 55% female Ethnicity: not reported Setting: 4 elementary schools in the Bedford Central School District, Westchester County, New York Country: USA Attrition: the study consisted of 367 "potential participants" (p 45). Data on 74 participants (20%) were excluded due to missing or incomplete data, or absence during a portion of the study |
|
| Interventions | Intervention: "Good Touches/Bad Touches: A Program to Prevent Child Sexual Abuse" devised by the MHAWC 1984 (group 1 and group 3)
Control: wait‐list control (group 2 and group 4) Duration: 2 x 45‐minute sessions, once per week for 2 weeks |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Sexual Abuse Knowledge Inventory (SAKI), a 27‐item multiple choice format test Knowledge (questionnaire‐based knowledge): Personal Safety Questionnaire (PSQ) (Saslawsky 1986), a 13‐item test. Used to establish construct validity of the SAKI Knowledge (vignette‐based knowledge): no Disclosures: not reported Harm: not reported Other: no Last outcome assessment: 3 months after programme completion |
|
| Notes | Author contact: no Solomon 4‐group design consisted of: group 1: pre‐tested treatment; group 2: pre‐tested control; group 3: unpre‐tested treatment; group 4: unpre‐tested control |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Fourth and fifth grade children (n = 293) were randomly assigned to one of four groups" (p iii). Method of randomisation was not reported |
| Allocation concealment (selection bias) | High risk | Method of concealment was not described. Potentially unconcealed procedure. Tests of baseline imbalances were conducted: "successful randomisation of Groups 1 & 2 did not occur" (pp 60 ‐ 61). There were differences in pre‐test mean scores for groups 1 and 2. Group 1 had higher scores on the pre‐test SAKI than group 2. Group 3 had higher scores on the SAKI and PSQ than group 4 |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. It did not seem that the intervention groups were blinded to their own condition. Homeroom teachers were present during programme delivery, so it was not possible for them to be blinded to the students' conditions |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Group administration of the outcome assessment meant that outcome assessors would need to be blinded to the condition of each entire class or homeroom. Given that the assessors were school staff, blinding was not possible. On some occasions the outcome assessor was the researcher who was not blinded to the groups. On some other occasions the outcome assessor was the programme presenter who was also not blinded to the groups |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Data on 74 participants (20%) were excluded due to missing or incomplete data, or absence during a portion of the study |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the thesis were also reported in the results. Significant and insignificant results were reported |
Daigneault 2012.
| Methods | Design: quasi‐experimental design with random assignment of participants to groups Unit of allocation: schools Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Participants: 160 1st, 2nd, 3rd, and 4th grade students
Mean age: 7.75 years
Gender: not reported Ethnicity: reported as country of birth. 48% Canada; 14.5% Middle East; 13% Asia; 10% Africa; 7% Europe; 4% South America; 3% North America; 0.5% Oceania Setting: 3 public schools in low socioeconomic areas of Montreal, Canada Country: Canada Attrition: not reported |
|
| Interventions | Intervention: ESPACE child sexual abuse prevention programme, "a French adaptation of the CAP workshop (Cooper 1991)" (p 525) for children aged 3 to 12 years
Booster: Confidence, Solidarity, Respect (CSR) based on ESPACE (p 526)
Control: wait‐list control (table 2) Duration: 1 x 90 minute workshop |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): French translation of 24‐item CKAQ (Tutty 1995) Knowledge (vignette‐based knowledge): adaptation of the WIST (Wurtele 1998) comprising 3 vignettes matching ESPACE content with response options (yes/no) to 4 possible behaviours for each vignette (12 items in total) Disclosures: not reported Harm: children's feelings of safety, an 11‐item measure adapted from Schwab‐Stone 1995 Other: children's peer victimisation over the past week, a 10‐item measure adapted from Orpinas 1995 Last outcome assessment: "in the second year of the study" (p 530) |
|
| Notes | Author contact: yes Study reports on booster component with 4 additional outcome measures: general knowledge about violence; confidence in others; empathic concern; and respect towards others |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Schools were randomly assigned to conditions across two years of the study" (p 527) |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Interviewers (n = 7) and ESPACE instructors (n = 4) were blind to school status at T1 and T2. Only interviewers were blind to school status at T4 and T5" (p 527). Blinding procedures were not described |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Interviewers (n = 7) and ESPACE instructors (n = 4) were blind to school status at T1 and T2. Only interviewers were blind to school status at T4 and T5" (p 527). Blinding procedures were not described |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition was not reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article are reported in the results |
Dake 2003.
| Methods | Design: cluster‐RCT
Unit of allocation: schools (20 classrooms in 8 schools) Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 450 3rd grade students (20 classrooms in 8 schools)
Mean age: 8.7 years
Gender: 51% male; 49% female Ethnicity: 56.0% Black; 33.7% White; 2.4% Hispanic; 6.0% Other Setting: 6 urban and 2 rural public schools in the greater metropolitan area of a large Midwestern city Country: USA Attrition: 24% |
|
| Interventions | Intervention: child abuse prevention curriculum modified from an existing curriculum (title not reported)
Control: wait‐list control Duration: 2 x 1‐hour sessions |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): custom made 26‐item questionnaire including: 16 knowledge items; 5 efficacy expectation items (confidence take action in abuse situations); 4 demographic items; and 1 item that determined if the children knew an extra familial adult they could talk to about abuse Knowledge (vignette‐based knowledge): no Disclosures: not reported Harm: not reported Other: no Last outcome assessment: 3 months after programme completion |
|
| Notes | Author contact: yes | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Method of randomisation was not reported. Evidence of computer randomisation provided after author contact (Zwi 2007) |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. Tests for baseline imbalances were conducted. No statistical differences were evident between intervention and control groups on outcome measures for knowledge or efficacy expectations |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding procedures were not reported |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Group administration of the outcome assessment meant that outcome assessors would need to be blinded to the condition of whole schools. This may not have been possible under the circumstances. The identities of the outcome assessors were not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Attrition was reported as 24% due to "absenteeism" and "unmatchable questionnaires" (p 78) |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article were also reported in the results |
Dawson 1987.
| Methods | Design: cluster‐RCT Unit of allocation: classrooms Intention‐to‐treat analysis: no Adjustment of clustering: no |
|
| Participants | Total number randomised: 237 4th, 5th, and 6th grade students Mean age: 10.6 years Gender: 54% male; 46% female Ethnicity: 53.2% White; 46.8% Black Setting: 2 Memphis City public schools Country: USA Attrition: intervention group, 7/96 (7.3%); control group 1, 2/76 (2.6%); control group 2, 2/65 (3.1%) |
|
| Interventions | Intervention: child sexual abuse prevention programme presentation, including the appropriate grade level film from the series "Child Sexual Abuse: A Solution" (Adams 1984)
Control 1: no presentation (same school as intervention group) Control 2: no presentation (different school) Duration: 1 x 60‐minute session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Personal Safety Issues Test, a 10‐item multiple choice test Knowledge (vignette‐based knowledge): no Disclosures: not reported Harm: not reported Other: no Other: State‐Trait Anxiety Inventory for Children (STAIC) (Speilberger 1966), 20 statements designed to measure transitory anxiety Last outcome assessment: 6 weeks post intervention |
|
| Notes | Author contact: no | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Classes in the selected schools were randomly assigned to the different treatment groups" (p 45). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. Tests of baseline imbalances were conducted. Age, race, and gender ratios were not significantly different among groups. However, results showed that the mean pre‐test knowledge test score for group B (control 1) was significantly higher than A (intervention) or C (control 2) on the pre‐test (p 82) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. Students within one school were receiving both treatment and control conditions. Authors indicate that children may have been exposed to "grapevine" effect (p 51) whereby information was transmitted informally throughout the school, or between siblings in a family or across families having contact with each other outside of school. School personnel did not appear to be blinded to group or class membership so there is risk of differential treatment of groups |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Classroom teachers, a guidance counsellor, and the researcher served as outcome assessors. Outcome assessors remained in the classroom during the child sexual abuse prevention presentation, therefore, it was not possible for them be blinded to the groups they were assessing. It is not clear if outcome assessment was administered individually to children, or in group format with whole classes |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition is noted as 7.3% intervention, 2.6% control 1, 3.1% control 2 Incomplete data were noted as due to student absence or withdrawal from school. It is possible that there were differences between students with complete and incomplete data |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article were also reported in the results. Additional interaction effects were presented |
Del Campo Sanchez 2006.
| Methods | Design: quasi‐experimental design with random assignment of subjects to groups Unit of allocation: individuals Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 382 3rd, 4th, 5th and 6th grade students Mean age: not reported; grade levels included 8 to 12‐year old children Gender: 54% male; 46% female Ethnicity: not reported Setting: 5 public and religious elementary schools in Salmanca, Spain Country: Spain Attrition: not reported |
|
| Interventions | Intervention 1: prevention of child sexual abuse programme (Lopez 1997)
Intervention 2: conventional sex education
Control: no intervention Duration: 2 x 1‐hour sessions, once per week for 2 weeks, delivered during school hours |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): questionnaire on knowledge about sexual abuse, a 35‐item test comprising 33 knowledge and skill items and 2 items on communication with parents about child sexual abuse Knowledge (questionnaire‐based knowledge): Personal Safety Questionnaire (PSQ) (Saslawsky 1986), a 13‐item test. Used to establish construct validity of the questionnaire on knowledge about sexual abuse Knowledge (vignette‐based knowledge): no Disclosures: spontaneous child disclosures reported (8/277 or 2.9% in experimental groups; 2/105 or 1.9% in control group) Harm: information on programme side effects was collected in a questionnaire for parents (12‐item version) and educators (9‐item version) asking for observations of positive and negative changes in children's behaviour after programme completion Other: qualitative assessment of children's participation in the programme during delivery. These data were collected using an observation sheet completed by educators acting as "participant observers" (p 2) Last outcome assessment: 8 months after programme completion |
|
| Notes | Author contact: yes The curriculum evaluated in this study is the 1st elementary school curriculum of its type developed for delivery in Spain |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Subjects were randomly assigned" (p 2). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. Tests for baseline imbalances were conducted. There were no baseline imbalances regarding pre‐treatment knowledge and skills in groups |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding procedures were not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | The method of assessment (group or individual administration) was not reported. The measures used to blind outcome assessors from knowledge of which intervention participants received was not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition not reported |
| Selective reporting (reporting bias) | High risk | All measures discussed in the methods section of the article were also reported in the results. However, data were incomplete (i.e. missing means and standard deviations on total knowledge scores for each of the 3 conditions) |
Fryer 1987a.
| Methods | Design: RCT
Unit of allocation: individuals Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 48 kindergarten, 1st, and 2nd grade students
Mean age: not reported
Gender: not reported Ethnicity: not reported Setting: 1 mid‐town Denver elementary school Country: USA Attrition: < 10% |
|
| Interventions | Intervention: "Children Need to Know Personal Safety Training Program" (Kraizer 1981)
Control: wait‐list control Duration: 1 x 20‐minute presentation, once per day for 8 days |
|
| Outcomes | Protective behaviours simulation: yes. Involved staging of actual simulations used to record children's responses indicating their "degree of vulnerability to abuse" (p 175) Knowledge (questionnaire‐based knowledge): Children Need to Know Knowledge Attitude Test, a 20‐item examination (results not reported) Knowledge (vignette‐based knowledge): no Disclosures: not reported Harm: discussed but not measured Other: Harter Perceived Competence Scale for Children (Harter 1982) used to measure self esteem (results not reported) Last outcome assessment: for the simulation "the day after the classroom program" (p 175); for the questionnaire measures "immediately following the instruction" (p 177) |
|
| Notes | Author contact: yes The results of this study are also reported in Fryer 1987b |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Twenty‐four each were randomly assigned to the experimental and control groups tested" (p 174). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. Tests of baseline imbalances revealed "pretest scores on each of the three tests administered were very nearly the same for the two study groups" (p 177) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | As there was only 1 intervention group, there was no possibility for systematic differences between groups in the way in which the programme was delivered. However, as the control group were from the same school, they may have experienced some contamination or exposure to the programme via other students in the playground, or friends, or siblings outside of the study setting |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Children were blinded to the simulation test. "A research assistant, posing as a stranger" (p 175) conducted the outcome assessment. The blinding of the assessor (if any) is not reported. "A hidden camera and wireless microphone produced an audiovisual record of the encounter which was later reviewed and scored by research team members" (p 176). Interrater reliability was established as 1.0 (total reliability) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Missing data were reported for 1/24 in experimental group (4%) and 3/24 for the control group (12.5%). Data were gathered only from children present on both testing days |
| Selective reporting (reporting bias) | High risk | Not all measures discussed in the methods section of the article were also reported in the results. The results reported in the papers refer only to the simulation |
Grendel 1991.
| Methods | Design: cluster‐RCT Unit of allocation: classrooms and individuals Intention‐to‐treat analysis: no Adjustment for clustering: no, although in some analyses ANCOVA was used to enable adjustment for confounding because of the influence of intact groups |
|
| Participants | Total number randomised: 100 1st grade students Mean age: 6.9 years Gender: 48% male; 52% female Ethnicity: 84.3% White; 15.7% African‐American (intervention group); 79.6% White; 18.4% African‐American (control group) Setting: "2 public schools serving a middle income, predominantly white population from a large school district in the northern part of the Greater Cincinnati area" (p 66) Country: USA Attrition: intervention group, 12/62 (19%); control group, 14/63 (22%) |
|
| Interventions | Intervention: "Child Sexual Abuse Prevention Program" (developed by Women Helping Women, Ohio)
Control: wait‐list control Duration: 1 x 50‐minute session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (Questionnaire‐based knowledge): Personal Safety Questionnaire (PSQ) (Saslawsky 1986), 15 items. "A few minor changes were made in the wording of the PSQ fort his study, but the meaning of the questions remained unchanged" (p 80) Knowledge (vignette‐based knowledge): "What If" Situations Test (Wurtele 1989), 6 hypothetical situations, including 3 appropriate and 3 inappropriate touch situations. After each vignette there are 5 questions Disclosures: not reported Harm: not reported Other: Parent Perception Questionnaire (Wurtele 1989); Teacher Perception Questionnaire (Wurtele 1989); Children's Reactions to Prevention Program (adapted from Binder 1987b; Hazzard 1991) Last outcome assessment: 1‐day post intervention |
|
| Notes | Author contact: no | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "In each school one intact class was randomly assigned to the treatment group, a second intact class was randomly assigned to the control group, and the students in the third class were randomly assigned to ether the treatment or control group" (p 69). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. Tests of baseline imbalances were conducted: "the results of the demographic data indicate that the treatment and control groups were very similar on the variables assessed... both groups demonstrated comparable knowledge about sexual abuse and sexual abuse prevention skills" (pp 88‐90) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | The intervention groups were not blinded to their own condition and school personnel were not blinded to group or class conditions since teachers attended training and completed measures. Since both intervention and control groups were from the same school, there is a possibility of treatment‐control contamination effects |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessment was conducted individually with each participant. "Every effort was made to keep the assistants naive to the hypotheses and to the group membership of the subjects" (p 72) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Incomplete outcome data, mainly in the form of "missing data due to students' absence, withdrawal from school, unwillingness to participate" (p 70). This is high: 19% intervention group; 22% control group |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article were also reported in the results |
Harvey 1988.
| Methods | Design: RCT
Unit of allocation: individuals Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 90 kindergarten children
Mean age: 5.8 years (70 months)
Gender: not reported Ethnicity: 56.3% Caucasian; 43.7% Black Setting: 4 schools in a rural area near Georgia Country: USA Attrition: 21% |
|
| Interventions | Intervention: "Good Touch‐Bad Touch" programme (citation not reported)
Control: story, discussion, film, and song not related to child sexual abuse Duration: 3 x 30‐minute sessions across 3 consecutive days |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): basic knowledge, a 5‐item test Knowledge (vignette‐based knowledge): good touch/sexually abusive touch pictures, comprising 10 pictures of young children interacting with an adult. 5 pictures represented good touches, and 5 pictures represented sexually abusive touches Knowledge (vignette‐based knowledge): direct test, comprising 2 scenes (taught as part of the programme) followed by 6 questions Knowledge (vignette‐based knowledge): generalisation test, comprising 2 scenes (not taught as part of the programme) followed by 6 questions Disclosures: not reported Harm: not reported Other: no Last outcome assessment: 7 weeks after programme completion |
|
| Notes | Author contact: yes | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Children in each of the four schools were randomly assigned (with the restriction that at the pre intervention assessment there was approximately an equal number of black and white boys and girls per group) to one of two groups: an experimental group and a placebo control group" (p 432). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. In terms of baseline imbalances, results indicated no significant differences in the age of children, family socioeconomic status, gender, or race between experimental and control groups |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. 2 "experimenters" delivered the intervention programme (p 431). "Each experimenter conducted experimental and placebo control sessions in two schools" (p 431). These individuals could not have been blinded to study conditions, however the use of 2 individuals increases the risk that compared groups received different interventions |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessment was conducted "individually for each child at pre intervention, postintervention, and follow up" (pp 431‐2). The measures used to blind outcome assessors from knowledge of which intervention participants received was not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Attrition was reported only for the study overall, and not specified for intervention and control groups. Attrition and missing data were attributed to student absence during the programme or testing, and moving from the school. Attrition was calculated overall as 19/90 (21%) |
| Selective reporting (reporting bias) | High risk | Not all measures discussed in the methods section of the article were also reported in the results. Means and SDs for knowledge outcomes were measured but not reported |
Hazzard 1991.
| Methods | Design: cluster‐RCT
Unit of allocation: schools Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 399 3rd and 4th grade students
Mean age: not reported
Gender: 50% male; 50% female Ethnicity: 68% Caucasian; 23% Black; 4% Hispanic; 3% Asian; 2% Other Setting: 27 classrooms (14 x 3rd grade and 13 x 4th grade) in 8 city elementary schools from a suburban school district in a large southeastern city Country: USA Attrition: not reported |
|
| Interventions | Intervention 1: teacher and child training comprising a 6‐hour workshop for teachers and adaptation of "Feeling Yes, Feeling No" (National Film Board of Canada 1985) sexual abuse prevention curriculum for children and homework handouts
Intervention 2: child training only as per intervention 1 Intervention 3: teacher training only as per intervention 1 Control: fire or water safety programme, and wait‐listed to receive the programme after follow‐up testing was completed Duration: 3 x 1‐hour sessions |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): What I Know About Touching scale, a 25‐item measure testing knowledge of concepts, including: definitions of sexual abuse, characteristics of abusers, who can be abused, it's ok to say no, it's okay to tell about abuse, and sexual abuse is not the child's fault Knowledge (vignette‐based knowledge): What Would You Do? A video tape measure comprising 6 x 30‐second scenarios, which were not shown or discussed in the prevention programme. This outcome assessment was administered to 4 to 6 randomly selected children from each treatment group at post‐test and follow‐up Disclosures: yes Harm: not reported Other: State‐Trait Anxiety Inventory for Children (STAIC) (Spielberger 1973); parent measure (adapted from Miller‐Perrin 1986) Last outcome assessment: 1‐year follow‐up |
|
| Notes | Author contact: yes | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "One school from each set was randomly assigned to one of four conditions" (p 125). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "All teachers were aware that different schools were receiving different services and were told that we were evaluating the effectiveness of different models of sexual abuse prevention training" (pp 125‐6). "Since the child prevention program was presented by professional trainers rather than teachers themselves, the teacher training component was not expected to have a major impact on children's gains at post‐testing. However, it was expected that if Condition 1 teachers became more knowledgeable and supportive of prevention education as a result of their own training, their students might demonstrate continued increases in prevention knowledge and skills over the 6‐week follow‐up period" (p 126) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessments were conducted via group administration by a research assistant who read the scripts to participating children in each class. However, the video measure was administered at post‐test and follow‐up to a random sample of 4 to 6 children from each group. The video measure was "administered by a trained research assistant to each child as an individual structured interview. Interviewers were not blind to subjects' treatment condition since schools were assigned to condition" (p 128) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition between pre‐ and post‐test was not reported. However, complete data were reported for 103/399 at 1‐year follow‐up (25.8%) |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article were also reported in the results |
Hébert 2001.
| Methods | Design: quasi‐experimental randomised Solomon 4‐group design Unit of allocation: schools Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Participants: 133 1st and 3rd grade students
Mean age: 7 years 2 months
Gender: 50% male; 50% female Ethnicity: not reported Setting: 2 primary schools in Quebec City situated in middle‐income areas Country: Canada Attrition: not reported |
|
| Interventions | Intervention: ESPACE child sexual abuse prevention program, "an adaptation of the widely implemented American Child Assault Prevention Program [CAPP] (Cooper 1991)" (p 508)
Control: wait‐list control, scheduled to receive the programme in the next calendar year Duration: 1 x 60‐ to 75‐minute workshop |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): knowledge questionnaire, an 11‐item measure derived from the CKAQ (Tutty 1995) and the PSQ (Saslawsky 1986) Knowledge (vignette‐based knowledge): vignette measure of skills, comprising 5 video vignettes (4 depicting abuse situations; 1 non‐abusive situation) Disclosures: not reported Harm: data on potential side effects of the programme were gathered from parents who completed the PPQ 2 weeks after programme completion Other: children's programme satisfaction measure; parent questionnaire adapted from the PPQ (Wurtele 1989); programme fidelity measure Last outcome assessment: 2 months after programme completion |
|
| Notes | Author contact: yes Solomon 4‐group design consisted of: group 1 treatment group (pre‐test, post‐test and follow‐up); group 2 control group (pre‐test and post‐test); group 3 treatment group (post‐test and follow‐up only); group 4 control group (post‐test only) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Assignment of schools to conditions was determined randomly" (p 509). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. Tests for baseline imbalances were conducted. There were no significant differences between intervention and control groups with respect to "exposure to prevention information prior to their participation in the program" (p 512) |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. Students in the same school received the same intervention. It is likely that participants were not blinded to their condition. School personnel were not blinded to the conditions of children within the school as teachers received training as part of the programme |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | "The program was delivered in class by three female community workers. Six graduate students were recruited as interviewers, all of whom had extensive experience with children in school settings" (p 511). "The questionnaire was administered collectively in class" (p 509) meaning that outcome assessors would need to have been blinded to the condition of whole schools. This is unlikely under the circumstances. The video vignettes were watched in small groups of 4 or 5 children and questions were answered individually |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition not reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article were also reported in the results section |
Kolko 1989.
| Methods | Design: cluster‐RCT
Unit of allocation: school districts
Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Participants: 337 3rd grade students
Mean age: 8.3 years (experimental group); 8.5 years (control group)
Gender: 52% male, 48% female (experimental group); 57% male, 43% female (control group) Ethnicity: not reported Setting: elementary schools in Washington County, Pennsylvania Country: USA Attrition: from enrolment to 2‐week post‐test 16.2%; from enrolment to 6‐month follow‐up 25.3% |
|
| Interventions | Intervention: Red Flag/Green Flag programme (Williams 1980)
Control: wait‐list control Duration: 2 x 45‐minute sessions |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): child self report, a 25‐item questionnaire comprising 4 scales (awareness, subjective disturbance, likelihood of talking, programme concepts/skills). The programme concepts/skills scale comprised 11 items derived from the programme training manual in multiple choice format Knowledge (vignette‐based knowledge): no Disclosure: data collected from school guidance counsellor incident reports Harm: discussed. No adverse reactions were reported by children, parents, teachers, or volunteers Other: programme integrity monitored using a rating scale completed by volunteers Last outcome assessment: 6 months after the second classroom training session and less than 1 month before the end of the school year |
|
| Notes | Author contact: yes | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. No baseline imbalances were detected between groups. There were 6 intervention schools and only 1 control school meaning that the groups were not equivalent. Adjustment procedures to address these imbalances were not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. However, it is likely that participants were not blinded to their condition. Blinding of key personnel within the school was not possible as they were involved in programme delivery |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It was not clear if outcome assessment was administered individually to children, or in group format with the whole class. The identities of outcome assessors were not reported. Methods of blinding were not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Attrition was high (as noted above). Reasons for attrition were not reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section were reported in the results section |
Krahé 2009.
| Methods | Design: cluster‐RCT Unit of allocation: school Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 148 1st and 2nd grade students Mean age: 7.55 years Gender: 47.3% male; 52.7% female Ethnicity: not reported Setting: 3 schools in a large suburban district of Berlin Country: Germany Attrition: not reported |
|
| Interventions | Intervention 1: LIVE (i.e. live performance), participants watched a live performance of a theatre play entitled "(No) Child's Play"
Intervention 2: DVD (i.e. performance captured on DVD), participants watched a filmed performance of the theatre play as above, on DVD Control: wait‐list control Duration: 1 x 60‐minute session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): no Knowledge (vignette‐based knowledge): self protective skills, comprising 8 short scenarios depicting "interactions of a child with an adult where the child was uneasy about the adult's behaviour or uncertain as to the adult's intention" (p 324). Scenarios presented with a simple cartoon, followed by a set of up to 4 questions Disclosures: not reported Harm: 1 vignette assessed possible negative side effects (fear of adults) Other: no Last outcome assessment: 30 weeks post intervention |
|
| Notes | Author contact: no Intervention 1 (LIVE) was accompanied by a 3‐hour training session for teachers and a 3‐hour information evening for parents |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Schools that were "first to sign up for participation in the (No) Child's Play prevention programme offered by Berlin police were randomly assigned to three conditions" (p 323). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure. In terms of baseline imbalances, demographic characteristics of each group were not reported. Results showed that the mean knowledge scores of students in the 3 study conditions did not differ significantly at baseline |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. Intervention schools were not blinded to their own condition by virtue of the fact that they volunteered to receive the programme or were wait‐listed to receive it. Schools may or may not have been blinded to other schools' conditions, that is, they may or may not have been aware that they were getting/not getting something equivalent to other groups (e.g. via correspondence with the Berlin Police). It is possible that students were blinded, but teachers were not. It is possible that teaching staff in the DVD group may have compensated for not having the live performance which may have altered results |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Group administration of the outcome assessment meant that outcome assessors would need to be blinded to the condition of whole schools. 4 interviewers conducted the outcome assessments. "One of them was the second author, who was not blind with regard to the hypotheses and experimental conditions. Half of the sessions in each school were conducted by the second author, the remaining sessions were conducted by the three additional interviewers who were blind as to the hypotheses of the study and the group membership of the children they tested. In this way, the same number of sessions was run by the second author and the additional interviewers in each condition. No differences between the conditions were found in relation to different interviewers" (p 325 footnote 3) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition not reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section were reported in the results section |
Kraizer 1991.
| Methods | Design: cluster‐RCT Unit of allocation: schools Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 670 preschool, kindergarten, 1st, 2nd, and 3rd grade students Mean age: not reported. Programme was designed for children aged 3 to 10 years Gender: not reported Ethnicity: not reported Setting: 3 sites (New York, New Jersey, Colorado), 10 schools (3 schools from each site + 1 additional preschool) Country: USA Attrition: 26/670 (3.8%) |
|
| Interventions | Intervention 1: "The Safe Child Program" (written by Kraizer for this PhD) for children aged 3 to 10 years. Phase 1 is teacher training; phase 2 is parent training; phase 3 is training with the children
Intervention 2: the Safe Child Program (revised version) Control: wait‐list control Duration: preschool and kindergarten, 1 session per day for 10 days. 1st to 3rd grade, 1 session per day for 5 days |
|
| Outcomes | Protective behaviours simulation: stranger simulation, involved staging of actual simulations to evaluate children's "degree of vulnerability to abduction and abuse by strangers" (p 175) Protective behaviours simulation: yes. Role‐play, a protocol used as the "basis for measuring behavioural change and actual mastery of skills associated with prevention of sexual abuse... the role play measures the child's ability and willingness to terminate unwanted touch effectively and appropriately in the face of flattery, emotional coercion, rejection, bribery, and secrecy" (p 29) Knowledge (questionnaire‐based knowledge): Children Need to Know Knowledge Attitude Test, comprising a 20‐item self report instrument "measuring a child's cognitive awareness, understanding and attitudes" (p 31) Knowledge (vignette‐based knowledge): no Disclosures: not reported Harm: not reported Other: Battle Culture Free Self Esteem Inventory (Battle 1981); The Children's Nowicki‐Strickland Internal External Locus of Control Inventory (Nowicki 1973); self care simulation; Teacher Knowledge/Attitude Questionnaire and Demographics Sheet; Teacher Questionnaire Last outcome assessment: 6 months after the programme |
|
| Notes | Author contact: yes An overview of this study is reported in Kraizer 1989 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation was not reported |
| Allocation concealment (selection bias) | High risk | Method of concealment was not reported. Potentially unconcealed procedure. The following statement: "student samples were selected, in cooperation with school officials, to meet the following research objectives and criteria..." (p 27) indicates there was not adequate allocation concealment and therefore high risk of bias |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Teachers, as key personnel, could not have been blinded to group allocation as they delivered the video tape intervention. It is not clear if children from the same school were allocated to treatment and control groups as this detail is not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Role‐plays were conducted by a research team member trained in child development and the prevention of child abuse who was not associated with the prevention program being conducted in the school" (p.30). "Scoring was completed by an observer via contemporaneous video monitoring rather than the person conducting the role‐play" (p 30). It is not clear if these outcome assessors were blinded to study condition and hypotheses |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition for the study overall was reported as 3.8% and was attributed to student withdrawals or exclusions or both. Attrition was not specified for intervention and control groups |
| Selective reporting (reporting bias) | High risk | Not all measures discussed in the methods section of the article were also reported in the results. Means and SDs for knowledge outcomes were measured but not reported |
Lee 1998.
| Methods | Design: RCT
Unit of allocation: individuals Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 77 female students attending schools for children with mental retardation
Mean age: 13.44 years
Gender: 0% male; 100% female Ethnicity: 100% Chinese Setting: 4 special schools in Hong Kong Country: China Attrition: 6.3% |
|
| Interventions | Intervention: Behavioral Skills Training Program (Wurtele 1990) encompassing 7 safety rules, 1 personal body safety rule, and 4 self protection skills
Control: Attention Control Program (Wurtele 1992) covering safety skills unrelated to sexual abuse Duration: 2 x 45‐minute sessions on consecutive days |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Personal Safety Questionnaire (Wurtele 1990) comprising 15 items covering personal safety and 3 control questions Knowledge (vignette‐based knowledge): What If Situations Test (Wurtele 1990) comprising 6 brief vignettes (3 appropriate and 3 inappropriate touch requests) Disclosure: not reported Harm: discussed. Lower levels of fear reported at 2‐month follow‐up compared with pre‐test and post‐test Other: baseline assessment of intellectual ability using Raven's Standard Progressive Matrices (Raven 1960); Fear Assessment Thermometer Scale (Wurtele 1986b), 12 items collecting data on fear of objects, people and situations Last outcome assessment: 2 months after programme implementation |
|
| Notes | Author contact: yes, no reply | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "The 72 completers were randomly assigned to either the treatment (n = 38) or control group (n = 34)" (p 107). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "To control for intergroup contamination, we assigned participants from the same school to the same program. Both programs were led by the first author, who read from narrative scripts with pictures as visual aids" (p 108). Blinding of school personnel (e.g. teachers) would not be possible under the circumstances. Analysis of baseline data indicated no significant differences between groups on outcome measures, intellectual ability, or age |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | All outcome assessments were individually administered "by one of three female interviewers, who read the questions aloud in a standardized format and recorded the participants' exact responses" (p 108). Baseline assessment of intellectual ability was administered to groups of 8 to 10. Measures used to blind outcome assessors were not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition was reported as 2/38 (5.3%) for the intervention group and 3/34 (8.8%) for the control group (p 109). Reasons for attrition were failure to attend the intervention programme after pre‐testing or failing to take part in the post‐test |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the paper were also discussed in the results |
Oldfield 1996.
| Methods | Design: cluster‐RCT Unit of allocation: classrooms Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 1269 1st to 6th grade students
Mean age: not reported
Gender: 47% male; 53 % female Ethnicity: 86% Caucasian; 7% African American; 3% Hispanic; 3% Asian American; 1% Native American Setting: 4 public schools in a Midwestern city Country: USA Attrition: not reported |
|
| Interventions | Intervention: Project TRUST (Anderson 1990)
Control: wait‐list control, received the programme after all data were collected Duration: 1 x 45‐minute session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Children's Knowledge of Abuse Questionnaire‐Revised (CKAQ‐R) (Tutty 1995) comprising 33 true/false items Knowledge (vignette‐based knowledge): no Disclosure: Maltreatment Disclosure Report Form was used to record information about student disclosures (date, type of disclosure, nature of the report, student age, gender, race, and socioeconomic status) Harm: discussed. No significant difference in anxiety between intervention and control groups Other: Revised Children's Manifest Anxiety Scale (RCMAS) (Reynolds 1985), a 37‐item self report anxiety measure for children in grades 1 to 3; The State‐Trait Anxiety Inventory for Children (STAIC) (Spielberger 1973) a 20‐item self report measure for children in grades 4 to 6 Last outcome assessment: within 2 days after viewing the play |
|
| Notes | Author contact: yes, no reply | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Classrooms at each grade level were randomly assigned to the treatment or control conditions" (p 822). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. Students within 1 school were receiving treatment and control conditions. There was a possibility of treatment‐control contamination of information transmitted informally throughout the school. School personnel did not appear to be blinded to group or class membership so there is risk of differential treatment of groups |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Data were collected by assigned evaluators from subjects in both treatment and control groups on the same day... All data were collected in a blind assessment format with the evaluators unaware of which classrooms were assigned to treatment or control conditions" (p 824). Outcome assessments were administered in group format in classrooms |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition not was reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the paper were also discussed in the results |
Poche 1988.
| Methods | Design: cluster‐RCT
Unit of allocation: classrooms Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 74 students (29 kindergarten students; 45 1st grade students)
Mean age: not reported. Age range reported as 5 to 7 years
Gender: 55% male; 45% female Ethnicity: 74.3% White; 25.7% Black Setting: 3 public schools located in low to upper‐middle income neighbourhoods in Kalamazoo, Michigan Country: USA Attrition: not reported |
|
| Interventions | Intervention 1: videotape only
Intervention 2 (videotape plus behaviour rehearsal): as above with the addition of behaviour rehearsal conducted in the classroom with a trainer playing the role of a friendly abductor
Intervention 3 (standard programme): a presentation of 2 safety rules, discussion of several abduction situations, and a brief film on personal safety Control: wait‐list control, who received the programme at the end of the study Duration: video only (25 minutes); videotape plus behaviour rehearsal (45 minutes); standard programme (60 minutes) |
|
| Outcomes | Protective behaviours simulation: yes. Staging of scenarios in which an adult male (a doctoral student) "posed as a potential abductor, approached each child in a friendly manner, and attempted to entice the child to go with him. The child's responses (verbal and motor) to the enticements were directly observed and recorded on a data sheet" (p 256). At follow‐up the simulation was conducted in an identical manner, at or near the child's home (with parental permission) Knowledge (questionnaire‐based knowledge): no Knowledge (vignette‐based knowledge): no Disclosures: not reported Harm: not reported Other: no Last outcome assessment: 1 month after training |
|
| Notes | Author contact: yes, no reply | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Each kindergarten and each first‐grade class were randomly assigned to one of four conditions" (p 257). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. Students within 1 school were receiving treatment and control conditions therefore there was a possibility of treatment‐control contamination. It was not possible for school personnel (e.g. teachers) to be blinded to the study condition of their classes |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "The adult portraying an abductor served as the primary observer and recorded each child's verbal and motor responses as soon as the simulation was over. This observer was blind to the experimental condition of each subject" (p 257). Another adult "served as a reliability observer" (p 257). Agreement between the two observers was 100% (total reliability) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Attrition between pre‐ and post‐test was not reported. At 1‐month follow‐up, only 23/74 children (31%) met the criteria for outcome assessment (pp 256‐7). Of these only 9 were available to partake (12%). Reasons for attrition were "summer vacations, disconnected phones, illnesses and accidents" (p 257) |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the paper were also discussed in the results |
Saslawsky 1986.
| Methods | Design: quasi‐experimental randomised Solomon 4‐group design
Unit of allocation: individuals Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 67 students (26 kindergarten and 1st grade students; 41 5th and 6th grade students)
Mean age: 6.2 years; 11.1 years
Gender: 52% male; 48% female Ethnicity: not reported Setting: 2 public schools in a lower to middle class areas in rural eastern Washington Country: USA Attrition: not reported |
|
| Interventions | Intervention: children viewed the 35‐minute film "Touch" (Illusion Theater Company 1984)
Control: discussion about self concept and personal values with no mention of sexual abuse Duration: 1 x 50‐minute session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Personal Safety Questionnaire (PSQ), a 15‐item measure with 2 practice questions and 13 personal safety questions covering topics typically taught in child sexual abuse prevention programmes. Knowledge (vignette‐based knowledge): What If Situations Test (WIST), comprising 6 hypothetical situations (2 non‐threatening and 4 threatening situations) after which children respond to a standard list of 4 questions Disclosure: not reported Harm: not reported Other: no Last outcome assessment: 3 months post intervention |
|
| Notes | Author contact: yes | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Subjects in schools A and B were assigned randomly, balanced for sex and grade, to one of two conditions" (p 240). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding procedures were not reported. Students within 1 school were receiving treatment and control conditions therefore there was a possibility of treatment‐control contamination. It was not possible for school personnel (e.g. teachers) to be blinded to the study condition of their classes |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Research assistants conducted the outcome assessments. They were blind to each child's group assignment (p 240). PSQ was administered in group format to children in classes. WIST was individually administered to children in an interview format |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition not was reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article are reported in the results |
Snyder 1986.
| Methods | Design: quasi‐experimental Solomon 4‐group design Unit of allocation: classes Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 177 4th grade students Mean age: 9.6 years Gender: 40.7% male; 49.3% female Ethnicity: 97% White; 3% Black, Asian, Hispanic‐American, Other Setting: 7 elementary schools in Erie county, Pennsylvania Country: USA Attrition: 8/177 (4.5%) |
|
| Interventions | Intervention: "Good Secrets, Bad Secrets" (citation not reported) sexual abuse prevention programme
Control: students played hangman between pre‐test and post‐test, and were wait‐listed to receive the programme Duration: 1 x 45‐minute session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Good Secrets Bad Secrets Quiz, a 35‐item covering general safety skills, distinguishing appropriate touching from sexual touching, knowing sexual touches can come from known people, recognising assertive responses for dealing with persuasive adults, recognising how to obtain help in an assault situation, recognising the appropriate course of action for dealing with a potentially dangerous situation. Criterion referenced standard of 80% was applied Knowledge (vignette‐based knowledge): no Disclosures: not reported Harm: not reported Other: no Last outcome assessment: 1‐day post intervention |
|
| Notes | Author contact: no | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "A coin was tossed to determine group assignments" (p 45). No other information was provided |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding procedures were not reported. Children may not have been blinded to their condition. Blinding of key personnel (e.g. teachers) may not have been possible in the school delivery context. The programme and testing were conducted on the same day in an attempt to control for contamination effects |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Group administration of outcome assessment meant that outcome assessors would have to be blinded to the condition of entire classes. This was not possible as outcome assessors were also programme presenters |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Missing data were noted for 8/177 participants (4.5%) owing to parental omissions on the child data sheet. Attrition from the study is not reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section were also reported in the results section |
Tutty 1997.
| Methods | Design: RCT
Unit of allocation: individuals Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 231 1st to 6th grade students
Mean age: not reported
Gender: 47% male; 53% female Ethnicity: 88% Caucasian; 8% Asian or East Indian; 2% Latino; 2% Black Setting: 2 elementary Catholic schools in Calgary (from Tutty 2000) Country: Canada Attrition: not reported |
|
| Interventions | Intervention: "Who Do You Tell" programme developed by the Calgary Sexual Assault Centre in 1983 (citation not reported)
Control: wait‐list control Duration: 2 x 45‐ to 60‐minute sessions on consecutive days |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Children's Knowledge of Abuse Questionnaire‐Revised (CKAQ‐R) (Tutty 1995) comprising 9‐item Appropriate Touch subscale, and 24‐item Inappropriate Touch subscale (33 items in all) testing concepts taught in the programme Knowledge (vignette‐based knowledge): no Disclosure: not reported Harm: parent questionnaire gathered data on children's reactions to the programme Other: no Last outcome assessment: "shortly after" programme completion (p 284) |
|
| Notes | Author contact: yes, no reply Secondary analysis comparing younger (5 to 7 years) and older children (8 to 13 years) was presented in Tutty 2000 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Children were randomly assigned (matched by age) to participate in the program (N = 117) or in a wait‐list control condition (N = 114)" (p 869). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not reported. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding procedures were not reported. Students within the same school were receiving the intervention or participating in the wait‐listed control group. There is risk of treatment‐control contamination effects. It is likely that children were not blinded to their condition. Teachers participated in a training workshop, therefore blinding of key personnel (e.g. teachers) was not possible in this delivery context |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | The method of assessment (group or individual administration) was not reported. The measures used to blind outcome assessors from knowledge of which intervention participants received was not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition was not reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section were also reported in the results section |
Wolfe 1986.
| Methods | Design: cluster‐RCT
Unit of allocation: classrooms Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 290 students (214 4th grade and 76 5th grade students)
Mean age: 10.3 years
Gender: 49% male; 51% female Ethnicity: not reported Setting: 3 public schools comprising children from middle‐ and lower‐income families in the central area of a Southeastern city Country: USA Attrition: not reported |
|
| Interventions | Intervention: 2 x 5‐minute plays written and performed by volunteer medical students who consulted with child abuse specialists
Control: wait‐list control Duration: 1 x 70‐minute session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): a brief 10‐item true/false questionnaire focusing on programme objectives Knowledge (vignette‐based knowledge): no Disclosure: not reported Harm: not reported Other: no Last outcome assessment: 3 to 5 days following the presentation |
|
| Notes | Author contact: yes, no reply | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "The 12 classrooms participating in the study were randomly assigned to a control or treatment condition" (p 88). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding procedures were not reported. It is not known whether whole schools were allocated to conditions or whether schools comprised classes allocated to both treatment and control conditions. The latter presents a higher risk of treatment‐control contamination |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Method of assessment (group or individual administration) was not specified. The measures used to blind outcome assessors from knowledge of group membership was not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition was not reported |
| Selective reporting (reporting bias) | High risk | "Three items were dropped from the final questionnaire due to their inability to contribute to the validity of the measure" (p 89), therefore outcome data for only 7 questionnaire items are reported |
Wurtele 1986.
| Methods | Design: RCT
Unit of allocation: individuals Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 71 students (28 kindergarten and 1st grade students and 43 5th and 6th grade students)
Mean age: 6.1 years; 11.0 years
Gender: 50% male; 50% female Ethnicity: not reported Setting: 1 public school serving a lower to middle class population in a small rural town in eastern Washington Country: USA Attrition: not reported |
|
| Interventions | Intervention 1: 35‐minute film entitled "Touch" (Illusion Theater Company 1984)
Intervention 2: Body Safety Training (BST) (Wurtele 1986a)
Intervention 3: combined group (film and BST). Children viewed the "Touch" film followed by a shortened discussion led by the first graduate student and a shortened version of the BST led by the second graduate student Control: 50‐minute discussion of self concept and personal values with no sexual abuse content Duration: groups 1 and 2: 1 x 50‐minute session; group 3: 1 x 60‐minute session |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Personal Safety Questionnaire (PSQ), a 15‐item measure with 2 practice questions and 13 personal safety questions covering topics typically taught in child sexual abuse prevention programmes Knowledge (vignette‐based knowledge): What If Situations Test (WIST), comprising 6 hypothetical situations (2 non‐threatening and 4 threatening situations) after which children respond to a standard list of 4 questions Disclosure: not reported Harm: not reported Other: no Last outcome assessment: 3 months later |
|
| Notes | Author contact: yes Children gave verbal and written consent for their participation in the study |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Subjects were randomly assigned, in balanced numbers for sex and grade, to one of four experimental conditions" (p 689). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding procedures were not reported. Students within 1 school were receiving treatment and control conditions therefore there was a possibility of treatment‐control contamination. It was not possible for school personnel (e.g. teachers) to be blinded to the study condition of their classes |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | PSQ was administered in group format to children in classes. WIST was individually administered to children in an interview format. Interviewers "were unaware of each child's group assignment" (p 690) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition was not reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article are reported in the results |
Ҫeҫen‐Eroğul 2013.
| Methods | Design: RCT
Unit of allocation: individuals Intention‐to‐treat analysis: no Adjustment for clustering: no |
|
| Participants | Total number randomised: 36 4th grade students
Mean age: not reported
Gender: 55% male; 45% female Ethnicity: not reported Setting: "schools" (p 727), not otherwise specified Country: Turkey Attrition: not reported |
|
| Interventions | Intervention: "Preventing child sexual abuse psycho‐educational training program" (p 727) based on the Good Touch Bad Touch (GTBT) program (Childhelp 2011) adapted for the Turkish culture
Control: no programme Duration: 4 x 60‐minute sessions on consecutive days |
|
| Outcomes | Protective behaviours simulation: no Knowledge (questionnaire‐based knowledge): Good Touch Bad Touch Curriculum Test (Church 1988), a 10‐item measure covering touch differentiation, knowledge of coping with sexual abuse and application to situations. Response options correct, incorrect, don't know. In this study test/retest reliability (0.80) and internal consistency (0.78) Knowledge (vignette‐based knowledge): no Disclosure: not reported Harm: not reported Other: no Last outcome assessment: 8 weeks after post‐test |
|
| Notes | Author contact: pending | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "The subjects consisted of 36 fourth grade students; 18 randomly assigned to the experimental and 18 randomly to the control group" (p 725, abstract). Method of randomisation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment was not described. Potentially unconcealed procedure |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Blinding procedures were not reported. It was not clear if some students within a single school participated the intervention while others received no intervention. This would increase the risk of contamination |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Method of assessment (group or individual administration) was not specified. The measures used to blind outcome assessors from knowledge of group membership was not reported |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Missing data were not reported. Attrition was not reported |
| Selective reporting (reporting bias) | Low risk | All measures discussed in the methods section of the article are reported in the results |
ANCOVA: analysis of covariance CKAQ: Children's Knowledge of Abuse Questionnaire CSA: child sexual abuse RCT: randomised controlled trial PPQ: Parental Perception Questionnaire PSQ: Personal Safety Questionnaire WIST: What If Situations Test WLC: wait list control
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ages 1991 | Pre‐test and post‐test study. No control group |
| Alexander 1998 | Post‐test only study. No control group. No random allocation of students or classes to groups |
| Araji 1995 | Pre‐test and post‐test study. No control group |
| Bae 2009 | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Baker 2013 | Quasi‐experimental study. No random allocation of students or classes to groups |
| Baker 2014 | Intervention is about sexual violence in peer dating relationships. Quasi‐experimental study. No random allocation of students or classes to groups |
| Barron 2013 | Quasi‐experimental study. No random allocation of students or classes to groups |
| Binder 1987a | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Bodzy 1988 | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| Boyle 2005 | Not school‐based |
| Briggs 1994 | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Briggs 1996 | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Casper 1999 | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Conte 1985 | Not school‐based |
| Counts 2003 | Controlled before‐and‐after study. No random allocation of students or classes to groups. Students' results selected randomly from an archival pool |
| Currier 1996 | Comparative group design (abused versus non‐abused children). Not school‐based |
| Deretzotes 1989 | Quasi‐experimental study. No random allocation of students or classes to groups |
| Dhooper 1995 | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| Foshee 1996 | Intervention is about dating and relationship violence prevention. Reports baseline findings for Foshee 1998 |
| Foshee 1998 | Intervention is about dating and relationship violence prevention. This study is included in the Cochrane Review of Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults (Fellmeth 2013) |
| Garbarino 1987 | Post‐test only study. No control group |
| Herman 1987 | Pre‐test and post‐test with multiple baseline study. No control group. No random allocation of students or classes to groups |
| Jacobs 1995 | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Johnson 1994 | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Johnson 2006 | Intervention is about abduction prevention. Not school‐based |
| Kernsmith 2011 | Intervention is about rape and sexual relationship victimisation prevention. Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Kindt 1995 | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| Kolko 1987 | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| MacIntyre 1999a | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| MacIntyre 1999b | Cross‐sectional comparative study |
| Madak 1992 | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Martin 2012 | Intervention is about coercive sexual relationships prevention. Controlled before‐and‐after study. No random allocation of students or classes to groups |
| Michaelson 2001 | Controlled before‐and‐after study + Solomon 4‐group design. No random allocation of students or classes to groups |
| Miller 2011 | Intervention is about sexual violence prevention in the context of partner relationships This study is included in the Cochrane Review of Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults (Fellmeth 2013) |
| Miller 2012 | Intervention is about sexual violence prevention in the context of partner relationships This study is included in the Cochrane Review of Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults (Fellmeth 2013) |
| Miller 2013 | Intervention is about sexual violence prevention in the context of partner relationships This study provides follow‐up data for Miller 2012, which is included in the Cochrane Review of Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults (Fellmeth 2013) |
| Moreno‐Manso 2014 | Intervention is about prevention of physical neglect and emotional abuse (i.e. broader focus than prevention of child sexual abuse). Quasi‐experimental study. No random allocation of students or classes to groups |
| Ogunfowokan 2012 | Participants outside age criteria (13 to 24 years of age) |
| Pacifici 2001 | Intervention is about coercive sexual relationships prevention. This study is included in the Cochrane Review of Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults (Fellmeth 2013) |
| Peraino 1990 | Not school‐based (preschool) |
| Pohl 1990 | Post‐test only design. No control group. No random allocation of students or classes to groups |
| Smothers 2011 | Pre‐test and post‐test study. No control group. No random allocation of students or classes to groups |
| Taal 1997 | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| Taylor 1991 | Post‐test only design. No random allocation of students or classes to groups |
| Taylor 2010a | Intervention is about gender violence and harassment. This study was excluded in the Cochrane Review of Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults (Fellmeth 2013) on the basis of participant age |
| Taylor 2010b | Intervention is about gender violence and harassment. This study was excluded in the Cochrane Review of Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults (Fellmeth 2013) on the basis of participant age |
| Telljohann 1997 | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| Tutty 1991 | Quasi‐experimental study. No random allocation of students or classes to groups |
| Tutty 1992 | Quasi‐experimental study. No random allocation of students or classes to groups |
| Volpe 1984 | Post‐test only study. No random allocation of students or classes to groups |
| Warden 1997 | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| Weatherley 2012 | Controlled before‐and‐after study. No random allocation of students or classes to groups |
| Webb 1997 | Not school‐based |
| Weisz 2001 | Intervention is about dating and relationship violence prevention. This study was excluded in the Cochrane Review of Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults (Fellmeth 2013) as it was not a RCT |
| Wurtele 1987a | Pre‐test and post‐test study. No control group |
RCT: randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
NCT02181647.
| Trial name or title | Safe touches: a rigorous evaluation of a sexual abuse prevention program for children |
| Methods | Randomised controlled trial |
| Participants | Students: second and third graders at participating New York City public schools, at least 7 years old, have not participated in Safe Touches programme in the past |
| Interventions | Behavioural: Safe Touches: Personal Safety Training for Children The intervention includes a 50‐minute interactive training and an age‐appropriate activity book on personal body safety to take home and complete with caregivers. Using culturally appropriate puppets, workshop facilitators use role‐play to model scenarios to help children: a) recognise safe and not‐safe touches, b) understand body safety, c) practise assertiveness skills, and d) help children identify whom they can go to for help |
| Outcomes | Children's Knowledge of Abuse Questionnaire |
| Starting date | Start date: April 2012 Completion date: June 2014 |
| Contact information | Principal Investigator: Mary L. Pulido, Ph.D, The New York Society for the Prevention of Cruelty to Children |
| Notes | This study was not assessed for inclusion as published studies reporting its conduct and results are not yet available |
Differences between protocol and review
There are five main differences between the protocol, Zwi 2003, and the review update.
Types of outcome measures. On p 2 of the review protocol, five outcomes were specified: (i) the development of protective behaviours; (ii) knowledge of sexual abuse and abuse prevention concepts; (iii) retention of knowledge over time; (iv) parental or child anxiety; and (v) disclosure of sexual abuse by child or adolescent during or after participating in programmes. In this review update we reported on six more precise outcomes: (i) protective behaviours; (ii) knowledge (questionnaire‐based knowledge and vignette‐based knowledge); (iii) retention of protective behaviours over time; (iv) retention of knowledge over time; (v) harm manifesting as parental or child anxiety or fear; and (vi) disclosures of past or current child sexual abuse.
Measures of treatment effect. On p 4 of the review protocol, calculation of odds ratios (OR) for dichotomous outcomes was specified in strategies for data synthesis, while relative risk (RR) and risk difference (RD) were specified for reporting on dichotomous measures of treatment effects. In this review update, we used the OR as this is the statistic used most often in this field and for ease of interpretation.
Unit of analysis issues. On p 4 of the review protocol, we indicated we would adjust for unit of analysis errors where the ICC was available. However, ICCs were not reported in the studies or available from study authors. Instead, we used estimates of 0.1 and 0.2 that had been previously used in a review of school‐based violence prevention programmes (Mytton 2006).
Dealing with missing data. Requirements for Cochrane Reviews have changed since this study's protocol was written. In this review update we identified the following types of missing data: missing outcomes, missing summary data, and missing participants. For missing outcomes (e.g. disclosures, adverse outcomes) and missing summary data (i.e. group size totals, means, standard deviations (SDs)), we contacted corresponding study authors to provide outstanding data.
Data synthesis. Before starting the 2015 update of this review we had intended to combine data with a fixed effect model in the absence of moderate statistical heterogeneity (I square <30%) and to adopt a random effects model where I square exceeded this threshold. Further consideration of the differences between the characteristics of the included studies prompted us to revise this approach. We decided to use a random effects model throughout the review in the expectation that variation between the results of the studies represented a distribution of related intervention effects.
Subgroup analyses. On p 4 of the review protocol, we specified the conduct of subgroup analyses to determine differential effects according to participant age, gender and previous reported abuse, and intervention type (passive or active involvement of participants). Subgroup analyses were only conducted for age, but not for other variables, as there was insufficient information provided in the included studies.
Contributions of authors
The original protocol and review was developed and written by Karen Zwi, Susan Woolfenden, Danielle M Wheeler, Tracey O'Brien, Paul Tait, and Katrina J Williams. Danielle Wheeler and Joanne Abbott (TSC for the Cochrane Developmental, Psychosocial and Learning Problems Group) conducted searches for the review.
Trial selection was performed by KW, KZ, SW, and AS. Data extraction and assessment of risk of bias were performed by KW, KZ, SW, and AS. Building on the original review, KW led the re‐writing of results, discussion, and conclusions with input from all authors.
Sources of support
Internal sources
No sources of support supplied
External sources
Financial Markets Foundation for Children, Australia.
Nordic Campbell Centre, Denmark.
Queensland University of Technology Vice Chancellor's Research Fellowship, Australia.
Declarations of interest
Kerryann Walsh ‐ acknowledges the Australian Research Council Discovery Projects Scheme (DP1093717) funding for research about sexual abuse prevention programmes in Australia that was conducted in parallel to this review.
Karen Zwi and Susan Woolfenden have access to 'training, education, and study leave' (TESL) funds from their organisation, to attend conferences to present or to learn. This pays for travel, accommodation, per diem allowance, and registration fees.
Aron Shlonsky ‐ none known.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Blumberg 1991 {published and unpublished data}
- Blumberg EJ. The Effects of Two Sexual Abuse Prevention Training Programs on the Evaluation of Touches [MA Psych thesis]. San Diego: San Diego State University, 1987. [Google Scholar]
- Blumberg EJ, Chadwick MW, Fogarty LA, Speth TW, Chadwick DL. The touch discrimination component of sexual abuse prevention training: unanticipated positive consequences. Journal of Interpersonal Violence 1991;6(1):12‐28. [Google Scholar]
- Chadwick MW. A Comparative Evaluation of Two Sexual Abuse Prevention Programs for Children [PhD thesis]. Irvine, United States: University of California, 1989. [Google Scholar]
Chen 2012 {published and unpublished data}
- Chen YI, Fortson BL, Tseng KW. Pilot evaluation of a sexual abuse prevention program for Taiwanese children. Journal of Child Sexual Abuse 2012;21(6):621‐45. [DOI] [PubMed] [Google Scholar]
Crowley 1989 {unpublished data only}
- Crowley KJ. Evaluation of Good Touches/Bad Touches: A Program to Prevent Child Sexual Abuse in School Age Children [Psy.D. thesis]. New York, United States: Pace University, 1989. [Google Scholar]
Daigneault 2012 {published data only}
- Daigneault I, Hébert M, McDuff P, Frappier JY. Evaluation of a sexual abuse prevention workshop in a multicultural, impoverished urban area. Journal of Child Sexual Abuse 2012;21(5):521‐42. [DOI] [PubMed] [Google Scholar]
Dake 2003 {published data only}
- Dake JA, Price JH, Murnan J. Evaluation of a child abuse prevention curriculum for third‐grade students: assessment of knowledge and efficacy expectations. Journal of School Health 2003;73(2):76‐82. [DOI] [PubMed] [Google Scholar]
Dawson 1987 {unpublished data only}
- Dawson GF. An Evaluation of Cognitive and Affective Outcomes of a Prevention Program for Childhood Sexual Abuse [EdD thesis]. Tennessee, United States: Memphis State University, 1987. [Google Scholar]
Del Campo Sanchez 2006 {published data only}
- Campo Sanchez A, Sanchez F. Evaluation of school‐based child sexual abuse prevention program [Evaluacion de un programa de prevencion de abusos sexuales a menores en Educacion Primaria]. 2006 Psicothema;18(1):1‐8. [PubMed] [Google Scholar]
Fryer 1987a {published data only}
- Fryer Jr GE, Kraizer SK, Miyoshi T. Measuring actual reduction of risk to child abuse: a new approach. Child Abuse & Neglect 1987;11(2):173‐9. [DOI] [PubMed] [Google Scholar]
- Fryer Jr GE, Kraizer SK, Miyoshi T. Measuring children's retention of skills to resist stranger abduction: use of the simulation technique. Child Abuse & Neglect 1987;11(2):181‐5. [DOI] [PubMed] [Google Scholar]
Grendel 1991 {unpublished data only}
- Grendel MA. Cognitive and Emotional Effects of a Brief Child Sexual Abuse Prevention Program for First Graders [EdD thesis]. Ohio, United States: University of Cincinnati, 1991. [Google Scholar]
Harvey 1988 {published data only}
- Harvey P, Forehand R, Brown C, Holmes T. The prevention of sexual abuse: examination of the effectiveness of a program with kindergarten‐age children. Behavior Therapy 1988;19(3):429‐35. [Google Scholar]
Hazzard 1991 {published data only}
- Hazzard A, Webb C, Kleemeier C, Angert L, Pohl J. Child sexual abuse prevention: evaluation and one‐year follow‐up. Child Abuse & Neglect 1991;15(1‐2):123‐38. [DOI] [PubMed] [Google Scholar]
Hébert 2001 {published data only}
- Hébert M, Lavoie F, Piche C, Poitras M. Proximate effects of a child sexual abuse prevention program in elementary school children. Child Abuse & Neglect 2001;25(4):505‐22. [DOI] [PubMed] [Google Scholar]
Kolko 1989 {published data only}
- Kolko DJ, Moser JT, Hughes J. Classroom training in sexual victimization awareness and prevention skills: an extension of the Red Flag/Green Flag people program. Journal of Family Violence 1989;4(1):25‐45. [Google Scholar]
Krahé 2009 {published data only}
- Krahé B, Knappert L. A group‐randomized evaluation of a theatre‐based sexual abuse prevention programme for primary school children in Germany. Journal of Community & Applied Social Psychology 2009;19(4):321‐9. [Google Scholar]
Kraizer 1991 {published and unpublished data}
- Kraizer S. The Safe Child Program for the Prevention of Child Abuse: Development and Evaluation of a School‐Based Curriculum [PhD thesis]. Ohio, United States: The Union Institute, 1991. [Google Scholar]
- Kraizer S, Witte SS, Fryer GE. Child sexual abuse prevention programs: what makes them effective in protecting children?. Children Today 1989;18(5):23‐7. [PubMed] [Google Scholar]
Lee 1998 {published data only}
- Lee YK, Tang CS. Evaluation of a sexual abuse prevention program for female Chinese adolescents with mild mental retardation. American Journal of Mental Retardation 1998;103(2):105‐16. [DOI] [PubMed] [Google Scholar]
Oldfield 1996 {published data only}
- Oldfield D, Hays BJ, Megel ME. Evaluation of the effectiveness of Project Trust: an elementary school‐based victimization prevention strategy. Child Abuse & Neglect 1996;20(9):821‐32. [DOI] [PubMed] [Google Scholar]
Poche 1988 {published data only}
- Poche C, Yoder P, Miltenberger R. Teaching self‐protection to children using television techniques. Journal of Applied Behavior Analysis 1988;21(3):253‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Saslawsky 1986 {published data only}
- Saslawsky DA, Wurtele SK. Educating children about sexual abuse: implications for pediatric intervention and possible prevention. Journal of Pediatric Psychology 1986;11(2):235‐45. [DOI] [PubMed] [Google Scholar]
Snyder 1986 {unpublished data only}
- Snyder CM. An Evaluation of the "Good Secrets, Bad Secrets" Assault Prevention Program [PhD thesis]. California, United States: International University, 1986. [Google Scholar]
Tutty 1997 {published data only}
- Tutty LM. Child sexual abuse prevention programs: evaluating 'Who do you tell'. Child Abuse & Neglect 1997;21(9):869‐81. [DOI] [PubMed] [Google Scholar]
- Tutty LM. What children learn from sexual abuse prevention programs: difficult concept and developmental issues. Research on Social Work Practice 2000;10(3):275‐300. [Google Scholar]
Wolfe 1986 {published data only}
- Wolfe DA, MacPherson T, Blount R, Wolfe VV. Evaluation of a brief intervention for educating school children in awareness of physical and sexual abuse. Child Abuse & Neglect 1986;10(1):85‐92. [DOI] [PubMed] [Google Scholar]
Wurtele 1986 {published data only}
- Wurtele SK, Saslawsky DA, Miller CL, Marrs SR, Britcher JC. Teaching personal safety skills for potential prevention of sexual abuse: a comparison of treatments. Journal of Consulting and Clinical Psychology 1986;54(5):688‐92. [DOI] [PubMed] [Google Scholar]
Ҫeҫen‐Eroğul 2013 {published data only}
- Ҫeҫen‐Eroğul AR, Kaf Hasirci Ӧ. The effectiveness of psycho‐educational school‐based child sexual abuse prevention training program on Turkish elementary students. Educational Sciences, Theory & Practice 2013;13(2):725‐9. [Google Scholar]
References to studies excluded from this review
Ages 1991 {published data only}
- Ages SE. An Evaluation of the Maintenance of Changes in Knowledge and Behaviour Skills Effected by a School‐Based Personal Safety Program for the Primary Grades [PhD thesis]. Ottawa, Canada: Carleton University, 1991. [Google Scholar]
Alexander 1998 {published data only}
- Alexander AD. The Assessment of a School‐Based Intervention for the Prevention of Child Sexual Abuse [EdD thesis]. Toronto, Canada: University of Toronto, 1998. [Google Scholar]
Araji 1995 {published data only}
- Araji SK, Fenton R, Straugh T. Child sexual abuse: description and evaluation of a K‐6 prevention curriculum. Journal of Primary Prevention 1995;16(2):149‐64. [DOI] [PubMed] [Google Scholar]
Bae 2009 {published data only}
- Bae J, Panuncio R. Development of computer‐assisted instruction program for child sexual abuse prevention. International Journal of Computer Science and Network Security 2009;9(3):142‐7. [Google Scholar]
Baker 2013 {published data only}
- Baker CK, Gleason K, Naai R, Mitchell J, Trecker C. Increasing knowledge of sexual abuse: a study with elementary school children in Hawai'i. Research on Social Work Practice 2013;23(2):167‐78. [Google Scholar]
Baker 2014 {published data only}
- Baker CK, Naai R, Mitchell J, Trecker C. Utilizing a train‐the‐trainer model for sexual violence prevention: findings from a pilot study with high school students of Asian and Pacific Islander descent in Hawai'i. Asian American Journal of Psychology 2014;5(2):106‐15. [Google Scholar]
Barron 2013 {published data only}
- Barron IG, Topping KJ. Exploratory evaluation of a school‐based child sexual abuse prevention program. Journal of Child Sexual Abuse 2013;22(9):931‐48. [DOI] [PubMed] [Google Scholar]
Binder 1987a {published data only}
- Binder RL, McNiel DE. Evaluation of a school‐based sexual abuse prevention program: cognitive and emotional effects. Child Abuse & Neglect 1987;11(4):497‐506. [DOI] [PubMed] [Google Scholar]
Bodzy 1988 {published data only}
- Bodzy LL. The Effects of a Personal Safety Program on Affective Measures of Child Development [EdD thesis]. Tennessee, United States: Peabody College for Teachers of Vanderbilt University, 1988. [Google Scholar]
Boyle 2005 {published data only}
- Boyle CL, Lutzker JR. Teaching young children to discriminate abusive from nonabusive situations using multiple exemplars in a modified discrete trial teaching format. Journal of Family Violence 2005;20(2):55‐69. [Google Scholar]
Briggs 1994 {published data only}
- Briggs F, Hawkins RMF. Follow‐up data on the effectiveness of New Zealand's national school‐based child protection program. Child Abuse & Neglect 1994;18(8):635‐43. [DOI] [PubMed] [Google Scholar]
Briggs 1996 {published data only}
- Briggs F, Hawkins RMF. Low socio‐economic status children are disadvantaged in the provision of school‐based child protection programmes. British Journal of Social Work 1996;26(5):664‐78. [Google Scholar]
Casper 1999 {published data only}
- Casper R. Characteristics of children who experience positive or negative reactions to a sexual abuse prevention program. Journal of Child Sexual Abuse 1999;7(4):97‐112. [Google Scholar]
Conte 1985 {published data only}
- Conte JR, Rosen C, Saperstein L, Shermack R. An evaluation of a program to prevent the sexual victimization of young children. Child Abuse & Neglect 1985;9(3):319‐28. [DOI] [PubMed] [Google Scholar]
Counts 2003 {published data only}
- Counts MA. Smart Kids/Safe Kids: Evaluation of a Child Sexual Abuse Prevention Program [PhD thesis]. Tennessee, United States: Tennessee State University, 2003. [Google Scholar]
Currier 1996 {published data only}
- Currier LL, Wurtele SK. A pilot study of previously abused and non‐sexually abused children's responses to a personal safety program. Journal of Child Sexual Abuse 1996;5(1):71‐87. [Google Scholar]
Deretzotes 1989 {published data only}
- Deretzotes DS. Evaluation of High School Level CAPTA Child Abuse Prevention Programs [PhD thesis]. Berkeley, California, United States: University of California, 1989. [Google Scholar]
Dhooper 1995 {published data only}
- Dhooper SS, Schneider PL. Evaluation of a school‐based child abuse prevention program. Research on Social Work Practice 1995;5(1):36‐46. [Google Scholar]
Foshee 1996 {published data only}
- Foshee VA, Linder GF, Bauman KE, Langwick SA, Arriaga XB, Heath JL, et al. The Safe Dates Project: theoretical basis, evaluation design, and selected baseline findings. American Journal of Preventive Medicine 1996;12(5 Suppl):39‐47. [PubMed] [Google Scholar]
Foshee 1998 {published data only}
- Foshee VA, Bauman KE, Arriaga XB, Helms RW, Koch GG, Linder GF. An evaluation of Safe Dates, an adolescent dating violence prevention program. American Journal of Public Health 1998;88(1):45‐50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Garbarino 1987 {published data only}
- Garbarino J. Children's response to a sexual abuse prevention program: a study of the Spiderman comic. Child Abuse & Neglect 1987;11(1):143‐8. [DOI] [PubMed] [Google Scholar]
Herman 1987 {published data only}
- Herman P. Evaluation of a Sexual Abuse Curriculum/Prevention Program [PhD thesis]. Washington, United States: Washington State University, 1987. [Google Scholar]
Jacobs 1995 {published data only}
- Jacobs JE, Hashima PY, Kenning M. Children's perceptions of the risk of sexual abuse. Child Abuse & Neglect 1995;19(12):1443‐56. [DOI] [PubMed] [Google Scholar]
Johnson 1994 {published data only}
- Johnson SG. The Effectiveness and Emotional Consequences of a School‐Based Child Sexual Abuse Prevention Program [MSCP thesis]. Sydney, Australia: Macquarie University, 1994. [Google Scholar]
Johnson 2006 {published data only}
- Johnson BM, Miltenberger RG, Knudson P, Egemo‐Helm K, Kelso P, Jostad C, et al. A preliminary evaluation of two behavioural skills training procedures for teaching abduction‐prevention skills to schoolchildren. Journal of Applied Behavior Analysis 2006;39(1):25‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kernsmith 2011 {published data only}
- Kernsmith PD, Hernandez‐Jozefowicz DM. A gender‐sensitive peer education program for sexual assault prevention in the schools. Children & Schools 2011;33(3):146‐57. [Google Scholar]
Kindt 1995 {published data only}
- Kindt MT. Evaluation of an Adolescent Sexual Abuse Prevention Program [PhD Thesis]. Ohio, United States: Bowling Green State University, 1995. [Google Scholar]
Kolko 1987 {published data only}
- Kolko DJ, Moser JT, Litz J, Hughes J. Promoting awareness and prevention of child sexual victimization using the Red Flag/Green Flag program: an evaluation with follow‐up. Journal of Family Violence 1987;2(1):11‐35. [Google Scholar]
MacIntyre 1999a {published data only}
- MacIntyre D, Carr A. Evaluation of the effectiveness of the stay safe primary prevention programme for child sexual abuse. Child Abuse & Neglect 1999;23(12):1307‐25. [DOI] [PubMed] [Google Scholar]
MacIntyre 1999b {published data only}
- MacIntyre D, Carr A. Helping children to the other side of silence: a study of the impact of the stay safe programme on Irish children's disclosures of sexual victimization. Child Abuse & Neglect 1999;23(12):1327‐40. [DOI] [PubMed] [Google Scholar]
Madak 1992 {published data only}
- Madak PR, Berg DH. The prevention of sexual abuse: an evaluation of "Talking About Touching". Canadian Journal of Counselling 1992;26(1):29‐40. [Google Scholar]
Martin 2012 {published data only}
- Martin AF, Baz M, Vicario‐Molina I, Martinez Alvarez JL, Fuertes AF, Gonzalez RJ. Assessment of a sexual coercion prevention program for adolescents. Spanish Journal of Psychology 2012;15(2):560‐70. [DOI] [PubMed] [Google Scholar]
Michaelson 2001 {published data only}
- Michaelson R. Development, Evaluation and Revision of the School‐Based Child Sexual Abuse Prevention Program (CSAPP Project) [PhD Thesis]. St Alban's, Australia: Victoria University of Technology, 2001. [Google Scholar]
Miller 2011 {published data only}
- Miller E, McCauley H, Virata MC, Decker M, Trancredi D, Moideen F, et al. Coaching boys into men: preliminary success of a sexual violence prevention program. Journal of Adolescent Health 2011;48(2 Suppl):S85‐6. [DOI] [PubMed] [Google Scholar]
Miller 2012 {published data only}
- Miller E, Tancredi DJ, McCauley HL, Decker MR, Virata MCD, Anderson HA, et al. Coaching boys into men: a cluster‐randomized controlled trial of a dating violence prevention program. Journal of Adolescent Health 2012;51(5):431‐8. [DOI] [PubMed] [Google Scholar]
Miller 2013 {published data only}
- Miller E, Tancredi DJ, McCauley HL, Decker MR, Virata MCD, Anderson HA, et al. One‐year follow‐up of a coach‐delivered dating violence prevention program: a cluster randomized controlled trial. American Journal of Preventive Medicine 2013;45(1):108‐12. [DOI] [PubMed] [Google Scholar]
Moreno‐Manso 2014 {published data only}
- Moreno‐Manso J, Garcia‐Baamonde E, Blazquez‐Alonso M, Pozueco‐Romero JM. Application of a child abuse prevention programme in an educational context. Anales de Psicologia 2014;30(3):1014‐24. [Google Scholar]
Ogunfowokan 2012 {published data only}
- Ogunfowokan AA, Fajemilehin RB. Impact of a school‐based sexual abuse prevention education program on the knowledge and attitude of high school girls. Journal of School Nursing 2012;28(6):459‐68. [DOI] [PubMed] [Google Scholar]
Pacifici 2001 {published data only}
- Pacifici C, Stoolmiller M, Nelson C. Evaluating a prevention program for teenagers on sexual coercion: a differential effectiveness approach. Journal of Consulting and Clinical Psychology 2001;69(3):552‐9. [PubMed] [Google Scholar]
Peraino 1990 {published data only}
- Peraino JM. Evaluation of a preschool antivictimization prevention program. Journal of Interpersonal Violence 1990;5(4):520‐8. [Google Scholar]
Pohl 1990 {published data only}
- Pohl JD, Hazzard A. Reactions of children, parents, and teachers to child sexual abuse prevention programs. Education 1990;110(3):337‐4. [Google Scholar]
Smothers 2011 {published data only}
- Smothers MK, Smothers DB. A sexual assault primary prevention model with diverse urban youth. Journal of Child Sexual Abuse 2011;20(6):708‐27. [DOI] [PubMed] [Google Scholar]
Taal 1997 {published data only}
- Taal M, Edelaar M. Positive and negative effects of a child sexual abuse prevention program. Child Abuse & Neglect 1997;21(4):399‐410. [DOI] [PubMed] [Google Scholar]
Taylor 1991 {published data only}
- Taylor S. An Evaluative Study of the Child Abuse Research and Education Program [Med Thesis]. Newfoundland and Labrador, Canada: Memorial University of Newfoundland, 1991. [Google Scholar]
Taylor 2010a {published data only}
- Taylor B, Stein N, Burden F. The effects of gender violence/harassment prevention programming in middle schools: a randomized experimental evaluation. Violence and Victims 2010;25(2):202‐23. [DOI] [PubMed] [Google Scholar]
Taylor 2010b {published data only}
- Taylor BG, Stein N, Burden FF. Exploring gender differences in dating violence/harassment prevention programming in middle schools: results from a randomized experiment. Journal of Experimental Criminology 2010;6(4):419‐45. [Google Scholar]
Telljohann 1997 {published data only}
- Telljohann SK, Everett SA, Price JH. Evaluation of a third grade sexual abuse curriculum. Journal of School Health 1997;67(4):149‐53. [DOI] [PubMed] [Google Scholar]
Tutty 1991 {published data only}
- Tutty LM. An Investigation of the Ability of Elementary School‐Aged Children to Learn Child Sexual Abuse Prevention Concepts [PhD thesis]. Alberta, Canada: University of Calgary, 1991. [Google Scholar]
Tutty 1992 {published data only}
- Tutty LM. The ability of elementary school children to learn child sexual abuse prevention concepts. Child Abuse & Neglect 1992;16(3):369‐84. [DOI] [PubMed] [Google Scholar]
Volpe 1984 {published data only}
- Volpe R. A psychoeducational program dealing with child abuse for elementary school children. Child Abuse & Neglect 1984;8(4):511‐7. [DOI] [PubMed] [Google Scholar]
Warden 1997 {published data only}
- Warden D, Moran E, Gillies J, Mays G, MacLeod L. An evaluation of a children's safety training programme. Education Psychology 1997;17(4):433‐48. [Google Scholar]
Weatherley 2012 {published data only}
- Weatherley R, Hajar S, Noralina O, John M, Preusser N, Yong M. Evaluation of a school‐based sexual abuse prevention curriculum in Malaysia. Children and Youth Services Review 2012;34(1):119‐25. [Google Scholar]
Webb 1997 {published data only}
- Webb A. An Evaluation of a School Based Sexual Abuse Prevention Program [MHealSc thesis]. Melbourne, Australia: Victoria University of Technology, 1997. [Google Scholar]
Weisz 2001 {published data only}
- Weisz AN. Evaluating a sexual assault and dating violence prevention program for urban youths. Social Work Research 2001;25(2):89‐102. [Google Scholar]
Wurtele 1987a {published data only}
- Wurtele SK, Marrs SR, Miller‐Perrin CL. Practice makes perfect? The role of participant modeling in sexual abuse prevention programs. Journal of Consulting and Clinical Psychology 1987;55(4):599‐602. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
NCT02181647 {published data only}
- NCT02181647. Safe touches: a rigorous evaluation of a sexual abuse prevention program for children. https://clinicaltrials.gov/ct2/show/NCT02181647 (accessed 8 February 2015).
Additional references
Adams 1984
- Adams A, Fey J. Child sexual abuse: a solution. James Stanfield Co, Inc, Santa Barbara (CA) 1984.
Albers 1991
- Albers E. Child sexual abuse programs: recommendation for refinement and study. Child and Adolescent Social Work Journal 1991;8(2):117‐25. [Google Scholar]
Anderson 1990
- Anderson C, Morris B, Robins M. Touch. Illusion Theater, Minneapolis (MN) 1990.
Andrews 2004
- Andrews G, Corry J, Slade T, Issakidis C, Swantson H. Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. In: Ezzati M, Lopez AD, Rogersand A, Murray CJL editor(s). Child Sexual Abuse. Geneva: World Health Organization, 2004. [Google Scholar]
Bandura 1986
- Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice Hall, 1986. [Google Scholar]
Barth 2013
- Barth J, Bermetz L, Heim E, Trelle S, Tonia T. The current prevalence of child sexual abuse worldwide: a systematic review and meta‐analysis. International Journal of Public Health 2013;58(3):469‐83. [DOI] [PubMed] [Google Scholar]
Battle 1981
- Battle J. Culture‐Free Self‐Esteem Inventories for Children and Adults. Seattle, Washington: Special Child Publications, 1981. [Google Scholar]
Bensley 1999
- Bensley LS, Eenwyk J, Spieker SJ, Schoder J. Self‐reported abuse history and adolescent problem behaviors. I. Antisocial and suicidal behaviors. Journal of Adolescent Health 1999;24(3):163‐72. [DOI] [PubMed] [Google Scholar]
Berrick 1991
- Berrick JD, Gilbert N. With the Best of Intentions: The Child Sexual Abuse Prevention Movement. New York: The Guilford Press, 1991. [Google Scholar]
Berrick 1992
- Berrick JD, Barth RP. Child sexual abuse prevention: research review and recommendations. Social Work Research and Abstracts 1992;28(4):6‐16. [Google Scholar]
Binder 1987b
- Binder RL, McNiel DE. Evaluation of a school‐based sexual abuse prevention program: cognitive and emotional effects. Child Abuse & Neglect 1987;11(4):497‐506. [DOI] [PubMed] [Google Scholar]
Blumberg 1987
- Blumberg EJ. The Effects of Two Sexual Abuse Prevention Training Programs on the Evaluation of Touches [MA Psych thesis]. San Diego: San Diego State University, 1987. [Google Scholar]
Boden 2007
- Boden JM, Horwood LJ, Fergusson DM. Exposure to childhood sexual and physical abuse and subsequent educational achievement outcomes. Child Abuse & Neglect 2007;31(10):1101‐14. [DOI] [PubMed] [Google Scholar]
Borenstein 2009
- Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta‐Analysis. Chichester, UK: John Wiley & Sons, 2009. [Google Scholar]
Buist 1998
- Buist A. Childhood abuse, postpartum depression and parenting difficulties: a literature review of associations. Australian and New Zealand Journal of Psychiatry 1998;32(3):370‐8. [DOI] [PubMed] [Google Scholar]
Campbell 1963
- Campbell DT, Stanley JC. Experimental and Quasi‐Experimental Designs for Research. Belmont, CA: Wadsworth Cengage Learning, 1963. [Google Scholar]
Campbell 2004
- Campbell MK, Elbourne DR, Altman DG. CONSORT Statement: extension to cluster randomised trials. BMJ 2004;328:702‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Carroll 1992
- Carroll LA, Miltenberger RG. A review and critique of research evaluating child sexual abuse prevention programs. Education and Treatment of Children 1992;15(4):335‐55. [Google Scholar]
Chadwick 1989
- Chadwick MKW. A Comparative Evaluation of Two Sexual Abuse Prevention Programs for Children [PhD thesis]. Irvine, United States: University of California, 1989. [Google Scholar]
Childhelp 2011
- Childhelp. Good Touch Bad Touch™ (GTBT) program. http://bit.ly/1L71F0Q (accessed 15 October 2013).
Church 1988
- Church P, Forehand R, Brown C, Holmes T. The prevention of sexual abuse: examination of the effectiveness of a program with kindergarten‐age children. Behaviour Therapy 1988;19(3):429‐35. [Google Scholar]
Conte 1986
- Conte JR, Rosen C, Saperstein L. An analysis of programs to prevent the sexual victimization of children. Journal of Primary Prevention 1986;6(3):141‐55. [DOI] [PubMed] [Google Scholar]
Cooper 1991
- Cooper SJ. New Strategies for Free Children: Child Abuse Prevention for Elementary School Children. Columbus, OH: The National Assault Prevention Center, 1991. [Google Scholar]
CSPV 2013
- Center for the Study and Prevention of Violence. Blueprints for healthy youth development. www.blueprintsprograms.com/ (accessed 15 October 2013).
Daro 1991
- Daro DA. Child sexual abuse prevention: separating fact from fiction. Child Abuse & Neglect 1991;15(1‐2):1‐4. [DOI] [PubMed] [Google Scholar]
Daro 1994
- Daro DA. Prevention of child sexual abuse. The Future of Children 1994;4(2):198‐223. [PubMed] [Google Scholar]
Davis 2000
- Davis MK, Gidycz CA. Child sexual abuse prevention programs: a meta‐analysis. Journal of Clinical Child Psychology 2000;29(2):257‐65. [DOI] [PubMed] [Google Scholar]
Duane 2002
- Duane Y, Carr A. Prevention: what works with children and adolescents. In: Carr A editor(s). Prevention of Child Sexual Abuse. New York: Brunner‐Routledge, 2002:181‐204. [Google Scholar]
Dunn 1981
- Dunn LM, Dunn LM. Peabody Picture Vocabulary Test‐Revised. Circle Pines, MN: American Guidance Service, 1981. [Google Scholar]
Egger 1997
- Egger M, Davey‐Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315(7109):629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fang 2012
- Fang X, Brown DS, Florence CS, Mercy JA. The economic burden of child maltreatment in the United States and implications for prevention. Child Abuse & Neglect 2012;36(2):156‐65. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fellmeth 2013
- Fellmeth GLT, Heffernan C, Nurse J, Habibula S, Sethi D. Educational and skills‐based interventions for preventing relationship and dating violence in adolescents and young adults. Cochrane Database of Systematic Reviews 2013, Issue 6. [DOI: 10.1002/14651858.CD004534.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fergusson 1996
- Fergusson DM, Lynskey MT, Horwood LJ. Childhood sexual abuse and psychiatric disorder in young adulthood: I. Prevalence of sexual abuse and factors associated with sexual abuse. Journal of the American Academy of Child and Adolescent Psychiatry 1996;35(10):1355‐64. [DOI] [PubMed] [Google Scholar]
Finkelhor 1986
- Finkelhor D, Barron L. Risk factors for child sexual abuse. Journal of Interpersonal Violence 1986;1(1):43‐71. [Google Scholar]
Finkelhor 1990
- Finkelhor D, Hotaling G, Lewis IA, Smith C. Sexual abuse in a national survey of adult men and women: prevalence, characteristics, and risk factors. Child Abuse & Neglect 1990;14(1):19‐28. [DOI] [PubMed] [Google Scholar]
Finkelhor 1992
- Finkelhor D, Strapko N. Sexual abuse prevention education: a review of evaluation studies. In: Willis DJ, Holden EW, Rosenberg M editor(s). Prevention of Child Maltreatment: Developmental and Ecological Perspectives. Hoboken, NJ: John Wiley & Sons, 1992:150‐67. [Google Scholar]
Finkelhor 1993
- Finkelhor D. Epidemiological factors in the clinical identification of child sexual abuse. Child Abuse & Neglect 1993;17(1):67‐70. [DOI] [PubMed] [Google Scholar]
Finkelhor 1995a
- Finkelhor D, Asidigian N, Dziuba‐Leatherman J. Victimization prevention programs for children: a follow‐up. American Journal of Public Health 1995;85(12):1684‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Finkelhor 1995b
- Finkelhor D, Asdigian N, Dziuba‐Leatherman J. The effectiveness of victimization prevention instruction: an evaluation of children's responses to actual threats and assaults. Child Abuse & Neglect 1995;19(2):141‐53. [DOI] [PubMed] [Google Scholar]
Finkelhor 1995c
- Finkelhor D, Dziuba‐Leatherman J. Victimization prevention programs: a national survey of children's exposure and reactions. Child Abuse & Neglect 1995;19(2):129‐39. [DOI] [PubMed] [Google Scholar]
Finkelhor 2007
- Finkelhor D. Prevention of sexual abuse through educational programs directed toward children. Pediatrics 2007;129(3):640‐5. [DOI] [PubMed] [Google Scholar]
Finkelhor 2008
- Finkelhor D. Childhood Victimization: Violence, Crime, and Abuse in the Lives of Young People. New York: Oxford University Press, 2008. [Google Scholar]
Flandreau‐West 1984
- Flandreau‐West P. Protective Behaviors: Anti‐Victim Training for Children, Adolescents and Adults. Madison, WI: Protective Behaviors Inc, 1984. [Google Scholar]
Fleming 1999
- Fleming J, Mullen PE, Sibthorpe B, Bammer G. The long‐term impact of childhood sexual abuse in Australian women. Child Abuse & Neglect 1999;23(2):145‐59. [DOI] [PubMed] [Google Scholar]
Fryer 1987b
- Fryer Jr GE, Kraizer SK, Miyoshi T. Measuring children's retention of skills to resist stranger abduction: use of the simulation technique. Child Abuse & Neglect 1987;11(2):181‐5. [DOI] [PubMed] [Google Scholar]
Gibson 2000
- Gibson LE, Leitenberg H. Child sexual abuse prevention programs: do they decrease the occurrence of child sexual abuse?. Child Abuse & Neglect 2000;24(9):1115‐25. [DOI] [PubMed] [Google Scholar]
Girard 1985
- Girard LW. Who is a Stranger and What Should I Do?. Morton Grove, IL: Albert Whitman & Company, 1985. [Google Scholar]
Grimm 1994
- Grimm C, Haseltine B, Schwandt P. Red Flag/Green Flag People II: A Sexual Abuse Prevention Program for Older Elementary Age Children. Fargo, ND: Rape and Abuse Crisis Center, 1994. [Google Scholar]
Harter 1982
- Harter S. Perceived Competence Scale for Children. Child Development 1982;53(1):87‐97. [PubMed] [Google Scholar]
Heidotting 1994
- Heidotting T, Keiffer S, Soled SW. A quantitative synthesis of child sexual abuse prevention programs. Paper presented at The American Educational Research Association, New Orleans. 1994.
Higgins 2002
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21(11):1539‐58. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Holmes 1998
- Holmes WD, Slap GB. Sexual abuse of boys: definition, prevalence, correlates, sequelae, and management. JAMA 1998;280(21):1855‐62. [DOI] [PubMed] [Google Scholar]
Hébert 2004
- Hébert M, Tourigny M. Child sexual abuse prevention: a review of evaluative studies and recommendations for program development. Advances in Psychology Research 2004;32:111‐43. [Google Scholar]
Illusion Theater Company 1984
- Illusion Theater Company, Media Ventures Inc. Touch. MTI Teleprograms, Deerfield, IL 1984.
Irish 2010
- Irish L, Kobayashi I, Delahanty DL. Long‐term physical health consequences of childhood sexual abuse: a meta‐analytic review. Journal of Pediatric Psychology 2010;35(5):450‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ji 2013
- Ji K, Finkelhor D, Dunne M. Child sexual abuse in China: a meta‐analysis of 27 studies. Child Abuse & Neglect 2013;37(9):613‐22. [DOI] [PubMed] [Google Scholar]
Kenny 2008
- Kenny MC, Capri V, Thakkar‐Kolar RR, Ryan EE, Runyon MK. Child sexual abuse: from prevention to self‐protection. Child Abuse Review 2008;17(1):36‐54. [Google Scholar]
Ko 2001
- Ko SF, Cosden MA. Do elementary school‐based child abuse prevention programs work? A high school follow‐up. Psychology in the Schools 2001;38(1):57‐66. [Google Scholar]
Kolko 1988
- Kolko DJ. Educational programs to promote awareness and prevention of child sexual victimization: a review and methodological critique. Clinical Psychology Review 1988;8(2):195‐209. [Google Scholar]
Kraizer 1981
- Kraizer SK. Children Need to Know Personal Training Program. New York: Health Education Systems Inc, 1981. [Google Scholar]
Kraizer 1989
- Kraizer S, Witte SS, Fryer GE. Child sexual abuse prevention programs: what makes them effective in protecting children?. Children Today 1989;18(5):23‐7. [PubMed] [Google Scholar]
Leclerc 2011
- Leclerc B, Wortley R, Smallbone S. Victim resistance in child sexual abuse: a look into the efficacy of self‐protection strategies based on the offender's experience. Journal of Interpersonal Violence 2011;26(9):1868‐83. [DOI] [PubMed] [Google Scholar]
London 2005
- London K, Bruck M, Ceci SJ, Shuman DW. Disclosure of child sexual abuse: what does the research tell us about the ways that children tell?. Psychology, Public Policy, and Law 2005;11(1):194‐226. [Google Scholar]
Lopez 1997
- Lopez F, DelCampo A. Prevention of child sexual abuse [Prevención de abusos sexuales a menores]. Ministerio de Trabajo y Asuntos Sociales y Amarú Ediciones, Madrid 1997.
Macdonald 2001
- Macdonald G. Effective Interventions for Child Abuse and Neglect. Chichester, UK: John Wiley & Sons, 2001. [Google Scholar]
MacIntyre 2000
- MacIntyre D, Carr A. Prevention of child sexual abuse: implications of programme evaluation research. Child Abuse Review 2000;9(3):183‐99. [Google Scholar]
MacMillan 1994
- MacMillan HL, MacMillan JH, Offord DR, Griffith L, MacMillan A. Primary prevention of child sexual abuse: a critical review. Part II. Journal of Child Psychology and Psychiatry 1994;35(5):857‐76. [DOI] [PubMed] [Google Scholar]
MacMillan 2013
- MacMillan HL, Wathen CN. Child sexual abuse of girls. In: Garcia‐Moreno C, Riecher‐Rӧssler A editor(s). Violence Against Women and Mental Health. Basel, Switzerland: Karger, 2013:96‐106. [Google Scholar]
Marvel Comics 1984
- Marvel Comics. Spiderman and power pack. National Committee for the Prevention of Child Abuse. P.O. Box 94283, Chicago, IL 60690, 1984.
MHAWC 1984
- Mental Health Association of Westchester County. Good Touches/Bad Touches: A Child Sexual Abuse Prevention Program Part II, for Fourth Through Sixth Grades, Revised Edition. White Plains: Mental Health Association of Westchester County, Inc, 1984. [Google Scholar]
Mikton 2009
- Mikton C, Butchart A. Child maltreatment prevention: a systematic review of reviews. Bulletin of the World Health Organization 2009;87(5):353‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Miller‐Perrin 1986
- Miller‐Perrin C, Wurtele S. Harmful effects of school‐based sexual abuse prevention programs? Reassure the parents. Paper presented at the meeting of the American Psychological Association, Washington, DC. Washington, DC, 1986.
Miller‐Perrin 1990
- Miller‐Perrin CL, Wurtele SK, Kondrick PA. Sexually abused and nonabused children's conceptions of personal body safety. Child Abuse & Neglect 1990;14(1):99‐112. [DOI] [PubMed] [Google Scholar]
Mytton 2006
- Mytton J, DiGuiseppi C, Gough D, Taylor R, Logan S. School‐based secondary prevention programmes for preventing violence. Cochrane Database of Systematic Reviews 2006, Issue 3. [DOI: 10.1002/14651858.CD004606.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
National Film Board of Canada 1985
- National Film Board of Canada. Feeling yes, feeling no. Perennial Education, Evanston, IL 1985.
NCMEC 1999
- National Center for Missing and Exploited Children. Guidelines for programs to reduce child victimization: a resource for communities when choosing a program to teach personal safety to children. www.safechild.org/PDF/Guidelines%20for%20Chid%20Safety.pdf (accessed 15 October 2013).
Nowicki 1973
- Nowicki S, Strickland BR. A locus of control scale for children. Journal of Consulting and Clinical Psychology 1973;40(1):148‐54. [DOI] [PubMed] [Google Scholar]
NSW Department of School Education 1998
- New South Wales Department of School Education. Child protection education: curriculum materials to support teaching and learning in personal development, health and physical education. www.curriculumsupport.education.nsw.gov.au/primary/pdhpe/safe/cpe.htm (accessed 15 October 2013).
O'Donohue 1992
- O'Donohue W, Geer JH, Elliott A. The primary prevention of child sexual abuse. In: O'Donohue WM, Geer JH editor(s). The Sexual Abuse of Children: Theory and Research. Hillsdale, NJ: Lawrence Erlbaum Associates, 1992:477‐517. [Google Scholar]
Orpinas 1995
- Orpinas P, Kelde RS. Students for Peace Project: Second Student Evaluation. Houston, TX: University of Texas Health Science Center at Houston, School of Public Health, 1995. [Google Scholar]
Pereda 2009
- Pereda N, Guilera G, Forns M, Gómez‐Benito J. The international epidemiology of child sexual abuse: a continuation of Finkelhor (1994). Child Abuse & Neglect 2009;33(6):331‐42. [DOI] [PubMed] [Google Scholar]
Perkins 1999
- Perkins DF, Luster T. The relationship between sexual abuse and purging: findings from community‐wide surveys of female adolescents. Child Abuse & Neglect 1999;23(4):371‐82. [DOI] [PubMed] [Google Scholar]
Putnam 2003
- Putnam FW. Ten‐year research update review: child sexual abuse. Journal of the American Academy of Child and Adolescent Psychiatry 2003;42(3):269–78. [DOI] [PubMed] [Google Scholar]
RAND Corporation 2013
- RAND Corporation. Promising practices network on children, families and communities. www.promisingpractices.net/ (accessed 15 October 2013).
Rape and Abuse Crisis Center 2008
- Rape and Abuse Crisis Center of Fargo‐Moorhead. Red Flag/Green Flag People: A Personal Safety Program for Early Elementary Age Children. Fargo, ND: Rape and Abuse Crisis Center of Fargo–Moorhead, 2008. [Google Scholar]
Raven 1960
- Raven JC. Guide to the Standard Progressive Matrices. London: Lewis, 1960. [Google Scholar]
Reppucci 1991
- Reppucci ND, Herman J. Sexuality education and child sexual abuse prevention programs in the schools. Review of Research in Education 1991;17(1):127‐66. [Google Scholar]
Reppucci 2005
- Reppucci DN, Haugaard JJ, Antonishak J. Is there empirical evidence to support the effectiveness of child sexual abuse prevention programs?. In: Loeske DR, Gelles RJ, Cavanaugh MM editor(s). Current Controversies in Family Violence. 2nd Edition. Thousand Oaks, CA: Sage, 2005:271‐84. [Google Scholar]
RevMan 2012 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Reynolds 1985
- Reynolds CR, Richmond BO. Revised Children's Manifest Anxiety Scale (RCMAS) Manual. Los Angeles, CA: Western Psychological Services, 1985. [Google Scholar]
Rispens 1997
- Rispens J, Aleman A, Goudena PP. Prevention of child sexual abuse victimization: a meta‐analysis of school programs. Child Abuse & Neglect 1997;21(10):975‐87. [DOI] [PubMed] [Google Scholar]
Roberts 1999
- Roberts JA, Miltenberger RG. Emerging issues in the research on child sexual abuse prevention. Education and Treatment of Children 1999;22(1):84‐102. [Google Scholar]
Roosa 1999
- Roosa MW, Reinholtz C, Angelini PJ. The relation of child sexual abuse and depression in young women: comparisons across four ethnic groups. Journal of Abnormal Child Psychology 1999;27(1):65‐76. [PubMed] [Google Scholar]
Rosenberg 1991
- Rosenberg ML, Mercy JA. Violence in America: A Public Health Approach. New York: Oxford University Press, 1991. [Google Scholar]
Sanderson 2004
- Sanderson J. Child‐focused sexual abuse prevention programs: how effective are they in preventing child abuse?. Crime and Misconduct Commission Research and Issues Paper Series 2004;5(1):1‐8. [Google Scholar]
Schochet 2008
- Schochet PZ. Statistical power for random assignment evaluations of education programs. Journal of Educational and Behavioral Statistics 2008;33(1):62‐87. [Google Scholar]
Schwab‐Stone 1995
- Schwab‐Stone ME, Ayers TS, Kasprow W, Voyce C, Barone C, Shriver T, et al. No safe haven: a study of violence exposure in an urban community. Journal of the American Academy of Child and Adolescent Psychiatry 1995;34(10):1343‐52. [DOI] [PubMed] [Google Scholar]
Shulz 2010
- Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:332. [DOI] [PubMed] [Google Scholar]
Smallbone 2008
- Smallbone S, Marshall WL, Wortley R. Preventing Child Sexual Abuse: Evidence, Policy and Practice. Portland, OR: Willan Publishing, 2008. [Google Scholar]
Solomon 1949
- Solomon RL. An extension of control group design. Psychological Bulletin 1949;46(2):137‐50. [DOI] [PubMed] [Google Scholar]
Spak 1998
- Spak L, Spak F, Allebeck P. Sexual abuse and alcoholism in a female population. Addiction 1998;93(9):1365‐73. [DOI] [PubMed] [Google Scholar]
Speilberger 1966
- Speilberger CD. Anxiety and Behavior. New York: Academic Press, 1966. [Google Scholar]
Spielberger 1973
- Spielberger C. State‐Trait Anxiety Inventory for Children: Preliminary Manual. Palo‐Alto, CA: Consulting Psychologist Press, 1973. [Google Scholar]
Stoltenborgh 2011
- Stoltenborgh M, Ijzendoorn MH, Euser EM, Bakermans‐Kranenburg MJ. A global perspective on child sexual abuse: meta‐analysis of prevalence around the world. Child Maltreatment 2011;16(2):79‐101. [DOI] [PubMed] [Google Scholar]
The World Bank 2013
- The World Bank. Data: countries and economies. data.worldbank.org/country (accessed 8 February 2015).
Topping 2009
- Topping KJ, Barron IG. School‐based child sexual abuse prevention programs: a review of effectiveness. Review of Educational Research 2009;79(1):431‐63. [Google Scholar]
Trickett 1997
- Trickett PK, Horowitz L, Reiffman A, Putnam FW. Characteristics of sexual abuse trauma and the prediction of developmental outcomes. In: Cicchetti D, Toth SL editor(s). Rochester Symposium on Developmental Psychopathology. Volume VIII: The Effects of Trauma on the Developmental Process. Rochester, NY: University of Rochester Press, 1997:289‐314. [Google Scholar]
Trickett 2006
- Trickett PK. Defining child sexual abuse. In: Feerick MM, Knutson JF, Trickett PK, Flanzer SM editor(s). Child Abuse and Neglect: Definitions, Classifications, and a Framework for Research. Baltimore, MD: Paul H Brookes Publishing Co, 2006:129‐49. [Google Scholar]
Turner 2011
- Turner HA, Finkelhor D, Hamby SL, Shattuck A, Ormrod RK. Specifying type and location of peer victimization in a national sample of children and youth. Journal of Youth and Adolescence 2011;40(8):1052‐67. [DOI] [PubMed] [Google Scholar]
Tutty 1993
- Tutty LM. Parent's perceptions of their child's knowledge of sexual abuse prevention concepts. Journal of Child Sexual Abuse 1993;2(1):83‐103. [Google Scholar]
Tutty 1995
- Tutty L. The revised Children’s Knowledge of Abuse Questionnaire: development of a measure of children’s understanding of sexual abuse prevention concepts. Social Work Research 1995;19(2):112–20. [Google Scholar]
Tutty 2000
- Tutty LM. What children learn from sexual abuse prevention programs: difficult concepts and developmental issues. Research on Social Work Practice 2000;10(3):275‐300. [Google Scholar]
United Nations 1989
- United Nations. UN convention on the rights of the child. www.unicef.org/crc (accessed 8 April 2014).
Valentine 2004
- Valentine JC, DuBois DL, Cooper H. The relation between self‐beliefs and academic achievement: a meta‐analytic review. Educational Psychologist 2004;39(2):111‐33. [Google Scholar]
Vygotsky 1986
- Vygotsky L. Thought and Language. Cambridge, MA: Massachusetts Institute of Technology Press, 1986. [Google Scholar]
Walsh 2013
- Walsh K, Berthelsen D, Nicholson JM, Brandon L, Stevens J, Rachele JN. Child sexual abuse prevention education: a review of school policy and curriculum provision in Australia. Oxford Review of Education 2013;39(5):649–80. [Google Scholar]
Westcott 1999
- Westcott H, Jones D. Annotation: the abuse of disabled children. Journal of Child Psychology and Psychiatry and Allied Disciplines 1999;40(4):497–506. [PubMed] [Google Scholar]
WHO 1999
- World Health Organization. Report of the consultation on child abuse prevention. Geneva, World Health Organization,1999 (document WHO/HSC/PVI/99.1) 1999.
Widom 1999
- Widom CS. Posttraumatic stress disorder in abused and neglected children grown up. American Journal of Psychiatry 1999;156(8):1223‐9. [DOI] [PubMed] [Google Scholar]
Williams 1980
- Williams J. Red Flag/Green Flag People Coloring Book. Fargo, ND: Rape and Abuse Crisis Center, 1980. [Google Scholar]
Wurtele 1986a
- Wurtele SK. Teaching Young Children Personal Body Safety: The Behavioral Skills Training Program. Colorado Springs, CO: Wurtele, SK, 1986. [Google Scholar]
Wurtele 1986b
- Wurtele SK, Miller‐Perrin CL. An evaluation of side effects associated with participation in a child sexual abuse prevention program. Journal of School Health 1986;57(6):228‐31. [DOI] [PubMed] [Google Scholar]
Wurtele 1987b
- Wurtele SK. School‐based sexual abuse prevention programs: a review. Child Abuse & Neglect 1987;11(4):483‐95. [DOI] [PubMed] [Google Scholar]
Wurtele 1989
- Wurtele SK, Kast LC, Miller‐Perrin CL, Kondrick PA. Comparison of programs for teaching personal safety skills to preschoolers. Journal of Consulting and Clinical Psychology 1989;57(4):505‐11. [DOI] [PubMed] [Google Scholar]
Wurtele 1990
- Wurtele SK. Teaching personal safety skills to four‐year‐old children: a behavioral approach. Behavior Therapy 1990;21(1):25‐32. [Google Scholar]
Wurtele 1992
- Wurtele SK, Gillispie EI, Currier LL, Franklin CF. A comparison of teachers vs. parents as instructors of a personal safety program for preschoolers. Child Abuse & Neglect 1992;16(1):127‐37. [DOI] [PubMed] [Google Scholar]
Wurtele 1998
- Wurtele SK, Hughes JW, Owens JS. An examination of the reliability of the "what if" situations test: a brief report. Journal of Child Sexual Abuse 1998;7(1):41‐52. [Google Scholar]
Wurtele 2002
- Wurtele SK. School‐based child sexual abuse prevention. In: Schewe PA editor(s). Preventing Violence in Relationships: Interventions Across the Life Span. Washington, DC: American Psychological Association, 2002:9‐25. [Google Scholar]
Wurtele 2007
- Wurtele SK. Body Safety Training Workbook. Colorado Springs, CO: Sandy K Wurtele, 2007. [Google Scholar]
Wurtele 2009
- Wurtele SK. Preventing sexual abuse of children in the twenty‐first century: preparing for challenges and opportunities. Journal of Child Sexual Abuse 2009;18(1):1‐18. [DOI] [PubMed] [Google Scholar]
Wurtele 2010
- Wurtele S, Kenny MC. Primary prevention of child sexual abuse: child‐ and parent‐focused approaches. The Prevention of Sexual Violence: A Practitioner's Sourcebook. Holyoake, MA: NEARI Press, 2010:107‐19. [Google Scholar]
Wyatt 1999
- Wyatt GE, Loeb TB, Solis B, Carmona JV. The prevalence and circumstances of child sexual abuse: changes across a decade. Child Abuse & Neglect 1999;23(1):45‐60. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Zwi 2003
- Zwi KJ, Woolfenden SR, Wheeler DM, O'Brien TA, Tait P, Williams KW. School‐based education programmes for the prevention of child sexual abuse. Cochrane Database of Systematic Reviews 2003, Issue 4. [DOI: 10.1002/14651858.CD004380] [DOI] [PubMed] [Google Scholar]
Zwi 2007
- Zwi K, Woolfenden S, Wheeler DM, O'Brien T, Tait P, Williams KJ. School‐based education programmes for the prevention of child sexual abuse. Cochrane Database of Systematic Reviews 2007, Issue 3. [DOI: 10.1002/14651858.CD004380.pub2] [DOI] [PubMed] [Google Scholar]