

Abstract
Objective:
The lack of objective documentation of pre-neoadjuvant chemotherapy (NAC) tumour margins is a major constraint in performing safe breast conserving surgery (BCS) in patients with breast cancer. Using a novel method of marking pre-NACT tumour margins with indigenous silver wire markers, this retrospective observational study attempted to assess the feasibility of safe BCS in breast cancer patients by performing excision wide of the marked pre-NACT margins.
Materials and Methods:
This retrospective observational study was conducted on breast cancer patients who were attending our oncology centre between May, 2015 and April, 2022. All patients had received NAC followed by surgery as recommended by our multidisciplinary team. All the patients had a primary operable solitary breast cancer. We used radiopaque metallic rods made from silver to localize tumour margins prior to NAC.
Results:
Sixty-four breast cancer patients were included; none had marker-related complications. Following NAC, BCS could be easily performed in 60 patients guided by the silver markers, which were used as temporary implants and removed during surgery. Only 2 patients were seen with positive margins and were converted to mastectomy.
Conclusion:
Breast cancer localization using sterile silver markers before the initiation of NAC is safe, easy, inexpensive, and effective, causing no morbidity or significant pain to the patients.
Keywords: BCS, breast cancer, breast imaging, neoadjuvant chemotherapy, silver rod localization
Key Points
• Tumor marking before neoadjuvant chemotherapy is importnant in cases with expected complete response.
• Silver wire markers are faesible , safe and inexpensive tumor marking method.
• It is effective method and wire could be dected in nearly all cases.
Introduction
Neoadjuvant chemotherapy (NAC) has become a cornerstone of the multidisciplinary treatment approach for breast cancer and has a long history which goes back almost forty years (1). Several values have been proven for NAC, such as downsizing the breast tumour to facilitate breast conserving surgery (BCS), down-staging the axilla to allow sentinel lymph node biopsy in node positive cases and permitting in vivo tests of treatment response (2). To date, surgery is essential even in those cases which achieved complete clinical response (3). The BCS after down-staging by NAC has proven to be safe in terms of local recurrence and survival. However, selection criteria should be fulfilled, and accurate localization of the tumour bed should be carried out before surgery. Usually, marking the tumour location is difficult if no pre-treatment localization method has been performed, and the surgeon experiences a dilemma when he is unable to localize the tumour bed and sometimes finds himself forced to perform a mastectomy (4). That is why pre-treatment tumour localization has become the standard in patients undergoing NAC and planned for BCS (5). Globally, several pre-treatment localization methods have been described and accepted. Tattoo inks, radioactive iodine seeds and metallic clips have been studied. However, no standard approach has been settled upon (6). This study aimed to evaluate the safety and accuracy of an inexpensive method for marking the margins of breast tumours before initiating NAC by using radiopaque metallic rods made from silver wire.
Materials and Methods
This retrospective observational study was conducted between May, 2015 and August, 2022. All cases received NAC and then underwent subsequent surgery according to our multidisciplinary team (MDT) decision. All patients gave informed consent before enrolment in this study. Our study was approved by the local institutional board (R.22.09.1869). Patients were included when presenting with unifocal operable breast cancer which required NAC and subsequent BCS after NAC. Those with metastatic disease, inflammatory types of breast cancer, those with unplanned excision, recurrent cancer, multicentric or multifocal lesions, those with WHO performance status >2 or those with echocardiography which showed an ejection fraction (EF) ≤45% were excluded from this study. Moreover, patients who progressed on NAC were transferred for surgery and were excluded from this study. The patient and tumour characteristics are listed in Table 1.
Table 1. Patients and their tumour characteristics.
Initial Evaluation
All of the patients received anamnesis and clinical examination to assess their palpable breast tumour location, nipple and/or skin affection and enlarged locoregional lymph nodes. All cases had undergone an ultrasound guided core needle biopsy, with histopathological and immunohistochemical staining for ER, PR, HER2, and Ki67. Breast imaging included mammogram and breast magnetic resonance imaging (MRI) (if indicated as in cases of dense breast, doubtful multifocality or multicentricity, lobular cancer, or discrepancy between mammography and ultrasound). Routine metastatic work-up was carried out. Alkaline phosphatase was used for early-stage disease, and whole body computed tomography scan and bone scan for locally advanced disease. Pre-chemotherapy routine laboratory investigations (CBC, liver functions, renal functions etc.) and echocardiography were performed. According to our MDT decisions, the patients were designated for NAC followed by BCS based on their biological subtyping and the tumour/breast ratio.
Tumour Localization Prior to Neoadjuvant Therapy by Silver Wire Rods
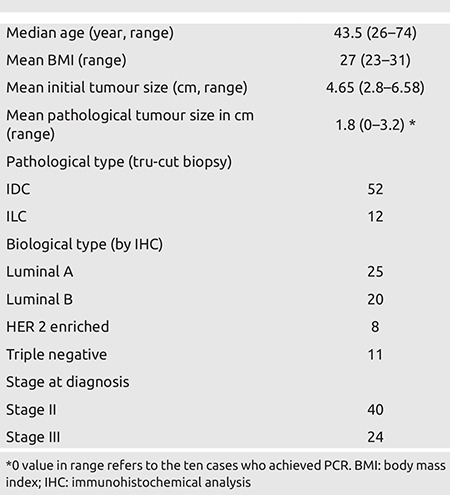
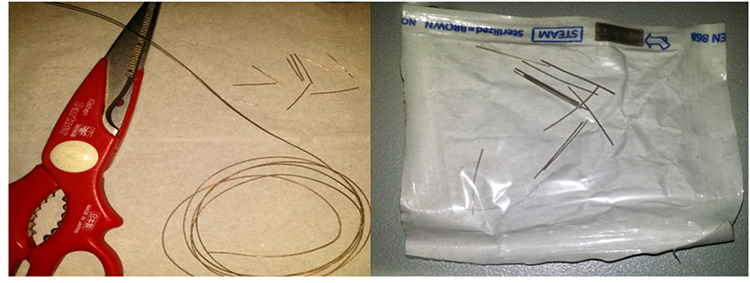
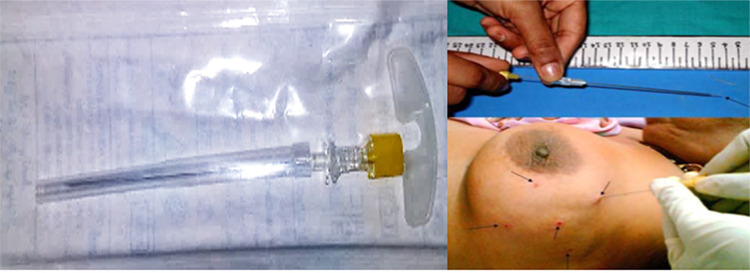
The tumour margins were marked by 3–5 metallic rods made from silver wire which was bought from a supplier as a roll and designed to be 1-meter in length and 1-mm in diameter. This roll was cut into small rods which were 2–3 cm long and were sterilized by autoclave, then kept in a plastic sterile bag (Figure 1). One metallic rod was placed at each margin of the tumour (upper, lower, medial, lateral, and posterior if possible). One metallic rod was loaded into a 20-gauge spinal needle (Figure 2), which was introduced through the skin after a local anaesthetic injection. Our radiologist propelled the spinal needle tip to reach one margin of the tumour under ultrasonography (US) guidance. The metallic rod was pushed with the needle’s stylet when the spinal needle tip touched the margin (Figure 2). This was repeated for each margin. To confirm the correct placement of the markers, a mammogram was carried out after the procedure (Figure 3, 4A).
Figure 1.
Silver wire roll cut into small rods and pocketed in a sterile plastic bag after autolaving
Figure 2.
Twenty gouge spinal needle and technique of marker insertion
Figure 3.
Post-procedural mammogram showing 4 silver markers at tumor margins
Figure 4.
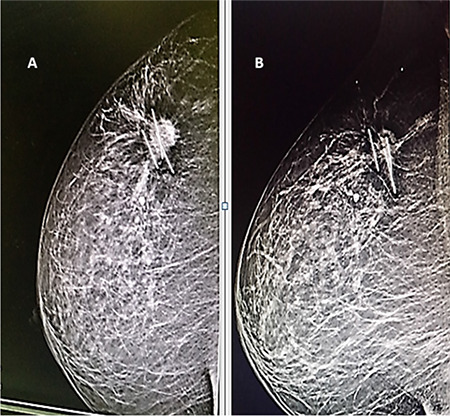
A. Pre-neoadjuvant therapy mammography showing the silver rods incorporated into the tumor margins, B. Post-treatment mammography showing marked tumor regression with the markers in place
Neoadjuvant Chemotherapy
Our patients received the standard regimens according to the molecular type and as recommended by our medical oncologists. CBC was performed before each cycle. The full course of the planned neoadjuvant therapy regimens was administered. The patients were examined after each cycle, and their response was recorded by clinical examination. The only indication for cessation of NAC and referral to surgery was disease progression.
Clinical Response
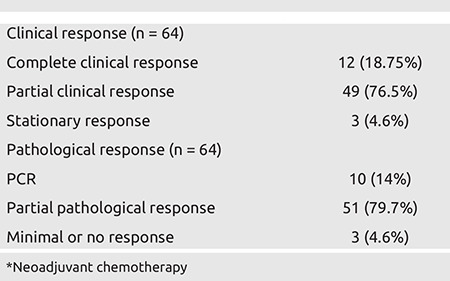
The assessment of clinical response was based on imaging studies (Table 2). US was performed for all patients to assess clinical tumour size and LN status after finishing the planned treatment (Figure 4B). Breast MRI was performed on 28 patients as requested by our radiologists. Response to treatment was categorized as complete, partial, stationary, and progressive according to RECIST criteria.
Table 2. Clinical and pathological responses to NAC*.
Surgery
After the completion of preoperative therapy, the patients underwent surgery at least 14 days after the last cycle to attain normal CBC. Patients who fulfilled the criteria for breast preservation were offered BCS either by traditional lumpectomy or by oncoplasty.
Tumour Bed Identification
Pre-operatively, if the tumour became impalpable, a skin mark was placed by the radiologist in order to allow easy identification of the tumour bed (Figure 5). When the residual lesion became invisible on imaging, the radiologist relied on the metallic markers to localize the tumour bed and place his mark. Intraoperatively, we performed wide local excision (WLE) of the tumour bed by obtaining a distance of about 1 cm to the of the palpated markers. We were usually able to detect the markers in almost all cases and used them as a guide when addressing the WLE, taking care to remove all visible or palpable rods (although there are newer tools to detect the wire but they are more sophisticated and not yet available in our practice) (Figure 6). Imaging of the specimen by mammogram was carried out in order to confirm the extraction of all markers. The pathologist could detect the rods during sectioning of the tumour (Figure 7). Confirmation of clear safety margins was performed by intraoperative frozen section examination.
Figure 5.

Preoperative skin marking at site of silver markers
Figure 6.
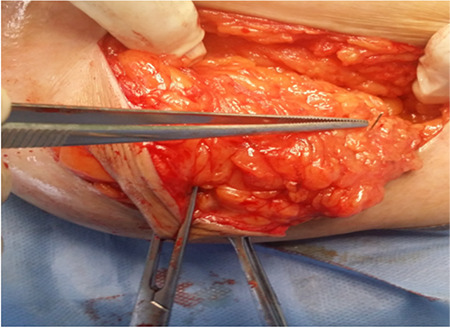
Intra-operative silver marker detection
Figure 7.
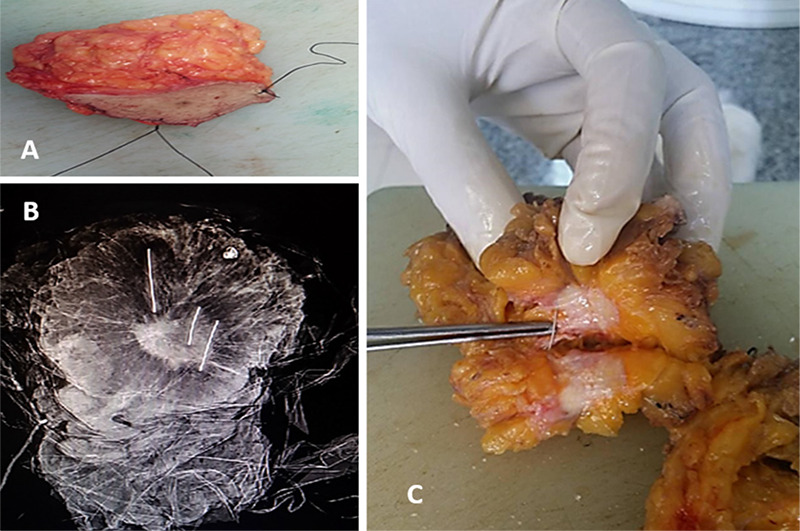
A. Lumpectomy specimen marked by threads, B. Specimen mammography showing the markers at tumor margins, C. Silver marker detected during gross pathology examination
Results
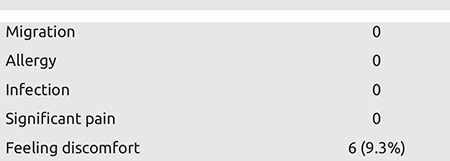
Sixty-four patients with operable breast cancer were enrolled in our study. The mean age of the cases was 43.5±10.5 years (range 26–74 years). At diagnosis, forty patients had stage II and 24 had stage III disease. Fifty-two patients had invasive duct carcinoma and 12 patients had invasive lobular carcinoma. The mean clinical tumour size was 4.65±1.6 cm. The mean pathological tumour size was 1.8±1.4 cm. At the end of the neoadjuvant course, 49 patients (76.5%) showed partial response, 3 patients (4.6%) showed stationary response and 12 patients (18.75%) showed complete response of whom, 10 (14%) had achieved pathological complete response (PCR) at their final pathological examination. The patient and tumour characteristics are provided in Table 1. Table 2 shows the clinical and pathologic response to the NAC. Metallic silver rods were placed in all cases with a median number of four (range 3–5) prior to NAC. No patient complained of pain after one day of marker insertion. Six patients complained of feeling the markers in their breast owing to its superficial placement, and their complaints were easily managed by assurance and mild analgesia. No patient had allergy, infection, or extrusion of the markers. After completion of NAC, the markers were easily detected by US in all cases without any reported migration with the radiologist fixing the new borders or clips in cases of complete response with an external marker on the patient’s skin (Table 3). In the 28 cases who had MRI, the residual lesions, if present, were clearly described despite marker artefacts, which did not substantially limit the interpretation of the radiologists. All patients underwent surgery. Sixty out of 64 patients underwent BCS and 4 patients underwent mastectomy (one patient was not amenable to BCS and mastectomy was preferred for the other 3). In all 60 patients who underwent BCS, we were able to perform WLE with 1 cm wide margins guided by the metallic markers placed at the tumour borders, which could be easily palpated in all cases. The specimen mammogram documented the primary removal of metallic markers in 56 patients at the first attempt. The other four cases required re-excision to ensure the removal of all of the markers. Fifty-eight cases had clear margins at final pathology with acceptable cosmetic results. Only two cases had positive margins and had to convert to mastectomy (conversion rate 3.3%). Table 3 shows complications related to this technique.
Table 3. Complication rate (n = 64).
Discussion and Conclusion
Neoadjuvant systemic therapy has become an integral part of the treatment panel for breast cancer. The response to neoadjuvant therapy is dramatic in some patients, and the rate of PCR has been recorded to be as high as 32.9% in some publications (6). However, an excellent response to NAC may make identification of the tumour bed extremely difficult on post treatment imaging studies, and, therefore, precise localization and safe BCS may be impossible (7). Edeiken et al. (8) found that 46.9% of tumours (23/49) were not detected on mammography after NAC. Moreover, Dash et al. (9) found that no residual tumours were visualized on 35.7% of mammograms (10/28). In such cases, preoperative marking and intraoperative identification of the tumour bed is nearly impossible if a breast tissue marker has not been placed previously. As localization is required in order to decide the extent of surgery and to guide pathologists to identify the main residual lesion, the insertion of breast tissue markers is crucial for breast cancer patients before starting NAC (10). The BCS after NAC has proven to be safe in terms of local recurrence and survival. However, to perform optimal disease eradication at WLE, the whole tumour bed situated within the pre-NAC margins should be resected (11) although there are a newer trends which recommend resection according to the new tumour borders after response to NAC (12). Typically, safe BCS after NAC is sometimes uncertain owing to the difficult identification of the tumour bed by examination and imaging studies once the tumour has regressed. Thus, marking the tumour bed before initiation or after the first few cycles of neoadjuvant therapy is crucial to perform safe BCS (13). To date, there is no standard method to mark the tumour bed prior to neoadjuvant therapy (14). Multiple tumour localization techniques have been studied. The devices used for marking the tumour site prior to chemotherapy in clinical practice include tattoo ink, radioactive iodine seeds, ultrasound detectable clips, and magnetic implants (15). Cutaneous tattoos are among the cheapest and most rapid techniques used to mark breast lesions, but they are less accurate than metallic clips (16). Another marking method is the intralesional injection of a charcoal suspension. During surgery, the target area is visually identified by the dark stain left on the patient’s skin. Its major drawbacks are the risk of colour migration to nearby healthy tissue or the risk of confusing the charcoal suspension with the tumour architecture on histopathological examination (17). Radioactive markers can be used as well. This is an effective technique, but it requires complex safety regulations (18). In addation to these methods, magnetic implants such as the MagSeed® have been approved for long-term implantation in any soft tissue, thus allowing the direct insertion of the magnetic seed in the lesion before NACT (19). However, the most popular method used in practice is commercial titanium clips. Generally, to avoid an extra session for the placement of the clips, their placement is performed in the same session of the core needle biopsy. A commercial breast marker needle is inserted through the same small incision for the core biopsy needle. As the exact response to NAC cannot be anticipated, the placement of breast markers has become routine (20). There are several versions of titanium-based commercial breast markers on the market offered by several companies. In Egypt, the price of one commercial titanium clip ranges from 3000 LE to 4000 LE which is considered too expensive and so this technique has not become popular in our country (21). In our study, we used small rods made from silver which acts as radiopaque metallic markers and are placed at the tumour margins via the well-known spinal puncture needle. The placement of the silver markers was easy to perform, and the procedure was carried out in less than 10 minutes. Since the silver rods were autoclaved, and insertion was performed with US-guidance under aseptic condition, it was considered a relatively safe technique with low complication rates. Several trials have been made to replace the expensive commercial breast clips and they have shown that low-cost metallic markers are effective for tumour localisation and do not interfere with post-treatment radiologic assessments, including MRI (22). Youn et al. (23), in South Korea, inserted surgical clips with a semiautomatic gun using a guiding needle and concluded that surgical clips are easy, safe and low cost. The same results were reported by Uematsu et al. (24), but in their study, the surgical clip was introduced via an automated gun. In 2008, Aggarwal et al. (5) published a feasibility study on safe BCS in patients with locally advanced breast cancer using silver wire to mark tumour borders prior to NAC. They performed the same technique used in our study, but the insertion of silver markers was carried out by palpation without US guidance. They concluded that these wire markers were safe, effective, and low cost. One of the possible complications of silver marker insertion is migration. The low tissue resistance of breast parenchyma may allow the rods to move from their original location; however, the rods are generally lodged in the border of the tumour with half being inside it. Thus, the possibility of marker migration was low owing to higher tissue resistance (18). Although the mean duration between marker insertion and surgery was approximately four months, there were no cases of marker migration in our study as shown in post treatment imaging studies and specimen mammograms after surgery. Additionally, other possible complications such as allergic reactions, infections and intolerable pain were not reported. Many publications have proven that radiopaque markers are crucial for tumour localization without disturbing post treatment imaging assessments, including MRI (25, 26, 27, 28). We could assess tumour response to therapy and make sure of the marker location by use of multimodal imaging studies; the markers were seen as a radiopaque metal density on mammogram, and as a hyperechoic linear structure with or without posterior shadowing on US. While breast MRI has proven better than mammography in evaluating tumour response after NAC (28, 29), metallic markers may result in artefacts on MRI, based on clip quality, magnetic susceptibility, shape, size, position, orientation, and the MRI parameters used (29). In our study, the silver markers created a small signal void on MRI; however, the residual disease was easily evaluated on MRI. In this study, even when the tumour completely disappeared in response to NAC, we were still able to identify the tumour bed preoperatively by imaging as well as intraoperative by palpation. This can explain the low rate of positive margins as we had removed the whole pathologic tissue, including all tumour-bearing breast parenchyma guided by the metallic markers placed at the tumour margins. A reduction of 2.8 cm in tumour size, on average, as revealed by the centripetal displacement of the margin markers and a reduction in the palpable tumour size suggest that the tumour tissue had been replaced by fibrotic tissue in response to NAC, leading to a shrinkage of the margins. The use of radiopaque sterile silver rods for marking the borders of breast cancer is one of the few attempts of its kind, despite the fact that they have been routinely used for marking radiation portals with good safety in different body tissues by radiotherapists (30). We used silver wire, which is available on the market in the form of rolls of one meter in length and 1 mm in diameter, which can be cut into small pieces and sterilized by autoclaving. In comparison to commercial titanium clips, the silver markers are much less expensive, and their length can be adjusted to be easily palpated in the breast tissue during BCS. The use of silver markers and the spinal puncture needle for their insertion costs approximately 40 LE. The anticipated complications associated with leaving silver markers in the breast for a few months, migration from their original site, allergic reaction and infection were not reported in any of our cases. None of the patients complained of significant pain one day after the procedure. A few patients complained of discomfort owing to the superficially placed markers, and their complaints were easily addressed by counselling. Some limitations should be discussed in this study. Firstly, this was a retrospective study, and only those patients who had accepted to have silver marker insertion and had preoperative imaging for scheduled BCS after NAC were selected. Therefore, a selection bias may exist. Secondly, the number of cases was limited to only 64, which may not allow for a generalisation of our results to the total population. Further studies are required for the evaluation of this procedure. Thirdly, the insertion of the metallic marker using a spinal puncture needle is not a globally approved method.
Breast cancer localization using sterile silver markers before the initiation of NAC is safe, easy, inexpensive, and effective, causing no morbidity or significant pain to the patients.
Footnotes
Ethics Committee Approval: Our study was approved by the Mansoura University Ethics Committee Institutional Review Board (R.22.09.1869, date: 03.11.2022).
Informed Consent: All patients gave informed consent before enrolment in this study.
Peer-review: Internally peer-reviewed.
Authorship Contributions
Surgical and Medical Practices: A.H., A.E.B., A.K., A.S., S.R., K.A., E.H.; Concept: A.H., A.E.B.; Design: A.H.; Data Collection and/or Processing: A.H., A.E.B., A.K., A.S., S.R., K.A., E.H.; Analysis and/ or Interpretation: A.H., A.K., A.S., S.R., K.A., E.H.; Literature Searching: A.H., A.K.; Writing: A.H., A.E.B., A.K., A.S., S.R., K.A., E.H.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declare that this study received no financial disclosure.
References
- 1.Killelea BK, Yang VQ, Mougalian S, Horowitz NR, Pusztai L, Chagpar AB, et al. Neoadjuvant chemotherapy for breast cancer increases the rate of breast conservation: results from the National Cancer Database. J Am Coll Surg. 2015;220:1063–1069. doi: 10.1016/j.jamcollsurg.2015.02.011. [DOI] [PubMed] [Google Scholar]
- 2.Zaher HAE, Fathy H, Abozeid M, Faisal M. Neoadjuvant chemotherapy for stage II–III breast cancer: A single-center experience. Research square. 2021. doi: 10.1186/s12957-023-03199-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Espinosa-Bravo M, Sao Avilés A, Esgueva A, Córdoba O, Rodriguez J, Cortadellas T, et al. Breast conservative surgery after neoadjuvant chemotherapy in breast cancer patients: comparison of two tumor localization methods. Eur J Surg Oncol. 2011;37:1038–1043. doi: 10.1016/j.ejso.2011.08.136. [DOI] [PubMed] [Google Scholar]
- 4.Criscitiello C, Curigliano G, Burstein HJ, Wong S, Esposito A, Viale G, et al. Breast conservation following neoadjuvant therapy for breast cancer in the modern era: Are we losing the opportunity? Eur J Surg Oncol. 2016;42:1780–1786. doi: 10.1016/j.ejso.2016.10.011. [DOI] [PubMed] [Google Scholar]
- 5.Aggarwal V, Agarwal G, Lal P, Krishnani N, Mishra A, Verma AK, et al. Feasibility study of safe breast conservation in large and locally advanced cancers with use of radiopaque markers to mark pre-neoadjuvant chemotherapy tumor margins. World J Surg. 2008;32:2562–2569. doi: 10.1007/s00268-007-9289-7. [DOI] [PubMed] [Google Scholar]
- 6.Koo JH, Kim EK, Moon HJ, Yoon JH, Park VY, Kim MJ. Comparison of breast tissue markers for tumor localization in breast cancer patients undergoing neoadjuvant chemotherapy. Ultrasonography. 2019;38:336–344. doi: 10.14366/usg.19004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kim SY, Moon HJ, Kim MJ, Lee SH, Kim EK. US-guided clip implantation for tumor localization in breast cancer patients who undergo neoadjuvant chemotherapy: feasibility study. J Korean Soc Ultrasound Med. 2013;32:51–58. [Google Scholar]
- 8.Edeiken BS, Fornage BD, Bedi DG, Singletary SE, Ibrahim NK, Strom EA, et al. US-guided implantation of metallic markers for permanent localization of the tumor bed in patients with breast cancer who undergo preoperative chemotherapy. Radiology. 1999;213:895–900. doi: 10.1148/radiology.213.3.r99dc34895. [DOI] [PubMed] [Google Scholar]
- 9.Dash N, Chafin SH, Johnson RR, Contractor FM. Usefulness of tissue marker clips in patients undergoing neoadjuvant chemotherapy for breast cancer. AJR Am J Roentgenol. 1999;173:911–917. doi: 10.2214/ajr.173.4.10511147. [DOI] [PubMed] [Google Scholar]
- 10.Chu QD, Adjepong-Tandoh EK, Duda RB. Locally advanced breast cancer (LABC) Surg Oncol. 2015:113–140. [Google Scholar]
- 11.Espinosa-Bravo M, Sao Avilés A, Esgueva A, Córdoba O, Rodriguez J, Cortadellas T, et al. Breast conservative surgery after neoadjuvant chemotherapy in breast cancer patients: comparison of two tumor localization methods. Eur J Surg Oncol. 2011;37:1038–1043. doi: 10.1016/j.ejso.2011.08.136. [DOI] [PubMed] [Google Scholar]
- 12.Banys-Paluchowski M, Thill M, Kühn T, Ditsch N, Heil J, Wöckel A, et al. AGO Recommendations for the Surgical Therapy of Breast Cancer: Update 2022. Geburtshilfe Frauenheilkd. 2022;82:1031–1043. doi: 10.1055/a-1904-6231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Oh JL, Nguyen G, Whitman GJ, Hunt KK, Yu TK, Woodward WA, et al. Placement of radiopaque clips for tumor localization in patients undergoing neoadjuvant chemotherapy and breast conservation therapy. Cancer. 2007;110:2420–2427. doi: 10.1002/cncr.23068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ramos M, Díez JC, Ramos T, Ruano R, Sancho M, González-Orús JM. Intraoperative ultrasound in conservative surgery for non-palpable breast cancer after neoadjuvant chemotherapy. Int J Surg. 2014;12:572–577. doi: 10.1016/j.ijsu.2014.04.003. [DOI] [PubMed] [Google Scholar]
- 15.Shalaby LASED, Moussa MM. Clip and wire localization of locally advanced malignant breast masses in patients undergoing neoadjuvant chemotherapy and breast conservation therapy. Egyptian Journal of Radiology and Nuclear Medicine. 2019;50:1–9. [Google Scholar]
- 16.Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384:164–172. Erratum in: Lancet 2019; 393: 986. doi: 10.1016/S0140-6736(13)62422-8. [DOI] [PubMed] [Google Scholar]
- 17.Clinicaltrials.Gov Website. Available Online: [Internet] https://Clinical trials.gov/Ct2 /Show/Nct02945579.2017.
- 18.Oh JL, Nguyen G, Whitman GJ, Hunt KK, Yu TK, Woodward WA, et al. Placement of radiopaque clips for tumor localization in patients undergoing neoadjuvant chemotherapy and breast conservation therapy. Cancer. 2007;110:2420–2427. doi: 10.1002/cncr.23068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sever AR, O’Brien ME, Humphreys S, Singh I, Jones SE, Jones PA. Radiopaque coil insertion into breast cancers prior to neoadjuvant chemotherapy. Breast. 2005;14:108–117. doi: 10.1016/j.breast.2004.08.008. [DOI] [PubMed] [Google Scholar]
- 20.Pinkney DM, Mychajlowycz M, Shah BA. A prospective comparative study to evaluate the displacement of four commercially available breast biopsy markers. Br J Radiol. 2016;89:20160149. doi: 10.1259/bjr.20160149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schulz-Wendtland R, Dankerl P, Bani MR, Fasching PA, Heusinger K, Lux MP, et al. Evaluation of a Marker Clip System in Sonographically Guided Core Needle Biopsy for Breast Cancer Localization Before and After Neoadjuvant Chemotherapy. Geburtshilfe Frauenheilkd. 2017;77:169–175. doi: 10.1055/s-0042-124191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Alm El-Din MA, Taghian AG. Breast conservation therapy for patients with locally advanced breast cancer. Semin Radiat Oncol. 2009;19:229–235. doi: 10.1016/j.semradonc.2009.05.005. [DOI] [PubMed] [Google Scholar]
- 23.Youn I, Choi SH, Kook SH, Choi YJ, Park CH, Park YL, et al. Ultrasonography-guided surgical clip placement for tumor localization in patients undergoing neoadjuvant chemotherapy for breast cancer. J Breast Cancer. 2015;18:44–49. doi: 10.4048/jbc.2015.18.1.44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Uematsu T, Kasami M, Takahashi K, Watanabe J, Yamasaki S, Tanaka K, et al. Clip placement after an 11-gauge vacuum-assisted stereotactic breast biopsy: correlation between breast thickness and clip movement. Breast Cancer. 2012;19:30–36. doi: 10.1007/s12282-011-0252-y. [DOI] [PubMed] [Google Scholar]
- 25.Soliman AH, Osman AM. Cost-effectiveness of ultrasound-guided surgical clips placement for breast cancer localization prior to neoadjuvant chemotherapy. The Egyptian Journal of Radiology and Nuclear Medicine. 2018;49:1163–1168. [Google Scholar]
- 26.Rüland AM, Hagemann F, Reinisch M, Holtschmidt J, Kümmel A, Dittmer-Grabowski C, et al. Using a New Marker Clip System in Breast Cancer: Tumark Vision® Clip - Feasibility Testing in Everyday Clinical Practice. Breast Care (Basel) 2018;13:116–120. doi: 10.1159/000486388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Alonso-Bartolome P, Ortega Garcia E, Garijo Ayensa F, de Juan Ferre A, Vega Bolivar A. Utility of the tumor bed marker in patients with breast cancer receiving induction chemotherapy. Acta Radiol. 2002;43:29–33. doi: 10.1080/028418502127347600. [DOI] [PubMed] [Google Scholar]
- 28.Masroor I, Zeeshan S, Afzal S, Sufian SN, Ali M, Khan S, et al. Outcome and Cost Effectiveness of Ultrasonographically Guided Surgical Clip Placement for Tumor Localization in Patients undergoing Neo-adjuvant Chemotherapy for Breast Cancer. Asian Pac J Cancer Prev. 2015;16:8339–8343. doi: 10.7314/apjcp.2015.16.18.8339. [DOI] [PubMed] [Google Scholar]
- 29.Kaufmann M, von Minckwitz G, Mamounas EP, Cameron D, Carey LA, Cristofanilli M, et al. Recommendations from an international consensus conference on the current status and future of neoadjuvant systemic therapy in primary breast cancer. Ann Surg Oncol. 2012;19:1508–1516. doi: 10.1245/s10434-011-2108-2. [DOI] [PubMed] [Google Scholar]
- 30.Baron LF, Baron PL, Ackerman SJ, Durden DD, Pope TL Jr. Sonographically guided clip placement facilitates localization of breast cancer after neoadjuvant chemotherapy. AJR Am J Roentgenol. 2000;174:539–540. doi: 10.2214/ajr.174.2.1740539. [DOI] [PubMed] [Google Scholar]