

ABSTRACT
Virility and sexual pleasure have long been associated with penile size and this, in turn, has typically been linked to some anthropometric measurements, such as foot size or height, leading to various misconceptions from both men and women. Our intention is to estimate penile size parameters in Argentina and evaluate the correlation between penile size and certain anthropometric measurements. This is a cross-sectional, descriptive, multicenter, and observational study. Male patients who underwent a urological procedure were included in four hospitals located in different regions of the country. Different anthropometric measurements were obtained: height, weight, penile circumference, flaccid and stretched length, and foot length. A total of 800 patients were evaluated. Mean left foot was 26.4 cm. Mean flaccid penile length was 11.4 (95% confidence interval [CI]: 8–14) cm, and mean penile circumference was 10.1 (95% CI: 8–12) cm. Finally, mean stretched penis was 15.2 (95% CI: 11–18.5) cm. We can confirm that estimates of the average penile measurements in Argentina are flaccid penis length of 11.4 cm, penile circumference of 10.1 cm, and stretching the penis to the maximum in flaccidity of 15.2 cm. Correlations between flaccid penis length, stretched out, penile circumference, height, weight, and length of the left foot were evaluated, finding low or no correlation between those mentioned, except for flaccid and stretched length.
Keywords: anthropometric measurements, micropenis, penile, percentile
INTRODUCTION
Virility and sexual pleasure have long been associated with penile size and this, in turn, has typically been linked to some anthropometric measurements, such as foot size or height, leading to various misconceptions from both men and women.
Although sexual customs have evolved over time, the importance of penile size is still a relevant issue. Office visits because of “small penis anxiety” (also known as “small penis syndrome”) are common. The literature describes this as suffered by men who have a penis with a normal size but believe it is small and consequently, they are excessively self-conscious.1,2
For male patients, penis size can be a sign of masculinity and sexual performance. Some men are afraid that their penis size might be negatively appraised by either sexual partners or peers, and generally give it more significance than women.3,4 Although some studies show an alleged standard penile size, men around the world differ in their physiognomy so measurements should not be extrapolated across countries.
Several countries have carried out studies on penile size and its correlation with different anthropometric measures.5,6,7,8,9,10,11,12,13 This is an original study in Argentina. The aim is to inform and adequately advise the patient who comes to the office to try to solve problems he thinks he has with the size of his penis.
The primary objective of this study is to estimate penile size parameters in Argentina and evaluate the correlation between penile size and certain anthropometric measurements.
PARTICIPANTS AND METHODS
This is a multicenter descriptive cross-sectional observational study conducted with data prospectively collected from and ethically approved by a sample of 800 male patients from July 2017 to December 2020.
The sample is composed by male patients born in Argentina, over 18 years of age, who underwent urological procedures for pathologies other than penile size performed with general anesthesia in four hospitals located in different regions of Argentina (the department of Urology at Hospital Italiano, Buenos Aires; Sanatorio Allende, Córdoba; Hospital Privado de la Comunidad, Mar del Plata; and Hospital Central, Mendoza).
Patients with congenital or acquired anomalies of the penis, such as Peyronie’s disease, partial or total penectomies, penile prosthesis, urethral surgeries, severe phimosis, and those who did not consent to our research protocol were excluded.
Trained medical personnel from the Department of Urology of the hospitals cited above obtained prior consent of the patient, various anthropometric measurements, namely height, weight, flaccid penile length, stretched penile length, penile base circumference, and foot length using a centimeter. All measurements were taken in centimeters (cm) and weight in kilograms (kg). The moment was during the patient’s anesthetic induction, lying in supine position.
To measure the length of the flaccid penis, the pubic bone (exerting pressure on the prepubic fat) and the tip of the glans with the foreskin retracted were taken as reference points. The circumference was measured at the base of the flaccid penis. To measure flaccid stretched penis, the same abovementioned criteria were considered, from pubic bone to glans tip with retracted foreskin, stretching it to the maximum (Figure 1).14 Regarding the foot, the left foot was measured in all cases, from the tip of the thumb to the end of the heel. Information regarding height, weight, body mass index (BMI), and age has been collected from anesthetic records.
Figure 1.

Procedure for penile measurements. The arrows show the pubic bone and the tip of the glans with the foreskin retracted.
The data collected were entered into a spreadsheet preserving the anonymity of patients. This research was approved by the Bioethics Committee of the Hospital Italiano de Buenos Aires, Buenos Aires, Argentina (approval No. CEPI N 3893).
To estimate the penile size of the study population, a precision calculation was performed. The software used was SPSS 22.0 (IBM Corp, New York, NY, USA). For an average 14-cm estimate (based on a previous exploratory study) with a 95% confidence interval (CI) between 13.82 cm and 14.17 cm, the inclusion of 800 patients was deemed necessary. A total of 200 patients were included per center to maintain the representativeness of the population through consecutive nonprobability sampling.
Continuous variables are expressed as their mean and standard deviation (s.d.). To offer better precision on the measurements made, the medians, interquartile ranges (IQR), and percentiles 5 and 95 are also reported. To estimate correlation between variables, the Pearson correlation test is used. Correlation coefficients and P values are reported. P values under 0.05 are considered significant.
RESULTS
A total of 800 patients were evaluated, 200 of which came from each hospital. Mean age of the sample was 54.2 (s.d.: 17.6) years. Mean population height and weight were 174 (s.d.: 6.9) cm and 85.2 (s.d.: 15.7) kg, respectively. Mean left foot was 26.4 (s.d.: 1.8) cm. Mean flaccid penile length was 11.4 (s.d.: 2) cm, mean penile circumference was 10.1 (s.d.: 1.3) cm. Finally, mean stretched penis was 15.2 (s.d.: 2.2) cm. Percentiles of penile parameters studied are summarized in Table 1 and represented in Figure 2.
Table 1.
Penile measurements percentiles
| Variable | Percentile | ||||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| 0 | 5 | 25 | 50 | 75 | 95 | 100 | |
| Flaccid penile length (cm) | 6 | 8 | 10 | 11 | 13 | 14 | 16.5 |
| Penile circumference (cm) | 6 | 8 | 9 | 10 | 11 | 12 | 15 |
| Stretched penile length (cm) | 8 | 11 | 14 | 15 | 17 | 18.5 | 21.5 |
Figure 2.
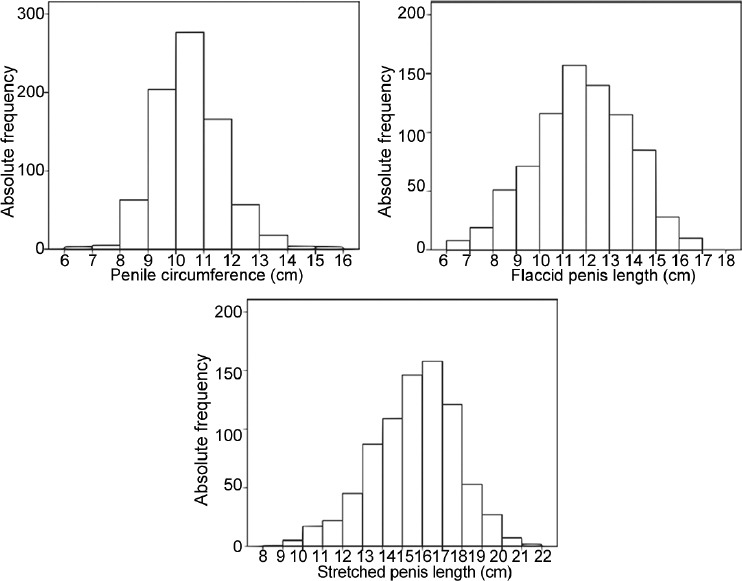
Penile measurement histograms.
Correlations between flaccid and stretched penile length, circumference, height, BMI, age, weight, and left foot length were evaluated. A low or no correlation was found between the aforementioned, with the exception of flaccid and stretched length (r = 0.7; P=0.0001; Table 2).
Table 2.
Correlation coefficients
| Variable | Flaccid penile length (cm) | Penile circumference (cm) | Stretched penile length (cm) | Left foot length (cm) | Height (cm) | Weight (kg) | BMI (kg m−2) | Age (year) |
|---|---|---|---|---|---|---|---|---|
| Flaccid penile length (cm) | NA | 0.3 | 0.7* | 0.2 | 0.2 | −0.1 | −0.1 | −0.1 |
| Penile circumference (cm) | 0.3 | NA | 0.4 | 0.1 | 0.2 | 0.1 | 0.1 | 0 |
| Stretched penile length (cm) | 0.7* | 0.4 | NA | 0.2 | 0.2 | −0.1 | −0.2 | −0.1 |
| Left foot length (cm) | 0.2 | 0.1 | 0.2 | NA | 0.3 | 0.2 | - | - |
| Height (cm) | 0.2 | 0.2 | 0.2 | 0.3 | NA | - | NA | - |
| Weight (kg) | −0.1 | 0.1 | −0.1 | 0.2 | - | NA | NA | - |
| BMI (kg m−2) | −0.1 | 0.1 | −0.2 | - | NA | NA | NA | - |
| Age (year) | −0.1 | 0 | −0.1 | - | - | - | - | NA |
*Statistically significant correlation between flaccid and stretched penis length. -: correlation between height and weight was not assessed as it goes beyond the scope of this research; BMI: body mass index; NA: not apply
DISCUSSION
Given the social relevance that penile size bears and its possible relationship with certain anthropometric measurements, we conducted an original study in Argentina with a representative sample, successfully obtaining average penile dimensions (flaccid and stretched penile length when maximum and flaccid penile circumference) and its correlation with height, weight, and foot length.
The literature reviewed shows significant variability in the methodology used for penile measurement and the environmental conditions in which it is carried out. We have standardized the measurement method and circumstances to ensure its repeatability with different operators and locations. Unlike Khan et al.8 who took measurements with a rigid ruler and changed the location and conditions when measuring patients of whom some in the office with room temperature, others in the operating room under general anesthesia and ambient temperatures lower than those in an office. We used a centimeter, as it can provide more accuracy in some cases (penile circumference) and we took all measurements under the same environmental conditions. Measurements in environments with different temperatures may lead to bias since cold affects penile length and manipulation of an awake patient as opposed to one under general anesthesia is different considering the discomfort or pain that the measurement can cause in the awake patient. In our study, patients were in supine position in the operating room at the same temperature and during anesthetic induction.
As to the penile measurement procedure, Habous et al.9 did not take into account sinking the prepubic fat pad when measuring penile length. This simple gesture considers a few hidden centimeters in the adipose tissue, thus giving more accuracy to the measurement. To measure the length of the erection, the patient was administered intracavernous drugs,9 said length may vary according to the response of each patient, not reaching its maximum length in some cases. To avoid variability, we stretched the penis to its maximum and depressed the prepubic pad to obtain a correct penile measurement.
As to environmental conditions for measurements, Chen et al.10 is a good example to follow to avoid biases due to external situations. In their study, penis measurement was performed by the same doctor in his office at 24°C with a rigid ruler; patients obtained an erection through self-stimulation with sex tapes and the length was assessed by exerting force controlled by the doctor. Although we agree with the environmental requirements for measurements, our methodology differs, we followed standardized methods to achieve more reliable results.
Another point to discuss is whether the stretched penile length is a good estimate of the erect penile length. Veale et al.,14 in a systematic review, state that by exerting adequate pressure to stretch the penis (it may cause pain), it is possible to obtain measurements similar to those generated by an erection. In our case, since all the patients were under general anesthesia, the correct extension of the penis could be achieved to measure its stretched length, for the pain and discomfort that may occur when the patient is awake are eliminated. Like Chen et al.10 and Wessells et al.,11 we observed adequate correlation between the stretched penile length and that in erection.
A contrastive analysis among studies on penile measures from different countries is very difficult to make because, as it was mentioned before, criteria used for measurements differ so any comparison would be unfair. Variability is reflected in the different results since some obtained positive associations between penile and anthropometric measures and others did not.
Our research is of medical importance because it allows the practitioner to be aware of reference values in a studied population, which is extremely useful when a patient inquires about possible abnormality in his penile size. Furthermore, the information published makes it possible to identify real problems in penile size in order to advise for or against invasive and noninvasive procedures to lengthen the penis or increase its circumference in cases of malformations, miscellaneous accidents, or micropenis, but not in patients with “Small penis syndrome”, who suffer from an alteration of reality and may be seduced by different procedures, many of which have not been proven effective, to increase the size of their genitals and may end up with serious secondary complications, when a better approach would be to resort to psychological or sexological assistance.15,16
In the case of micropenis, it is important to note that the numerical value varies across countries although some may show the same. According to our study population, micropenis is defined as penile measurements below the 5th percentile, i.e., a flaccid penis length less than or equal to 7 cm, a flaccid circumference less than or equal to 7 cm and a stretched penile length less than or equal to 10 cm. There is no professional consensus as to performing penile lengthening techniques below a certain measure. The safest technique known to date is physician-supervised mechanical traction as the first line. Then, there are some surgical approaches such as the section of the suspensory ligament of the penis, liposuction of the fat located in the prepubic pad or dermolipectomy, and the section of the penoscrotal junction with subsequent suture of tissues that significantly mark the angle of the penis with the scrotum, which creates a favorable visual effect. The results of these techniques are modest with a low satisfaction rate. Different techniques other than the ones mentioned here should be considered experimental since they present significant complications.17
We consider our 800-patient sample to be representative to obtain results on penile measurements of Argentine men; however, similar studies with a larger sample size should be furthered to increase accuracy and thus better advise patients. We did a nonprobability convenience sampling. A representative random sample of the entire society would have been the best way to carry out our work, but it was beyond our reach.
CONCLUSIONS
We can confirm that estimates of the average penile measurements in Argentina are flaccid penis length of 11.4 (s.d.: 2.0) cm, penile circumference of 10.1 (s.d.: 1.3) cm, and stretching the penis to the maximum in flaccidity of 15.2 (s.d.: 2.2) cm.
Correlations between flaccid penis length, stretched out, penile circumference, height, weight, and length of the left foot were evaluated, finding low or no correlation between those mentioned, except for flaccid and stretched length.
AUTHOR CONTRIBUTIONS
MS and ITG planned the project and wrote the manuscript. MS, MC, GC, MD, and BC participated in data collection. ITG performed the statistical analysis. GRV, GG, ITG, and OAL participated in the interpretation and revision of the manuscript. All authors read and approved the final manuscript.
COMPETING INTERESTS
All authors declare no competing interests.
ACKNOWLEDGMENTS
The authors thank all the residents of the institutes involved in the work for their commitment.
REFERENCES
- 1.Wylie KR, Eardley I. Penile size and the ‘small penis syndrome’. BJU Int. 2007;99:1449–55. doi: 10.1111/j.1464-410X.2007.06806.x. [DOI] [PubMed] [Google Scholar]
- 2.Veale D, Miles S, Read J, Bramley S, Troglia A, et al. Relationship between self-discrepancy and worries about penis size in men with body dysmorphic disorder. Body Image. 2016;17:48–56. doi: 10.1016/j.bodyim.2016.02.004. [DOI] [PubMed] [Google Scholar]
- 3.Veale DM, Lambrou C. The importance of aesthetics in body dysmorphic disorder. CNS Spectr. 2002;7:429–31. doi: 10.1017/s1092852900017922. [DOI] [PubMed] [Google Scholar]
- 4.Veale D, Miles S, Read J, Troglia A, Carmona L, et al. Phenomenology of men with body dysmorphic disorder concerning penis size compared to men anxious about their penis size and to men without concerns:a cohort study. Body Image. 2015;13:53–61. doi: 10.1016/j.bodyim.2014.09.008. [DOI] [PubMed] [Google Scholar]
- 5.Ponchietti R, Mondaini N, Bonafè M, Di Loro F, Biscioni S, et al. Penile length and circumference:a study on 3,300 young Italian males. Eur Urol. 2001;39:183–6. doi: 10.1159/000052434. [DOI] [PubMed] [Google Scholar]
- 6.Spyropoulos E, Borousas D, Mavrikos S, Dellis A, Bourounis M, et al. Size of external genital organs and somatometric parameters among physically normal men younger than 40 years old. Urology. 2002;60:485–9. doi: 10.1016/s0090-4295(02)01869-1. [DOI] [PubMed] [Google Scholar]
- 7.Promodu K, Shanmughadas KV, Bhat S, Nair KR. Penile length and circumference:an Indian study. Int J Impot Res. 2007;19:558–63. doi: 10.1038/sj.ijir.3901569. [DOI] [PubMed] [Google Scholar]
- 8.Khan S, Somani B, Lam W, Donat R. Establishing a reference range for penile length in Caucasian British men:a prospective study of 609 men. BJU Int. 2012;109:740–4. doi: 10.1111/j.1464-410X.2011.10338.x. [DOI] [PubMed] [Google Scholar]
- 9.Habous M, Tealab A, Williamson B, Binsaleh S, Dawy SE, et al. Erect penile dimensions in a cohort of 778 Middle Eastern men:establishment of a nomogram. J Sex Med. 2015;12:1402–6. doi: 10.1111/jsm.12894. [DOI] [PubMed] [Google Scholar]
- 10.Chen XB, Li RX, Yang HN, Dai JC. A comprehensive, prospective study of penile dimensions in Chinese men of multiple ethnicities. Int J Impot Res. 2014;26:172–6. doi: 10.1038/ijir.2014.9. [DOI] [PubMed] [Google Scholar]
- 11.Wessells H, Lue TF, McAninch JW. Penile length in the flaccid and erect states:guidelines for penile augmentation. J Urol. 1996;156:995–7. [PubMed] [Google Scholar]
- 12.Hussein NS, Abid AF, Alnuaimi AS. Reference range of flaccid and stretched penile lengths of adult males in Baghdad:a cross-sectional study. Arab J Urol. 2017;15:68–73. doi: 10.1016/j.aju.2017.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hoai BN, Minh QP, Cao TN, Sansone A, Colonnello E, et al. Data from 14,597 penile measurements of Vietnamese men. Andrology. 2021;9:906–15. doi: 10.1111/andr.12978. [DOI] [PubMed] [Google Scholar]
- 14.Veale D, Miles S, Bramley S, Muir G, Hodsoll J. Am I normal? A systematic review and construction of nomograms for flaccid and erect penis length and circumference in up to 15,521 men. BJU Int. 2015;115:978–86. doi: 10.1111/bju.13010. [DOI] [PubMed] [Google Scholar]
- 15.Ghanem H, Glina S, Assalian P, Buvat J. Position paper:management of men complaining of a small penis despite an actually normal size. J Sex Med. 2013;10:294–303. doi: 10.1111/j.1743-6109.2012.02725.x. [DOI] [PubMed] [Google Scholar]
- 16.Hehemann MC, Towe M, Huynh LM, El-Khatib FM, Yafi FA. Penile girth enlargement strategies:what’s the evidence? Sex Med Rev. 2019;7:535–47. doi: 10.1016/j.sxmr.2018.11.003. [DOI] [PubMed] [Google Scholar]
- 17.Chevallier D, Haertig A, Faix A, Droupy S. Cosmetic surgery of the male genitalia. Prog Urol. 2013;23:685–95. doi: 10.1016/j.purol.2013.02.011. [DOI] [PubMed] [Google Scholar]