

Abstract
Rationale.
Delay discounting, or the devaluation of delayed outcomes, appears to play an etiological role in tobacco and other substance-use disorders.
Objectives
No human studies to our knowledge have been designed to examine whether experimental reductions in delay discounting produce concomitant reduction in drug use.
Methods.
Using methods from prior studies on delay discounting and obesity, we examined the effects of episodic future thinking (EFT; a form of mental prospection) on delay discounting and cigarette self-administration in smokers.
Results.
Consistent with prior data, EFT significantly reduced both delay discounting (Cohen’s d effect size = 0.65) and the number of cigarette puffs earned in a cigarette self-administration task (d = 0.58).
Conclusions.
The effects of EFT on delay discounting generalize to smokers; EFT also reduces laboratory-based cigarette self-administration. Potential mechanisms of EFT’s effects are discussed as well as implications of EFT for clinical treatment of substance-use disorders.
Keywords: Delay discounting, Episodic future thinking, Prospection, Cigarettes, Smoking
The book was Maniacs in the Fourth Dimension, by Kilgore Trout. It was about people whose mental diseases couldn’t be treated because the causes… were all in the fourth dimension [time], and three-dimensional Earthling doctors couldn’t see those causes at all, or even imagine them.
Introduction
Delay discounting, or the devaluation of delayed reinforcement, serves as a reliable behavioral marker of tobacco and other drug use (Bickel et al. 2014). For example, high discount rate for commodities such as money, food, and health differentiates cigarette smokers from demographically matched controls (Odum et al. 2002; Odum and Baumann 2007) predicts initiation of smoking in adolescence (Audrain-McGovern et al. 2009) and is associated with higher indices of smoking addiction severity (e.g., Sweitzer et al. 2008; Ohmura et al. 2005). Moreover, this phenomenon appears general across species, as delay discounting is similarly associated with self-administration of nicotine and other drugs in rodent models of addiction (for review, see Stein and Madden 2013).
The role of delay discounting in tobacco and other drug may be causal, as rapid devaluation of the delayed reinforcement associated with drug abstinence (e.g., long-term good health) likely serves to increase the relative value of immediate drug effects. In this view, drug abuse and dependence are partial products of being “stuck in time,” with the long-term health costs of drug use outside of one’s restricted temporal horizon and therefore unable to impact behavior. This suggests that experimental reductions in delay discounting would be accompanied by simultaneous reductions in drug self-administration. If so, extension of such methods could, in turn, be used clinically to disrupt the immediacy bias observed in addiction and, hence, reduce drug use.
Indirect evidence along these lines comes from a recent study of delay discounting and obesity (Daniel et al. 2013a), in which we investigated the effects of episodic future thinking (EFT; i.e., mental simulation of future events; Atance and O’Neill 2001) on delay discounting and caloric intake. Overweight and obese adults in an EFT group vividly imagined positive future autobiographical events and were then presented with cues reminding them of these events during both a delay-discounting task and an eating task featuring ad libitum access to highly palatable foods. In contrast, participants in a control group were presented with temporally nonspecific cues taken from a travel journal. We found that EFT reduced not only delay discounting but also caloric intake, compared to the control condition—an approximate difference in consumption of 300 cal between groups. We subsequently reproduced these effects in both laboratory and natural settings (Daniel et al. 2015; O’Neill et al. 2016; Sze et al. 2015) and extended them to addiction, finding that EFT reduces both delay discounting and behavioral-economic demand for alcohol in alcohol-dependent participants (Snider et al. 2016).
In the present study, we examined the effects of EFT on delay discounting and cigarette self-administration in cigarette smokers. As a control condition, we employed episodic recent thinking (ERT), in which participants imagined real events that occurred the previous day. This ERT condition, used frequently in studies of EFT and delay discounting (e.g., Daniel et al. 2015; Lin and Epstein 2014;), serves to isolate the effects of prospection in active EFT by ensuring that episodic content in both groups engages memory and is autobiographical (and, hence, matched for vividness). Compared to ERT, we hypothesized that EFT would reduce delay discounting and cigarette self-administration, similar to our previously reported effects of EFT on caloric intake in overweight/obese participants. Specifically, if EFT serves to reduce delay discounting by broadening the temporal window over which individuals integrate the value of reinforcement, then EFT should reduce the behavioral impact of immediate drug reinforcement and therefore reduce cigarette smoking.
Method
Participants
Participants (N = 54) were recruited from Roanoke, VA, and surrounding areas using flyers, the internet, and word-of-mouth referral. To be eligible, participants had to meet DSM-IV criteria for nicotine dependence; smoke at least ten cigarettes per day; smoke every day for the last 30 days; exhale at least 14 ppm carbon monoxide (CO) at intake, as measured by a CO monitor (CoVita Smokerlyzer; Haddonfield, NJ); and be at least 18 years of age. Participants also had to report a desire to quit smoking, but were excluded if they reported they were actively trying to quit smoking or taking medications that aid in smoking cessation (e.g., varenicline, bupropion), met DSM-IV dependence for any drug of abuse other than nicotine, reported unstable mental or physical health, or were pregnant.
After providing informed consent, n = 26 and 28 participants were randomly assigned to the EFT or control groups, respectively. Of these, seven never returned and could not be reached, three voluntarily withdrew from the study, and two were discontinued due to changes in eligibility criteria (i.e., development of alcohol dependence or unmanaged depression due to a recent life event). This left sample sizes of n = 20 and 22 in the EFT and control groups, respectively. Terminal sample sizes were chosen to approximate those sufficient in prior studies to show an effect of EFT on discounting and energy intake (e.g., Daniel et al. 2013a, 2015).
Apparatus and materials
All experimental procedures were implemented using the Python software package (v. 2.5; Python Software Foundation) and the web-based survey software, LimeSurvey (Schmitz 2012). Participants completed sessions in ventilated smoking booths equipped with a desktop computer and a console featuring three Lindsley response plungers (Med Associates, St. Albans, VT) requiring approximately 20 N to operate. Plungers were aligned horizontally, equidistant from one another along the front of the console.
In order to measure cigarette puff volume, the computer interfaced with a pressure sensor (Rayfield Equipment, Waitsfield, VT) attached to a cigarette holder via approximately 90 cm of polyvinyl tubing. Puff-induced pressure changes were processed by an A/D card (PCI-DAS08, using Instacal software; Measurement Computing Corp., Norton, MA). During the cigarette self-administration task, the experimenters provided participants with their self-reported usual brand of cigarettes.
Procedures
Session 1.
Participants initially answered a number of demographic questions and completed the Fagerström Test for Cigarette Dependence (FTCD; Fagerström 2012) and a timeline follow-back survey (Brown et al. 1998) to estimate average daily cigarette consumption over the past 30 days.
Participants then received training on how to use the smoking apparatus. Cigarette puff volume was standardized at approximately 70 mL in this and the subsequent session (Johnson et al. 2004). Participants were trained to light a cigarette without inhaling, place it in a cigarette holder connected to the pressure sensor, and inhale from the cigarette while estimated puff volume was displayed in real time on a computer screen. Upon reaching 60 mL, the displayed puff volume turned from white to red, which signaled the approximate time participants should stop inhaling in order to reach 70 mL. Using these procedures, participants took five practice puffs before the end of the session.
Session 2.
Participants were asked to abstain from smoking for approximately 6 h prior to session 2, verified by a breath CO level less than or equal to half of that at session 1. If participants did not meet this CO criterion, session 2 was rescheduled for another time.
EFT or control cue generation.
Next, participants in both groups completed a guided interview process to generate EFT or control cues. The EFT group generated three positive, autobiographical events that could realistically occur following each of five delays in the subsequent delay-discounting task: 1 day, 1 week, 1 month, 3 months, and 1 year. In contrast, participants in the ERT control group reported three real, positive events that occurred the previous day during each of five time frames: 7:00 AM to 9:59 AM, 10:00 AM to 12:59 PM, 1:00 PM to 3:59 PM, 4:00 PM to 6:59 PM, and 7:00 PM to 9:59 PM.
Participants in both groups were told not to include events that related specifically to smoking (e.g., BI [will go/went] to the store to buy cigarettes^). Using a five-point Likert scale, both groups rated each event according to four dimensions: vividness, enjoyment, importance, and excitement. The event at each time frame that participants rated the most vivid was chosen for use in subsequent behavioral testing (ties settled randomly).
Participants were then recorded reciting a self-created two or three-sentence summary of each event (e.g., “In one year, I will be attending my sister’s wedding. My entire family will be there and I will be having a lot of fun”). These recordings served as subsequent audio cues (see below). Participants also created abbreviated versions of each description (e.g., “In one year, I will be at my sister’s wedding”) to serve as textual cues.
Delay discounting.
Following cue generation, participants completed a delay-discounting task. At each of five delays (randomly presented) in each task, participants chose between two different hypothetical amounts: US$1000 available after a delay or a smaller amount of money available immediately. The smaller amount was titrated across six consecutive trials until reaching a point of subjective equality between choice options (see Du et al. 2002). The value of this smaller amount at indifference indexes the discounted value of the larger option at each delay. This titration process was repeated at each of five delays: 1 day, 1 week, 1 month, 3 months, and 1 year. Participant-generated textual EFT or ERT cues (described above) appeared continuously on the screen during each trial. For the EFT group, the time frame of the presented cue matched that of the active task delay. For the ERT group, the time frame of each cue corresponded inversely with the active task delay (e.g., the cue for the most recent time frame from the previous day [7:00–9:59 PM] was presented during the shortest future delay [1 day]).
Cigarette self-administration.
Finally, participants completed a 60-min self-administration task, in which they could earn single cigarette puffs for each completion of a fixed-ratio (FR) ten-response requirement on one of the plungers. Following completion of each response requirement, puff self-administration procedures were identical to those practiced in session 1. Participants were instructed that they could smoke as much or as little as they wanted during the task, and that they could listen to the radio or read available magazines or newspapers, but could not read books or use cell phones or other handheld devices. Textual and audio EFT or ERT cues (described previously) were presented throughout the task with a randomly sampled inter-stimulus interval (1 – 5 s). Audio cues were used because, unlike the delay discounting task, participants were not expected to continuously attend to the computer monitor during the self-administration task. The time frame of each EFT or ERT cue at each presentation was chosen randomly with each presentation.
Data analysis
All analyses were conducted using GraphPad Prism (v. 6.05; La Jolla, CA, USA). Demographic data were compared between the EFT and ERT groups using either t tests (age, income, cigarettes per day, and FTCD scores) or Fisher’s exact tests (sex and race).
Delay discounting.
Discounting data for all participants were included in primary analyses, as the presence of data that are not systematically affected by delay and sometimes considered for exclusion (Johnson and Bickel 2008) may, in this case, be a direct effect of EFT. Details of these analyses may be found in Table S1 in Online Resource 1. Briefly, Johnson and Bickel (2008) outlined two criteria to identify nonsystematic discounting data. Criterion 1 assumes consistent local effects of contiguous delays, with no or few increments in delay containing an increase in discounted value. We made no hypotheses regarding effects of EFT on criterion 1 and observed no group difference in the frequency of data that failed to meet this criterion. In contrast, criterion 2 assumes a decreasing trend in discounted value across delays, wherein the magnitude of the reduction in value from the first to last delay should equal at least 10 % of the undiscounted large reward value. We hypothesized that EFT would increase the frequency with which data violated criterion 2, as effective EFT in some cases would likely produce little to no discounting across the time spans investigated (1 day to 1 year). Indeed, this is what we observed, as significantly more EFT than ERT participants showed little to no evidence of delay discounting (i.e., flat discounting functions; see Table S1), thus indicating that such data are a direct effect of EFT and may be assumed to reflect the construct of interest, rather than extraneous variability that may otherwise produce non-systematic data.
Delay discounting was compared between groups using 2 (Group) × 5 (Delay) repeated measures ANOVA. Post hoc comparisons at each delay were conducted using the sequential Bonferroni correction. Area under each participant’s discounting curve (AUC; Myerson et al. 2001) served as a summary measure of discounting, wherein AUC is inversely proportional to degree of discounting. Values of AUC were compared between groups using t tests.
Cigarette self-administration.
One EFT participant misunderstood task instructions, spontaneously reporting at the end of the session that he believed the purpose of the task was to smoke as much as possible. This participant’s self-administration puff data (more than two standard deviations above the group mean) was therefore excluded from subsequent analyses. The dependent measure of cigarette self-administration was the number of puffs earned during the task. These values were compared between groups using a t test. We also used Spearman rho correlations to examine the relation between number of self-administered puffs and AUC in the delay-discounting task.
Results
Demographic characteristics and addiction severity
Table 1 presents demographic characteristics, cigarettes per day, and FTCD scores for the EFT and ERT groups. We observed no significant between-group differences in any of these measures (in all cases, p > .250).
Table 1.
Sample size and demographic characteristics of the EFT and ERT groups, including results of Fisher’s exact or t tests of between-group differences for each variable
| Group |
p-value | ||
|---|---|---|---|
| EFT | ERT | ||
| Sex | |||
| Male (n) | 13 | 11 | >0.250 |
| Female (n) | 7 | 11 | |
| Race | |||
| Caucasian (n) | 10 | 13 | >0.250 |
| Non-Caucasian (n) | 10 | 8 | |
| Age (y; +SD) | 38.65 (11.96) | 39.86 (11.01) | >0.250 |
| Education (y; ±SD) | 12.75 (1.80) | 12.41 (1.29) | >0.250 |
| Monthly Income (US$; ±SD) | 741.05 (612.99) | 929.90 (1067.00) | >0.250 |
| Cigarettes/day (±SD) | 18.90 (7.89) | 19.55 (8.02) | >0.250 |
| FTCD score (±SD) | 5.70 (1.90) | 5.33 (1.98) | >0.250 |
Y years, C/d cigarettes/day at intake, FTCD Fagerström Test for Cigarette Dependence
Delay discounting
The left panels of Fig. 1 depict discounted value across increasing delays in the delay-discounting task, as well as corresponding AUC values. Results of ANOVA indicated significant main effects of group (F(1,40) = 5.89, p = .020) and delay (F(4,160) = 31.79, p < .0001) on discounted value of US$1000; the Group × Delay interaction trended toward significance (F(4,160) = 2.07, p = .090). Post hoc tests revealed that money retained more value (i.e., subjects discounted less) in the EFT than ERT groups at delays of 3 months (p = .012) and 1 year (p = .001). Similarly, we observed significantly higher AUC in the EFT than ERT groups (t(40) = 2.20, p = .034; see Fig. 1), with an AUC effect size of d = 0.651 (a medium effect; Cohen 1988).
Figure 1.
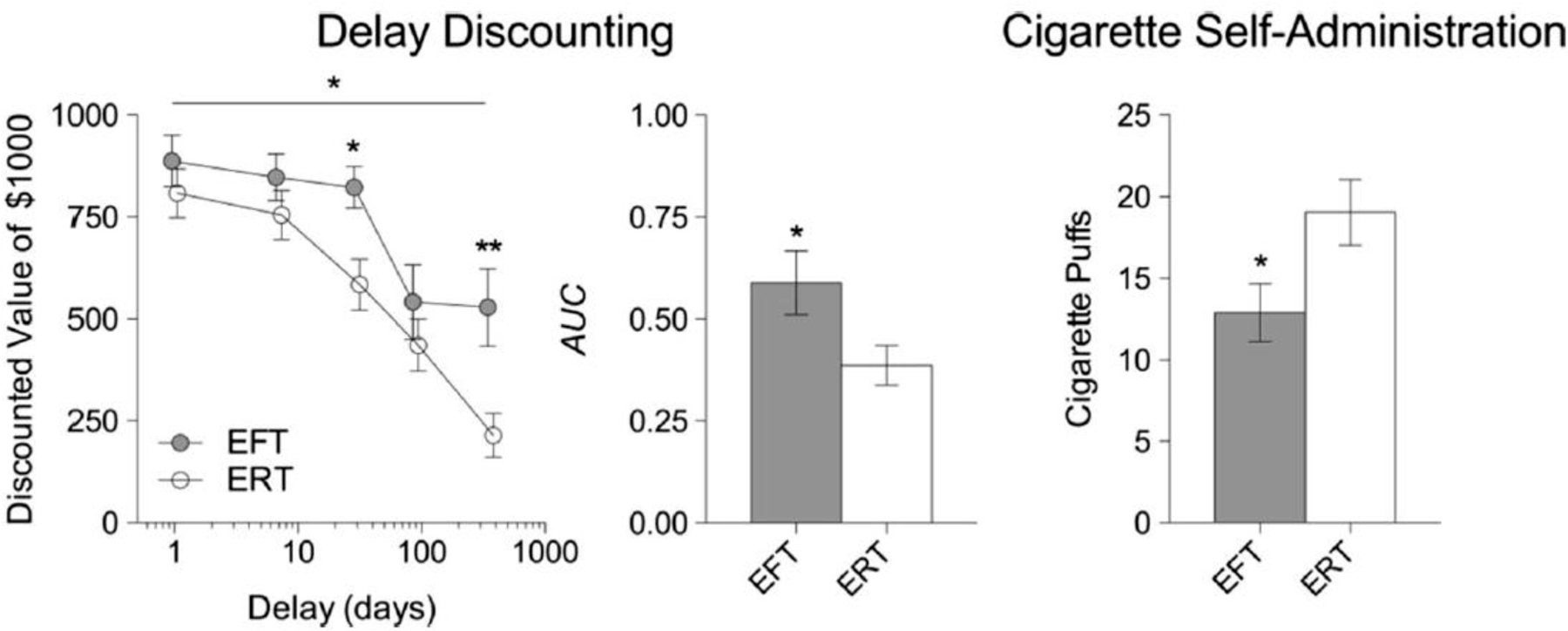
Discounted value of US$1000 across increasing delays and corresponding values of AUC in EFT (n = 20) and ERT (n = 22) participants (left panels). Also pictured is the number of cigarette puffs earned in the cigarette self-administration task (right panel) in EFT (n = 19) and ERT (n = 22) participants. Error bars represent standard error of the mean. The x axis in the left panel appears in log scale to facilitate inspection of data points at short delays. Data points have also been displaced slightly on this axis, for clarity *p < .05; **p < .01
Comparable effects of EFT on discounted value and AUC were observed in a supplementary analysis (see Fig. S1 in Online Resource 1) in which we excluded the small amount of data (n = 1 participant from each group) that violated Johnson and Bickel’s (2008) criterion 1 (consistency across contiguous delays).
Cigarette self-administration
The right panel of Fig. 1 depicts the number of cigarette puffs earned during the 60-min self-administration task in EFT and ERT groups. The EFT group smoked significantly less than the ERT group (t(39) = 2.27, p = .029). Further analysis revealed an effect size of d = −0.58 (a medium effect; Cohen 1988).
The number of puffs during the self-administration task was negatively correlated with AUC in the delay discounting task in both the EFT (rho = −.28) and ERT (rho = −.33) groups, although these values were not statistically significant (ps = .248 and .135, respectively). When data were collapsed across group, however, the correlation remained negative and was statistically significant (rho = −.37, p = .018).
Discussion
EFT in the present study reduced delay discounting in cigarette smokers, which systematically reproduces our own and others’ prior findings in both obese and healthy populations (e.g., Daniel et al. 2013a, 2013b, 2015; Kaplan et al. 2016; Peters and Büchel 2010). This effect was observed in both primary and supplementary analyses (i .e., when inconsistencies in discounting data were either retained or excluded; see Figs. 1 and S1, respectively). Next, comparable to our prior findings in which EFT reduced calorie intake in obese participants (Daniel et al. 2013a, 2015), EFT in the present study reduced cigarette self-administration—a behavior that provides small, short-term benefits at the cost of larger, delayed health costs.
Potential mechanisms
Rapid devaluation of delayed rewards, overly restricted time perspective, and failure to consider future consequences are defining features of addiction (Alvos et al. 1993; Bickel et al. 2014; Fieulaine and Martinez 2010; Keough et al. 1999; MacKillop et al. 2007; Manganiello 1978; Petry et al. 1998; Roos and Albers 1965), obesity (Amlung et al. 2016, Weller et al. 2008), and a broad range of maladaptive health behaviors (Bickel and Stein 2016). Those suffering from these disorders appear “stuck in time,” persistently engaging in immediately reinforced behavior (e.g., smoking, overeating) without regard for delayed, negative health outcomes. Thus, any variable that remediates this bias toward restricted time perspective is likely to improve health-related decision-making. Consistent with this hypothesis, the EFT-related shift-in-time perspective and resulting improvement in valuation of future consequences in present and prior studies appears to increase the likelihood of acting in one’s long-term best interest, whether that involves decisions regarding cigarette smoking (as in the present study) or calorie intake (e.g., Daniel et al. 2013a, 2015). These effects are also consistent with other findings, in which naturally occurring variation in time perspective modulates health behaviors such as exercise and fruit and vegetable consumption (e.g., Gellert et al. 2012).
At the neural level, EFT enhances activity in several brain regions implicated in executive function, such as the dorsolateral prefrontal cortex and anterior cingulate cortex, as well as functional connectivity between executive areas and hippocampus and amygdala (Okuda et al. 2003; Peters and Büchel 2010). However, whether these neural changes are cause or consequence of the shift-in-time perspective and future reward valuation is, as of yet, unclear. Specifically, prior data show that poor quality EFT is associated with poor executive control (de Vito et al. 2012). Likewise, the ability of EFT to modulate delay discounting depends partially on healthy working memory capacity (Lin and Epstein 2014). Thus, intact executive function may serve as a prerequisite for EFT’s effect on delay discounting and cigarette smoking—an important point that awaits further investigation.
Use of the ERT condition in the present and prior studies is an appropriate control for EFT. Effects of EFT on delay discounting cannot be attributed to the absolute difference in temporal distance between EFT and ERT cues (up to 1 year in EFT, but only 24 h in ERT, in the present study), as recent data indicate that episodic thinking of the distant past does not affect future discounting (Daniel et al. 2016). Moreover, both EFT and ERT conditions activate autobiographical memory (Conway and Pleydell-Pearce 2000; Schacter et al. 2007), thus isolating the effects of prospection in EFT on measures of delay discounting and cigarette smoking.
EFT and clinical treatment
In the present study, EFT significantly reduced cigarette smoking and was thus useful as an experimental tool to investigate relations between delay discounting and tobacco use. However, EFT as implemented in the present study is unlikely to produce sustained changes in delay discounting and smoking. Instead, changes observed in these measures following EFT are likely to be context dependent. A critical question for future research is whether some iteration of EFT can produce clinically relevant and sustained reductions in tobacco and other drug use in the natural environment. If so, then sustained exposure to EFT in situations where impulse control is needed may be required. Recent data from our group show that EFT may be employed outside the laboratory in such a manner, via web-based ecological momentary intervention, to aid in dietary and weight control in overweight and obese participants (O’Neill et al. 2016; Sze et al. 2015). Adapting this method for cigarette smoking or other drug use may yield similar success. If drug dependence is the partial product of being “stuck in time,” as the present and prior data suggest, then its treatment is likely to see little progress until clinical strategies explicitly attempt to address this deficit in those whose behavior is otherwise restricted to temporally proximal sources of reinforcement.
The ability to exploit knowledge of delay discounting as a potential underlying cause of drug dependence, however, is not limited to EFT. Other experimental variables known to reduce discounting, such as mindfulness and acceptance based treatments (Hendrickson and Rasmussen 2013; Morrison et al. 2014), explicit training to increase tolerance to delayed reinforcement (e.g., Stein et al. 2013, 2015; Whiting and Dixon 2015), or working memory training (Bickel et al. 2011) may also be useful in reducing subsequent drug use via extension of the temporal horizon. But, as they say: only time will tell.
Limitations
Two limitations of the present study deserve note. First, we did not independently verify that participants engaged in episodic future thinking. However, the methods used in the present and prior studies (e.g., Daniel et al. 2013a, b) robustly affect discounting and related behavior, suggesting strong engagement in episodic thought. Moreover, prior research in this line explicitly measured such engagement and found these methods effective in this regard (e.g., Daniel et al. 2013b). Finally, explanations for observed effects other than episodic thought are unlikely. For example, prior research indicates that framing delays in a discounting task as specific calendar dates also reduces delay discounting (LeBoeuf 2006; Read et al. 2005); however, a control condition in prior research specifically implicates episodic imagery in EFT-related reductions in discounting, rather than temporal specificity (Peters and Büchel 2010).
A second limitation of the present study is that our study design and sample size constrains our ability to link EFT-related reductions in discounting with reductions in smoking. One potential mechanism, reviewed above, is that observed reductions in discounting mediated the relation between EFT and cigarette smoking. However, we cannot rule out with certainty the possibility that observed changes in discounting were independent of observed changes in smoking. If delay discounting was directly responsible for reduction in cigarette smoking (e.g., by increasing valuation of the delayed benefits of not smoking), then one would expect AUC and cigarette puffs to be negatively correlated. Indeed, such a significant correlation was observed in the combined analysis across groups, although limited sample sizes may have prevented individual group analyses from reaching significance. Future studies should utilize larger sample sizes combined with mediation analysis (Ten Have and Joffe 2012) to examine potential mechanisms more directly.
Conclusions and future directions
We conclude that EFT simultaneously reduces delay discounting and cigarette self-administration in cigarette smokers. Future work should be designed to examine the extent to which these effects generalize to other populations and drug commodities (e.g., alcohol self-administration in alcohol-dependent participants), as well as whether these methods can be adapted for clinical treatment of tobacco and other drug use.
Supplementary Material
Acknowledgments
All authors thank Corey Judd, Mariah Kelly, Nicole Seymour, and Jessica Washington for assistance in data collection. This research was supported financially by NIH grant 5R01DA034755 and operational funds, awarded to the last author (W. K. Bickel).
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest.
References
- Alvos L, Gregson RA, Ross MW (1993) Future time perspective in current and previous injecting drug users. Drug Alcohol Depend 31: 193–197. doi: 10.1016/0376-8716(93)90072-X [DOI] [PubMed] [Google Scholar]
- Amlung M, Petker T, Jackson J, Balodis I, MacKillop J (2016) Steep discounting of delayed monetary and food rewards in obesity: a meta-analysis. Psychol Med 46:2423–2434 [DOI] [PubMed] [Google Scholar]
- Atance CM, O’Neill DK (2001) Episodic future thinking. Trend Cogn Sci 5:533–539. doi: 10.1016/s1364-6613(00)01804-0 [DOI] [PubMed] [Google Scholar]
- Audrain-McGovern J, Rodriguez D, Epstein LH, Cuevas J, Rodgers K, Wileyto EP (2009) Does delay discounting play an etiological role in smoking or is it a consequence of smoking? Drug Alcohol Depend 103:99–106. doi: 10.1016/j.drugalcdep.2008.12.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel WK, Stein JS (2016) Self-control and its failure: Intertemporal dimensions of health behavior. Big Data (in press) [Google Scholar]
- Bickel WK, Yi R, Landes RD, Hill PF, Baxter C (2011) Remember the future: working memory training decreases delay discounting among stimulant addicts. Biol Psychiat 69:260–265. doi: 10.1016/j.biopsych.2010.08.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel WK, Koffarnus MN, Moody L, Wilson AG (2014) The behavioral- and neuro-economic process of temporal discounting: a candidate behavioral marker of addiction. Neuropharmacology 76: 518–527. doi: 10.1016/j.neuropharm.2013.06.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown RA, Burgess ES, Sales SD, Whiteley JA, Evans DM, Miller IW (1998) Reliability and validity of a smoking timeline follow-back interview. Psychol Addict Behav 12:101–112. doi: 10.1037/0893-164x.12.2.101 [DOI] [Google Scholar]
- Cohen J (1988) Statistical power analysis for the behavioral sciences Lawrence Erlbaum Associates, Mahwah. doi: 10.4324/9780203771587 [DOI] [Google Scholar]
- Conway MA, Pleydell-Pearce CW (2000) The construction of autobiographical memories in the self-memory system. Psychol Rev 107(2):261–288. doi: 10.1037/0033-295X.107.2.261 [DOI] [PubMed] [Google Scholar]
- Daniel TO, Stanton CM, Epstein LH (2013a) The future is now: reducing impulsivity and energy intake using episodic future thinking. Psychol Sci 24:2339–2342. doi: 10.1016/j.appet.2013.07.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daniel TO, Stanton CM, Epstein LH (2013b) The future is now: comparing the effect of episodic future thinking on impulsivity in lean and obese individuals. Appetite 71:120–125. doi: 10.1177/0956797613488780 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daniel TO, Said M, Stanton CM, Epstein LH (2015) Episodic future thinking reduces delay discounting and energy intake in children. Eat Behav 18:20–24. doi: 10.1016/j.eatbeh.2015.03.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daniel TO, Sawyer A, Dong Y, Bickel WK, Epstein LH (2016) Remembering versus imagining: when does episodic retrospection and episodic prospection aid decision making? J Appl Res Mem Cogn doi: 10.1016/j.jarmac.2016.06.005 [DOI] [Google Scholar]
- de Vito S, Gamboz N, Brandimonte MA, Barone P, Amboni M, Della Sala S (2012) Future thinking in Parkinson’s disease: an executive function? Neuropsychologia 50:1494–1501. doi: 10.1016/j.neuropsychologia.2012.03.001 [DOI] [PubMed] [Google Scholar]
- Du W, Green L, Myerson J (2002) Cross-cultural comparisons of discounting delayed and probabilistic rewards. Psychol Rec 52: 479. doi: 10.1037/0033-2909.130.5.769 [DOI] [Google Scholar]
- Fagerström K (2012) Determinants of tobacco use and renaming the FTND to the Fagerström test for cigarette dependence. Nicotine Tob Res 14:75–78. doi: 10.1093/ntr/ntr137 [DOI] [PubMed] [Google Scholar]
- Fieulaine N,Martinez F (2010) Time under control: time perspective and desire for control in substance use. Addict Behav 35:799–802. doi: 10.1016/j.addbeh.2010.03.022 [DOI] [PubMed] [Google Scholar]
- Gellert P, Ziegelmann JP, Lippke S, Schwarzer R (2012) Future time perspective and health behaviors: temporal framing of self regulatory processes in physical exercise and dietary behaviors. Ann Behav Med 43:208–218. doi: 10.1007/s12160-011-9312-y [DOI] [PubMed] [Google Scholar]
- Hendrickson KL, Rasmussen EB (2013) Effects of mindful eating training on delay and probability discounting for food and money in obese and healthy-weight individuals. Behav Res Ther 51:399–409. doi: 10.1016/j.brat.2013.04.002 [DOI] [PubMed] [Google Scholar]
- Johnson MW, Bickel WK (2008) An algorithm for identifying nonsystematic delay-discounting data. Exp Clin Psychopharm 16:264–274. doi: 10.1037/1064-1297.16.3.264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson MW, Bickel WK, Kirshenbaum AP (2004) Substitutes for tobacco smoking: a behavioral economic analysis of nicotine gum, denicotinized cigarettes, and nicotine-containing cigarettes. Drug Alcohol Depend 74:253–264. doi: 10.1016/j.drugalcdep.2003.12.012 [DOI] [PubMed] [Google Scholar]
- Kaplan BA, Reed DD, Jarmolowicz DP (2016) Effects of episodic future thinking on discounting: personalized age-progressed pictures improve risky long-term health decisions. J Appl Behav Anal 49:148–169. doi: 10.1002/jaba.277 [DOI] [PubMed] [Google Scholar]
- Keough KA, Zimbardo PG, Boyd JN (1999) Who’s smoking, drinking, and using drugs? Time perspective as a predictor of substance use. Basic Appl Soc Psych 21:149–164. doi: 10.1207/15324839951036498 [DOI] [Google Scholar]
- LeBoeuf RA (2006) Discount rates for time versus dates: the sensitivity of discounting to time-interval description. J Mark Res 43:59–72. doi: 10.1509/jmkr.43.1.59 [DOI] [Google Scholar]
- Lin H, Epstein LH (2014) Living in the moment: effects of time perspective and emotional valence of episodic thinking on delay discounting. Behav Neurosci 128:12–19. doi: 10.1037/a0035705 [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKillop J, Mattson RE, Anderson MacKillop EJ, Castelda BA, Donovick PJ (2007) Multidimensional assessment of impulsivity in undergraduate hazardous drinkers and controls. J Stud Alcohol Drugs 68:785–788. doi: 10.15288/jsad.2007.68.785 [DOI] [PubMed] [Google Scholar]
- Manganiello JA (1978) Opiate addiction: a study identifying three systematically related psychological correlates. Int J Addict 13:839–847. doi: 10.3109/10826087809039307 [DOI] [PubMed] [Google Scholar]
- Morrison KL, Madden GJ, Odum AL, Friedel JE, Twohig MP (2014) Altering impulsive decision making with an acceptance-based procedure. Behav Ther 45(5):630–639. doi: 10.1016/j.beth.2014.01.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myerson J, Green L, Warusawitharana M (2001) Area under the curve as a measure of discounting. J Exp Anal Behav 76:235–243. doi: 10.1901/jeab.2001.76-235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odum AL, Baumann AA (2007) Cigarette smokers show steeper discounting of both food and cigarettes than money. Drug Alcohol Depend 91:293–296. doi: 10.1016/j.drugalcdep.2007.07.004 [DOI] [PubMed] [Google Scholar]
- Odum AL, Madden GJ, Bickel WK (2002) Discounting of delayed health gains and losses by current, never-and ex-smokers of cigarettes. Nicotine Tob Res 4:295–303. doi: 10.1080/14622200210141257 [DOI] [PubMed] [Google Scholar]
- Ohmura Y, Takahashi T, Kitamura N (2005) Discounting delayed and probabilistic monetary gains and losses by smokers of cigarettes. Psychopharmacology 182:508–515. doi: 10.1007/s00213-005-0110-8 [DOI] [PubMed] [Google Scholar]
- Okuda J, Fujii T, Ohtake H, Tsukiura T, Tanji K, Suzuki K, Kawashima R, Fukuda H, Itoh M, Yamadori A (2003) Thinking of the future and past: the roles of the frontal pole and the medial temporal lobes. NeuroImage 19:1369–1380. doi: 10.1016/s1053-8119(03)00179-4 [DOI] [PubMed] [Google Scholar]
- O’Neill J, Daniel TO, Epstein LH(2016) Episodic future thinking reduces eating in a food court. Eat Behav 20:9–13. doi: 10.1016/j.eatbeh.2015.10.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters J, Büchel C (2010) Episodic future thinking reduces reward delay discounting through an enhancement of prefrontal-mediotemporal interactions. Neuron 66:138–148. doi: 10.1016/j.neuron.2010.03.026 [DOI] [PubMed] [Google Scholar]
- Petry NM, Bickel WK, Arnett M (1998) Shortened time horizons and insensitivity to future consequences in heroin addicts. Addiction 93: 729–738. doi: 10.1046/j.1360-0443.1998.9357298.x [DOI] [PubMed] [Google Scholar]
- Read D, Frederick S, Orsel B, Rahman J (2005) Four score and seven years from now: the date/delay effect in temporal discounting. Manag Sci 51(9):1326–1335 [Google Scholar]
- Roos P, Albers R (1965) Performance of alcoholics and normals on a measure of temporal orientation. J Clin Psychol 21:34–36. doi: [DOI] [PubMed] [Google Scholar]
- Schacter DL, Addis DR, Buckner RL (2007) Remembering the past to imagine the future: the prospective brain. Nat Rev Neurosci 8(9): 657–661 [DOI] [PubMed] [Google Scholar]
- Schmitz C. Limesurvey: an open source survey tool limesurvey project Hamburg, Germany. URL http://www.limesurvey.org. 2012. [Google Scholar]
- Snider SE, LaConte SM, Bickel WK (2016) Episodic future thinking: expansion of the temporal window in individuals with alcohol dependence. Alcohol Clin Exp Res 40:1558–1566. doi: 10.1111/acer.13112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stein JS, Madden GJ (2013) Delay discounting and drug abuse: empirical, conceptual, and methodological considerations. The Wiley-Blackwell handbook of addiction. Psychopharmacology 7:165–208. doi: 10.1002/9781118384404.ch7 [DOI] [Google Scholar]
- Stein JS, Johnson PS, Renda CR, Smits RR, Liston KJ, Shahan TA, Madden GJ (2013) Early and prolonged exposure to reward delay: effects on impulsive choice and alcohol self-administration in male rats. Exp Clin Psychopharm 21:172–180. doi: 10.1037/a0031245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stein JS, Renda CR, Hinnenkamp JE, Madden GJ (2015) Impulsive choice, alcohol consumption, and pre-exposure to delayed rewards: II. Potential mechanisms. J Exp Anal Behav 103:33–49. doi: 10.1002/jeab.116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sweitzer MM, Donny EC,Dierker LC, Flory JD,Manuck SB (2008) Delay discounting and smoking: association with the Fagerström test for nicotine dependence but not cigarettes smoked per day. Nicotine Tob Res 10:1571–1575. doi: 10.1080/14622200802323274 [DOI] [PubMed] [Google Scholar]
- Sze YY, Daniel TO, Kilanowski CK, Collins RL, Epstein LH (2015) Web-based and mobile delivery of an episodic future thinking intervention for overweight and obese families: a feasibility study. JMIR mHealth and uHealth 3(4):e97. doi: 10.2196/mhealth.4603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ten Have TR, Joffe MM (2012) A review of causal estimation of effects in mediation analyses. Stat Methods Med Res 21(1):77–107 [DOI] [PubMed] [Google Scholar]
- Vonnegut K (1969) Slaughterhouse-five, or, the children’s crusade: a duty-dance with death Laurel, New York [Google Scholar]
- Weller RE, Cook EW, Avsar KB, Cox JE (2008) Obese women show greater delay discounting than healthy-weight women. Appetite 51(3):563–569 [DOI] [PubMed] [Google Scholar]
- Whiting SW, Dixon MR (2015) Delayed reinforcement and self-control: increasing tolerance for delay with children and adults with autism. In autism service delivery Springer, New York, pp. 407–435. doi: 10.1007/978-1-4939-2656-5_15 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.