

Abstract
Background
In order to achieve better hemostasis of puncture holes in the femoral artery (FA) after an endovascular procedure, this study evaluated the effect and safety of manual compression (MC) with QuikClot Combat Gauze (QIC) and with mechanical compression (using a C-clamp) of the common access site, the FA, in patients with peripheral arterial occlusive disease (PAOD) combined with anterior femoral artery calcification (AFAC).
Methods
We prospectively reviewed 100 patients receiving either MC with QIC or mechanical compression (control group) after endovascular intervention for PAOD plus AFAC from February 2014 to September 2018 in a single unit, which was assessed using computerized tomography angiography (CTA).
Results
The mean time to completion of hemostasis was 30±0 minutes in the control group and 18±2.20 minutes in the QIC group (P<0.001). The time to ambulation of the QIC and control groups was 4.38±0.46 and 4.86±0.30 hours (P<0.001), respectively. Eight (16%) patients in the control group had hematoma, as compared with one patient (2%) in the QIC group (P=0.031), while sixteen (32%) patients in the control group had ecchymosis, as compared with four (8%) in the QIC group (P=0.005). Use of QIC and coronary artery disease (CAD) were identified as independent factors correlated with an increased risk of minor complications.
Conclusions
QIC facilitated effective and safe hemostasis in patients with PAOD and AFAC.
Keywords: Ankle-brachial index (ABI), anterior femoral artery calcification (AFAC), coronary artery disease (CAD), computerized tomography angiography (CTA), peripheral arterial occlusive disease (PAOD), QuikClot Combat Gauze (QIC)
Introduction
The most common vascular access location for peripheral or cardiac artery interventions is the femoral artery (FA) (1). FA complications are frequently encountered, in particular in patients with underlying hemostasis problems, and with use of larger-sized introducer sheaths, intraoperative use of heparin, and preoperative and postoperative potent antithrombotic and antiplatelet therapy (2). Thus, these conditions can aggravate bleeding, which increases the duration of surgery, global blood loss, and risk of artery-related complications (3).
The conventional primary treatment for puncture bleeding is direct manual compression (MC) with gauze pads and pressure, followed by compressors or tourniquets depending on the puncture site. However, the head, neck, groin, popliteal fossa, and axilla are examples of junctional zones that are unsuitable wound locations for the application of tourniquets (4). Thus, maintaining sufficient compression to prevent severe bleeding is challenging in these anatomical areas (5). Depending on the particular condition or anatomy, heparin reversal, vascular closure devices (VCDs), and vascular repair are auxiliary or alternative methods.
According to previous studies (6), VCDs have been recognized as an efficacious alternative to conventional mechanical compression to achieve hemostasis of puncture holes in the FA after an endovascular procedure. However, some risks related to the use of VCDs exist, including a small FA caliber and calcification on the anterior wall, on more than half of the posterior wall, or circumferentially at the target area of the common femoral artery (CFA) (6). Owing to increasing complexity in patient conditions, anatomic variations, and use of antithrombotic agents during interventions, these devices cannot always be used for hemostasis; thus, other, alternative methods should be considered for prompt and effective hemostasis.
QuikClot Combat Gauze (QIC) has been designated by the U.S. Armed Forces the primary hemostatic management for the treatment of severe hemorrhage (7,8). An aluminum silicate (kaolin) is the main component of QIC, which is a very potent coagulation initiator that acts as a surface activator (7,8). Its mechanism of action involves rapid absorption of the water content of blood, which results in concentration of the protein and cellular elements, facilitating clot formation (7,8). Numerous studies have reported that QIC should be applied with pressure directly to the bleeding site (7,8). Guidelines suggest the application of direct pressure using this material to the site of bleeding or deeper inside the wound, and even for local management and control of surface bleeding from vascular access sites, percutaneous catheters, or tubes utilizing introducer sheaths, for the treatment of patients with drug-induced anticoagulation (7,8).
To date, scant information is available with regards to the efficacy and safety of using hemostatic combat gauze on patients undergoing endovascular interventions for peripheral arterial disease.
This prospective study investigated the effectiveness and safety of MC using QIC applied directly to the sheath hole of a punctured CFA in patients with peripheral arterial occlusive disease (PAOD) combined with anterior femoral artery calcification (AFAC). We present the following article in accordance with the TREND reporting checklist (available at https://qims.amegroups.com/article/view/10.21037/qims-21-1164/rc).
Methods
Patient data
The study is a prospective nonrandomized observational study. From February 2014 to September 2018, 100 subjects with chronic PAOD combined with severe calcification of the femoral arteries, as confirmed via the ankle-brachial index (ABI), Doppler ultrasonography, and computerized tomography angiography (CTA), were enrolled in this study. The 100 participants underwent successful endovascular interventions with the use of various sheaths, ranging from 6 to 8 F. Because QIC is a self-pay medical material in Taiwan, the patients were informed and decided to use QIC or not for compression the puncture site. In this study, 50 participants decided MC with QIC, and the other 50 participants selected mechanical compression with C-clamp. Besides, we followed up all of the participants during hospitalization, and also arranged a return visit in outpatient department (OPD) and closely telephone contact. Therefore, there was no loss to follow-up of the participants during the investigation.
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Institutional Review Board of Taipei Veterans General Hospital (the registration number from clinicaltrials.gov. is TVGH IRB No. 2013-08-020B), and written informed consent was obtained from all patients prior to the endovascular interventions.
Definition of calcification of femoral arteries
CFA calcification was measured through Doppler ultrasonography and CTA prior to the operation. Calcification involving the anterior femoral artery (AFA) wall (270–90° from inguinal ligament to FA bifurcation) was considered calcification of the anterior FA wall (6). FAs with greater than 50% AFA calcification were defined as AFAC. No and less than 50% AFA calcification and calcification of the posterior FA were defined as non-AFA calcification (NAFAC).
The inclusive criteria were that the patient with chronic peripheral artery occlusive disease (PAOD) combined with greater than 50% AFA calcification, and underwent successful endovascular interventions. The exclusive criteria were that the patient with PAOD but less than 50% AFA calcification. These patients were recruited from our cardiovascular OPD or referred from Internal medicine department, and they were indicated for endovascular interventions.
Technical specifications
All patients were punctured at the inguinal area through ultrasonography in our department. This allowed the puncture of the CFA superior to the bifurcation to avoid the area of heavy calcification and avoid compromising the ipsilateral inflow. Assuming that the groin was already accessed, we used a puncture needle to gain access, inserted a short sheath, crossed over the bifurcation using a pigtail catheter, and replaced the short sheath with a 6–8-F long sheath. Patients were then administered 50–80 U/kg of heparin to maintain an activated clotting time (ACT) between 200 and 300 seconds. If the surgical duration was greater than two hours, an extra dose of heparin was injected on the basis of the ACT.
Percutaneous interventions were performed in all patients. Postoperatively, the arterial sheath was removed in patients with an ACT below 160 seconds, and mechanical compression (using a C-clamp) or firm MC in combination with QIC was subsequently applied above the entry site while removing the sheath. The method of compression using QIC was modified based on the trial conducted by Trabattoni et al. (8), and mechanical compression was applied using a C-clamp for 30 minutes.
The puncture site was then characterized through Doppler ultrasonography 1 hour after complete hemostasis. After complete hemostasis had been achieved, the patients received a compression sandbag for 2 hours. Ambulation was subsequently allowed 4–5 hours after complete hemostasis. A complete blood count was obtained at baseline and at 24 h in all cases.
The cardiovascular attending physicians delivered the whole endovascular intervention, and they performed mechanical compression (using a C-clamp) or firm MC in combination with QIC, and routinely recorded the outcomes. Besides, the cardiovascular attending physicians regularly followed using the Doppler ultrasonography. On the other hand, the patients had written informs and knew the study in progress.
After the aforementioned procedures, subjects attended regular clinical follow-ups. Doppler ultrasonography was performed on the operative day, first postoperative day, and discharge day, as well as at 1, 3, 6 and 12 months. Patients undergoing stent implantation were administered dual antiplatelets, and single antiplatelets were prescribed for patients undergoing a simple angioplasty. Additionally, prostaglandin E 1 (PGE 1) 40 mcg was postoperatively administered twice per day (once per twelve hours) for all participants.
Study endpoints
The primary endpoints included complete hemostasis and safety outcome. Safety outcome was defined in terms of major or minor vascular complications in the patients. Complete hemostasis (time to hemostasis) was defined as the time from the beginning of the application of direct pressure using QIC or mechanical compression to the time at which no further compression was needed to control bleeding at the access site. The puncture site was assessed through Doppler ultrasonography 1 hour after complete hemostasis to ascertain whether a vascular entity and hemostasis had developed. The assessment was performed by the same cardiovascular attending physician and technician.
A minor complication was considered a hematoma of less than 5 cm in diameter or ecchymosis of less than 10 cm in diameter. Major vascular complications were a hematoma exceeding 5 cm in diameter, retroperitoneal bleeding in which the perioperative hemoglobin level fell by more than 3 g/dL, arteriovenous fistula, pseudoaneurysm, shock or vessel occlusion, and loss of pulse (9,10). Hematoma was evaluated by Doppler ultrasonography, and ecchymosis was evaluated by inspection.
The secondary endpoints comprised time to ambulation, defined from the beginning of direct pressure using QIC or mechanical compression to ambulation, and successful hemostasis was defined as hemostasis without late complications detected through Doppler ultrasonography at 6 months.
Statistical analysis
The Kolmogorov-Smirnov test was employed to analyze the normality of numerical variable distributions. According to the distributed data, the median and interquartile range (IQR) or mean ± standard deviation are used to present continuous data, and percentages and numbers are used to express categorical data. Regarding numerical variables, the Mann-Whitney U test and independent-samples t-test were employed to determine intergroup differences. Frequencies and categorical variables were compared using the χ2 test.
In addition, predisposing factors of complications were confirmed using univariate and multivariate logistic regression methods. A 2-tailed P<0.05 was deemed significant. All analyses were performed using SPSS v.22.
Results
From February 2014 to September 2018, 100 subjects were enrolled in this study, and underwent follow-up for 12 months. A flow diagram of this study is shown in Figure 1.
Figure 1.
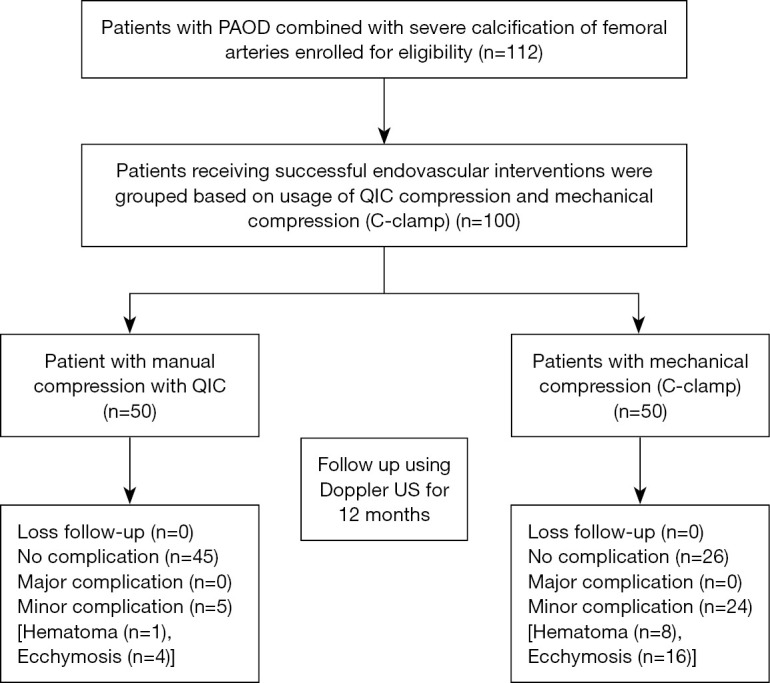
Flow diagram of this study. Major complications: massive hematoma greater than 5 cm in diameter; retroperitoneal bleeding in which the hemoglobin level decreases by more than 3 g/dL; arteriovenous fistula, pseudoaneurysm; vessel dissection; loss of pulse. Minor complications: hematoma less than 5 cm in diameter; ecchymosis less than 10 cm in diameter. PAOD, peripheral arterial occlusive disease; QIC, QuikClot Combat Gauze; US, ultrasound.
The participants included 41 women and 59 men, with a mean age of 71.30±10.20 years (47–90 years). The mean follow-up duration was 12.90±1.20 months. Of the 100 patients, 50 (50%) were assigned to the control (non-QuikClot) group and 50 (50%) were assigned to the QIC group on the basis of method of compression.
Data on baseline demographics, sheath size, extent and location of FA calcification, Fontaine classification, and body mass index (BMI) were collected and are listed in Table 1. The patients in the two groups were well-matched in terms of clinical characteristics and antithrombotic therapy, as shown in Table 1.
Table 1. Baseline demographics and characteristics of enrolled patients.
| Characteristic | Control (N=50) | QuikClot (N=50) | P value |
|---|---|---|---|
| Age, years | 71.70±9.60 | 73.30±9.30 | 0.38 |
| Gender (female) | 19 [38] | 22 [44] | 0.542 |
| BMI, kg/m2 | 24.90±4.10 | 24.30±4.30 | 0.525 |
| SBP, mmHg | 133.40±19.70 | 134.40±20.00 | 0.812 |
| Puncture site (left) | 24 [48] | 23 [46] | 0.841 |
| CAD | 34 [68] | 34 [68] | 1.000 |
| DM | 43 [86] | 42 [84] | 0.779 |
| ESRD with dialysis | 28 [56] | 28 [56] | 1.000 |
| Hypertension | 45 [90] | 42 [84] | 0.372 |
| Hyperlipidemia | 40 [80] | 35 [70] | 0.248 |
| CHF, NYHA II | 9 [18] | 11 [22] | 0.617 |
| CVA | 9 [18] | 9 [18] | 1.000 |
| AF | 7 [14] | 10 [20] | 0.424 |
| Smoking | 24 [48] | 21 [42] | 0.546 |
| Antithrombotics aspirin | 38 [78] | 35 [70] | 0.499 |
| Aspirin + clopidogrel | 3 [6] | 5 [10] | 0.715 |
| Warfarin | 5 [10] | 7 [14] | 0.760 |
| None | 4 [8] | 4 [8] | 1.000 |
| Fontaine classification | |||
| Stage II plus III | 21 [42] | 25 [50] | 0.422 |
| Stage IV | 29 [58] | 25 [50] | |
| Sheath size (Fr) | 7 [6–7] | 7 [6–7] | 0.6 |
| Heparin dose, units | 5,000 [4,000–5,000] | 5,000 [4,000–5,000] | 0.779 |
| ACT, seconds | 260 [255–278.8] | 260 [254.8–276.3] | 0.732 |
| Prothrombin (seconds) | 22.50±5.00 | 21.60±3.10 | 0.302 |
| Baseline hemoglobin, g/dL | 11.80±2.20 | 11.80±2.30 | 0.979 |
| Baseline platelet, /µL | 2.13×105 [1.75–2.56×105] | 2.15×105 [1.51–2.68×105] | 0.694 |
Continuous variables are presented as mean ± standard deviation and median [IQR]. Categorical variables are presented as number [%]. BMI, body mass index; SBP, systolic blood pressure; CAD, coronary artery disease; DM, diabetes mellitus; ESRD, end-stage renal disease; CHF, congestive heart failure; NYHA, New York Heart Association; CVA, cerebral vascular accident; AF, atrial fibrillation; ACT, activated clotting time; IQR, interquartile range.
The treatment methods and study endpoints at 12 months for all participants and subgroups are summarized in Table 2. Thirty-six (72%) patients in the control group and 35 (70%) in the QIC group underwent stent implantation. No significant difference was noted between the two groups (P=0.933). The mean baseline and postoperative ABI showed no significant differences between the two groups (P=0.334 and P=0.949).
Table 2. Treatment methods and study endpoints.
| Endpoints | Control (N=50) | QuikClot (N=50) | P value |
|---|---|---|---|
| Stent implantation | 36 [72] | 35 [70] | 0.933 |
| Baseline ABI | 0.58±0.19 | 0.55±0.16 | 0.334 |
| Post ABI | 0.93±0.19 | 0.92±0.19 | 0.949 |
| Baseline hemoglobin, g/dL | 11.80±2.20 | 11.80±2.30 | 0.979 |
| Postoperative hemoglobin, g/dL | 11.00±2.20 | 10.80±2.20 | 0.803 |
| Perioperative hemoglobin loss, g/dL | 0.82±0.88 | 0.91±1.07 | 0.62 |
| Time to complete hemostasis, minutes | 30.00±0.00 | 18.00±2.20 | <0.001 |
| Mean time to ambulation, hours | 4.86±0.30 | 4.38±0.46 | <0.001 |
Continuous variables are presented as mean ± standard deviation. Categorical variables are presented as number (%). ABI, ankle-brachial index.
The mean baseline (preoperative) hemoglobin levels of the control and QIC groups were 11.80±2.20 and 11.80±2.30 g/dL, respectively (P=0.979), and the mean postoperative hemoglobin (HB) levels of the control and QIC groups were 11.00±2.20 and 10.80±2.20 g/dL, respectively (P=0.803). The mean perioperative hemoglobin loss (baseline HB subtracted by postoperative HB) showed non-significant differences between the two groups (P=0.620).
The mean time to complete hemostasis of the patients in the QIC group was 18.00±2.20 minutes, as compared with 30.00±0.00 minutes for the patients in the control group (P<0.001).
The mean time to ambulation of the QIC and control groups was 4.38±0.46 and 4.86±0.30 hours, respectively (P<0.001).
Adverse effects experienced by all participants and subgroup patients are summarized in Table 3. Twenty-nine patients had minor complications, including ecchymosis (n=20) and hematoma (n=9). Nine patients had hematoma <5 cm in diameter, detected via ultrasonography. One (2%) of the patients in the QIC group had a hematoma, as compared with 8 (16%) patients in the control group (P=0.031). The QIC group and the control group included 4 (8%) and 16 (32%) patients with ecchymosis, respectively (P=0.005). Additionally, none of the 100 patients had pseudoaneurysm, massive bleeding, retroperitoneal hematoma, or arteriovenous fistula requiring surgical repair.
Table 3. Adverse effects in all patients and subgroup patients.
| Outcomes | All patients (N=100) | Controls (N=50) | QuikClot (N=50) | P |
|---|---|---|---|---|
| Adverse events | ||||
| Major complication | 0 | 0 | 0 | |
| Massive hematoma | 0 | 0 | 0 | |
| Retroperitoneal bleeding | 0 | 0 | 0 | |
| Pseudoaneurysm | 0 | 0 | 0 | |
| Arteriovenous fistula | 0 | 0 | 0 | |
| Minor complication | 29 [29] | 24 [48] | 5 [10] | <0.001 |
| Hematoma | ||||
| ≤5 cm in diameter | 9 [9] | 8 [16] | 1 [2] | 0.031 |
| >5 cm in diameter | 0 | 0 | 0 | |
| Ecchymosis | 0.005 | |||
| ≤10 cm in diameter | 20 [20] | 16 [32] | 4 [8] | |
| >10 cm | 0 | 0 | 0 | |
| Successful hemostasis | 100 [100] | 50 [100] | 50 [100] | 1.000 |
Categorical variables are presented as number [%]. Major complications: massive hematoma greater than 5 cm in diameter; retroperitoneal bleeding in which the hemoglobin level decreases by more than 3 g/dL; arteriovenous fistula, pseudoaneurysm; vessel dissection; loss of pulse. Minor complications: hematoma less than 5 cm in diameter; ecchymosis less than 10 cm in diameter.
Through logistic regression analysis, we examined the effects of all influencing factors, including those associated with minor complications (ecchymosis and hematoma), and coronary artery disease (CAD), hyperlipidemia, end-stage renal disease (ESRD), diabetes mellitus (DM), use of antithrombotic drugs, use of QIC, Fontaine classification, etc. Significant factors and potential factors for which P<0.3 were integrated and analyzed through multivariate logistic regression after adjusting for age and sex using the stepwise regression method.
CAD and use of QIC were significant factors associated with minor complications [CAD, odds ratio (OR) =6.38, 95% confidence interval (CI): 1.69–24.1, P=0.006; use of QIC, OR =0.08, 95% CI: 0.03–0.28, P<0.001) (Table 4).
Table 4. Logistic regression analysis of risk factors associated with minor complications.
| Variable | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| OR (95% CI) | P value | OR (95% CI) | P value | ||
| Age, years | 0.99 (0.94–1.03) | 0.563 | |||
| Gender (F/M) | 0.64 (0.28–1.50) | 0.308 | |||
| BMI, kg/m2 | 0.98 (0.89–1.09) | 0.760 | |||
| Smoking (yes/no) | 1.60 (0.68–3.77) | 0.282 | 1.84 (0.61–5.57) | 0.283 | |
| Hyperlipidemia (yes/no) | 2.20 (0.75–6.50) | 0.154 | 1.84 (0.46–7.33) | 0.388 | |
| CAD (yes/no) | 4.64 (1.47–14.70) | 0.009 | 6.38 (1.69–24.10) | 0.006 | |
| DM (yes/no) | 2.17 (0.58–8.20) | 0.252 | 1.39 (0.20–9.92) | 0.741 | |
| Hypertension (yes/no) | 1.62 (0.42–6.29) | 0.484 | |||
| ESRD (yes/no) | 1.63 (0.68–3.92) | 0.271 | 1.25 (0.38–4.09) | 0.713 | |
| Sheath size (7+8/5+6) | 1.25 (0.56–2.82) | 0.587 | |||
| Fontaine IV/II+III | 1.83 (0.76–4.38) | 0.177 | 1.42 (0.44–4.54) | 0.557 | |
| Intervention (PTA/stent) | 0.61 (0.23–1.62) | 0.320 | |||
| Antithrombotic drug (yes/no) | 3.97 (0.47–33.60) | 0.206 | 2.08 (0.18–24.40) | 0.561 | |
| QuikClot (yes/no) | 0.12 (0.04–0.35) | <0.001 | 0.08 (0.03–0.28) | <0.001 | |
| ACT | 1.01 (0.98–1.05) | 0.380 | |||
| Involved leg (L/R) | 0.81 (0.34–1.91) | 0.627 | |||
Multivariate analysis adjusted for age and sex. OR, odds ratio; CI, confidence interval; BMI, body mass index; CAD, coronary artery disease; DM, diabetes mellitus; ESRD, end-stage renal disease; PTA, percutaneous transluminal angioplasty; ACT, activated clotting time; L, left; R, right.
Discussion
Medical conditions of increasing complexity, anatomic variations, and antithrombotic agents used in perioperative interventions are becoming more commonly encountered, and VCDs cannot always be used for hemostasis in patients with AFAC.
This prospective, non-randomized study demonstrated that direct MC using QIC may attain satisfactory successful hemostasis and a good safety outcome for sheath-hole bleeding in patients with PAOD complicated by severe calcification of the femoral arteries.
According to a literature review, the CFA is the most common vascular access site used for peripheral or cardiac artery interventions. When situated above the most inferior border of the inferior epigastric artery or below the distal common femoral bifurcation, the risk of access-site complications is increased by arteriotomy (11,12).
Many studies have reported complications of vascular access sites, including hematoma, groin bleeding, pseudoaneurysm, arteriovenous fistula, and artery dissection. In addition, the following incidences associated with endovascular interventions have been indicated: groin hematoma, 5–23%; pseudoaneurysm, 0.5–9%; and arteriovenous fistula, 0.2–2% (1,12,13). Moreover, groin bleeding causes not only morbidity, but also worsens mortality related to endovascular interventions accompanied by cardiovascular events, contrast-induced nephropathy, and reperfusion injury (13,14). Compared with previous studies, our results showed incidences of hematoma <5 cm of 18% and ecchymosis of 20% in all the participants in this study, whereas one (2%) patient in the QIC group had a hematoma, as compared with eight (16%) patients in the control group (P=0.031). No major complications such as massive and retroperitoneal hematoma, pseudoaneurysm, or arteriovenous fistula occurred.
Although no major complications were observed in this study, the incidence of oozing was 20% (10) and 8% (4) in the control and QIC groups, respectively (P=0.148). Oozing frequently occurred in patients treated with PCI, under dual antiplatelet therapy, or with ESRD requiring heparin usage for dialysis on the first postoperative day. The occurrence of oozing easily resulted in consequent hematoma and ecchymosis, and was completely resolved with prolonged MC and compression with sandbags. Consequently, the patients in the control group were susceptible to later minor hematoma and ecchymosis. Notably, the mean time to hemostasis was longer in this study than reported in the study by Trabattoni et al. (8). Prolonged compression was probably attributed to severe arterial calcification and CAD under dual antiplatelet therapy, leading to difficult hemostasis.
Overall, the study confirmed that QIC safely and effectively reduces the risk of major bleeding complications and the hazard of delayed bleeding in patients with complicated PAOD and comorbidity.
Arthurs et al. (15) established ultrasound-led access for the aforementioned procedures. The complication rate was lowered from 7% to 0% by using ultrasound-guided access. Additionally, the technical success increased from 94% to 98.15%, and the conversion rate fell from 7% to 1.2% (15). All patients in the present study were punctured using ultrasound-guided assistance, with a technical success rate of 100% and a 0% conversion rate.
In addition to puncture techniques and anatomical concerns regarding the puncture site, numerous factors affecting hemostasis include sheath size, antithrombotic drugs (e.g., heparin, aspirin, clopidogrel), vasodilator (PGE 1), hemostatic technique, and underlying diseases. Thus, individual manipulation and assessment, and the assistance of Doppler ultrasound, were necessary for all patients requiring intervention to prevent unnecessary and potentially lethal complications.
VCDs were developed for the management of groin bleeding at the sheath hole. VCD use substantially enhanced the comfort and contentment of patients and lowered the hemostatic and ambulation times (16). According to multiple small randomized controlled trials, meta-analyses, and a Cochrane review, complication rates, safety and efficacy, and outcomes remain comparable between VCDs and MC (12% for VCDs vs. 13% for MC) (16). In addition, VCDs have a low incidence of major complications and high success rates (16). Despite a lower incidence of vascular complications with the use of VCDs, numerous anatomical contraindications for VCDs exist, including diseased peripheral arteries (defined as visual stenosis ≥50%), a small vessel size, severe vessel calcification, prior multiple FA sutures, and bifurcation-site punctures (17-19). Moreover, VCDs have a risk of infectious (0.6% with VCDs vs. 0.2% with MC) and thrombotic complications (0.3% with VCDs vs. none with MC) that is small but may be increased compared with MC (16). Compared with the patients with use of QIC, the patients in the control group were equally likely to develop minor complications. Thus, we suggest MC with QIC as an alternative method for managing sheath-hole bleeding, especially in patients with AFAC.
The QIC [Kaolin-impregnated hemostatic gauze (HG)] also can be used in various clinical situations. Kim et al. study (20) presented that the use of HG during preperitoneal pelvic packing (PPP) did not reduce hemorrhage-induced mortality, but did reduce the need for additional packed red blood cell (RBC) transfusions in patients with hemodynamic instability due to severe pelvic fractures. Song et al. (21) study revealed that prophylactic use of a kaolin-impregnated gauze reduced the incidence of postoperative bleeding after a loop electrosurgical excision procedure (LEEP). Abbott et al. (22) study stated that the use of a kaolin-impregnated intraoperative trauma pad seems to be an effective and inexpensive method to reduce intraoperative blood loss and transfusion volume in pediatric spinal deformity surgery.
Our study identified no anatomical contraindications to MC with QIC, and the incidences of bleeding and major complications were minimal, excepting small hematoma and ecchymosis around the puncture site. The results of this study suggested that MC with QIC may provide similar safety and effectiveness with regards to hemostasis in patients with PAOD together with severe artery calcification as are observed with mechanical compression.
The mean time to complete hemostasis of mechanical compression (C-clamp) group (30 minutes) was compatible with that of the report of Bogart et al. (23) (31 minutes). Moreover, the mean time taken to stop the bleeding with C-clamp (21.22±5.13 minutes) mentioned by Kaur et al.’s study (24), was shorter than that of the control group and longer than that of our QIC group (18±2.20 minutes). These findings supported more that QIC could provide effective hemostasis in patients with severely calcified PAOD.
The time to ambulation is the most concerning problem in these patients. Several patients who have required repeat catheterization frequently complain of being bed-ridden for a long-time post-procedure. The results of this study indicated that patients who received MC using QIC may have been able to ambulate earlier than those who received mechanical compression.
CAD was identified as an independent risk factor for minor complications, and patients with CAD were 6.38 times more likely to exhibit minor complications than those without. This may be attributable to the poor hemodynamic after-effects linked to systemic atherosclerotic changes and vascular calcification; additionally, in this study, antiplatelet treatment was continually provided for almost all patients with CAD until the time of intervention. This may have aggravated bleeding events and led to delayed hematoma, whereas the use of QIC avoided such major complications and reduced the risk of hematoma. Additional larger trials are therefore required to clarify the effect of QIC on vascular complications related to CAD.
Our results did not favor routine usage of QIC in patients with PAOD. In patients with PAOD plus severe arterial calcification of access sites, combined with CAD, QIC can be an alternative and effective strategy to facilitate rapid hemostasis of access sites.
Some limitations were noted in this study. First, this was a nonrandomized study that did not provide sufficient power for extensive statistical comparisons. Second, the number of patients with PAOD and AFAC enrolled in the study was small. Third, subgroup analysis was not a head-to-head or matched comparison.
Conclusions
In conclusion, QIC enables effective and safe hemostasis, and allows quicker ambulation, in patients with PAOD combined with severe AFAC following endovascular interventions. Patients with CAD, which was found to be an independent risk factor for minor complications, who are taking regular antiplatelet agents prior to intervention have a higher risk of minor complications, and use of QIC may reduce the risk of hematoma. Additional randomized studies with larger sample sizes to verify the role of QIC in patients with PAOD are warranted.
Supplementary
The article’s supplementary files as
Acknowledgments
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Institutional Review Board of Taipei Veterans General Hospital (the registration number from clinicaltrials.gov. is TVGH IRB No. 2013-08-020B), and written informed consent was obtained from all patients prior to the endovascular interventions.
Footnotes
Reporting Checklist: The authors have completed the TREND reporting checklist. Available at https://qims.amegroups.com/article/view/10.21037/qims-21-1164/rc
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-21-1164/coif). The authors have no conflicts of interest to declare.
References
- 1.van den Berg JC. Optimal Technique for Common Femoral Artery Access. Endovascular Today 2013:58-61. [Google Scholar]
- 2.Deitch SG, Gupta R. Radioembolization complicated by dissection of the common femoral artery. Semin Intervent Radiol 2011;28:133-6. 10.1055/s-0031-1280650 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Milne AA, Murphy WG, Reading SJ, Ruckley CV. A randomised trial of fibrin sealant in peripheral vascular surgery. Vox Sang 1996;70:210-2. 10.1111/j.1423-0410.1996.tb01328.x [DOI] [PubMed] [Google Scholar]
- 4.Michael Menna. How to stop bleeding in an emergency. Verywell Health. 2021 August. Available online: https://www.verywellhealth.com/how-to-control-bleeding-1298304
- 5.Mabry RL, Holcomb JB, Baker AM, Cloonan CC, Uhorchak JM, Perkins DE, Canfield AJ, Hagmann JH. United States Army Rangers in Somalia: an analysis of combat casualties on an urban battlefield. J Trauma 2000;49:515-28; discussion 528-9. 10.1097/00005373-200009000-00021 [DOI] [PubMed] [Google Scholar]
- 6.Manunga JM, Gloviczki P, Oderich GS, Kalra M, Duncan AA, Fleming MD, Bower TC. Femoral artery calcification as a determinant of success for percutaneous access for endovascular abdominal aortic aneurysm repair. J Vasc Surg 2013;58:1208-12. 10.1016/j.jvs.2013.05.028 [DOI] [PubMed] [Google Scholar]
- 7.Roberts JS, Niu J, Pastor-Cervantes JA. Comparison of Hemostasis Times With a Kaolin-Based Hemostatic Pad (QuikClot Radial) vs Mechanical Compression (TR Band) Following Transradial Access: A Pilot Prospective Study. J Invasive Cardiol 2017;29:328-34. [PubMed] [Google Scholar]
- 8.Trabattoni D, Montorsi P, Fabbiocchi F, Lualdi A, Gatto P, Bartorelli AL. A new kaolin-based haemostatic bandage compared with manual compression for bleeding control after percutaneous coronary procedures. Eur Radiol 2011;21:1687-91. 10.1007/s00330-011-2117-3 [DOI] [PubMed] [Google Scholar]
- 9.Carere RG, Webb JG, Buller CE, Wilson M, Rahman T, Spinelli J, Anis AH. Suture closure of femoral arterial puncture sites after coronary angioplasty followed by same-day discharge. Am Heart J 2000;139:52-8. 10.1016/S0002-8703(00)90308-9 [DOI] [PubMed] [Google Scholar]
- 10.Amin FR, Yousufuddin M, Stables R, Shamim W, Al-Nasser F, Coats AJ, Clague J, Sigwart U. Femoral haemostasis after transcatheter therapeutic intervention: a prospective randomised study of the angio-seal device vs. the femostop device. Int J Cardiol 2000;76:235-40. 10.1016/S0167-5273(00)00386-7 [DOI] [PubMed] [Google Scholar]
- 11.Nasser TK, Mohler ER, 3rd, Wilensky RL, Hathaway DR. Peripheral vascular complications following coronary interventional procedures. Clin Cardiol 1995;18:609-14. 10.1002/clc.4960181105 [DOI] [PubMed] [Google Scholar]
- 12.Arora N, Matheny ME, Sepke C, Resnic FS. A propensity analysis of the risk of vascular complications after cardiac catheterization procedures with the use of vascular closure devices. Am Heart J 2007;153:606-11. 10.1016/j.ahj.2006.12.014 [DOI] [PubMed] [Google Scholar]
- 13.Koreny M, Riedmüller E, Nikfardjam M, Siostrzonek P, Müllner M. Arterial puncture closing devices compared with standard manual compression after cardiac catheterization: systematic review and meta-analysis. JAMA 2004;291:350-7. 10.1001/jama.291.3.350 [DOI] [PubMed] [Google Scholar]
- 14.Huppert P, Tacke J, Lawall H; Deutschen Gesellschaft für Angiologie/Gefässmedizin. S3 guidelines for diagnostics and treatment of peripheral arterial occlusive disease. Radiologe. 2010;50:7-15. 10.1007/s00117-009-1911-2 [DOI] [PubMed] [Google Scholar]
- 15.Arthurs ZM, Starnes BW, Sohn VY, Singh N, Andersen CA. Ultrasound-guided access improves rate of access-related complications for totally percutaneous aortic aneurysm repair. Ann Vasc Surg 2008;22:736-41. 10.1016/j.avsg.2008.06.003 [DOI] [PubMed] [Google Scholar]
- 16.Noori VJ, Eldrup-Jørgensen J. A systematic review of vascular closure devices for femoral artery puncture sites. J Vasc Surg 2018;68:887-99. 10.1016/j.jvs.2018.05.019 [DOI] [PubMed] [Google Scholar]
- 17.Dangas G, Mehran R, Kokolis S, Feldman D, Satler LF, Pichard AD, Kent KM, Lansky AJ, Stone GW, Leon MB. Vascular complications after percutaneous coronary interventions following hemostasis with manual compression versus arteriotomy closure devices. J Am Coll Cardiol 2001;38:638-41. 10.1016/S0735-1097(01)01449-8 [DOI] [PubMed] [Google Scholar]
- 18.Martin JL, Pratsos A, Magargee E, Mayhew K, Pensyl C, Nunn M, Day F, Shapiro T. A randomized trial comparing compression, Perclose Proglide and Angio-Seal VIP for arterial closure following percutaneous coronary intervention: the CAP trial. Catheter Cardiovasc Interv 2008;71:1-5. 10.1002/ccd.21333 [DOI] [PubMed] [Google Scholar]
- 19.Bensley RP, Hurks R, Huang Z, Pomposelli F, Hamdan A, Wyers M, Chaikof E, Schermerhorn ML. Ultrasound-guided percutaneous endovascular aneurysm repair success is predicted by access vessel diameter. J Vasc Surg 2012;55:1554-61. 10.1016/j.jvs.2011.12.042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kim K, Shim H, Jung PY, Kim S, Choi YU, Bae KS, Lee JK, Jang JY. Effectiveness of kaolin-impregnated hemostatic gauze use in preperitoneal pelvic packing for patients with pelvic fractures and hemodynamic instability: A propensity score matching analysis. PLoS One 2020;15:e0236645. 10.1371/journal.pone.0236645 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Song T, Kim KH, Lee KW. Efficacy of a kaolin-impregnated gauze in the prevention of postoperative bleeding after cervical conization. Eur J Gynaecol Oncol 2021;42:1153-8. 10.31083/j.ejgo4206168 [DOI] [Google Scholar]
- 22.Abbott EM, Nandyala SV, Schwend RM. Does a kaolin-impregnated hemostatic dressing reduce intraoperative blood loss and blood transfusions in pediatric spinal deformity surgery? Spine (Phila Pa 1976) 2014;39:E1174-80. 10.1097/BRS.0000000000000466 [DOI] [PubMed] [Google Scholar]
- 23.Bogart MA. Time to hemostasis: a comparison of manual versus mechanical compression of the femoral artery. Am J Crit Care 1995;4:149-56. 10.4037/ajcc1995.4.2.149 [DOI] [PubMed] [Google Scholar]
- 24.Kaur N, Kaur S, Sharma YP. The effect of “Manual vs. ‘c’ Clamp” pressure at the catheter puncture site with reference to comfort level and prevention of vascular complications among patients undergoing cardiac angiography. Nursing & Midwifery Research Journal 2007. doi: 10.1177/0974150X20070303. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as