

It is almost impossible to extract all the stone fragments from the renal collecting system during retrograde intrarenal surgery (RIRS) [1]. The process of self‐elimination is a time‐consuming process that may cause renal colic, residual stone fragments may cause haematuria in the process of self‐elimination [2]. Usually, a ureteric access sheath (UAS) is placed under the pelvi‐ureteric junction (PUJ) in RIRS [3]. This causes the irrigation fluid in the kidney to pass through the PUJ to enter the UAS. The PUJ is relatively narrow and acts as a functional valve between the renal pelvis and proximal ureter [3].
We performed surgery using a novel UAS: a flexible vacuum‐assisted ureteric access sheath (FV‐UAS). The FV‐UAS (12/14 Fr; ZHANGJIAGANG, Jiang Su, China [Fig. 1A–C]) includes a 10‐cm‐long tube at the tip of the UAS that has good flexibility and deformability. The most crucial feature of FV‐UAS is that it can passively bend (bend angle >90°) with the bending of the flexible ureteroscope (f‐URS). The maximum bend achieved with the help of the f‐URS was approximately 145°. The FV‐UAS is reinforced with wire springs to ensure that the lumen does not collapse, and it connects to a vacuum suction device.
Fig. 1.
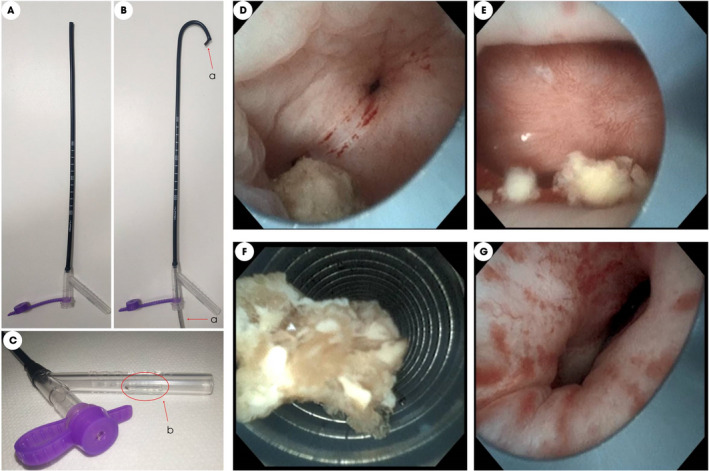
Images showing the flexible vacuum‐assisted ureteric access sheath (FV‐UAS): (A) Normal form of the FV‐UAS. (B) FV‐UAS bent with the flexible ureterorenoscope (f‐URS). (C) Pressure‐regulating vent of the FV‐UAS. (D) FV‐UAS in the renal pelvis and approaching the stone. (E) FV‐UAS in the renal calyx. (F) Stones were removed from the body when the f‐URS was withdrawn. (G) The collection system is shown as not completely filled and in a semicollapsed state. [Colour figure can be viewed at wileyonlinelibrary.com]
A total of 53 consecutive patients (29 male) with renal stones (size 11–25 mm) were treated with RIRS, during which the FV‐UAS was used, between August 2021 and January 2022. The mean (range) patient age was 50 (26–73) years (Table S1). In six cases (11.3%) J tubes were indwelled peri‐operatively. The mean (range) largest stone size was 17.1 (11–25) mm, the mean stone volume was 2555.3 (955.6–5748.8) mm3, and the mean stone density was 1330.6 (892–1965) HU.
This study was approved by the institutional ethics committees (2021–080). Written informed consent was obtained from each of the patients or their guardians. The study followed the principles of the Helsinki Declaration.
The placement method for the FV‐UAS (12/14 Fr; female: 36 cm; male: 46 cm) was the same as that used for the traditional UAS. The position of the FV‐UAS was adjusted to approach the target stone under direct vision of the f‐URS (8.6 Fr; ZebraScopeTM, Guangdong, China). A holmium‐YAG (Moses Laser, Yokneam, Israel) and coupled 200‐μm laser fibre are inserted for stone fragmentation (20–40 Hz, 0.6–1.2 J). The irrigation fluid velocity was 60 mL/min. The tail end of the FV‐UAS was connected to a vacuum suction device and fully vacuum‐assisted (negative pressure: 50–150 cmH2O). The f‐URS was repeatedly inserted and withdrawn slowly to remove stone fragments from the body. A JJ ureteric stent (6 Fr) was inserted during surgery, and removed 2 weeks later. Ultra‐low‐dose CT was performed on the first day after surgery. All patients were followed up for 1 month, and ultra‐low‐dose CT was performed. Stone clearance efficiency on the first postoperative day was reflected by the stone volume clearance rate []. Stone volume was obtained by automatic CT measurements (uCT 520; United‐Imaging, ShangHai, China).
The mean (range) operation time was 70.8 (36–154) min (Table S2). A basket was not used in 29 cases (54.7%). Two patients developed fever symptoms after surgery. The mean (range) stone volume clearance rate was 97.7% (81.1%–100%). Thirty‐seven cases (69.8%) were 100% stone‐free. The mean (range) haemoglobin drop was 0.5 (0–3.2) g/dL on the first postoperative day. The FV‐UAS was able to reach the renal pelvis in all cases when it was successfully placed in the ureter. Six patients had residual stones after 1 month.
Residual fragments (RFs) may lead to an increase in stone size and eventually to reintervention [2, 4], and have therefore been found to have a profound effect on the psychological, functional and social life of patients. At present, there are some novel basket, biocompatible adhesive and magnetic extraction methods that can be used to improve stone‐free rates (SFRs), but these methods have some drawbacks that mean they do not result in stone‐free status [1]. Application of the UAS is conducive to the outflow of irrigation fluid, facilitates operation of the f‐URS, and can also reduce intrarenal pressure, shorten the operation time, and prevent infection [5, 6, 7].
Our research was based on an FV‐UAS that can follow the f‐URS into the renal pelvis and renal calyx to avoid restriction of the PUJ on discharge of irrigation fluid. We obtained good results in vitro using the FV‐UAS, actively controlling intrarenal pressure and obtaining complete stone‐free status during RIRS [8]. Intrarenal pressure was confirmed to be maintained at low levels (<10 cmH2O) in vitro.
During this study, negative pressure was applied to actively suck the irrigation fluid out of the body instead of allowing it to flow out naturally. Therefore, the irrigation fluid velocity could be increased. RFs were carried out of the body by irrigation fluid. The irrigation fluid velocity was 60 mL/min, and the negative pressure was 50–150 cmH2O. The collection system was not filled and remained in a semi‐collapsed state. The degree of collapse of the collection system could be accurately adjusted. The collection system was filled by increasing the irrigation fluid velocity or reducing negative pressure.
We found that stone dust (≤1 mm) can be discharged from the gap between the f‐URS and FV‐UAS. RFs (>1 mm) are discharged when withdrawing the f‐URS slowly. More RFs can be sucked out of the body as the FV‐UAS gets closer to the target stone. Therefore, 37 cases (69.8%) were 100% stone‐free. The principle behind this device is the same as that of the vacuum cleaner. Dust cannot be sucked out when a vacuum cleaner is placed far away. A basket was not used in 29 cases (54.7%), thus avoiding the need to change the basket.
The position of the FV‐UAS in the collection system was closely monitored, and no laceration of the mucous membrane was found. According to the surgeon's recollection, there were no significant differences in the operating procedure compared to placement of the traditional UAS. The FV‐UAS has the disadvantage that it cannot fully follow the movement of the f‐URS. The FV‐UAS can reach the upper calyx, middle calyx, and part of the lower calyx, but it cannot reach the lower calyx of the small infundibulum‐pelvic angle. We suggest using a basket to grab the stones and place them in the upper or middle calyx before stone fragmentation. The ultimate curvature of the f‐URS will be limited when the FV‐UAS is flush with the end of the f‐URS. The ultimate curvature of the f‐URS can be recovered by extending the f‐URS forward or withdrawing the FV‐UAS. The FV‐UAS can extend into the renal pelvis and calyces with the help of an f‐URS. Stone fragments can be efficiently cleaned by vacuum assistance. Baskets are not necessary in RIRS performed using the FV‐UAS.
Further clinical studies and comparisons with available techniques are required to identify more strengths or weaknesses of the FV‐UAS.
Disclosure of Interests
The authors declare no conflicts of interest.
Ethical Approval
The current study is approved by the Ethical Committee of the Jiangxi Provincial People's Hospital (2021–080). Written informed consent was obtained from each of the patients or their guardians. This study followed the principles of the Helsinki Declaration.
Author Contribution
Conception and design: Jie Chen and Renrui Kuang. Surgeons: Renrui Kuang and Jie Chen. Acquisition of data: Yujun Chen, Longhui Lin, Liangliang Zheng, Liang Gao and Chen Li. Analysis and interpretation of data: Yujun Chen and Longhui Lin, Liangliang Zheng. Drafting of the manuscript and statistical analysis: Longlong Ke, Yujun Chen and Longhui Lin. Critical revision: Jie Chen and Renrui Kuang.
Abbreviations
- f‐URS
flexible ureterorenoscope
- FV‐UAS
flexible vacuum‐assisted ureteric access sheath
- PUJ
pelvic‐ureteric junction
- RF
residual fragment
- RIRS
retrograde intrarenal surgery
- UAS
ureteric access sheath
Supporting information
Table S1. Patient demographics and preoperative data.
Table S2. Intra‐operative and postoperative data.
Video S1. Video of surgery.
Acknowledgements
Fund programmes: Health Commission Science and technology program of Jiangxi Province (202210011 to Jie Chen).
Y.C., L.Z. and L.L. contributed equally to this work.
Contributor Information
Renrui Kuang, Email: krrui@126.com.
Jie Chen, Email: cyj13087829362@163.com.
References
- 1. Suarez‐Ibarrola R, Hein S, Miernik A. Residual stone fragments: clinical implications and technological innovations. Curr Opin Urol 2019; 29: 129–34 [DOI] [PubMed] [Google Scholar]
- 2. Brain E, Geraghty R, Lovegrove C, Yang B, Somani B. Natural history of post‐treatment kidney stone fragments: a systematic review and meta‐analysis. J Urol 2021; 206: 526–38 [DOI] [PubMed] [Google Scholar]
- 3. Oratis A, Subasic J, Hernandez N, Bird J, Eisner B. A simple fluid dynamic model of renal pelvis pressures during ureteroscopic kidney stone treatment. PLoS One 2018; 13: e0208209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Prezioso D, Barone B, Di Domenico D, Vitale R. Stone residual fragments: a thorny problem. Urologia 2019; 86: 169–76 [DOI] [PubMed] [Google Scholar]
- 5. De Coninck V, Keller E, Rodríguez‐Monsalve M, Audouin M, Doizi S, Traxer O. Systematic review of ureteral access sheaths: facts and myths. BJU Int 2018; 122: 959–69 [DOI] [PubMed] [Google Scholar]
- 6. Tonyali S. Suctioning ureteral access sheath use in flexible ureteroscopy might decrease operation time and prevent infectious complications. World J Urol 2019; 37: 393–4 [DOI] [PubMed] [Google Scholar]
- 7. Noureldin Y, Kallidonis P, Ntasiotis P, Adamou C, Zazas E, Liatsikos E. In VivoThe effect of irrigation power and ureteral access sheath diameter on the maximal intra‐pelvic pressure during ureteroscopy: experimental study in a live anesthetized pig. J Endourol 2019; 33: 725–9 [DOI] [PubMed] [Google Scholar]
- 8. Chen Y, Li C, Gao L et al. Novel flexible vacuum‐assisted ureteral access sheath(FV‐UAS) can actively control intrarenal pressure and obtain a complete stone‐free status. J Endourol 2022. (Online ahead of print). 10.1089/end.2022.0004 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Patient demographics and preoperative data.
Table S2. Intra‐operative and postoperative data.
Video S1. Video of surgery.