

Abstract
Background
The prevalence of root filled teeth (RFT) worldwide will inform about the amount of clinical activity of dentists dedicated to treat endodontic disease.
Objectives
To carry out a systematic review with meta‐analysis answering the following question: What is the prevalence of RFT around the world? The percentage of people with at least one RFT was also investigated.
Methods
A systematic review including population‐based studies using the following databases: PubMed, EMBASE and Scielo. Studies related to prevalence of RFT were included. The outcome of interest of the study was the prevalence of RFT. The meta‐analyses were calculated with the Open Meta Analyst software to determine the global prevalence of RFT. Subgroups analyses were performed comparing geographical distribution, radiographic method and year of the study (classified in 20th or 21th century). The prevalence of people with at least one RFT was also analysed.
Results
Seventy‐four population‐based studies fulfilled the inclusion criteria. Twenty‐eight, forty‐four and two studies reported high, moderate and low risk of bias, respectively. No obvious publication bias was observed. Prevalence of RFT was estimated with 1 201 255 teeth and 32 162 patients. The calculated worldwide prevalence of RFT was 8.2% (95% CI = 7.3%–9.1%; p < .001). The global prevalence of people with at least one RFT was 55.7% (95% CI = 49.6%–61.8%; p < .001). In 20th century, the prevalence of RFT was 10.2% (95% CI = 7.9%–12.5%; p < .001), whereas in the 21st century the overall calculated prevalence of RFT was 7.5% (95% CI = 6.5%–8.6%; p < .001). Brazilian people (12%) and the European population (9.3%) showed the highest prevalence of RFT. In Europe, 59.6% (95% CI = 52.4%–66.8%) of people has at least one RFT.
Conclusions
This review showed that root canal treatment is a very common therapy throughout the world. More than half of the studied population have at least one RFT. A limitation of the present study is that most of the studies did not consider random sampling for population selection.
Registration
PROSPERO Systematic review registration number: (CRD42022329053).
Keywords: epidemiology, population‐based study, prevalence, root canal treatment, root filled teeth, survey
INTRODUCTION
Irreversible pulpitis and pulp necrosis, without treatment, progress to apical periodontitis (AP), an inflammation of the periapical periodontium, accompanied or not by clinical symptoms, and commonly showing periapical bone resorption (American Association of Endodontists, 2020). Numerous epidemiological studies have investigated the prevalence of apical periodontitis in the general population (Segura‐Egea et al., 2004; Tibúrcio‐Machado et al., 2021). The systematic review carried out by Tibúrcio‐Machado et al. (2021), including studies carried out all over the world, showed a very high global prevalence (52%), with values ranging from less than 30% (Eriksen, 1995; Gulsahi et al., 2008; Skudutyte‐Rysstad & Eriksen, 2006), to values greater than 80% (Al‐Omari et al., 2011; Marotta et al., 2012).
Root canal treatment (RCT) is the indicated endodontic therapy in cases of irreversible pulpitis and/or apical periodontitis (American Association of Endodontists, 2020). Studies carried out recently suggest that the clinical diagnosis of irreversible pulpitis should not always imply root canal treatment (Wolters et al., 2017), as cure of pulpitis has been achieved with less invasive treatments, such as pulp capping and pulpotomy (Asgary et al., 2014, 2018; Careddu & Duncan, 2021). Nevertheless, to date, no study has investigated how these new diagnostic paradigms are affecting endodontic practice.
Root canal treatment continues to be the treatment with which the majority of AP cases are treated and with which it is possible to keep the affected mature tooth functional in the patient's mouth (Trowbridge, 1990).
Considering the high prevalence of AP globally (Tibúrcio‐Machado et al., 2021), the prevalence of RCT can be also expected to be very high. Some studies have investigated the frequency of RCT in different countries (Jiménez‐Pinzón et al., 2004, Kamberi et al., 2011, López‐López et al., 2012), finding a very wide range of percentages of RFT, from 0.7% (Hussein et al., 2016) to 87% (Marotta et al., 2012), as well as people with at least one RFT, from 19.9% (Timmerman et al., 2017) up to 97.3% (Allard & Palmqvist, 1986).
In short, the data on the prevalence of RFT differs from one study to another, reflecting the differences in the needs and availability of RCT in different countries and populations (Caires et al., 2018; Connert et al., 2019), as well as the different impact of the new diagnostic and therapeutic trends in the management of deep carious lesions and pulpitis (Crespo‐Gallardo et al., 2019; Edwards et al., 2021; Wolters et al., 2017). Knowing the prevalence of RFT in the worldwide will allow dentists and policy makers to evaluate the impact that RCT has on the world population.
Taking into account that RCT is the most frequent treatment carried out by endodontists, determining the worldwide prevalence of RFT will also inform about the fraction of clinical activity of dentists dedicated to treat endodontic diseases, which will allow the frequency of RCT to be compared with that of other medical or dental therapies. Finally, the prevalence of RFT worldwide will also tell us how often dentists around the world continue to carry out RCT.
Since no systematic review has been conducted to investigate the prevalence of RFT worldwide, the aim of this study was to conduct a systematic review and meta‐analysis analysing the prevalence of RFT in the adult worldwide population.
MATERIAL AND METHODS
This systematic review is reported using the PRISMA guidelines (Page et al., 2021). The review was registered in the PROSPERO database: (CRD42022329053). This study was conducted following the methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data (Munn et al., 2015).
Search strategy
A literature search was undertaken with no limits on time or language until the 6th of February 2022 in PubMed‐MEDLINE (1949 – present), EMBASE (1949 – present) and Scielo. Most cited descriptors in the previous publication on this theme were used in the electronic search strategy, using combining Medical Subject Heading (MeSH) terms and text word (tw). The search strategies are presented in Table S1. A complementary screening on the references of the selected studies was performed to find any additional study that did not appear in the primary database search. Grey literature was searched (https://opengrey.eu/; https://scholar.google.com/; https://www.greynet.org/) but did not provide useful data.
Eligibility criteria
The review question was formulated following the CoCoPop mnemonic (Munn et al., 2015), as follows:
Condition (Co): What is the prevalence of RFT.
Population (Pop): In the adult population.
Context (Co): Around the world.
The main outcome was the percentage of RFT. Nevertheless, a secondary outcome, the percentage of people with at least one RFT was also considered.
All studies reporting the prevalence of RFT in a healthy adult population by radiographic examination (panoramic, periapical radiographs or cone beam computed tomography) were included.
The following exclusion criteria were applied:
Studies that did not report information about the prevalence of RFT.
Studies that did not provide full mouth information (excluded third molars).
Studies whose entire sample were RFT.
Studies including patients with mixed dentition.
Studies that did not contrast their findings with radiographic examination.
Reviews, letters, posters, conference abstracts or case series and dissertations/thesis with data available in a journal article.
Selection of the studies
Three authors (M.L‐L., D.C‐B. and J.J.S‐E.) selected the studies individually by screening the titles and abstracts. When the title and abstract did not allow judging the study, the full text was accessed. A second stage consisted of reading the full texts and judging the potential studies to be included based on the eligibility criteria. Disagreements on study inclusion were solved by consensus between the three authors. Duplicated studies in the databases search were considered only once.
Data collection/extraction process
The three authors collected the information of the studies that matched the inclusion criteria individually. A fourth author (J.M‐G.) solved disagreements. All the information related to publication were extracted:
Article's identification: Authors, country and year of publication.
Participants: Gender, range and/or mean age of the sample and sample size.
Methods: Method of image acquisition.
Results: Number of people with at least one RFT, number of teeth, number of root filled teeth and distribution of RFT in the sample.
Quality assessment
The quality of evidence of the included studies was analysed according to the guidelines provided by the Centre for Evidence‐Based Medicine at Oxford: http://www.cebm.net/index.aspx?o=5653 (Howick et al., 2011).
Each study was evaluated for inner methodological risk of bias independently by three authors (M.L‐L, D.C‐B and J.M‐G). In case of disagreement, the authors discussed until they reached an agreement.
The methodology used for quality assessment and risk of bias of the individuals studies was based on the Newcastle‐Ottawa Scale adapted for cross‐sectional studies proposed by (Herzog et al., 2013), with the modifications of Tibúrcio‐Machado et al. (2021). This scale was adapted to the outcome of interest, classifying the items into two domains: sample selection and outcome. They were given a point (*) depending on the aspect required were present or missing.
Sample selection (maximum of six points)
Representativeness of the sample
The representativeness of the sample was evaluated depending on the aim of the primary study. To study the prevalence from a certain country, the size and characteristics of the sample should be accordingly to the population and selected randomly. It should use the total target population or use random or non‐random (such as systematic sampling) strategies.
Truly representative of the average in the target population (all subjects or random sampling) ➔ three points.
Somewhat representative of the average in the target population (non‐random sampling) ➔ two points.
Selected group of users ➔ one point.
No description of the sampling strategy ➔ no points.
Sample size
Justified and satisfactory size (study provided sample size calculation) ➔ one point. If the sample size calculation was not available, but the entire population was recruited (and the loss rate was ≤20%), and it was also considered as justified and satisfactory.
Not justified size.
Non‐respondents
Comparability between respondents and non‐respondents characteristics is established, and the response rate is satisfactory (>80%) ➔ two points.
The response rate is unsatisfactory, or the comparability between respondents and non‐respondents is unsatisfactory ➔ one point.
No description of the response rate or the characteristics of the responders ➔ no points.
Outcome (maximum of six points)
Assessment of the outcome
Training and calibration for the methodology of assessing root filled teeth, with inter‐ and intra‐agreement values provided ➔ two points.
Training and calibration for the methodology of assessing root filled teeth, with inter‐ or intra‐agreement values not provided ➔ one point.
Training and calibration not mentioned ➔ no points.
Inclusion of third molar in total sample of teeth
Third molar included ➔ one point. If the study did not mention that third molar was excluded, it got one point in this domain.
Third molar not included ➔ no points.
Inclusion of edentulous in total sample of patients
Edentulous not included ➔ two points.
Edentulous included ➔ one point.
Study did not mention if edentulous were included or not ➔ no points.
Number of observers
Radiographs were studied by two or more examiners ➔ one point.
Only one examiner studied the radiographs ➔ no points.
Studies could score a maximum of 12 points; they were defined as high risk of bias if they scored 0–4 points, moderate risk of bias if they scored 5–8 points and low risk of bias if they scored 9–12 points.
Only dentate patients were taking into account for statistical analysis in studies that included edentulous patients in the sample. Those studies that did not specified if they had or not edentulous patients in the total sample were also included, but it was considered a risk of bias.
Outcome of interest
The main outcome variable was the prevalence of RFT in the population sample study. The prevalence of RFT was first calculated, taking the teeth as the unit of analysis, as the total number of RFT in the sample divided by the total number of teeth in the sample and expressed as a percentage. As a secondary outcome variable, the prevalence of people with at least one RFT was calculated.
Meta‐analysis
To determine the global prevalence of RFT, a meta‐analysis was performed with the OpenMeta Analyst version 10.10 software (Wallace et al., 2012), using the binary random effects model. Additionally, other meta‐analyses were performed using subgroups based on the continent in which the study was carried out, the year of publication and the radiographic method for diagnosis.
To estimate the variance and heterogeneity amongst trials, the Higgings I2 test was employed, considering a slight heterogeneity if it is between 25 and 50%, moderate between 50% and 75%, and high if >75% (Higgins & Thompson, 2002).
RESULTS
Selection of the studies
The flow diagram of literature search strategy and selected studies for this review is shown in Figure 1, according to PRISMA 2020 instructions. Initial search of different databases resulted in 1821 published studies. Duplicated studies (n = 322) were excluded. Then, of the 1499 eligible papers, after analysing the titles and abstracts, 1394 that did not investigate RFT were excluded, selecting 105 for reading the full text. After comprehensive reading, 29 studies were excluded for the reasons specified in Table S2, and 76 studies were selected for the systematic review and meta‐analysis.
FIGURE 1.
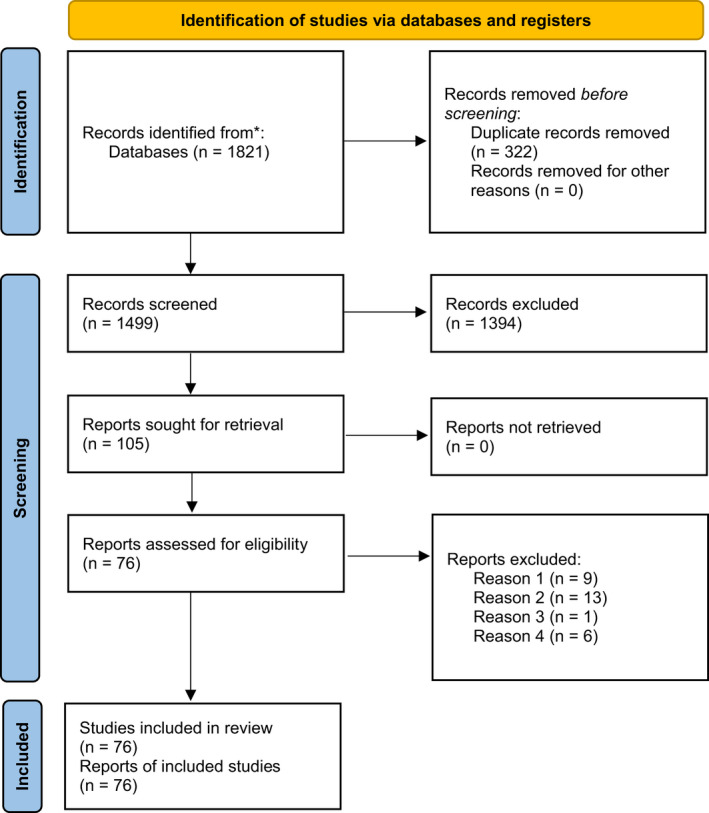
Flow diagram of the search strategy of the systematic review and meta‐analysis following the preferred reporting items for systematic reviews and Meta‐analyses (PRISMA) guidelines 2020 (Page et al., 2021).
Characteristics of the included studies
The main characteristics of the 76 included studies are summarized in Table 1. All the included studies showed the prevalence of RFT in a sample of patients in different populations and countries around the world (Table 2). Thirty‐five of them also provided data on the percentage of people with at least one RFT.
TABLE 1.
Summary of descriptive characteristics of included studies classified geographically
| Authors | Year | Country | Study design | Number of teeth (N) | Sample size | Gender (%) | Age | Image method | Type of evidence |
|---|---|---|---|---|---|---|---|---|---|
| Africa | |||||||||
| Touré et al. | 2008 | Senegal | Cross‐sectional | 6234 | 208 |
MS (55) FS (45) |
>18 years | Periapical | 3 |
| Oginni et al. | 2015 | Nigeria | Cross‐sectional | 21 468 | 756 |
MS 414 FS 342 |
>20 years | Periapical | 3 |
| Ahmed et al. | 2017 | Sudan | Cross‐sectional | 4976 | 200 |
FS 153 MS 47 |
34 ± 12.9 years mean | Panoramic and periapical | 3 |
| America | |||||||||
| Buckley et al. | 1995 | USA | Cross‐sectional | 5272 | 208 |
MS (47.3) FS (52.7) ME 135 FE156 |
44.5 years mean | Bitewing and periapical | 3 |
| Dugas et al. | 2003 | Canada | Cross‐sectional | 16 148 | 610 |
FS 328 (53.8) MS 282 (46.2) |
25–40 years | Panoramic and periapical | 3 |
| Terças et al. | 2006 | Brazil | Cross‐sectional | 5008 | 200 |
FS 112 MS 88 |
Periapical | 3 | |
| Chen et al. | 2007 | USA | Cross‐sectional | 3533 | 206 |
FS (58) MS (42.2) |
55–97 years 67 years mean |
Panoramic | 3 |
| Hollanda et al. | 2008 | Brazil | Cross‐sectional | 29 467 | 1401 | 48 years | Panoramic | 3 | |
| Zhong et al. | 2008 | USA | Cross‐sectional | 27 296 | 853 | Only men | 25–85 years | Periapical | 3 |
| Paes da Silva Ramos et al. | 2013 | Brazil | Cross‐sectional | 5585 | 214 |
FS 124 MS 90 |
CBCT scan | 3 | |
| Hebling et al. | 2014 | Brazil | Cross‐sectional | 942 | 98 |
FS 57 MS 41 |
>60 years | Periapical | 3 |
| Berlinck et al. | 2015 | Brazil | Cross‐sectional | 25 292 | 1126 |
FS 738 MS 388 |
37.1 ± 16.4 years mean | Periapical | 3 |
| Jalali et al. | 2017 | USA | Cross‐sectional | 3395 | 131 |
FS 112 MS 19 |
56.14 years | Panoramic or periapical | 3 |
| Asia | |||||||||
| Tsuneishi et al. | 2005 | Japan | Cross‐sectional | 16 232 | 672 |
MS 244 FS 428 |
20–89 years | Periapical | 3 |
| Sunay et al. | 2007 | Turkey | Cross‐sectional | 8731 | 375 |
MS 147 (39.2) FS 228 (60.8) |
16–82 years | Panoramic | 3 |
| Gulsahi et al. | 2008 | Turkey | Cross‐sectional | 24 433 | 1000 |
MS (39.3) FS (60.7) 555 (3.75) female teeth with endo 257 (2.67) male teeth with endo |
16–80 years 41.4 ± 15.8 years mean |
Panoramic | 3 |
| Asgary et al. | 2010 | Iran | Cross‐sectional | 28 463 | 1064 |
MS 445 (41.8) FS 619 (58.2) |
>18 years | Panoramic | 3 |
| Gencoglu et al. | 2010 | Turkey | Cross‐sectional | 9460 | 400 |
MS 138 (34.5) FS 262 (65.5) |
>20 years 38.7 ± 13.8 years mean |
Panoramic and periapical | 3 |
| Al‐Omari et al. | 2011 | Jordan | Cross‐sectional | 7390 | 294 |
FS 136 (46.3) MS 158 (53.7) |
16–59 years | Panoramic | 3 |
| Gumru et al. | 2011 | Turkey | Cross‐sectional | 28 974 | 1077 |
FS 663 MS 414 |
19 years | Panoramic | 3 |
| Ozbas et al. | 2011 | Turkey | Cross‐sectional | 11 542 | 438 |
FS 234 MS 204 |
10–79 years | Periapical | 3 |
| Mukhaimer et al. | 2012 | Palestine | Cross‐sectional | 6482 | 258 |
FS 142 MS 116 |
39 years 17–62 years |
Panoramic | 3 |
| Kalender et al. | 2013 | Turkey | Cross‐sectional | 24 730 | 1006 |
MS 423 FS 583 |
18–50 years | Panoramic | 3 |
| Ureyen Kaya et al. | 2013 | Turkey | Cross‐sectional | 23 268 | 1000 | >18 years | Panoramic | 3 | |
| Archana et al. | 2015 | India | Cross‐sectional | 30 098 | 1340 | Panoramic | 3 | ||
| Alrahabi et al. | 2016 | Saudi Arabia | Cross‐sectional | 15 686 | 630 |
FS 314 MS 316 |
Panoramic | 3 | |
| Hussein et al. | 2016 | Malaysia | Cross‐sectional | 6409 | 233 |
FS 147 (63.1) MS 86 (36.9) |
26 years | Panoramic | 3 |
| Europe | |||||||||
| Allard et al. | 1986 | Sweden | Cross‐sectional | 2567 | 188 | >65 years | Periapical series | 3 | |
| Petersson et al. | 1986 | Sweden | Cross‐sectional | 4985 | 861 | 20–60 years | Bitewing and periapical | 3 | |
| Bergström et al. | 1987 | Sweden | Cross‐sectional | 6593 | 250 | 21–60 years | Periapical series | 3 | |
| Eckerbom et al. | 1988 | Sweden | Longitudinal | 4889 | 200 |
MS 93 FS 107 |
>20 years | Bitewing and periapical | 3 |
| Eriksen et al. | 1988 | Sweden | Cross‐sectional | 3917 | 141 | 35 years | Panoramic and periapical | 3 | |
| Petersson et al. | 1989 | Sweden | Cross‐sectional | 11 497 | 567 | >20 years | Periapical series | 2 | |
| Odesjo et al. | 1990 | Sweden | Cross‐sectional | 17 430 | 733 |
MS 392 FS 351 |
>20 years | Periapical series | 2 |
| Eriksen et al. | 1991 | Norway | Cross‐sectional | 2940 | 119 | 50 years | Panoramic | 3 | |
| Imfeld et al. | 1991 | Switzerland | Cross‐sectional | 2004 | 143 |
MS 69 (47.7) FS 74 (52.3) |
66 years | Panoramic and periapical | 3 |
| De Cleen et al. | 1993 | Netherlands | Cross‐sectional | 4196 | 184 |
FS 90 (48.9) MS 94 (51.1) |
>20 years | Panoramic | 3 |
| Ainamo et al. | 1994 | Finland | Cross‐sectional | 2355 | 169 |
MS 54 FS 115 |
76–86 years | Panoramic and periapical | 3 |
| Eriksen et al. | 1995 | Norway | Longitudinal | 3282 | 118 | 35 years | Panoramic | 3 | |
| Soikonen et al. | 1995 | Finland | Cross‐sectional | 2355 | 169 |
MS 54 FS 115 |
Panoramic and periapical | 3 | |
| Weiger et al. | 1997 | Germany | Cross‐sectional | 7987 | 323 |
FS (54) MS (46) |
35.2 years | Panoramic and periapical | 3 |
| Marques et al. | 1998 | Portugal | Cross‐sectional | 4446 | 179 | 30–39 years | Panoramic and bitewings | 3 | |
| Sidaravicius et al. | 1999 | Lithuania | Cross‐sectional | 3892 | 147 | Panoramic | 2 | ||
| De Moor et al. | 2000 | Belgium | Cross‐sectional | 4617 | 206 | Panoramic | 3 | ||
| Narhi et al. | 2000 | Finland | Cross‐sectional | 1016 | 77 |
FS 51 MS 26 |
Panoramic | 3 | |
| Kirkevang et al. | 2001 | Denmark | Cross‐sectional | 15 984 | 614 |
FS 303 (49.3) MS 311 (50.7) |
20–60 years | Bitewing and periapical | 2 |
| Boucher et al. | 2002 | France | Cross‐sectional | 5373 | 208 | FS (62) | 45.9 ± 12.9 years | Periapical | 3 |
| Lupi‐Pegurier et al. | 2002 | France | Cross‐sectional | 7561 | 344 |
MS 164 FS 180 |
>20 years | Panoramic | 3 |
| Jimenez‐Pinzon et al. | 2004 | Spain | Cross‐sectional | 4453 | 180 |
MS 66 FS 114 |
Periapical | 3 | |
| Georgopoulou et al. | 2005 | Greece | Cross‐sectional | 7664 | 320 |
FS (65.3) MS (34.7) |
16–77 years | Periapical | 3 |
| Kabak et al. | 2005 | Belarus | Cross‐sectional | 31 212 | 1423 | >15 years | Panoramic | 3 | |
| Loftus et al. | 2005 | Ireland | Cross‐sectional | 7424 | 302 |
MS 127 FS 175 M.RFT 57 F.RFT 95 |
16–98 years | Panoramic | 3 |
| Kirkevang et al. | 2006 | Denmark | Longitudinal | 12 329 | 473 |
FS 239 MS 234 |
>18 years | Bitewing and periapical | 3 |
| Skudutyte‐Rysstad et al. | 2006 | Norway | Cross‐sectional | 3971 | 146 | 35 years mean | Panoramic | 3 | |
| Frisk et al. | 2008 | Sweden | Longitudinal | 12 433 | 491 |
MS 242 FS 249 |
10–80 years | Panoramic and periapical | 3 |
| Segura‐Egea et al. | 2008 | Spain | Cross‐sectional | 4453 | 180 |
MS 66 (36.7) FS 114 (63.3) |
>18 years | Periapical | 3 |
| Covello et al. | 2010 | Italy | Cross‐sectional | 9423 | 384 |
MS (44.3) FS (55.7) |
18–60 years 43 years mean |
Panoramic | 3 |
| Kamberi et al. | 2011 | Kosovo | Cross‐sectional | 4131 | 193 |
ME (3) FE (1.8) |
34.5 ± 11.2 years | Panoramic | 3 |
| Matijevic et al. | 2011 | Croatia | Cross‐sectional | 38 440 | 1462 | >15 years | Panoramic | 3 | |
| Peters et al. | 2011 | Netherlands | Cross‐sectional | 4594 | 178 |
MS 84 FS 94 |
Female 35.4 ± 13.2 Male 40.2 ± 12.6 |
Panoramic | 3 |
| Huumonen et al. | 2012 | Finland | Cross‐sectional | 120 250 | 5244 | MS 48% | 30–95 years | Panoramic | 3 |
| López‐López et al. | 2012 | Spain | Cross‐sectional | 9390 | 397 |
FS 203 MS 194 |
52 years | Panoramic | 3 |
| Rocha et al. | 2012 | Portugal | Cross‐sectional | 5552 | 222 |
FS 119 (53.76) MS 103 (46.24) |
>18 years 41.26 ± 15.86 years mean |
Panoramic | 3 |
| Jersa et al. | 2013 | Latvia | Cross‐sectional | 7065 | 312 | 35–44 years | Panoramic | 3 | |
| Di Filippo et al. | 2014 | UK | Cross‐sectional | 3396 | 136 |
FS 73 MS 63 |
Panoramic | 3 | |
| Dutta et al. | 2014 | Scotland | Cross‐sectional | 3595 | 245 |
FS 117 MS 128 |
>18 years | CBCT scan | 3 |
| Lemagner et al. | 2015 | France | Cross‐sectional | 2368 | 100 |
FS 53 MS 47 |
47.1 years | CBCT scan | 3 |
| Huumonen et al. | 2017 | Finland | Cross‐sectional | 120 635 | 5335 | MS (47) | 50.2 years | Panoramic | 2 |
| Kielbassa et al. | 2017 | Austria | Cross‐sectional | 22 586 | 1000 |
FS 570 MS430 |
Panoramic | 3 | |
| Van der Veken et al. | 2017 | Belgium | Cross‐sectional | 11 117 | 631 |
MS 267 FS 364 |
45.6 years | CBCT scan | 3 |
| Vengerfeldt et al. | 2017 | Estonia | Cross‐sectional | 181 495 | 6552 |
FS 3989 (60.9) MS 2563 (39.1) |
3–93 years | Panoramic | 3 |
| Bürklein et al. | 2019 | Germany | Cross‐sectional | 8244 | 500 |
FS 297 (59.4) MS 203 (40.6) |
50.21 years | CBCT scan | 2 |
| Meirinhos et al. | 2020 | Portugal | Cross‐sectional | 20 836 | 1160 |
FS 663 MS 497 |
48.4 years | CBCT scan | 3 |
| Oceania | |||||||||
| Punch | 1997 | Australia | Cross‐sectional | 5216 | 204 | Panoramic | 3 | ||
| Da Silva et al. | 2009 | Australia | Cross‐sectional | 5647 | 243 | Panoramic | 3 | ||
| Timmerman et al. | 2017 | Australia | Cross‐sectional | 16 936 | 695 | FS (58.3) |
10–88 years 41 years mean |
Panoramic | 3 |
Abbreviations: FS, prevalence in female subject; MS, prevalence in male subject; RFT, root filled teeth.
TABLE 2.
Prevalence of root filled teeth (RFT) and percentage of people with at least one RFT in the 74 included studies
| Authors | Year | Country | Prevalence of RFT (%; 95% CI) | Percentage of people with at least one RFT (95% CI) |
|---|---|---|---|---|
| Africa | ||||
| Touré et al. | 2008 | Senegal | 2.6 (2.2–3.0) | Not provided |
| Oginni et al. | 2015 | Nigeria | 12.2 (11.8–12.7) | 61.2 (57.8–64.7) |
| Ahmed et al. | 2017 | Sudan | 1.6 (1.3–2.0) | 21.0 (15.4–26.6) |
| America | ||||
| Buckley et al. | 1995 | USA | 5.5 (4.9–6.1) | Not provided |
| Dugas et al. | 2003 | Canada | 2.5 (2.3–2.8) | 62.8 (59.0–66.6) |
| Terças et al. | 2006 | Brazil | 11.0 (10.2–11.9) | Not provided |
| Chen et al. | 2007 | USA | 4.8 (4.1–5.5) | 38.8 (32.2–45.5) |
| Hollanda et al. | 2008 | Brazil | 21.4 (21.0–21.9) | Not provided |
| Zhong et al. | 2008 | USA | 2.2 (2.1–2.4) | 33.8 (30.6–36.9) |
| Paes da Silva Ramos et al. | 2013 | Brazil | 7.4 (6.7–8.1) | Not provided |
| Hebling et al. | 2014 | Brazil | 13.4 (11.2–15.5) | 49.0 (39.1–58.9) |
| Berlinck et al. | 2015 | Brazil | 6.9 (6.6–7.2) | Not provided |
| Jalali et al. | 2017 | USA | 5.7 (4.9–6.4) | 58.8 (50.3–67.2) |
| Asia | ||||
| Tsuneishi et al. | 2005 | Japan | 20.5 (19.8–21.1) | 86.5 (83.9–89.0) |
| Sunay et al. | 2007 | Turkey | 5.1 (4.7–5.6) | 46.9 (41.9–52.0) |
| Gulsahi et al. | 2008 | Turkey | 3.3 (3.1–3.5) | Not provided |
| Asgary et al. | 2010 | Iran | 3.6 (3.3–3.8) | 41.4 (38.5–44.4) |
| Gencoglu et al. | 2010 | Turkey | 9.4 (8.8–10.0) | Not provided |
| Al‐Omari et al. | 2011 | Jordan | 5.7 (5.2–6.3) | Not provided |
| Gumru et al. | 2011 | Turkey | 1.6 (1.4–1.7) | 61.2 |
| Ozbas et al. | 2011 | Turkey | 1.6 (1.3–1.8) | Not provided |
| Mukhaimer et al. | 2012 | Palestine | 13.2 (12.4–14.0) | Not provided |
| Kalender et al. | 2013 | Turkey | 8.9 (8.5–9.3) | 64.0 |
| Ureyen Kaya et al. | 2013 | Turkey | 2.6 (2.4–2.8) | Not provided |
| Archana et al. | 2015 | India | 4.1 (3.9–4.3) | Not provided |
| Alrahabi et al. | 2016 | Saudi Arabia | 6.4 (6.0–6.7) | 52.8 |
| Hussein et al. | 2016 | Malaysia | 0.7 (0.5–0.9) | Not provided |
| Europe | ||||
| Allard et al. | 1986 | Sweden | 17.6 (16.1–19.1) | 97.3 |
| Petersson et al. | 1986 | Sweden | 13.0 (12.1–14.0) | Not provided |
| Bergström et al. | 1987 | Sweden | 6.5 (5.9–7.1) | Not provided |
| Eckerbom et al. | 1988 | Sweden | 13.0 (12.1–14.0) | Not provided |
| Eriksen et al. | 1988 | Sweden | 3.4 (2.8–4.0) | 53.2 |
| Petersson et al. | 1989 | Sweden | 22.2 (21.4–22.9) | 93.0 |
| Odesjo et al. | 1990 | Sweden | 8.6 (8.1–9.0) | Not provided |
| Eriksen et al. | 1991 | Norway | 6.0 (5.1–6.8) | 56.0 |
| Imfeld et al. | 1991 | Switzerland | 20.3 (18.5–22.0) | 77.6 |
| De Cleen et al. | 1993 | Netherlands | 2.3 (1.9–2.8) | Not provided |
| Ainamo et al. | 1994 | Finland | 21.0 (19.4–22.7) | 76.0 |
| Eriksen et al. | 1995 | Norway | 1.3 (0.9–1.7) | 24.0 |
| Soikonen et al. | 1995 | Finland | 21.5 (19.9–23.2) | Not provided |
| Weiger et al. | 1997 | Germany | 2.7 (2.3–3.0) | Not provided |
| Marques et al. | 1998 | Portugal | 1.6 (1.2–1.9) | 22.0 |
| Sidaravicius et al. | 1999 | Lithuania | 8.2 (7.4–9.1) | 64.6 |
| De Moor et al. | 2000 | Belgium | 6.8 (6.0–7.5) | Not provided |
| Narhi et al. | 2000 | Finland | 21.1(18.6–23.6) | Not provided |
| Kirkevang et al. | 2001 | Denmark | 4.8 (4.5–5.2) | 52.0 |
| Boucher et al. | 2002 | France | 19.1 (18.0–20.1) | Not provided |
| Lupi‐Pegurier et al. | 2002 | France | 18.9 (18.0–19.8) | Not provided |
| Jimenez‐Pinzon et al. | 2004 | Spain | 2.1 (1.7–2.5) | Not provided |
| Georgopoulou et al. | 2005 | Greece | 8.9 (8.2–9.5) | 65.6 |
| Kabak et al. | 2005 | Belarus | 20.3 (19.9–20.8) | Not provided |
| Loftus et al. | 2005 | Ireland | 2.0 (1.7–2.4) | 31.8 |
| Kirkevang et al. | 2006 | Denmark | 5.7 (5.2–6.1) | 58.8 |
| Skudutyte‐Rysstad et al. | 2006 | Norway | 1.5 (1.2–1.9) | 23.0 |
| Frisk et al. | 2008 | Sweden | 5.5 (5.1–5.9) | Not provided |
| Segura‐Egea et al. | 2008 | Spain | 2.1 (1.7–2.5) | 41.0 |
| Covello et al. | 2010 | Italy | 11.4 (10.8–12.1) | Not provided |
| Kamberi et al. | 2011 | Kosovo | 2.3 (1.8–2.8) | Not provided |
| Matijevic et al. | 2011 | Croatia | 8.5 (8.3–8.8) | 75.9 |
| Peters et al. | 2011 | Netherlands | 4.9 (4.3–5.5) | Not provided |
| Huumonen et al. | 2012 | Finland | 7.3 (7.2–7.5) | 61.3 |
| López‐López et al. | 2012 | Spain | 6.4 (5.9–6.9) | Not provided |
| Rocha et al. | 2012 | Portugal | 3.9 (3.4–4.4) | Not provided |
| Jersa et al. | 2013 | Latvia | 17.8 (16.9–18.7) | 87.0 |
| Di Filippo et al. | 2014 | UK | 3.4 (2.8–4.0) | Not provided |
| Dutta et al. | 2014 | Scotland | 4.8 (4.1–5.5) | Not provided |
| Lemagner et al. | 2015 | France | 18.2 (16.6–19.8) | Not provided |
| Huumonen et al. | 2017 | Finland | 6.6 (6.5–6.8) | 58.0 |
| Kielbassa et al. | 2017 | Austria | 11.1 (10.7–11.5) | Not provided |
| Van der Veken et al. | 2017 | Belgium | 12.2 (11.6–12.8) | 70.2 |
| Vengerfeldt et al. | 2017 | Estonia | 6.9 (6.8–7.1) | 58.2 |
| Bürklein et al. | 2019 | Germany | 8.2 (7.6–8.8) | Not provided |
| Meirinhos et al. | 2020 | Portugal | 11.1 (10.6–11.5) | Not provided |
| Oceania | ||||
| Punch | 1997 | Australia | 2.4 (2.0–2.8) | Not provided |
| Da Silva et al. | 2009 | Australia | 8.8 (8.1–9.5) | Not provided |
| Timmerman et al. | 2017 | Australia | 1.7 (1.5–1.9) | 19.9 |
Note: The studies have been ordered by continents and countries.
Outcomes of the primary meta‐analysis and publication bias
To conduct the meta‐analysis, only the last year of follow‐up in longitudinal studies were included. The 76 studies included added 32 162 people, who had 1 201 255 teeth, of which 92 999 were RFT. Figure 2 shows the forest plot of the primary meta‐analysis. The overall calculated prevalence of RFT was 8.2% (95% CI = 7.3%–9.1%). Heterogeneity value was I2 = 99.8% (p < .001).
FIGURE 2.
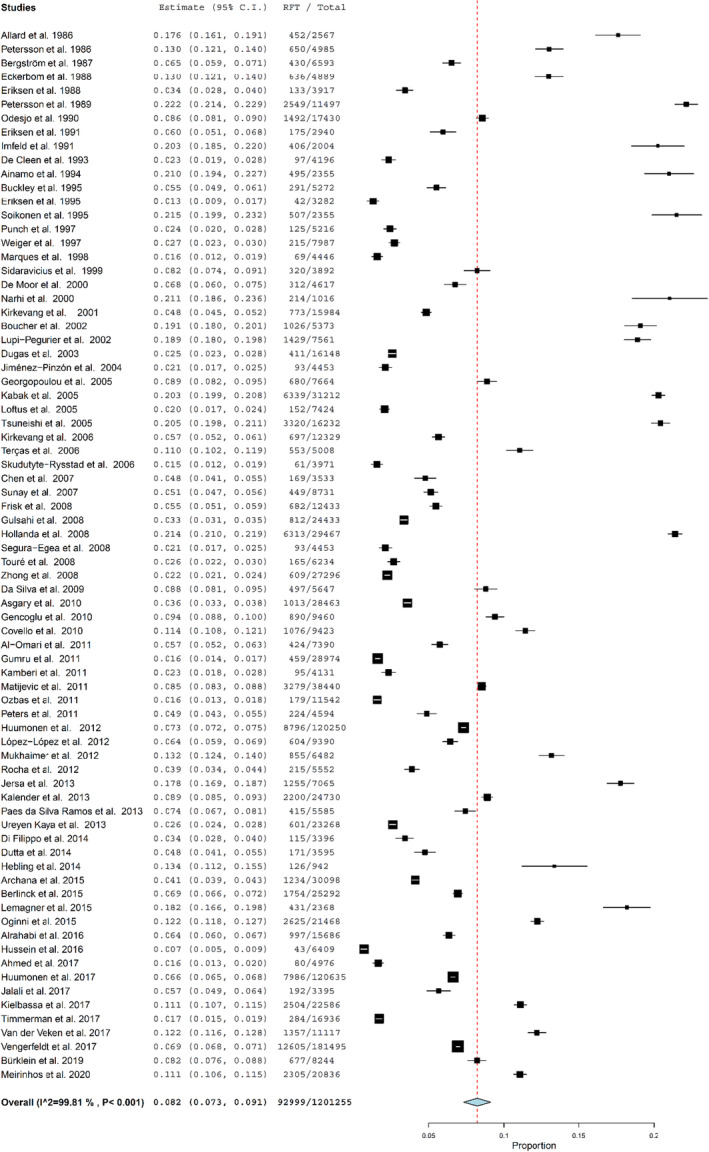
Forest plot of the prevalence of root filled teeth (RFT) in all the included studies.
Subgroup analysis: Prevalence of people with at least one RFT
A subgroup analysis was made including 35 studied that provided information about patients with at least one RFT (Figure 3). This meta‐analysis included 31 715 people, of which, 18 577 had at least one RFT (55.7%; 95% CI = 49.6%–61.8%). The heterogeneity was I2 = 99.3% (p < .001).
FIGURE 3.
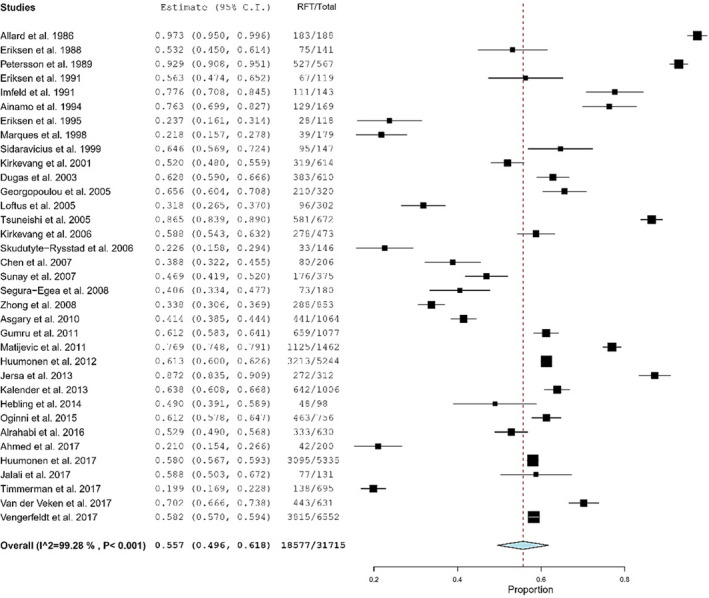
Forest plot of the studies that have calculated the percentage of people with at least one root filled teeth (RFT) in the total sample.
Subgroup analysis: Geographical distribution
The geographical distribution of the prevalence of RFT was analysed by grouping the studies according to the continent in which they had been carried out. The results are shown on the world map in Figure 4. By countries, Brazilian people showed the highest prevalence of RFT (12.0%; 95% CI = 5.2%–18.9%), five Brazilian studies being the only data available on the South American continent. For the rest of continents, the European population showed the highest prevalence of RFT, 9.3% (95% CI = 8.2%–10.4%), having 59.6% (95% CI = 52.4%–66.8%) of people at least one RFT. On the contrary, the North American population showed the lowest prevalence of RFT, 4.1% (95% CI = 3.0%–5.2%), and 48.5% (95% CI = 31.7%–65.2%) had at least one RFT.
FIGURE 4.
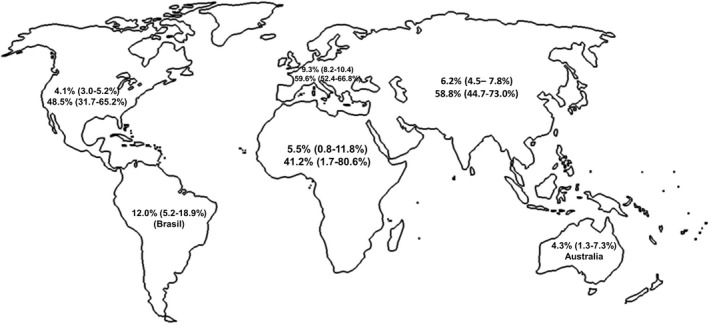
World map showing the prevalence of root filled teeth (RFT) (up) and the percentage of people with at least one RFT (down) calculated in the forest plots of the studies carried out in each continent. The values of South America are only from Brazil.
Subgroup analysis: Year of publication
To analyse the possible variation in the prevalence of RFT over time, separate meta‐analyses were performed for studies conducted in the 20th century and those conducted in the 21st century, including 19 articles from the 20th century and 54 articles from the 21th century (Figure 5). In the 20th century, the prevalence of RFT was 10.2% (95% CI = 7.9%–12.5%), whereas in the 21st century the overall calculated prevalence of RFT was 7.6% (95% CI = 6.5%–8.6%). Heterogeneity values were I2 = 99.7% (p < .001) for 20th century studies, and I2 = 99.8% (p < .001) for the studies carried out in the 21st century.
FIGURE 5.
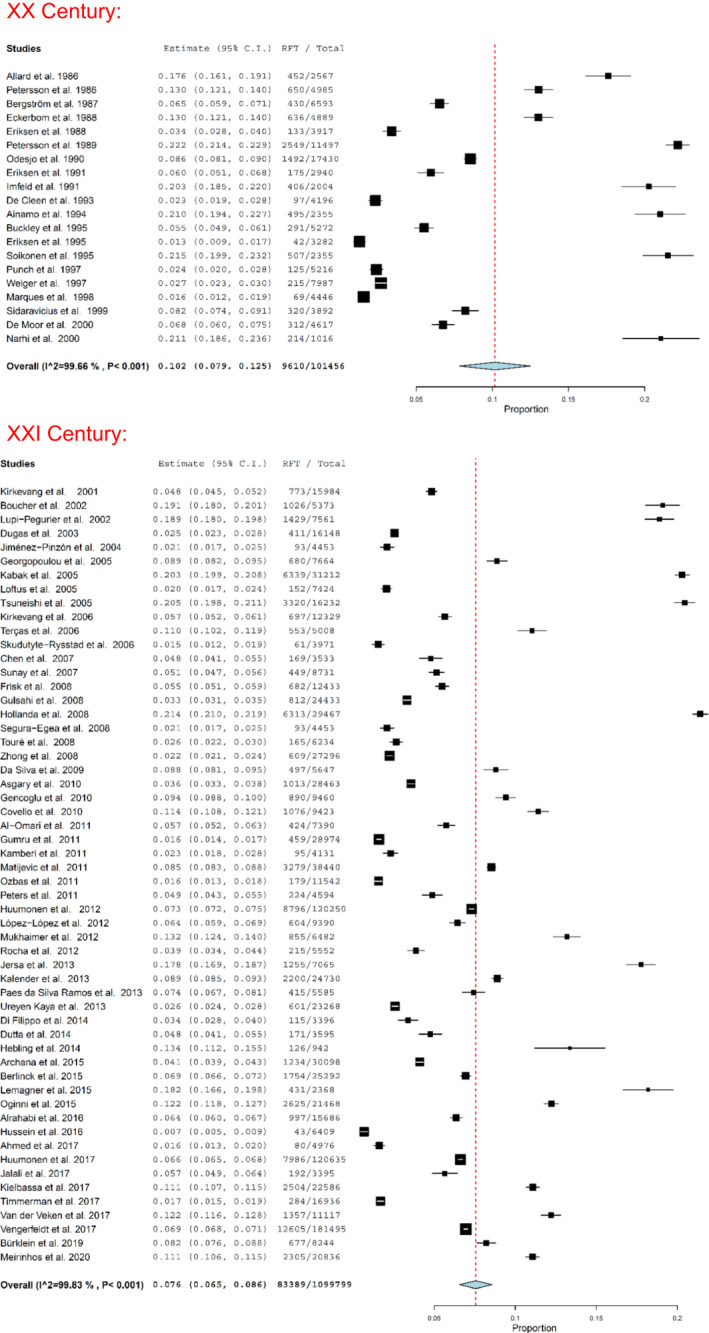
Forest plot of the prevalence of root filled teeth (RFT) in the studies carried out in the 20th and 21st centuries.
Subgroup analysis: Type of radiographic diagnosis
Another analysis of subgroup was made comparing the prevalence of RFT depending on the radiographic method of diagnosis. Studies were grouped according to the radiographic method used: periapical radiograph (n = 21), cone beam computed tomography (CBCT) (n = 6) and panoramic radiograph (n = 38). Studies that used more than one radiographic method for diagnosis were excluded. The forest plot of these subgroups of studies is shown in Figure 6.
FIGURE 6.
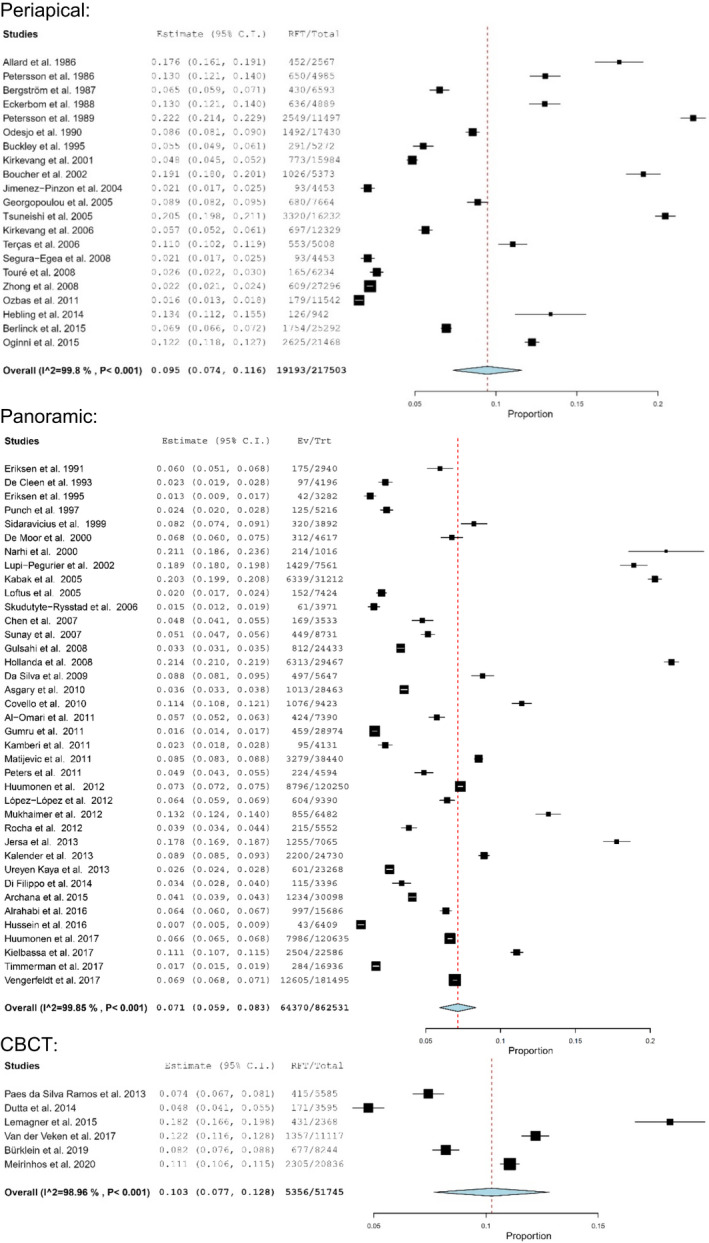
Forest plots of subgroups analysis according to the type of radiographic diagnosis: Periapical radiographs (up), panoramic radiographs (middle) and cone beam computed tomography (CBCT) (down).
The prevalence of RFT in the studies that used periapical radiographs was 9.5% (95% CI = 7.4%–11.6%). The heterogeneity was I2 = 99.8% (p < .001). The calculated prevalence of RFT for the studies that used panoramic radiographs was 7.2% (95% CI = 6.0%–8.5%), being the heterogeneity value I2 = 99.9% (p < .001). Only six of the included studies used CBCT for radiographic diagnosis (Bürklein et al., 2020; da Paes Silva Ramos Fernandes et al., 2013; Dutta et al., 2014; Lemagner et al., 2015; Meirinhos et al., 2020; Van der Veken et al., 2017). The prevalence of RFT calculated for CBCT studies was 10.3% (95% CI = 7.7%–12.8%), being the heterogeneity 99.0% (p < .001).
Quality assessment
Study quality was assessed to determine the risk of bias. For each study, data are showed in Table S3. Twenty‐nine studies were classified as high risk of bias (Ainamo et al., 1994; Allard & Palmqvist, 1986; Bergström et al., 1987; Berlinck et al., 2015; Boucher et al., 2002; Buckley & Spangberg, 1995; Chen et al., 2007; Covello et al., 2010; Dutta et al., 2014; Eckerbom et al., 1987; Eriksen, 1995; Eriksen et al., 1988; Eriksen & Bjertness, 1991; Frisk et al., 2008; Gumru et al., 2011; Hollanda et al., 2008; Jalali et al., 2017; Jersa & Kundzina, 2013; Loftus et al., 2005; López‐López et al., 2012; Meirinhos et al., 2020; Närhi et al., 2000; Oginni et al., 2015; Petersson et al., 1986; Punch, 1997; Soikkonen, 1995; Sunay et al., 2007; Vengerfeldt et al., 2017; Weiger et al., 1997). Forty‐five studies were classified as moderate risk of bias (Ahmed et al., 2017; Al‐Omari et al., 2011; Alrahabi & Younes, 2016; Archana et al., 2015; Asgary et al., 2010; Bürklein et al., 2020; da Paes Silva Ramos Fernandes et al., 2013; Da Silva et al., 2009; De Cleen et al., 1993; De Moor et al., 2000; Di Filippo et al., 2014; Dugas et al., 2003; Gencoglu et al., 2010; Georgopoulou et al., 2005; Gulsahi et al., 2008; Hebling et al., 2014; Hussein et al., 2016; Huumonen et al., 2012; Imfeld, 1991; Jersa & Kundzina, 2013; Jiménez‐Pinzón et al., 2004; Kabak & Abbott, 2005; Kalender et al., 2013; Kamberi et al., 2011; Kielbassa et al., 2017; Kirkevang et al., 2001, 2006; Lemagner et al., 2015; Lupi‐Pegurier et al., 2002; Marques et al., 1998; Matijević et al., 2011; Mukhaimer et al., 2012; Özbaş et al., 2011; Peters et al., 2011; Petersson et al., 1989; Rocha et al., 2012; Segura‐Egea et al., 2008; Sidaravicius et al., 1999; Skudutyte‐Rysstad & Eriksen, 2006; Terças et al., 2006; Timmerman et al., 2017; Touré et al., 2008; Tsuneishi et al., 2005; Ureyen Kaya et al., 2013; Van der Veken et al., 2017; Zhong et al., 2008), and only two of the 74 included studies were classified as low risk of bias (Huumonen et al., 2017; Ödesjö et al., 1990).
DISCUSSION
The aim of this systematic review has been to analyse the worldwide prevalence of RCT. Based on raw data from the primary study, it can be concluded that globally, 8.2% of teeth have been endodontically treated, and 55.7% of adults over the age of 18 have at least one RFT. In short, more than half of the world's population has had at least one RCT. The data provided by this systematic review can be considered the first scientific approximation to the prevalence of RCT worldwide.
Prevalence and incidence systematic review and meta‐analysis is an emerging methodology in the field of evidence synthesis. These reviews can provide useful information for healthcare professionals and policymakers on the burden of diseases, conditions or therapies, showing their geographical distribution and their changes and trends over time (Munn et al., 2015). Taking into account that the traditional PICO approach to inclusion criteria used in systematic reviews of effects evidently does not align with questions relating to prevalence, the CoCoPop mnemonic (condition, context, and population) approach has been used (Munn et al., 2015).
The high frequency of RFT showed in this study, together with the previously high prevalence of AP found in the world population, 52% of people and 5% of teeth (Tibúrcio‐Machado et al., 2021), place endodontic disease and RCT as one of the most frequent and important health problems in the world population. The high prevalence of AP (Tibúrcio‐Machado et al., 2021) and RCT should be taken into account by those responsible for health policies and the medical and dental communities, in view of the distribution of dental resources. Likewise, the academic authorities and the universities should also value the need to give the necessary extension to endodontics in the training curriculum of dentists.
The databases search provided nearly 2000 articles that, applying the inclusion criteria, resulted in a systematic review of 74 full‐text articles analysed. All the studies investigated the prevalence of RFT in a certain population of patients over 18 years of age using different diagnostic radiographic methods.
Both cross‐sectional and longitudinal studies were included in the present review. In the included longitudinal studies in which various stages of follow‐up are reported (Eriksen et al., 1988; Frisk et al., 2008; Kirkevang et al., 2006), only the most recent data have been taken into account.
Articles that studied the prevalence of RFT in people with systemic disease were excluded. Both the prevalence of AP (Katz & Rotstein, 2021; Liljestrand et al., 2016; Segura‐Egea et al., 2015) and RFT (Caplan et al., 2009; Gomes et al., 2016; Meurman et al., 2017) are influenced by the systemic status of the patient, so including these studies in the review would have altered the results by introducing confounding factors.
Subgroup analysis: Geographical distribution
When the studies included in this systematic review are classified geographically, the results show that the prevalence of RFT is very different from one country to another. Furthermore, different studies in the same country provide very different data. This is the case of Finland, where the prevalence of RCT ranges from 6.6% (Huumonen et al., 2012, 2017) to 21.5% (Ainamo et al., 1994; Närhi et al., 2000; Soikkonen, 1995). This variability, rather than by geographical factors, may be caused by an important confounding factor that must be taken into account when assessing the results of this study: age. Since RCT is the treatment for endodontic disease and it develops throughout life, older people, logically, have a higher frequency of RCT. For this reason, studies in which the sample is made up of elderly people (Ainamo et al., 1994, Närhi et al., 2000, Soikkonen, 1995) show a higher prevalence of RCT compared to studies in which the sample consisted of younger people (Huumonen et al., 2012, 2017). Something similar occurs with the data reported by the Swedish studies. However, almost none of the studies provided detailed information on the distribution by age or gender of the patients included in the sample.
Grouping the studies by continents, Europe and South America are the ones that show the highest prevalence of RFT. However, the data for South America come from studies carried out in a single country, Brazil, as well as the data for Oceania (only Australia). In the case of Brazil, the high frequency of RFT found may be a reflection of the fact that there are more studies on this subject in this country.
The African population shows the lowest prevalence of RFT. The differences in the age of the populations (Jiang et al., 2021), the different level of economic development (Bas & Azogui‐Lévy, 2022; Listl et al., 2015), and the different access to dental health services (Kodama et al., 2021) can explain the differences observed between continents. The highest levels of per capita dental expenditures has been found for High‐Income North America, Australasia, Western Europe, High‐Income Asia Pacific, and East Asia (Righolt et al., 2018).
Subgroup analysis: Year of publication
In the forest plot including the studies conducted in the 20th century the calculated prevalence of RFT was 10.2% (95% CI = 7.9%–12.5%), substantially higher than calculated for studies conducted in the 21st century 7.6% (95% CI = 6.5%–8.6%).
A possible explanation would be the improvement in oral health quality devoted to greater prevention, together with minimal intervention in operative dentistry (Mount, 2007). The increase in the standard of living that has been taking place in the last 50 year (Akachi & Canning, 2015), could have facilitated access to dental care, reducing the incidence of caries (Whelton et al., 2019), with the consequent reduction in the incidence of pulpitis and apical periodontitis around the world, thus explaining a progressive decrease in the prevalence of RFT.
On the contrary, another possible explanation could be the increase in dental implant treatments that has taken place in the last three decades (Elani et al., 2018). Dentists and patients could have chosen to extract the teeth affected by irreversible pulpitis and/or apical periodontitis and place dental implants, rather than perform RCT.
And yet there may still be another explanation. Dentists may be changing their prescription habits for RCT, reserving it only for cases of apical periodontitis. The impact that the development of minimally invasive dentistry has undoubtedly had on the practice of endodontics (Wolters et al., 2017), may have caused a reduction in the number of RCT performed in recent years. During the second half of the 20th century, and even during the first decade of the present century, RCT was still indicated by some endodontic societies (American Association of Endodontists, 2009) as the treatment of choice, not only for the treatment of apical periodontitis but also for irreversible pulpitis, diagnosed by the presence of spontaneous pain (American Association of Endodontists, 2020). This could have produced an endodontic overtreatment that would be reflected in a high prevalence of RFT (Crespo‐Gallardo et al., 2019). However, since the end of the 20th century and, especially in the past two decades, numerous studies (Careddu & Duncan, 2021; Duncan et al., 2021) have been demonstrating that spontaneous pain is not always indicative of irreversible pulpitis and that more conservative and less invasive therapeutic options, such as pulpotomy, could resolve, in many cases, supposedly irreversible pulpitis (Asgary et al., 2018; Marending et al., 2016). This change in therapeutic approaches has been able to influence the results of the most recent studies, in which lower RCT prevalence are found.
Subgroup analysis: Type of radiographic diagnosis
The radiographic method used in each study for the diagnosis of RFT was different. Most of the studies (36) used panoramic, 21 used periapical radiographs, and only six, all published after 2013, used CBCT. Although it might be thought that the detection of RFT can be performed with the same precision with any of the three methods, the studies using CBCT reported the highest prevalence of RFT (10.3%), followed by those using periapical radiographs (9.5%) and, finally, the studies using panoramic radiographs (7.1%). The results seem to indicate that, in addition to the publication date, the result of each study may be influenced by the radiographic method used for diagnosis. CBCT gives a three‐dimensional image of the entire root canal system making it easier to know the root anatomy. This three‐dimensional image helps to find supernumerary canals and roots, making easier the diagnosis of RFT (Liang et al., 2013; Nekoofar et al., 2006; Segato et al., 2018). The fact that studies in which CBCT is used provide the highest prevalence of RFT, all of them being carried out in the 21st century, in which the prevalence of RFT tends to decrease, indicates that, certainly, CBCT detects RFT with greater precision.
Implications for clinical practice and research
The progressive reduction of the prevalence of RFT showed in the present systematic review can be interpreted as a reflection of the impact that minimally invasive dentistry and endodontics (Wolters et al., 2017), and the new recommendations on the more conservative treatment of deep caries lesions (Duncan et al., 2021; Innes et al., 2016; Schwendicke et al., 2016) are having throughout the world (Machiulskiene et al., 2020).
Determining the real effect that the recommendations of international societies (Duncan et al., 2021; Innes et al., 2016) based on scientific evidence have on dental practice is very complex. For decades, pulpal conditions that could have been treated by vital pulp therapy procedures have been diagnosed as irreversible pulpitis based on the existence of spontaneous pain (American Association of Endodontists, 2009). On the contrary, this diagnosis, in many cases erroneous, has led to hundreds of teeth undergoing RCT unnecessarily (Crespo‐Gallardo et al. 2019). Scientific certainty that spontaneous pain does not always imply irreversible pulpitis has resulted in an increase in vital pulp therapy procedures within endodontic practice (Asgary et al., 2014; Careddu & Duncan, 2021). Added to this fact are the advances in the field of preventive dentistry, dental materials, and conservative dentistry, now focused on minimally invasive dentistry. In short, the results of this study show that the paradigm can be finally changing: the focus of endodontic practice may be shifting towards less invasive therapies, such as pulpotomy, pulp capping and dental pulp regenerative procedures.
Quality assessment
More than half of the studies were classified as moderate risk of bias and only two studies as low risk of bias (Huumonen et al., 2017; Ödesjö et al., 1990). The main drawbacks of the studies were from the sample selection, since most of the studies considered a selected group of patients, without taking into account the random sampling. Only five included studies calculated the sample size needed to improve the representativeness of the studied population (Bürklein et al., 2020; Hussein et al., 2016; Huumonen et al., 2017; Kirkevang et al., 2001; Timmerman et al., 2017). Then, a limitation of this systematic review is that, in most of the studies, the samples were drawn from patients seen in university dental clinics and are not representative of the general population. Similar limitation has been found in a previous systematic review analysing the prevalence of AP (Tibúrcio‐Machado et al., 2021). However, the large sample size of the analysis may, at least in part, compensate for this limitation.
Given the very low proportion of RCTs performed on third molars, whether or not the third molar was included in the study does not represent a major limitation. So, low risk of bias was considered if the third molar was included in the total sample. Similarly, if edentulous patients were not included in the total patient sample, low risk of bias was also considered. On the contrary, when the study did not specify whether it included edentulous patients in the total sample, it was considered to be a very high risk of bias.
Strength and limitations
As previously considered, the results of the present systematic review should be evaluated with caution, since the samples of the different studies are not representative of the general population. On the contrary, the large number of studies included in the systematic review, 76 can be considered a strength and compensate, at least partially, for the limitation of non‐random sampling.
CONCLUSIONS
Root canal treatment is a very common therapy throughout the world. More than half of the studied population have at least one RFT. The percentage of RFT worldwide is, on average, greater than 8%. When studies conducted in the 20th century are compared with those of the 21st century, a decrease in the prevalence of RFT is observed, which could indicate a change in the therapeutic attitudes of dentists in the management of endodontic diseases.
AUTHOR CONTRIBUTIONS
Conceptualization, D.C.‐B. & J.J.S.‐E.; Methodology and Software, D.C.‐B. & M.L.‐L.; Validation, J.J.S.‐E., J.M.‐G., D.C.‐B. & P.M.‐M.; Formal Analysis P.M.‐M. & D.C.‐B.; Investigation M.L.‐L., J.J.S.‐M., P.M.‐M., J.M.‐G., D.C.‐B. & J.J.S.‐E.; Data Curation J.J.S.‐E., M.L.‐L. & D.C.‐B.; Writing – Original Draft Preparation J.J.S.‐E., M.L.‐L., P.M‐M., & D.C.‐B.; Writing – Review & Editing, D.C.‐B., J.M.‐G. & J.J.S.‐E.; Visualization P.M.‐M., J.J.S.‐M., J.M.‐G. & J.J.S.‐E.; Supervision J.J.S.‐E. & D.C.‐B. All authors have reviewed and approved the submitted version. All authors developed the idea and contributed to the final version of the manuscript equally.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ETHICS STATEMENT
This systematic review did not need the Ethics Committee Approval due to the absence of research with patients.
Supporting information
Table S1
Table S2
Table S3
ACKNOWLEDGEMENTS
María Léon López is research fellow supported by Spanish Ministerio de Educación y Formación Profesional (collaboration grant 2020‐21).
León‐López, M. , Cabanillas‐Balsera, D. , Martín‐González, J. , Montero‐Miralles, P. , Saúco‐Márquez, J.J. & Segura‐Egea, J.J. (2022) Prevalence of root canal treatment worldwide: A systematic review and meta‐analysis. International Endodontic Journal, 55, 1105–1127. Available from: 10.1111/iej.13822
DATA AVAILABILITY STATEMENT
Data available on request from the authors.
REFERENCES
- Ahmed, I. , Ali, R.W. & Mudawi, A.M. (2017) Prevalence of apical periodontitis and frequency of root‐filled teeth in an adult Sudanese population. Clinical and Experimental Dental Research, 3, 142–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ainamo, A. , Soikkonen, K. , Wolf, J. , Siukosaari, P. , Erkinjuntti, T. , Tilvis, R. et al. (1994) Dental radiographic findings in the elderly in Helsinki, Finland. Acta Odontologica Scandinavica, 52, 243–249. [DOI] [PubMed] [Google Scholar]
- Akachi, Y. & Canning, D. (2015) Inferring the economic standard of living and health from cohort height: evidence from modern populations in developing countries. Economics and Human Biology, 19, 114–128. [DOI] [PubMed] [Google Scholar]
- Allard, U. & Palmqvist, S. (1986) A radiographic survey of periapical conditions in elderly people in a Swedish county population. Dental Traumatology, 2, 103–108. [DOI] [PubMed] [Google Scholar]
- Al‐Omari, M.A. , Hazaa, A. & Haddad, F. (2011) Frequency and distribution of root filled teeth and apical periodontitis in a Jordanian subpopulation. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, 111, e59–e65. [DOI] [PubMed] [Google Scholar]
- Alrahabi, M. & Younes, H.B. (2016) A cross‐sectional study of the quality of root canal treatment in Al‐Madinah Al‐Munawwarah. Saudi Endodontic Journal, 6, 31–35. [Google Scholar]
- American Association of Endodontists . (2009) AAE consensus conference recommended diagnostic terminology. Journal of Endodontics, 35, 1634. [Google Scholar]
- American Association of Endodontists . (2020) Glossary of endodontic terms, Vol. 9. Chicago: American Association of Endodontists, p. 33. [Google Scholar]
- Archana, D. , Gopikrishna, V. , Gutmann, J.L. , Savadamoorthi, K.S. , Pradeep Kumar, A.R. & Narayanan, L.L. (2015) Prevalence of periradicular radiolucencies and its association with the quality of root canal procedures and coronal restorations in an adult urban Indian population. Journal of Conservative Dentistry, 18, 34–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asgary, S. , Shadman, B. , Ghalamkarpour, Z. , Shahravan, A. , Ghoddusi, J. , Bagherpour, A. et al. (2010) Periapical status and quality of root canal fillings and coronal restorations in Iranian population. Iranian Endodontic Journal, 5, 74–82. [PMC free article] [PubMed] [Google Scholar]
- Asgary, S. , Eghbal, M.J. & Ghoddusi, J. (2014) Two‐year results of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter randomized clinical trial. Clinical Oral Investigations, 18, 635–641. [DOI] [PubMed] [Google Scholar]
- Asgary, S. , Hassanizadeh, R. , Torabzadeh, H. & Eghbal, M.J. (2018) Treatment outcomes of 4 vital pulp therapies in mature molars. Journal of Endodontics, 44, 529–535. [DOI] [PubMed] [Google Scholar]
- Bas, A.C. & Azogui‐Lévy, S. (2022) Socio‐economic determinants of dental service expenditure: findings from a french national survey. International Journal of Environmental Research and Public Health, 19, 1310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bergström, J. , Eliasson, S. & Ahlberg, K.F. (1987) Periapical status in subjects with regular dental care habits. Community Dentistry and Oral Epidemiology, 15, 236–239. [DOI] [PubMed] [Google Scholar]
- Berlinck, T. , Tinoco, J.M. , Carvalho, F.L. , Sassone, L.M. & Tinoco, E.M. (2015) Epidemiological evaluation of apical periodontitis prevalence in an urban Brazilian population. Brazilian Oral Research, 29, 51–57. [DOI] [PubMed] [Google Scholar]
- Boucher, Y. , Matossian, L. , Rilliard, F. & Machtou, P. (2002) Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. International Endodontic Journal, 35, 229–238. [DOI] [PubMed] [Google Scholar]
- Buckley, M. & Spangberg, L.S.W. (1995) The prevalence and technical quality of endodontic treatment in an American subpopulation. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, 79, 92–100. [DOI] [PubMed] [Google Scholar]
- Bürklein, S. , Schäfer, E. , Jöhren, H.P. & Donnermeyer, D. (2020) Quality of root canal fillings and prevalence of apical radiolucencies in a German population: a CBCT analysis. Clinical Oral Investigations, 24, 1217–1227. [DOI] [PubMed] [Google Scholar]
- Caires, N.C.M. , de Brito, L.C.N. , Vieira, L.Q. & Sobrinho, A.P.R. (2018) Epidemiological analysis and need for endodontic treatment among the indigenous Sateré‐Mawé and Tikuna. Brazilian Oral Research, 32, e19. [DOI] [PubMed] [Google Scholar]
- Caplan, D.J. , Pankow, J.S. , Cai, J. , Offenbacher, S. & Beck, J.D. (2009) The relationship between self‐reported history of endodontic therapy and coronary heart disease in the atherosclerosis risk in communities study. The Journal of the American Dental Association, 140, 1004–1012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Careddu, R. & Duncan, H.F. (2021) A prospective clinical study investigating the effectiveness of partial pulpotomy after relating preoperative symptoms to a new and established classification of pulpitis. International Endodontic Journal, 54, 2156–2172. [DOI] [PubMed] [Google Scholar]
- Chen, C.‐Y. , Hasselgren, G. , Serman, N. , Elkind, M.S.V. , Desvarieux, M. & Engebretson, S.P. (2007) Prevalence and quality of endodontic treatment in the northern Manhattan elderly. Journal of Endodontics, 33, 230–234. [DOI] [PubMed] [Google Scholar]
- Connert, T. , Truckenmüller, M. , ElAyouti, A. , Eggmann, F. , Krastl, G. , Löst, C. et al. (2019) Changes in periapical status, quality of root fillings and estimated endodontic treatment need in a similar urban German population 20 years later. Clinical Oral Investigations, 23, 1373–1382. [DOI] [PubMed] [Google Scholar]
- Covello, F. , Franco, V. , Schiavetti, R. , Clementini, M. , Mannocci, A. , Ottria, L. et al. (2010) Prevalence of apical periodontitis and quality of endodontic treatment in an Italian adult population. Oral Implantology, 3, 9–14. [PMC free article] [PubMed] [Google Scholar]
- Crespo‐Gallardo, I. , Hay‐Levytska, O. , Martín‐González, J. , Jiménez‐Sánchez, M.C. , Sánchez‐Domínguez, B. , Cabanillas‐Balsera, D. et al. (2019) Correction: criteria and treatment decisions in the management of deep caries lesions: is there endodontic overtreatment? Journal of Clinical and Experimental Dentistry, 11, e103. Erratum for: J Clin Exp Dent. 2018 Aug 1; 10(8): e751–e760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- da Paes Silva Ramos Fernandes, L.M. , Ordinola‐Zapata, R. , Húngaro Duarte, M.A. & Alvares Capelozza, A.L. (2013) Prevalence of apical periodontitis detected in cone beam CT images of a Brazilian subpopulation. Dento Maxillo Facial Radiology, 42, 80179163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Da Silva, K. , Lam, J.M. , Wu, N. & Duckmanton, P. (2009) Cross‐sectional study of endodontic treatment in an Australian population. Australian Endodontic Journal Endod, 35, 140–146. [DOI] [PubMed] [Google Scholar]
- De Cleen, M.J. , Schuurs a, H. , Wesselink, P.R. & Wu, M.K. (1993) Periapical status and prevalence of endodontic treatment in an adult Dutch population. International Endodontic Journal, 26, 112–119. [DOI] [PubMed] [Google Scholar]
- De Moor, R.J. , Hommez, G.M. , De Boever, J.G. , Delmé, K.I. & Martens, G.E. (2000) Periapical health related to the quality of root canal treatment in a Belgian population. International Endodontic Journal, 33, 113–120. [DOI] [PubMed] [Google Scholar]
- Di Filippo, G. , Sidhu, S.K. & Chong, B.S. (2014) Apical periodontitis and the technical quality of root canal treatment in an adult sub‐population in London. British Dental Journal, 216, E22. [DOI] [PubMed] [Google Scholar]
- Dugas, N.N. , Lawrence, H.P. , Teplitsky, P.E. , Pharoah, M.J. & Friedman, S. (2003) Periapical health and treatment quality assessment of root‐filled teeth in two Canadian populations. International Endodontic Journal, 36, 181–192. [DOI] [PubMed] [Google Scholar]
- Duncan, H.F. , Tomson, P.L. , Simon, S. & Bjørndal, L. (2021) Endodontic position statements in deep caries management highlight need for clarification and consensus for patient benefit. International Endodontic Journal, 54, 2145–2149. [DOI] [PubMed] [Google Scholar]
- Dutta, A. , Smith‐Jack, F. & Saunders, W.P. (2014) Prevalence of periradicular periodontitis in a Scottish subpopulation found on CBCT images. International Endodontic Journal, 47, 854–863. [DOI] [PubMed] [Google Scholar]
- Eckerbom, M. , Andersson, J.‐E. & Magnusson, T. (1987) Frequency and technical standard of endodontic treatment in a Swedish population. Dental Traumatology, 3, 245–248. [DOI] [PubMed] [Google Scholar]
- Edwards, D. , Bailey, O. , Stone, S.J. & Duncan, H. (2021) How is carious pulp exposure and symptomatic irreversible pulpitis managed in UK primary dental care? International Endodontic Journal, 54, 2256–2275. [DOI] [PubMed] [Google Scholar]
- Elani, H.W. , Starr, J.R. , Da Silva, J.D. & Gallucci, G.O. (2018) Trends in dental implant use in the U.S., 1999‐2016, and projections to 2026. Journal of Dental Research, 97, 1424–1430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eriksen, M. (1995) Changes in endodontic status 1973‐1993 amoog 35‐year‐olds in Oslo, Norway. International Endodontic Journal, 2, 129–132. [DOI] [PubMed] [Google Scholar]
- Eriksen, H.M. & Bjertness, E. (1991) Prevalence of apical periodontitis and results of endodontic treatment in middle‐aged adults in Norway. Endodontics & Dental Traumatology, 7, 1–4. [DOI] [PubMed] [Google Scholar]
- Eriksen, H.M. , Bjertness, E. & Brstavik, D. (1988) Prevalence and quality of endodontic treatment in an urban adult population in Norway. Dental Traumatology, 4, 122–126. [DOI] [PubMed] [Google Scholar]
- Frisk, F. , Hugoson, A. & Hakeberg, M. (2008) Technical quality of root fillings and periapical status in root filled teeth in Jönköping, Sweden. International Endodontic Journal, 41, 958–968. [DOI] [PubMed] [Google Scholar]
- Gencoglu, N. , Pekiner, F.N. , Gumru, B. & Helvacioglu, D. (2010) Periapical status and quality of root fillings and coronal restorations in an adult turkish subpopulation. European Journal of Dentistry, 4, 17–22. [PMC free article] [PubMed] [Google Scholar]
- Georgopoulou, M.K. , Spanaki‐Voreadi, A.P. , Pantazis, N. & Kontakiotis, E.G. (2005) Frequency and distribution of root filled teeth and apical periodontitis in a Greek population. International Endodontic Journal, 38, 105–111. [DOI] [PubMed] [Google Scholar]
- Gomes, M.S. , Hugo, F.N. , Hilgert, J.B. , Sant'Ana Filho, M. , Padilha, D.M.P. , Simonsick, E.M. et al. (2016) Apical periodontitis and incident cardiovascular events in the Baltimore longitudinal study of ageing. International Endodontic Journal, 49, 334–342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gulsahi, K. , Gulsahi, A. , Ungor, M. & Genc, Y. (2008) Frequency of root‐filled teeth and prevalence of apical periodontitis in an adult Turkish population. International Endodontic Journal, 41, 78–85. [DOI] [PubMed] [Google Scholar]
- Gumru, B. , Tarcin, B. , Pekiner, F.N. & Ozbayrak, S. (2011) Retrospective radiological assessment of root canal treatment in young permanent dentition in a Turkish subpopulation. International Endodontic Journal, 44, 850–856. [DOI] [PubMed] [Google Scholar]
- Hebling, E. , Coutinho, L.A. , Ferraz, C.C.R. , Cunha, F.L. & de Queluz, D.P. (2014) Periapical status and prevalence of endodontic treatment in institutionalized elderly. Brazilian Dental Journal, 25, 123–128. [DOI] [PubMed] [Google Scholar]
- Herzog, R. , Álvarez‐Pasquin, M.J. , Díaz, C. , Del Barrio, J.L. , Estrada, J.M. & Gil, Á. (2013) Are healthcare workers intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health, 13, 154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins, J.P.T. & Thompson, S.G. (2002) Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine, 21, 1539–1558. [DOI] [PubMed] [Google Scholar]
- Hollanda, A.C.B. , de Alencar, A.H.G. , de Estrela, C.R.A. , Bueno, M.R. & Estrela, C. (2008) Prevalence of endodontically treated teeth in a Brazilian adult population. Brazilian Dental Journal, 19, 313–317. [DOI] [PubMed] [Google Scholar]
- Howick, J. , Chalmers, I. , Glasziou, P. , Greenhalgh, T. , Heneghan, C. , Liberati, A. et al. (2011) The 2011 Oxford CEBM levels of evidence: introductory document. Oxford, UK: Centre for Evidence‐Based Medicine, pp. 1–3. http://www.cebm.net/index.aspx?o=5653 [Google Scholar]
- Hussein, F.E. , Liew, A.K.C. , Ramlee, R.A. , Abdullah, D. & Chong, B.S. (2016) Factors associated with apical periodontitis: a multilevel analysis. Journal of Endodontics, 42, 1441–1145. [DOI] [PubMed] [Google Scholar]
- Huumonen, S. , Vehkalahti, M.M. & Nordblad, A. (2012) Radiographic assessments on prevalence and technical quality of endodontically‐treated teeth in the Finnish population, aged 30 years and older. Acta Odontologica Scandinavica, 70, 234–240. [DOI] [PubMed] [Google Scholar]
- Huumonen, S. , Suominen, A.L. & Vehkalahti, M.M. (2017) Prevalence of apical periodontitis in root filled teeth: findings from a nationwide survey in Finland. International Endodontic Journal, 50, 229–236. [DOI] [PubMed] [Google Scholar]
- Imfeld, T.N. (1991) Prevalence and quality of endodontic treatment in an elderly urban population of Switzerland. Journal of Endodontics, 17, 604–607. [DOI] [PubMed] [Google Scholar]
- Innes, N.P.T. , Frencken, J.E. , Bjørndal, L. , Maltz, M. , Manton, D.J. , Ricketts, D. et al. (2016) Managing carious lesions: consensus recommendations on terminology. Advances in Dental Research, 28, 49–57. [DOI] [PubMed] [Google Scholar]
- Jalali, P. , Glickman, G.N. , Schneiderman, E.D. & Schweitzer, J.L. (2017) Prevalence of periapical rarefying osteitis in patients with rheumatoid arthritis. Journal of Endodontics, 43, 1093–1096. [DOI] [PubMed] [Google Scholar]
- Jersa, I. & Kundzina, R. (2013) Periapical status and quality of root fillings in a selected adult Riga population. Stomatologija, 15, 73–77. [PubMed] [Google Scholar]
- Jiang, C.M. , Chu, C.H. , Duangthip, D. , Ettinger, R.L. , Hugo, F.N. , Kettratad‐Pruksapong, M. et al. (2021) Global perspectives of oral health policies and oral healthcare schemes for older adult populations. Frontiers in Oral Health, 16(2), 703526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jiménez‐Pinzón, a. , Segura‐Egea, J.J. , Poyato‐Ferrera, M. , Velasco‐Ortega, E. & Ríos‐Santos, J.V. (2004) Prevalence of apical periodontitis and frequency of root‐filled teeth in an adult Spanish population. International Endodontic Journal, 37, 167–173. [DOI] [PubMed] [Google Scholar]
- Kabak, Y. & Abbott, P.V. (2005) Prevalence of apical periodontitis and the quality of endodontic treatment in an adult Belarusian population. International Endodontic Journal, 38, 238–245. [DOI] [PubMed] [Google Scholar]
- Kalender, A. , Orhan, K. , Aksoy, U. , Basmaci, F. , Er, F. & Alankus, A. (2013) Influence of the quality of endodontic treatment and coronal restorations on the prevalence of apical periodontitis in a turkish cypriot population. Medical Principles and Practice, 22, 173–177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kamberi, B. , Hoxha, V. , Stavileci, M. , Dragusha, E. , Kuçi, A. & Kqiku, L. (2011) Prevalence of apical periodontitis and endodontic treatment in a Kosovar adult population. BMC Oral Health, 11, 32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katz, J. & Rotstein, I. (2021) Prevalence of periapical abscesses in patients with hypertension: a cross‐sectional study of a large hospital population. Journal of Endodontics, 47, 1070–1074. [DOI] [PubMed] [Google Scholar]
- Kielbassa, A.M. , Frank, W. & Madaus, T. (2017) Radiologic assessment of quality of root canal fillings and periapical status in an Austrian subpopulation – an observational study. PLoS One, 12, e0176724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirkevang, L.L. , Hörsted‐Bindslev, P. , Ørstavik, D. & Wenzel, A. (2001) Frequency and distribution of endodontically treated teeth and apical periodontitis in an urban Danish population. International Endodontic Journal, 34, 198–205. [DOI] [PubMed] [Google Scholar]
- Kirkevang, L.L. , Væth, M. , Hörsted‐Bindslev, P. & Wenzel, A. (2006) Longitudinal study of periapical and endodontic status in a Danish population. International Endodontic Journal, 39, 100–107. [DOI] [PubMed] [Google Scholar]
- Kodama, T. , Ida, Y. , Oshima, K. & Miura, H. (2021) Are public oral care services evenly distributed?‐nation‐wide assessment of the provision of oral care in Japan using the national database of health insurance claims. International Journal of Environmental Research and Public Health, 18, 10850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lemagner, F. , Maret, D. , Peters, O.A. , Arias, A. , Coudrais, E. & Georgelin‐Gurgel, M. (2015) Prevalence of apical bone defects and evaluation of associated factors detected with cone‐beam computed tomographic images. Journal of Endodontics, 41, 1043–1047. [DOI] [PubMed] [Google Scholar]
- Liang, Y.‐H. , Jiang, L. , Chen, C. , Gao, X.J. , Wesselink, P.R. , Wu, M.K. et al. (2013) The validity of cone‐beam computed tomography in measuring root canal length using a gold standard. Journal of Endodontics, 39, 1607–1610. [DOI] [PubMed] [Google Scholar]
- Liljestrand, J.M. , Mäntylä, P. , Paju, S. , Buhlin, K. , Kopra, K.A.E. , Persson, G.R. et al. (2016) Association of endodontic lesions with coronary artery disease. Journal of Dental Research, 95, 1358–1365. [DOI] [PubMed] [Google Scholar]
- Listl, S. , Galloway, J. , Mossey, P.A. & Marcenes, W. (2015) Global economic impact of dental diseases. Journal of Dental Research, 94, 1355–1361. [DOI] [PubMed] [Google Scholar]
- Loftus, J.J. , Keating, A.P. & McCartan, B.E. (2005) Periapical status and quality of endodontic treatment in an adult Irish population. International Endodontic Journal, 38, 81–86. [DOI] [PubMed] [Google Scholar]
- López‐López, J. , Jané‐Salas, E. , Estrugo‐Devesa, A. , Castellanos‐Cosano, L. , Martín‐González, J. , Velasco‐Ortega, E. et al. (2012) Frequency and distribution of root‐filled teeth and apical periodontitis in an adult population of Barcelona, Spain. International Dental Journal, 62, 40–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lupi‐Pegurier, L. , Bertrand, M.F. , Muller‐Bolla, M. , Rocca, J.P. & Bolla, M. (2002) Periapical status, prevalence and quality of endodontic treatment in an adult French population. International Endodontic Journal, 35, 690–697. [DOI] [PubMed] [Google Scholar]
- Machiulskiene, V. , Campus, G. , Carvalho, J.C. , Dige, I. , Ekstrand, K.R. , Jablonski‐Momeni, A. et al. (2020) Terminology of dental caries and dental caries management: consensus report of a workshop organized by ORCA and cariology research group of IADR. Caries Research, 54, 7–14. [DOI] [PubMed] [Google Scholar]
- Marending, M. , Attin, T. & Zehnder, M. (2016) Treatment options for permanent teeth with deep caries. Swiss Dental Journal, 126, 1007–1027. [DOI] [PubMed] [Google Scholar]
- Marotta, P.S. , Fontes, T.V. , Armada, L. , Lima, K.C. , Roças, I.N. & Siqueira, J.F. (2012) Type 2 diabetes mellitus and the prevalence of apical periodontitis and endodontic treatment in an adult brazilian population. Journal of Endodontics, 38, 297–300. [DOI] [PubMed] [Google Scholar]
- Marques, M.D. , Moreira, B. & Eriksen, H.M. (1998) Prevalence of apical periodontitis and results of endodontic treatment in an adult Portuguese population. International Endodontic Journal, 31, 161–165. [DOI] [PubMed] [Google Scholar]
- Matijević, J. , Dadić, T.C. , Mehičić, G.P. , Anić, I. , Šlaj, M. & Krmek, S.J. (2011) Prevalence of apical periodontitis and quality of root canal fillings in population of Zagreb, Croatia: a cros‐ssectional study. Croatian Medical Journal, 52, 679–687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meirinhos, J. , Martins, J.N.R. , Pereira, B. , Baruwa, A. , Gouveia, J. , Quaresma, S.A. et al. (2020) Prevalence of apical periodontitis and its association with previous root canal treatment, root canal filling length and type of coronal restoration – a cross‐sectional study. International Endodontic Journal, 53, 573–574. [DOI] [PubMed] [Google Scholar]
- Meurman, J.H. , Janket, S. , Surakka, M. , Jackson, E.A. & Ackerson, L.K. (2017) Lower risk for cardiovascular mortality for patients with root filled teeth in a Finnish population. International Endodontic Journal, 50, 1158–1168. [DOI] [PubMed] [Google Scholar]
- Mount, G.J. (2007) A new paradigm for operative dentistry. Australian Dental Journal, 52, 264–270. [DOI] [PubMed] [Google Scholar]
- Mukhaimer, R. , Hussein, E. & Orafi, I. (2012) Prevalence of apical periodontitis and quality of root canal treatment in an adult Palestinian sub‐population. Saudi Dental Journal, 24, 149–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Munn, Z. , SM, M.C.S. , Lisy, K. , Riitano, D. & Tufanaru, C. (2015) Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. International Journal of Evidence‐Based Healthcare, 13, 147–153. [DOI] [PubMed] [Google Scholar]
- Närhi, T.O. , Leinonen, K. , Wolf, J. & Ainamo, A. (2000) Longitudinal radiological study of the oral health parameters in an elderly Finnish population. Acta Odontologica Scandinavica, 58, 119–124. [DOI] [PubMed] [Google Scholar]
- Nekoofar, M.H. , Ghandi, M.M. , Hayes, S.J. & Dummer, P.M.H. (2006) The fundamental operating principles of electronic root canal length measurement devices. International Endodontic Journal, 39, 595–609. [DOI] [PubMed] [Google Scholar]
- Ödesjö, B. , Helldén, L. , Salonen, L. & Langeland, K. (1990) Prevalence of previous endodontic treatment, technical standard and occurrence of periapical lesions in a randomly selected adult, general population. Dental Traumatology, 6, 265–272. [DOI] [PubMed] [Google Scholar]
- Oginni, A.O. , Adeleke, A.A. & Chandler, N.P. (2015) Root canal treatment and prevalence of apical periodontitis in a nigerian adult subpopulation: a radiographic study. Oral Health & Preventive Dentistry, 13, 85–90. [DOI] [PubMed] [Google Scholar]
- Özbaş, H. , Aşcı, S. & Aydın, Y. (2011) Examination of the prevalence of periapical lesions and technical quality of endodontic treatment in a Turkish subpopulation. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics, 112, 136–142. [DOI] [PubMed] [Google Scholar]
- Page, M.J. , McKenzie, J.E. , Bossuyt, P.M. , Boutron, I. , Hoffmann, T.C. , Mulrow, C.D. et al. (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. British Medical Journal, 372, n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters, L.B. , Lindeboom, J.A. , Elst, M.E. & Wesselink, P.R. (2011) Prevalence of apical periodontitis relative to endodontic treatment in an adult Dutch population: a repeated cross‐sectional study. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, 111, 523–528. [DOI] [PubMed] [Google Scholar]
- Petersson, K. , Petersson, A. , Olsson, B. , Hakansson, J. & Wennberg, A. (1986) Technical quality of root fillings in an adult Swedish population. Dental Traumatology, 2, 99–102. [DOI] [PubMed] [Google Scholar]
- Petersson, K. , Lewin, B. , Hakansson, J. , Olsson, B. & Wennberg, A. (1989) Endodontic status and suggested treatment in a population requiring substantial dental care. Dental Traumatology, 5, 153–158. [DOI] [PubMed] [Google Scholar]
- Punch, C. (1997) Prevalence and technical quality of root canal fillings in an Australian population. [MDSc thesis]. Melbourne: The University of Melbourne. [Google Scholar]
- Righolt, A.J. , Jevdjevic, M. , Marcenes, W. & Listl, S. (2018) Global‐, regional‐, and country‐level economic impacts of dental diseases in 2015. Journal of Dental Research, 97, 501–507. [DOI] [PubMed] [Google Scholar]
- Rocha, J.L. , Braga, A.C. , Carvalho, M.F. & Pina‐Vaz, I. (2012) Prevalence of apical periodontitis and endodontic treatment in an adult endodontic treatment. Archives of Oral Research, 8, 219–227. [Google Scholar]
- Schwendicke, F. , Frencken, J.E. , Bjørndal, L. , Maltz, M. , Manton, D.J. , Ricketts, D. et al. (2016) Managing carious lesions: consensus recommendations on carious tissue removal. Advances in Dental Research, 28, 58–67. [DOI] [PubMed] [Google Scholar]
- Segato, A.V.K. , Piasecki, L. , Felipe Iparraguirre Nuñovero, M. , da Silva Neto, U.X. , Westphalen, V.P.D. , Gambarini, G. et al. (2018) The accuracy of a new cone‐beam computed tomographic software in the preoperative working length determination ex vivo. Journal of Endodontics, 44, 1024–1029. [DOI] [PubMed] [Google Scholar]
- Segura‐Egea, J.J. , Jiménez‐Pinzón, A. , Poyato‐Ferrera, M. , Velasco‐Ortega, E. & Ríos‐Santos, J.V. (2004) Periapical status and quality of root fillings and coronal restorations in an adult Spanish population. International Endodontic Journal, 37, 525–530. [DOI] [PubMed] [Google Scholar]
- Segura‐Egea, J.J. , Jiménez‐Pinzón, A. , Ríos‐Santos, J.V. , Velasco‐Ortega, E. , Cisneros‐Cabello, R. & Poyato‐Ferrera, M.M. (2008) High prevalence of apical periodontitis amongst smokers in a sample of Spanish adults. International Endodontic Journal, 41, 310–316. [DOI] [PubMed] [Google Scholar]
- Segura‐Egea, J.J. , Martín‐González, J. & Castellanos‐Cosano, L. (2015) Endodontic medicine: connections between apical periodontitis and systemic diseases. International Endodontic Journal, 48, 933–951. [DOI] [PubMed] [Google Scholar]
- Sidaravicius, B. , Aleksejuniene, J. & Eriksen, H.M. (1999) Endodontic treatment and prevalence of apical periodontitis in an adult population of Vilnius, Lithuania. Endodontics & Dental Traumatology, 15, 210–215. [DOI] [PubMed] [Google Scholar]
- Skudutyte‐Rysstad, R. & Eriksen, H.M. (2006) Endodontic status amongst 35‐year‐old Oslo citizens and changes over a 30‐year period. International Endodontic Journal, 39, 637–642. [DOI] [PubMed] [Google Scholar]
- Soikkonen, K.T. (1995) Endodontically treated teeth and periapical findings in the elderly. International Endodontic Journal, 28, 200–203. [DOI] [PubMed] [Google Scholar]
- Sunay, H. , Tanalp, J. , Dikbas, I. & Bayirli, G. (2007) Cross‐sectional evaluation of the periapical status and quality of root canal treatment in a selected population of urban Turkish adults. International Endodontic Journal, 40, 139–145. [DOI] [PubMed] [Google Scholar]
- Terças, A.G. , de Oliveira, A.E.F. , Lopes, F.F. & Maia Filho, E.M. (2006) Radiographic study of the prevalence of apical periodontitis and endodontic treatment in the adult population of São Luís, MA, Brazil. Journal of Applied Oral Science, 14, 183–187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tibúrcio‐Machado, C.S. , Michelon, C. , Zanatta, F.B. , Gomes, M.S. , Marin, J.A. & Bier, C.A. (2021) The global prevalence of apical periodontitis: a systematic review and meta‐analysis. International Endodontic Journal, 54, 712–735. [DOI] [PubMed] [Google Scholar]
- Timmerman, A. , Calache, H. & Parashos, P. (2017) A cross sectional and longitudinal study of endodontic and periapical status in an Australian population. Australian Dental Journal, 62, 345–354. [DOI] [PubMed] [Google Scholar]
- Touré, B. , Kane, A.W. , Sarr, M. , Ngom, C.T.H. & Boucher, Y. (2008) Prevalence and technical quality of root fillings in Dakar, Senegal. International Endodontic Journal, 41, 41–49. [DOI] [PubMed] [Google Scholar]
- Trowbridge, H.O. (1990) Immunological aspects of chronic inflammation and repair. Journal of Endodontics, 16, 54–61. [DOI] [PubMed] [Google Scholar]
- Tsuneishi, M. , Yamamoto, T. , Yamanaka, R. , Tamaki, N. , Sakamoto, T. , Tsuji, K. et al. (2005) Radiographic evaluation of periapical status and prevalence of endodontic treatment in an adult Japanese population. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, 100, 631–635. [DOI] [PubMed] [Google Scholar]
- Ureyen Kaya, B. , Kececi, A.D. , Guldas, H.E. & Orhan, H. (2013) A retrospective radiographic study of coronal‐periapical status and root canal filling quality in a selected adult turkish population. Medical Principles and Practice, 22, 334–339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van der Veken, D. , Curvers, F. , Fieuws, S. & Lambrechts, P. (2017) Prevalence of apical periodontitis and root filled teeth in a Belgian subpopulation found on CBCT images. International Endodontic Journal, 50, 317–329. [DOI] [PubMed] [Google Scholar]
- Vengerfeldt, V. , Mändar, R. , Nguyen, M.S. , Saukas, S. & Saag, M. (2017) Apical periodontitis in southern Estonian population: prevalence and associations with quality of root canal fillings and coronal restorations. BMC Oral Health, 17, 147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace, B.C. , Dahabreh, I.J. , Trikalinos, T.A. , Lau, J. , Trow, P. & Schmid, C.H. (2012) Closing the gap between methodologists and end‐users: R as a computational Back‐end. Journal of Statistical Software, 49, 1–15. [Google Scholar]
- Weiger, R. , Hitzler, S. , Hermle, G. & Löst, C. (1997) Periapical status, quality of root canal fillings and estimated endodontic treatment needs in an urban German population. Endodontics and Dental Traumatology, 13, 69–74. [DOI] [PubMed] [Google Scholar]
- Whelton, H.P. , Spencer, A.J. , Do, L.G. & Rugg‐Gunn, A.J. (2019) Fluoride revolution and dental caries: evolution of policies for global use. Journal of Dental Research, 98, 837–846. [DOI] [PubMed] [Google Scholar]
- Wolters, W.J. , Duncan, H.F. , Tomson, P.L. , Karim, I.E. , McKenna, G. , Dorri, M. et al. (2017) Minimally invasive endodontics: a new diagnostic system for assessing pulpitis and subsequent treatment needs. International Endodontic Journal, 50, 825–829. [DOI] [PubMed] [Google Scholar]
- Zhong, Y. , Chasen, J. , Yamanaka, R. , Garcia, R. , Kaye, E.K. , Kaufman, J.S. et al. (2008) Extension and density of root fillings and postoperative apical radiolucencies in the veterans affairs dental longitudinal study. Journal of Endodontics, 34, 798–803. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1
Table S2
Table S3
Data Availability Statement
Data available on request from the authors.